
Abstract
Bone metastasis occurs frequently in patients with nasopharyngeal carcinoma (NPC). Although fluorine-18 fluorodeoxyglucose positron emission tomography with computed tomography (PET/CT) has been proven to be more sensitive at detecting bone metastases than Technetium-99m methylene diphosphonate skeletal scintigraphy in pretreatment patients with NPC in most clinical settings, there have been metastatic lesions that were positive on skeletal scintigraphy but negative on PET/CT scans. Herein, we report the case of a patient with stage IV NPC that manifested as multiple metabolically abnormal lesions on pretreatment skeletal scintigraphy and were considered malignant although they were negative on PET/CT examination. Follow-up evaluations with both skeletal scintigraphy and PET/CT scans as post-therapeutic imaging are also presented.
Keywords
Introduction
Among the head and neck malignancies, nonkeratinizing nasopharyngeal carcinoma (NPC) is a squamous cell carcinoma of the epithelium with a World Health Organization histologic classification of type II (differentiated nonkeratinizing carcinoma) or type III (undifferentiated carcinoma). 1 Epstein–Barr virus infection is etiologically associated with NPC; therefore, it shows an endemic distribution, with the highest incidence rates in South-Eastern Asia, including Singapore, Indonesia, Malaysia, and South-Eastern China. In the endemic region, NPC is the sixth most common cancer among male patients. 2
Compared with all other head and neck malignancies, NPC has the highest rate of lymph node and/or distant organ metastasis. 3 Skeletal metastases are the most common sites of distant metastasis (approaching 70%–80%), followed by hepatic (30%) and then pulmonary (18%) metastases.4–6 Like most other cancers, the most important predictor of patient survival is the presence of distant metastases, which is strongly associated with the lymphatic nodal status (N stage). 6 A previous study revealed that approximately 40% of patients with advanced N-stage nonkeratinizing NPC (N2 or N3) showed evidence that the bone marrow had been invaded by tumor cells following transiliac biopsy. 7
The most frequent site of distant metastasis by NPC is reported to be the skeleton. Skeletal metastases caused 30% of the deaths in patients with advanced NPC. A previous study also suggested that the sites and numbers of bone metastases were prognostic factors. 8 Growing evidence has shown that a small portion of patients with NPC with bone metastasis (especially with a solitary lesion) can achieve long‑term survival and complete responses with aggressive treatment. 9 Hence, it is crucial to detect distant metastases including bone metastases in the pretreatment evaluation to allow optimal prognosis predictions for patients with NPC.
Conventional skeletal scintigraphy using Technetium-99m methylene diphosphonate (Tc-99m MDP) is the most commonly used method of detecting bone metastases. It has the advantages of wide availability, reproducibility, and high cost-effectiveness. Additionally, the development of single-photon emission computed tomography/computed tomography (SPECT/CT) has improved clinical sensitivity and specificity. SPECT/CT has been increasingly used in clinical evaluations due to its increased ability to more accurately anatomically localize lesions.
Fluorine-18 fluorodeoxyglucose (F-18 FDG) positron emission tomography/computed tomography (PET/CT) is a whole-body examination that detects the increased glucose uptake of tumor cells, thereby offering anatomical and functional information in a single scan. 10 Using F-18 FDG PET/CT, bone metastases were found in 30 of 202 (15%) eligible patients by Liu et al. 6 PET/CT was more effective than skeletal scintigraphy (94.6% vs. 88.6% accuracy for patient-based analysis, and 93.1% vs. 88.1% accuracy for region-based analysis of the spine).
In the pretreatment staging of NPC, F-18 FDG PET/CT has been proven to be more sensitive than skeletal scintigraphy at detecting distant bone metastases. 6 However, in the clinical setting, we have faced situations where metastatic bone lesions were positive in skeletal scintigraphy but negative in PET/CT scans. Herein, we present a patient with NPC who manifested multiple metastatic lesions in a skeletal scintigraphy that were negative in a PET/CT scan.
Case Report
A 32-year-old man had presented at a local clinic with symptoms of blood-tinged sputum and a painless right neck lump for a 4-month period. He had received medical treatment, but the symptoms and signs persisted. He was the referred to the otorhinolaryngologic outpatient department. On physical examination, he was found to have right cervical lymphadenopathies, which were elastic, fixed, and painless. Endoscopic examination was performed and demonstrated a nasopharyngeal mass involving the nasopharyngeal roof. Biopsy for tissue confirmation was performed, and histopathological examination revealed a differentiated, nonkeratinizing carcinoma of the nasopharynx (WHO type II). Magnetic resonance imaging of the head and neck region revealed a mass lesion in the left Rosenmuller’s fossa. Regional invasion was not detected. Bilateral enlarged cervical lymph nodes were found in the right cervical levels IB, IIA, and VA and the left levels IIB, III, VA, and VB regions.
