
Abstract
Objective
To investigate the expression of interleukin (IL) 17A in Chinese patients with chronic rhinosinusitis (CRS) and analyse its correlation with clinical parameters.
Methods
Patients undergoing functional endoscopic sinus surgery and matched controls were included in this retrospective study. Clinical assessments (using a visual analogue scale of symptom severity, Johansson endoscopic score and Lund–Mackay computed tomography score) were performed preoperatively. Mucosal specimens were analysed for inflammatory infiltration and IL-17A expression, using immunohistochemistry.
Results
In total, 40 patients undergoing functional endoscopic sinus surgery and 16 controls were included in the study. IL-17A levels were significantly higher in tissues from patients with CRS (with or without nasal polyps) than in control tissues. In CRS, IL-17A expression tended to be higher in tissues with infiltrating neutrophils than in those with infiltrating eosinophils, but this difference was not significant. IL-17A expression in CRS was positively correlated with symptom severity, endoscopic findings and radiological appearance.
Conclusions
Expression of IL-17A was higher in Chinese patients with CRS than in controls, and was associated with infiltrating inflammatory cells, symptom severity, endoscopic findings and radiological appearance. These findings suggest that IL-17A may play a role in CRS pathogenesis and remodelling of nasal polyps.
Introduction
Chronic rhinosinusitis (CRS) is a common clinical syndrome characterized by inflammation of the mucosa of the nose and paranasal sinuses; it is typically classified into CRS with nasal polyps (CRSwNP) and CRS without nasal polyps (CRSsNP). 1 The exact aetiology and pathogenesis of CRS remain unclear. 2 Bacteria, viruses and fungi have been implicated in the establishment of the inflammatory process.3,4 In addition, a variety of cytokines may also play a part. Several studies have investigated the role of interleukin IL) 17, an inflammatory cytokine synthesized by T-helper (Th) 17 cells, 5 in the pathogenesis of CRS.6–8 However, the local expression of IL-17 in various CRS phenotypes is unclear. Zhang et al. 9 reported that polyp tissue showed neutrophilic inflammation with upregulation of Th17 cells in Chinese patients with CRSwNP, but not in Belgian patients with CRSwNP. However, Jiang et al. 8 demonstrated an IL-17 response in patients with CRSwNP from northeast China, regardless of whether eosinophilic or noneosinophilic inflammation was present.
In the present retrospective study, expression of IL-17A (the prototypic member of the IL-17 family) was investigated in CRS, and correlations between IL-17A expression and clinical parameters were analysed.
Patients and methods
Patients
Chinese patients with CRS – who had undergone functional endoscopic sinus surgery at the Department of Otolaryngology, People’s Hospital of Deqing County, Zhejiang, China, or the Department of Otolaryngology, First Affiliated Hospital, Zhejiang University Faculty of Medicine, Zhejiang, China, between May 2010 and April 2012 – were recruited to the study. Patients who had taken antibiotics, antihistamines or corticosteroids before surgery and patients with a history of aspirin intolerance, allergic rhinitis or asthma were excluded from analysis. The diagnosis of CRS was based on medical history, clinical examination, nasal endoscopic examination and computed tomography (CT) scanning, according to guidelines set out in the European Position Paper on Rhinosinusitis and Nasal Polyps, 2007. 10 Specimens were obtained from samples taken at the time of surgery, from excised nasal polyps that had been located in the middle meatus in patients with CRSwNP; samples were also taken from inflammatory sinus mucosal tissue in the middle meatus, in patients with CRSsNP; samples were processed immediately after surgical excision.
Uncinate process mucosal specimens obtained during septoplasty were used for histological analysis of control tissues. The control samples had been taken from patients from the same institutions as the patients with CRS. The control patients had undergone septoplasty because of nasal dysfunction caused by anatomical variation, and did not have sinus disease, chronic rhinitis, allergic rhinitis or asthma.
The study was approved by the Institutional Review Boards of the People’s Hospital of Deqing County and the First Affiliated Hospital, Zhejiang University Faculty of Medicine. Verbal informed consent was obtained from all study participants.
Clinical assessment
Preoperative symptom severity was categorized by study participants using a visual analogue scale (VAS) as mild (0–3), moderate (4–7) or severe (8–10). Symptoms included nasal drainage of pus, nasal obstruction/congestion, impaired sense of smell, facial pressure/pain, headache, bad breath, weakness/fatigue, dental pain, ear fullness/pain, and cough. The individual symptom scores were combined to give an overall mean symptom severity score, with a maximum score of 10.
