
Abstract
This paper reports an unusual case of recurrent canaliculitis who had a long history of chronic rhinosinusitis with nasal polyps. A 74-year-old woman complained of recurrent redness, purulent discharge, and occasional tearing of the left eye for 1 year. She has a 40-year untreated sinusitis history, with recurrent mucopurulent rhinorrhea, nasal obstruction and hyposmia, and loss of smell for 2 years. The patient’s various symptoms, such as epiphora, purulent discharge, rhinorrhea, nasal obstruction, and anosmia, poorly responded to antibiotics and canaliculotomy. However, relief came from the unintentional usage of systemic corticosteroids. Canaliculitis is a rare form of inflammation involving the proximal lacrimal drainage system. Unfortunately, it is often misdiagnosed, has frequent recurrences, and fails to respond to therapy. This case highlights the importance of medical history, lacrimal examinations, and regular therapy in managing recurrent canaliculitis. For those canaliculitis patients with nasal symptoms, simultaneous treatment of nasal-related disorders should be considered.
Introduction
Canaliculitis is a chronic infection of the canaliculus, presenting with epiphora, medial canthal swelling, recurrent conjunctivitis, a swollen pouting punctum, and, in some cases, yellowish or mucopurulent discharge.1,2 Canaliculitis is typically managed with surgical intervention.3–5 However, there is a high risk of relapse, and patients often endure extended conservative therapy with limited success.3,6,7 As a result, persistent epiphora and recurrent canaliculitis following canaliculotomy are frequently reported. 8
Case presentation
A 74-year-old female presented at our facility with recurrent redness, purulent discharge, and occasional tearing of the left eye, persisting for 1 year. She had a history of bacterial conjunctivitis, which was unresponsive to levofloxacin eye drops. A slit-lamp examination revealed erythema and edema of the lower canaliculus