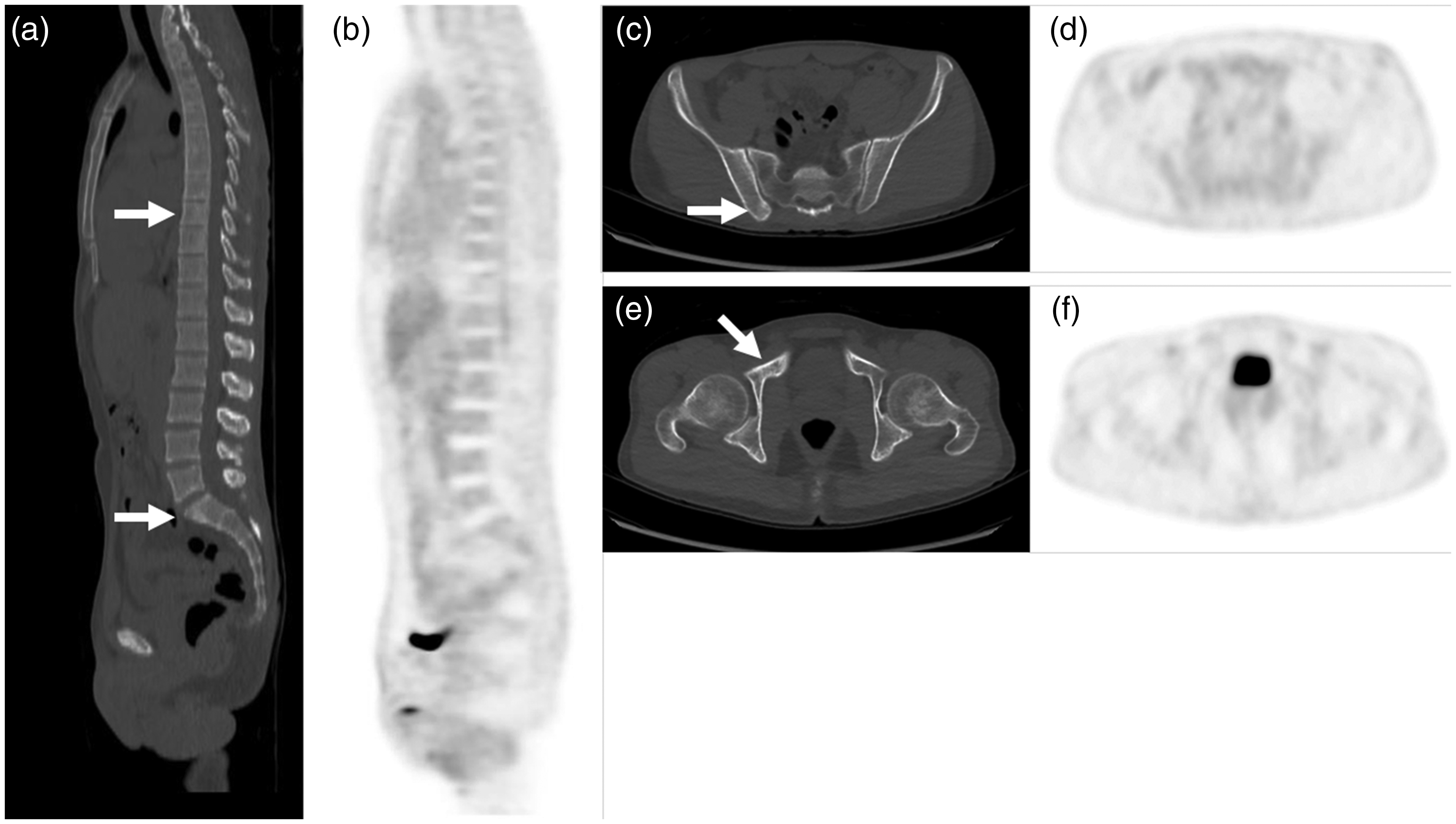
Tc-99m MDP skeletal scintigraphy was then performed as part of the pretreatment cancer work-up to detect bone metastases. This revealed metabolically abnormal lesions in the nasopharynx, left frontal and right parietal skull, T9 vertebral body, sacrum, right ilium near the sacroiliac joint, lower portion of the right acetabulum, right femoral greater trochanter, and sternal end of the right clavicle (Figure 1). To make a complete clinical staging, we examined the patient for possible visceral metastasis by performing a whole-body F-18 FDG PET/CT scan. After intravenous injection of 10 mCi (370 MBq) FDG, PET imaging revealed hypermetabolic activity in the primary nasopharyngeal lesion and bilateral cervical metastatic lymph nodes. There were osteosclerotic bone lesions (i.e., spine, right clavicle, and right ilium) on the CT from the PET/CT scan, which corresponded with the skeletal scintigraphy. However, FDG PET/CT detected barely any FDG abnormality in the sites on which skeleton scintigraphy showed abnormal radiotracer accumulation (Figure 2).

