
Abstract
Objective
The association of the IL-17A rs2275913 polymorphism with the risk of colorectal cancer (CRC) has been previously reported. However, the results are inconsistent. In this study, we comprehensively assessed the effect of the rs2275913 polymorphism on CRC risk.
Methods
The rs2275913 polymorphism of 208 CRC patients and 312 age- and gender-matched healthy controls was genotyped by the polymerase chain reaction-restriction fragment length polymorphism method, and then analyzed by logistic regression. In addition, a pooled analysis based on five single-center studies was performed using Stata 12.0 software.
Results
Logistic regression analysis indicated that the IL-17A rs2275913 polymorphism was associated with CRC risk (GA vs. GG: OR = 1.53, 95% CI = 1.02–2.28; AA vs. GG: OR = 1.89, 95% CI = 1.11–3.20; GA+AA vs. GG: OR = 1.62, 95% CI = 1.11–2.37; A vs. G: OR = 1.38, 95% CI = 1.07–1.77). Further pooled analysis also indicated a statistically significant association between the rs2275913 polymorphism and CRC risk in Asians and Northern Africans.
Conclusion
This study suggested that the IL-17A rs2275913 polymorphism may act as a biomarker for predicting CRC risk. However, further functional research should be performed to clarify the role of the rs2275913 polymorphism in the etiology of CRC.
Introduction
Colorectal cancer (CRC) is the third most common type of cancer in males and the second most common type of cancer in women. 1 Several lifestyle-related factors, such as obesity, heavy alcohol consumption, smoking and physical inactivity, have been reported to increase the risk of developing CRC.2,3 In addition, individual genetic factors can also play an important role in CRC development. KRAS, NRAS and BRAF gene mutations could serve as prognostic and predictive biomarkers in CRC. 4
The human interleukin 17A (IL17A) gene is located on chromosome 6p12.2 and encodes a cytokine which was initially identified in 1993 as cytotoxic T-lymphocyte-associated antigen (CTLA)-8. 5 The cytokine is produced mainly by activated T cells, while its receptor is distributed ubiquitously. 6 IL-17A participates in the regulation of diverse immune functions, such as the expression of various inflammatory cytokines and chemokines, production of antibodies, and activation and recruitment of leukocytes.7,8 IL-17A is often described as a mediator of inflammation with a crucial role in the development of multiple cancers.9–11 In CRCs, the expression levels of IL-17A were significantly increased compared with those of adjacent normal tissues.12,13 Serum cysteine–cysteine motif chemokine ligand 20 (CCL20) combined with IL-17A may act as early diagnostic and prognostic biomarkers for CRC. 13 In addition, several studies from different countries found that a single nucleotide polymorphism (SNP) located at the promoter region of the IL17A gene (rs2275913) may affect an individual’s risk of developing CRC.14–16 However, Bedoui et al. showed that there was no significant association between the rs2275913 polymorphism and CRC risk. 17 Although a case-control study explored the potential association in a Chinese population, the results needed to be further confirmed due to the small sample size of the study. 14 Hence, in the present study, we not only investigated the association of the rs2275913 polymorphism with CRC risk in a Chinese population by a case-control study method, but also systematically assessed the association of the rs2275913 polymorphism and CRC risk by a pooled analysis method. Overall, we found that the IL-17 rs2275913 polymorphism is associated with CRC risk and may act as a biomarker for predicting susceptibility to CRC.