and punctum. Firm compression of the lower canaliculus elicited purulent discharge from the lower punctum, with evidence of conjunctival congestion. Irrigation test revealed medium resistance upon fluid injection into the upper and lower punctum. The patient reported a 40-year history of untreated sinusitis with recurrent mucopurulent rhinorrhea, nasal obstruction, and anosmia for the past 2 years. Using a computed tomography (CT) scan, bilateral paranasal sinusitis was identified, and nasal endoscopy showed evidence of nasal polyps (Figure 1). The patient sought treatment at the ENT clinic 3 days ago, where she was diagnosed with chronic rhinosinusitis with nasal polyps (CRSwNP), and conservative treatment with medication was indicated.
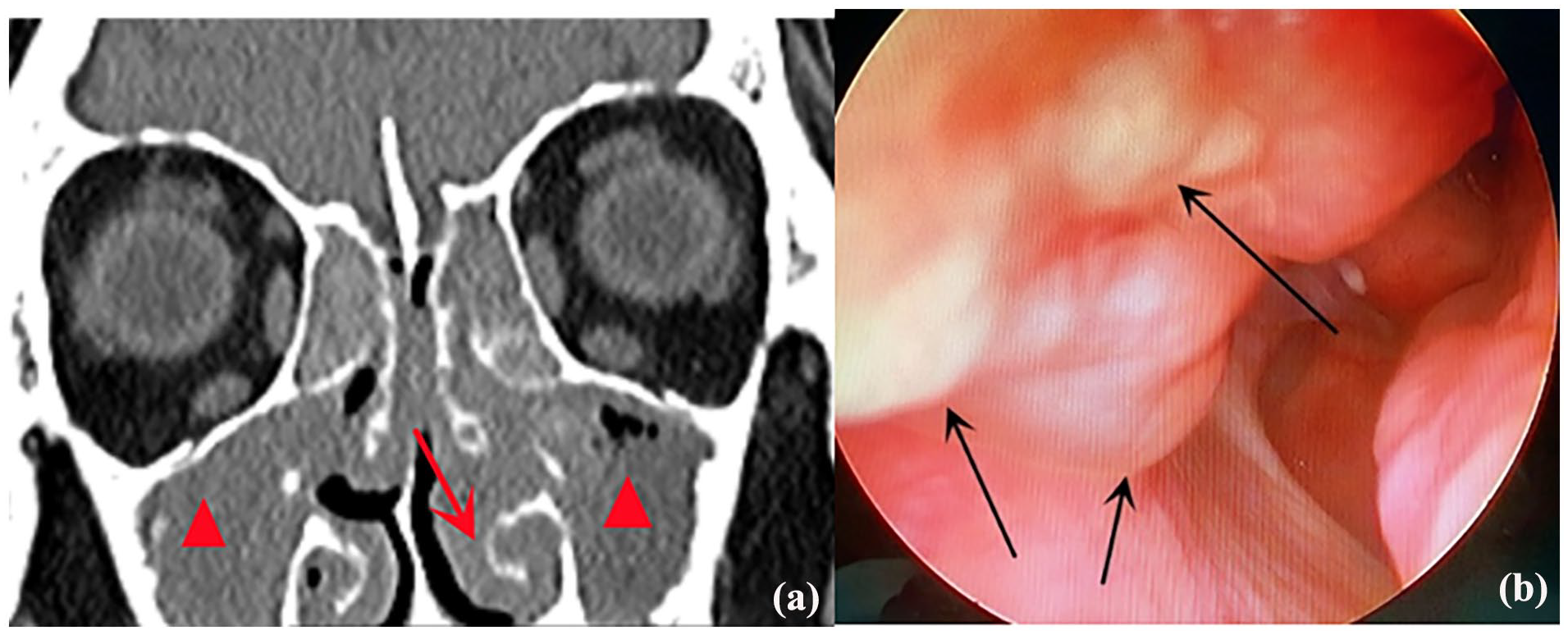
Nasal data for CRSwNP diagnosis prior to canaliculotomy. (a) Sinus CT scan demonstrating bilateral rhinosinusitis (red triangles) and significantly hypertrophic inferior turbinate (red arrow). (b) Nasal polyps observed in the olfactory fissure area via endoscopy (black arrow).
Canaliculotomy and curettage with bicanalicular silicone tube intubation were performed to address the patient’s symptoms. In short, the canaliculus was opened, the pus was evacuated, and multiple red polyps and granulomas were observed (Figure 2), but no concretion was found. Following polyp clearance, a bicanalicular silicone tube was inserted into the nasal cavity through the inferior and superior puncta. A 48-h abscess bacterial cultivation came back negative. She received oral cefuroxime proxetil for 3 days, and a continuous dose of levofloxacin drops post-operation. At the 1-month follow-up (30 days post-operation), the silicone tube was removed due to the persistence of epiphora and purulent discharge. Meanwhile, although the canaliculus and lacrimal passage were irrigated with gentamicin and dexamethasone once every 2 weeks, and the space was packed with gatifloxacin gel, the tearing and pus remained recurrent.