Nasal endoscopic findings were assessed using the Johansson staging system, 11 with scores assigned for polyps (0, none; 1, middle meatus only; 2, beyond the middle meatus; 3, complete obstruction), discharge (0, none; 1, clear and thin; 2, thick and purulent), oedema (0, absent; 1, mild; 2, severe) and scarring (0, absent; 1, mild; 2, severe). Scores for the right and left nasal cavities were added together, to give an overall score with a maximum score of 18. Any score ≥1 was defined as abnormal.
Findings on CT scans were quantified using the Lund–Mackay scale score. 12 Each sinus (maxillary, frontal, anterior ethmoid, posterior ethmoid and sphenoid) was scored as 0 (no opacification), 1 (partial opacification) or 2 (complete opacification). The ostiomeatal complex was scored as 0 (no opacification) or 2 (opacification). The right and left sides were scored separately and the scores were added together, giving a maximum possible overall score of 24. 12 Any score of ≥1 was defined as abnormal.
Immunohistochemical analysis
Paraffin-wax blocks containing formalin-fixed biopsies from the study participants were retrieved from the pathology archives. Sections 4 µm thick were immunostained with a rabbit polyclonal antibody specific for IL-17 (Santa Cruz Biotechnology, Santa Cruz, CA, USA), using an EliVision™ plus IHC Kit (Maixin Biological, Fuzhou, China) according to the manufacturers’ instructions. Briefly, sections were deparaffinized with xylene and dehydrated through an ethanol series. Endogenous peroxidase activity was blocked by incubating the slides in 1.5% hydrogen peroxide, in absolute methanol, at room temperature for 10 min. Primary antibodies were applied for 1 h at room temperature. Sections were then treated with 50 µl of polymer enhancer for 20 min and 50 µl of polymerized horseradish peroxidise-conjugated antimouse immunoglobulin G for 30 min. Reaction products were visualized using diaminobenzidine (Maixin Biological); sections were counterstained with haematoxylin and eosin, dehydrated and evaluated using light microscopy. Cells positive for IL-17A expression were stained brown. For negative controls, phosphate-buffered saline solution (pH 7.4) was used instead of the primary antibody. The number of cells positive for IL-17A (as a percentage of total number of cells) was counted in 10 randomly selected fields at high-power magnification (×400) by two independent observers, unaware of the source of the clinical materials. The mean percentage of positive cells was then calculated. Specimens were also assessed for the presence of inflammatory cells; infiltration was defined as >8% and >5% for eosinophils and neutrophils, respectively. 8
Statistical analyses
Results were given as the mean ± SD. The Student’s t-test was used to compare mean values and correlation analyses were performed using Spearman’s correlation coefficient. A P-value of <0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS® software, version 19.0 (SPSS Inc., Chicago, IL, USA).
Results
clinical characteristics
Interleukin (IL) 17A expression and clinical characteristics in patients with chronic rhinosinusitis (CRS) and matched controls (patients undergoing septoplasty).

P < 0.05 and P < 0.001 versus controls; Student’s t-test.
VAS, visual analogue scale; scores categorized as mild (0–3), moderate (4–7) or severe (8–10).
Histopathological and immunohistochemical findings
Light microscopic analysis of haematoxylin and eosin stained sections from patients with CRS showed epithelial thickening or squamous metaplasia, oedema and infiltration by many inflammatory cells (eosinophils, plasma cells, mucosal glands, neutrophils and mast cells) (Figure 1). Little proliferation of epithelial cells was observed in the control group (data not shown). Specimens showing infiltration by eosinophils, infiltration by neutrophils and co-infiltration with both eosinophils and neutrophils were significantly more frequently found in patients with CRS than in controls (P < 0.05) (Table 1).
Immunohistochemical staining of a nasal polyp specimen from a patient with chronic rhinosinusitis, showing interleukin-17A expression in epithelial cells (brown staining on the original slide), infiltrating inflammatory cells (eosinophils and neutrophils) and mucosal glands (scale bar represents 100 µm).