Materials and Methods
Subjects
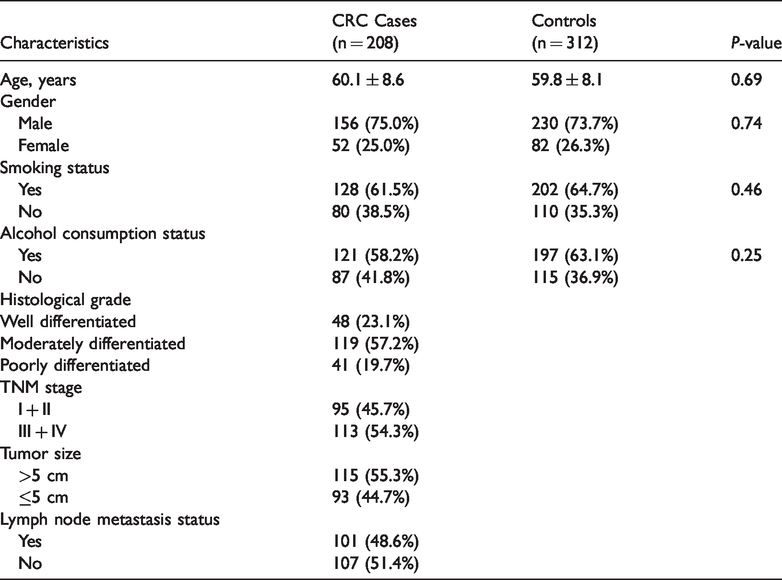
In the case–control study, 208 patients with histopathologically diagnosed CRC and 312 gender- and age-matched healthy controls were recruited from Xuhui District Central Hospital of Shanghai between October 2017 and December 2019. The healthy controls were selected from the health examination center at the same hospital. Any control subject with a personal or family history of cancer or digestive disease was excluded. The demographic and medical data of the patients and healthy controls were collected (Table 1). This study was approved by the Ethics Committees of the hospital (No: 047-001). Written informed consent was obtained from each subject.
Demographic and medical data of the colorectal cancer (CRC) patients and healthy controls.
Genomic DNA extraction and genotyping
Genomic DNA was extracted from peripheral blood leukocytes of each subject by using the QIAamp DNA Mini Kit (Qiagen, Hilden, Germany). The concentration and quality of the extracted DNA were measured by using a NanoDrop spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA). The rs2275913 polymorphism was genotyped using the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) method. The primers used for the nucleotide extension reaction were 5ʹ-
Data collection
The PubMed, Embase and CNKI databases were used to search for published studies on the association of the rs2275913 polymorphism with CRC risk. Search terms included “interleukin 17A or IL17A,” “rs2275913 or polymorphism or variant,” and “colorectal cancer or CRC.” The last search was performed on 20 April 2020. Specific information, including the first author's name, country, ethnicity, genotyping method, genotype frequency distribution of the rs2275913 polymorphism in cases and controls, and the results of Hardy–Weinberg equilibrium (HWE) tests in the control group, was collected independently by two researchers from relevant and eligible studies. An eligible study on the association of the rs2275913 polymorphism with CRC risk needed to meet the following conditions: a) be a case-control study; b) have a control group HWE test P-value > 0.05; c) have genotype and allele data available. Any discrepancies would be resolved by discussion with the third researcher.
Statistical analysis
The differences in age, gender, smoking and alcohol consumption between case and control subjects were calculated using a Student's t test or chi-square (χ2) test, respectively. The deviation between the observed and the expected frequencies among controls was evaluated by HWE test through a goodness-of-fit χ2 test. In the case-control study, the association between the rs2275913 polymorphism and CRC risk was evaluated by computing the adjusted odds ratios (ORs) and their 95% confidence intervals (CIs) using logistic regression analysis. In the pooled analysis, the crude ORs with 95% CI were calculated based on a random effect model to assess the association. In addition, the stability of the results of the pooled analysis was evaluated by sensitivity analysis. A possible publication bias was evaluated by Begg's test and Egger's test. All statistical analyses were conducted on SPSS 22.0 (IBM Corp., Armonk, New York, USA) or Stata 12.0 software (StataCorp LP, College Station, TX, USA) with the significance level at P<0.05.
Results
The mean age (mean ± SD) of patients and healthy controls was 60.1±8.6 and 59.8±8.1 years, respectively (P = 0.69). The ratio of males to females was 156:52 and 230:82 in patients and healthy controls, respectively (P = 0.74). The genotype and allele distributions for the IL-17A rs2275913 polymorphism were significantly different between CRC patients and healthy controls (Table 2). The genotype frequencies of the IL-17A rs2275913 polymorphism were in accordance with HWE test among the control subjects (PHWE = 0.85). The GA or AA genotype carriers showed a significantly increased risk for CRC (GA vs. GG: OR = 1.53, 95% CI = 1.02–2.28, P = 0.04; AA vs. GG: OR = 1.89, 95% CI = 1.11–3.20, P = 0.02). Similarly, under a dominant or additive model, the IL-17A rs2275913 polymorphism was also associated with an increased risk for CRC (GA+AA vs. GG: OR = 1.62, 95% CI = 1.11–2.37, P = 0.02; A vs. G: OR = 1.38, 95% CI = 1.07–1.77, P = 0.02).