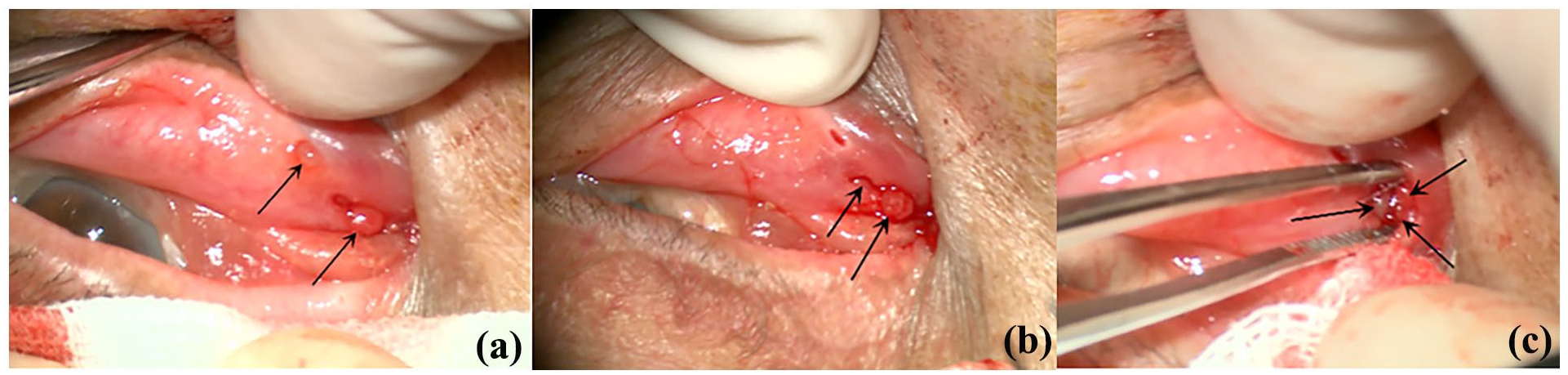
Red polyps observed during canaliculotomy. (a) Polyps (black arrow) identified in the inferior lacrimal punctum and the canaliculus incision. (b) Additional polyps (black arrow) emerging after curettage. (c) Multiple polyps and granulomas (black arrow) visible within the open lumen of the lacrimal canaliculus.
At the 3-month follow-up, the patient reported complete resolution of epiphora, purulent discharge, rhinorrhea, nasal obstruction, and anosmia during hospitalization following a thyroidectomy. Unfortunately, all aforementioned symptoms returned but eased upon hospital discharge. Upon review of the patient’s thyroid surgery, we noted that the primary postoperative medication included intravenous Hydrocortisone Sodium Succinate infusion (200 mg), which was administered once a day for 3 days with no antibiotics. Dacry-ocystography was performed in the fourth month of follow-up, 1 month after her thyroidectomy. According to the orbital CT, there was no absolute obstruction in the lacrimal system, as was evidenced by the weak signal from the contrast medium (Figure 3). The nasal turbinate volume and soft tissue density in the sinus cavity were significantly reduced (Figure 3) compared to the CT image taken 4 months ago (Figure 1). Then the mucosal edema was observed around the nasolacrimal duct opening in the inferior meatus under the nasal endoscopy (Figure 4). The patient expressed satisfaction with the appearance of a normal eyelid and accepted occasional epiphora, discharge, rhinorrhea, and hyposmia while continuing nasal, topical corticosteroids (Mometasone Furoate Aqueous Nasal Spray 50 μg), opting against endoscopic sinus surgery or dacryocystorhinostomy.

Dacryocystography findings on orbital CT. (a) Weak contrast medium signal in the nasolacrimal duct (white arrow) alongside reduced nasal turbinate volume (red arrow) and soft tissue density in the sinus cavity (red triangle) compared to Figure 1. (b) Sagittal CT showing a linear high-density area in the nasolacrimal duct (white arrow).

Endoscopic findings of mucosal edema. Mucosal edema (black arrow) observed around the lower end of the nasolacrimal duct in the inferior meatus under endoscopy.
Discussion
Canaliculitis is a rare disorder, accounting for 0.8% of all lacrimal drainage system infections. 9 Primary canaliculitis is commonly caused by proximal obstruction, often followed by infections with Streptococcus, Staphylococcus, or Actino-myces species.2,10 Secondary canaliculitis, on the other hand, is intricately associated with punctal or intracanalicular plug placement (86.72%), as well as silicone intubation, radiotherapy, tumor in the lacrimal drainage system, and eyelash plug. 7 Despite its well-defined clinical manifestations, the rarity of canaliculitis and complicating factors make it challenging to diagnose.10,11 In this patient, recurrent erythema of the left lower eyelid, a pouting punctum with purulent discharge, and the lack of prior ocular treatment suggested infectious primary canaliculitis. The bacterial culture of the punctal discharge sample was negative, indicating the possibility of aseptic inflammation. However, this did not rule out interference with the preoperative levofloxacin usage.