A 32-year-old male patient with nasopharyngeal carcinoma (NPC). Pretreatment staging with Technetium-99m methylene diphosphonate (Tc-99m MDP) skeletal scintigraphy ((a) anterior view; (b) posterior view) detected abnormal metabolic lesions, especially in left frontal skull, sternal end of the right clavicle (with posterior shine-through), T9 thoracic vertebral body, sacrum, right ilium near the sacroiliac junction, lower portion of the right acetabulum, and right femoral greater trochanter (all with arrows). Focal increased uptake in the maxillae and left mandibular area suggested certain dental problems.

Pretreatment fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) scan of the 32-year-old male patient with nasopharyngeal carcinoma (NPC)/((a), (c), (e), CT images; (b), (d), (f), PET images). FDG PET/CT detected osteosclerotic lesions (i.e., T9 vertebral body, sacrum, right ilium near the sacroiliac junction, and lower portion of the right acetabulum, all with arrows) with barely any FDG abnormalities where skeleton scintigraphy showed abnormal radiotracer accumulation.
The patient then was diagnosed with stage IV NPC with multiple bone metastases. After completing chemotherapy and radiation therapy, post-treatment Tc-99m MDP skeletal scintigraphy and F-18 FDG PET/CT were obtained to evaluate therapeutic response. Marked improvement with almost no abnormal uptake was noted on skeletal scintigraphy after treatment (Figure 3). Previous osteosclerotic lesions with very faint F-18 FDG uptake that corresponded with the metastatic bone lesions on skeletal scintigraphy had resolved on the follow-up PET/CT (Figure 4). In summary, skeletal scintigraphy detected multiple metabolically abnormal lesions, which were considered malignant despite being negative on PET/CT scan. The patient was then regularly followed-up at the outpatient department where he showed a disease-free status.

Post-therapeutic imaging evaluation with Technetium-99m methylene diphosphonate (Tc-99m MDP) skeletal scintigraphy ((a), anterior view; (b) posterior view). Marked improvement with nearly no abnormal uptake was noted on skeletal scintigraphy after the patient completed chemotherapy and radiation therapy for NPC.
Post-therapeutic imaging evaluation with a fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) scan ((a), (c), and (e), CT images; (b), (d), and (f), PET images). The FDG PET/CT revealed that previous osteosclerotic lesions with barely any FDG abnormalities had been resolved.
This is a retrospective case study in which all clinical data were retrospectively collected via medical chart review. No non-routine clinical procedures were used. The patient was treated in accordance with the World Medical Association Declaration of Helsinki.
Discussion
On the basis of their radiographic appearance, bone metastases are typically classified into three categories, i.e., lytic, sclerotic, or mixed types. Where bone resorption predominates, focal bone destruction occurs with little new bone formation, which leads the metastasis having an osteolytic appearance. Conversely, sclerotic appearance of lesions with bone metastases can be characterized by increased osteoblastic activity. 11 Owing to preferential uptake of the tracer at sites of active bone formation, bone scintigraphy is sensitive at detecting osteoblastic lesions and provides information and higher detectability of osteoblastic activity and skeletal vascularity. 12
FDG PET quantifies metabolic activity to directly detect the presence of tumor cells. 12 In osteolytic lesions, a higher glycolytic rate is usually found due to the presence of more tumor cells. 6 Consequently, FDG PET/CT was sensitive at detecting osteolytic or mixed types of bone metastatic lesions. 13 In patients with NPC, most bony metastases are osteolytic or mixed-type lesions,7,14 and therefore FDG PET/CT is considered to be better than bone scintigraphy at detecting bone metastases.
Although PET was more sensitive at detecting metastatic bone lesions from NPC, Yang et al. 15 reported that there are metastatic lesions that show as positive in skeletal scintigraphy but negative in FDG PET/CT. The reason is that these lesions had relatively smaller marrow spaces that might confine the number of proliferating tumor cells at the earlier phase of metastasis in which the osteoblastic reaction often occurs. Therefore, skeletal scintigraphy is advantageous at detecting lesions with smaller marrow space. Furthermore, Yang et al. found that skeletal scintigraphy had a detection accuracy similar to that of FDG PET/CT in a patient-based analysis.
In this case report, we demonstrated a clinical presentation in which skeletal scintigraphy was more sensitive than FDG PET/CT at detecting bone metastases from NPC. This case should remind clinicians that conventional skeletal scintigraphy should be used as an important complement for detecting bone metastasis in patients with NPC.
Conclusions
Although in most clinical settings FDG PET/CT has been proven to be more sensitive than skeletal scintigraphy at detecting bone metastases in patients with NPC, skeletal scintigraphy should remain an important complement for detecting metastatic bone lesions.
Footnotes
Author Contributions
Conceptualization, methodology, and writing‐original draft preparation, W.-J. Y. Validation, writing‐review and editing, supervision, C.-C. C. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Ethics approval and consent to participate
This report was performed in accordance with the ethical standards in the Declaration of Helsinki. Ethical committee approval was not required because the review process of the case report was done retrospectively without affecting the patient’s clinical management. Written informed consent was obtained from the patient to analyze their medical data in the future.
Funding
None.