A case-control study of the association between the rs2275913 polymorphism of the IL-17A gene and colorectal cancer (CRC) risk.

a: adjusted for age, gender, smoking and alcohol consumption; OR, odds ratio; CI, confidence interval.
Five studies with 1023 CRC cases and 1223 controls were enrolled in the pooled analysis (Table 3). Therein, there were three studies on Asian populations and two studies on Northern African populations. The overall results showed that the IL-17A rs2275913 polymorphism was associated with CRC risk for all the genotype comparisons (GA+AA vs. GG: OR = 1.65, 95% CI = 1.29–2.10, P<0.001; AA vs. (GA+GG): OR = 1.63, 95% CI = 1.12–2.35, P = 0.010; AA vs. GG: OR = 1.98, 95% CI = 1.29–3.05, P = 0.002; GA vs. GG: OR = 1.57, 95% CI = 1.23–2.00, P<0.001; A vs. G: OR = 1.48, 95% CI = 1.24–1.78, P<0.001) (Table 4). In addition, the effects of the IL-17A rs2275913 polymorphism on CRC risk were also observed in the subgroup analyses based on an Asian population (GA+AA vs. GG: OR = 1.62, 95% CI = 1.18–2.23, P =0.003; AA vs. (GA+GG): OR = 1.82, 95% CI = 1.14–2.89, P = 0.011; AA vs. GG: OR = 2.35, 95% CI = 1.30–4.24, P = 0.005; GA vs. GG: OR = 1.43, 95% CI = 1.14–1.80, P = 0.002; A vs. G: OR = 1.52, 95% CI = 1.16–2.01, P = 0.003) and a Northern African population (A vs. G: OR = 1.47, 95% CI = 1.11–1.95, P = 0.007). The sensitivity analysis showed the reliability and stability of the whole pooled results under four other genotype comparisons, except for AA vs. (GA+GG) (Figure 1). Furthermore, there was no remarkable publication bias in Begg's test. However, Egger’s test indicated a publication bias affecting the overall results under (AA+GA) vs. GG (Table 5).
Features of the studies included in the pooled analysis.

*: the current case-control study.
CRC, colorectal cancer; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism; F-RFLP, fluorescent-based restriction fragment length polymorphism.
A pooled analysis of the association between the IL-17A rs2275913 polymorphism and colorectal cancer (CRC) risk.

OR, odds ratio; CI, confidence interval.
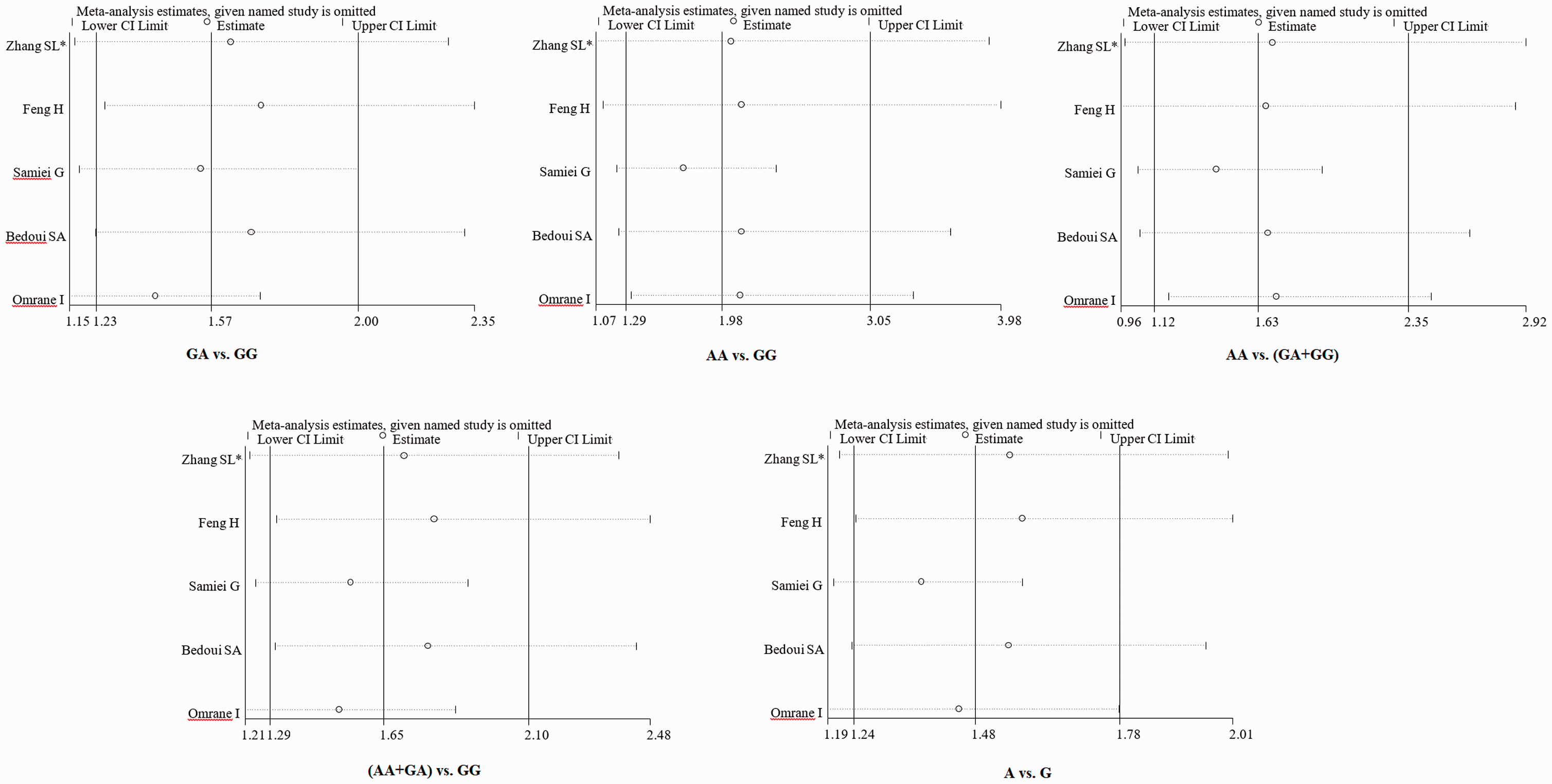
Sensitivity analysis for the overall pooled results.
Publication bias of the pooled analysis based on the overall population.

Discussion