Canaliculotomy, in combination with silicon intubation, significantly increases the accuracy of canalicular concretion removal and improves canaliculus patency, with an anatomical success rate of 92.7%–96.2% and functional success rate of 78.6%–94.3%.12–14 A minimally invasive canaliculotomy involving curettage and bicanalicular silicone tube intubation was performed, as described by Wang et al. 12 All procedures were successfully completed, and the patient received regular oral cefuroxime proxetil for 3 days post-operation. In addition, patients received continuous doses of levofloxacin throughout the postoperative month to combat purulent discharge until tube removal. Gentamicin and dexamethasone were further employed for lacrimal system irrigation once every 2 weeks, and gatifloxacin gel was administered directly into the canaliculi. Unfortunately, the administered antibiotics failed to resolve the patient’s purulent discharge.
Post-canaliculotomy canaliculitis recurrence can occur in up to 21% of canaliculotomy patients. 10 Most cases of recurrent canaliculitis are attributed to preexisting nasolacrimal duct pathology, prior improper lacrimal sac irrigation procedures, or exacerbation of preexisting nasolacrimal duct obstruction following canaliculotomy. 4 The patient suspected the presence of fluid flow into the nasal and oral cavity during the irrigation examination. This may be because of the mucosal edema and reduced CRSwNP sensation.
CRSwNP generally manifests as nasal obstruction, diminished sense of smell, nasal discharge, and sleep disturbance, adversely affecting the quality of life. 15 Topical corticosteroids, recommended in most clinical guidelines, reduce nasal polyp size and relieve sinonasal symptoms. 16 Among patients with more severe symptoms, short-term systemic corticosteroid usage successfully alleviates clinical symptoms. 17 Corticosteroids are known to alleviate both ocular and nasal symptoms, suggesting a potential link between the patient’s canaliculitis and CRSwNP. Studies show that canalicular polyps rarely share etiopathological mechanisms with nasal polyps, as the latter are more strongly linked to systemic inflammatory pathways rather than localized lacrimal infections in existing reports. 18 The pathological examination of the extracted polyps during canaliculotomy was not performed, so a comparison between the canalicular and nasal polyps could not be performed.
An unusual aspect of this case is unilateral canaliculitis despite the presence of bilateral CRSwNP. A review of the patient’s CT scans revealed more significant hypertrophy of the left inferior turbinate compared to the right, along with greater soft tissue density in the left sinuses (Figure 1). Anterior rhinoscopy revealed a slightly greater number of polyps in the left olfactory fissure compared to the right. Alternatively, a congenital anatomical anomaly in the left canaliculus may have increased its susceptibility to inflammation, exacerbated by CRSwNP. This likely explains the occurrence of unilateral canaliculitis in the context of bilateral CRSwNP.
Conclusions
This report highlights a rare case of recurrent canaliculitis associated with CRSwNP. Management of recurrent canaliculitis should involve a thorough medical history assessment, detailed lacrimal examinations, and routine therapy with antibiotics and corticosteroids. Simultaneous management of the underlying nasal disorder is recommended for canaliculitis patients presenting with nasal symptoms.
Footnotes
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki. This study was conducted with approval from the Ethics Committee of The First People’s Hospital of Changzhou (Approval number/2023-28).
Consent to participate
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Consent for publication
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Authors contributions
CC and YB conceptualized and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. YS provided the nasal data from ENT clinic. CC, YY, and YG designed the data collection instruments, collected data, carried out the initial analyses, and reviewed and revised the manuscript. YB coordinated and supervised data collection and critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The paper was supported by the Changzhou Science and Technology Project (CJ20220104).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.