On immunohistochemical staining, the percentage of cells positive for IL-17A expression was significantly higher (P < 0.05) in patients with CRS than in controls (Table 1). When divided according to the presence of nasal polyps, the percentages of cells positive for IL-17A expression in patients with CRSwNP and CRSsNP were 23.12 ± 8.46% and 17.00 ± 8.46%, respectively; the difference between these values was not statistically significant, but both were significantly higher than the percentage of cells positive for IL-17A expression in controls (P < 0.05). When divided according to the presence of inflammatory cells, the percentages of cells positive for IL-17A expression in CRS associated with infiltration of eosinophils, neutrophils, or eosinophils and neutrophils were 23.22 ± 8.98%, 18.27 ± 7.06% and 29.33 ± 4.62%, respectively. The only significant difference between these groups was between IL-17A expression in CRS with co-infiltration by eosinophils and neutrophils, with CRS with infiltration of neutrophils (P = 0.026). IL-17A expression was significantly higher in all these CRS groups, compared with in controls (P < 0.05).
IL-17A expression and clinical parameters
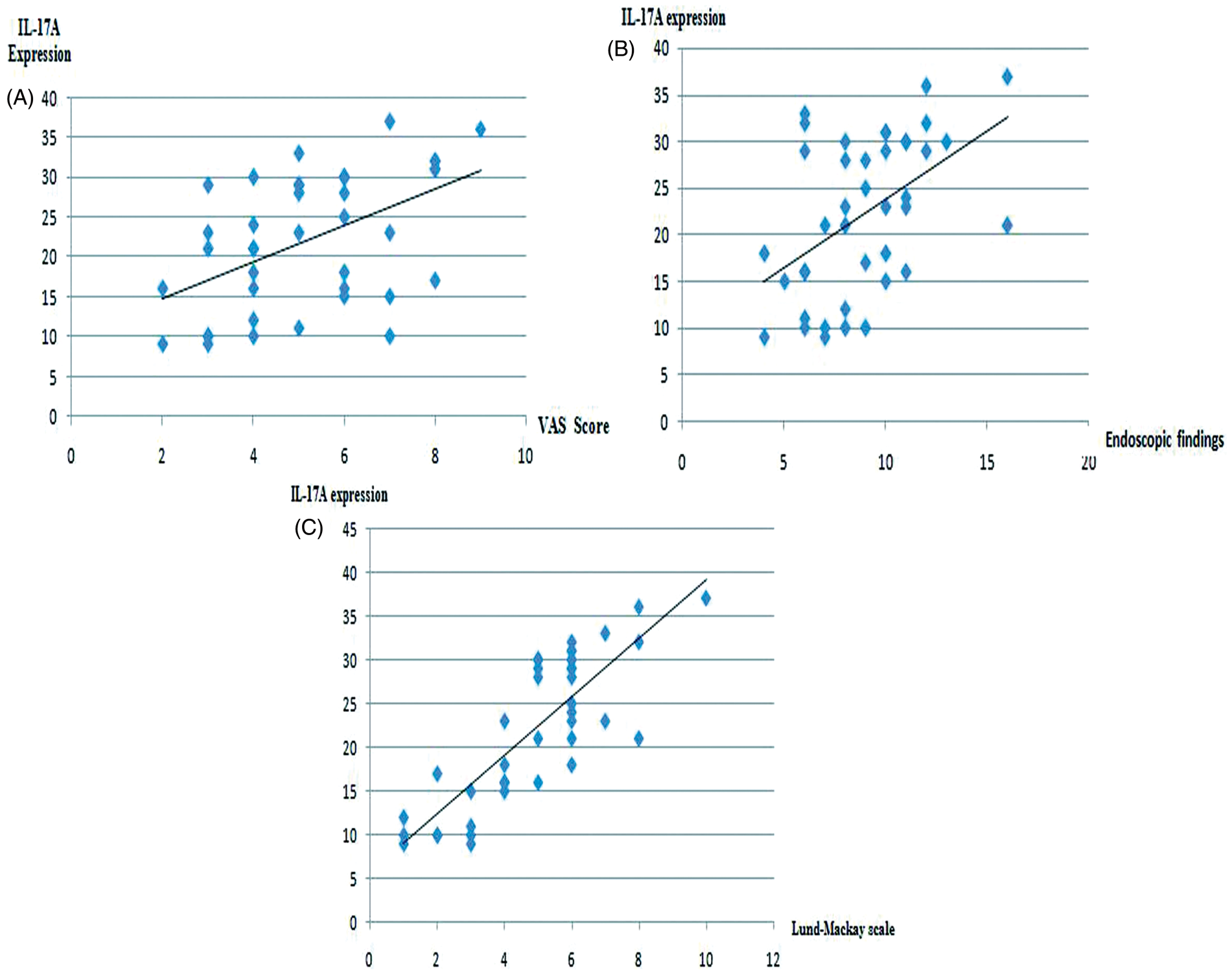
There were no significant differences in IL-17A expression according to age or sex (data not shown). There were significant positive correlations between IL-17A expression in patients with CRS and the symptom severity VAS score (r = 0.516; P = 0.001; Figure 2A), the Johansson endoscopic score (r = 0.485; P = 0.002; Figure 2B) and the Lund–Mackay CT score (r = 0.875; P < 0.001; Figure 2C). When divided according to the symptom severity VAS score, the percentages of cells positive for IL-17A expression in CRS patients with mild, moderate and severe symptoms were 15.88 ± 6.68%, 22.38 ± 7.74% and 29.83 ± 6.55%, respectively (P < 0.05).