Genetic polymorphisms are a main factor that can cause differences in an individual’s risk for cancer. An SNP is the most common type of human genetic variation. In the past decade, extensive research has been conducted about the association between certain SNPs and CRC risk, and dozens of SNPs have been reported to closely correlate with the occurrence of CRC. 18 Notably, the IL-17A rs2275913 polymorphism has been reported to be associated with the risk of multiple cancers.19–21 However, the published results about the association of the IL-17A rs2275913 polymorphism with CRC risk were inconsistent and needed further clarification.
In the present study, we found that the IL-17A rs2275913 polymorphism was significantly associated with CRC risk in a Chinese population based on a case-control study. Compared with GG genotype carriers, GA or AA genotype carriers had a significantly increased risk for CRC. Similarly, under a dominant or additive model, the IL-17A rs2275913 polymorphism was also associated with an increased risk for CRC in a Chinese population. Further pooled analysis also indicated that the IL-17A rs2275913 polymorphism could affect an individual’s risk of developing CRC. These findings were observed not only in an Asian population, but also in a Northern African population. Overall, the individuals carrying an A allele at this genomic locus had an increased risk of CRC, compared with those carrying a G allele.
Despite a comprehensive analysis of the association between the IL-17A rs2275913 polymorphism and the risk of developing CRC, there were some limitations that should be considered. First, the number of samples and eligible studies remained insufficient, which can possibly lead to an imbalance and publication bias. Second, SNP-SNP and SNP-environment interactions should be taken into consideration, which would help with drawing more exact conclusions. Third, the follow-up data of the patients should have been obtained to analyze the association of this polymorphism with CRC survival rates.
In conclusion, our study presents evidence that the IL-17A rs2275913 polymorphism is associated with CRC risk. However, further well-designed studies are necessary to verify the findings.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by scientific research project of Shanghai Municipal Health Commission (No. 201940389).