Discussion
Chronic rhinosinusitis is a multifactorial, heterogeneous group of diseases with different underlying aetiologies and pathophysiologies. 13 Imbalance in the T-helper cell subsets Th1, Th2 and Th17 is thought to be important in the pathogenesis of CRS.8,14 Th17 cells are characterized by the production of IL-17A7,15,16 and play a significant role in the pathogenesis of a diverse group of immune-mediated conditions, including asthma and other allergic diseases.17,18 Various studies have revealed that the expression of IL-17A in CRS differs among different populations. For example, studies involving Western and Japanese participants have shown that CRSwNP is characterized by a considerable number of IL-17A-positive cells, which are strongly correlated with the number of eosinophils.6,7 Zhang et al. 9 reported an increase in the level of IL-17A protein, which is responsible for neutrophil recruitment and activation, in nasal polyp tissue samples from Chinese patients compared with tissue samples from Belgian patients. However, Cao et al. 18 and Jiang et al. 8 found no significant difference in IL-17A expression between nasal polyps with and without eosinophilic inflammation. Molet et al. 19 reported that the main IL-17-positive inflammatory cell type in patients with nasal polyps in the USA was the T cell. Thus, the expression of IL-17A in CRS requires further study.
In the present study, increased IL-17A expression was demonstrated, in association with infiltrating eosinophils and neutrophils, in Chinese patients with CRS. This is consistent with reports by Cao et al. 18 and Jiang et al. 8 In the present study, significantly more cells expressed IL-17A in sinonasal tissue samples from patients with CRSwNP and CRSsNP than in controls, but there was no significant difference in expression between patients with CRSwNP and those with CRSsNP. In contrast, Makihara et al. 6 found that significantly more cells expressed IL-17A in sinonasal tissues from patients with CRSwNP than in samples from those with CRSsNP or those without CRS. The differences in these findings may be due to differences in sample selection: there were only six patients with CRSsNP in the present report and 16 in the report of Makihara et al. 6 The finding in the present study that expression of IL-17A was significantly higher in patients with CRS than in controls suggests that IL-17A expression may play a role in the pathogenesis of CRS and the remodelling of nasal polyps. Upper and lower airway inflammation may be related to frequent exposure to microbial and viral agents in the upper airway, which is known to trigger a strong IL-17 response.7,20
Few studies have explored the relationship between IL-17A expression and clinical features of CRS.6,7 In the present study, expression of IL-17A was associated with certain clinical features. There were no significant associations between IL-17A expression and age or sex. However, significant positive correlations were seen between IL-17A expression in CRS and symptom severity, endoscopic findings and CT appearance. Makihara et al. 6 found a significant positive correlation between the radiological severity of sinusitis and both the total number of IL-17A-positive cells and the degree of eosinophilia in sinonasal tissue samples from patients with CRSwNP. 6 However, Saitoh et al. 7 reported that CT and symptom scores were not correlated with the number of IL-17A-positive cells in CRS. Makihara et al. 6 have suggested that these differences may be due to differences in sample selection. The present study and the study by Makihara et al. 6 included various phenotypes such as non-CRS, CRSwNP and CRSsNP, whereas those in the study by Saito et al. 7 were all patients with CRSwNP.
In conclusion, the present study demonstrated that IL-17A expression was higher in Chinese patients with CRSwNP and CRSsNP than in controls. Using immunohistochemistry, IL-17A expression was shown to be associated with infiltrating eosinophils and neutrophils in CRS. IL-17A expression was higher in CRS samples with infiltrating neutrophils than in those with eosinophils, but the difference was not statistically significant. There were significant positive correlations between IL-17A expression in CRS and symptom severity, endoscopic findings and radiological appearance.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Science and Technology Bureau of Deqing County, Zhejiang, China (no. 2009Ny01).