
Abstract
Objective
To investigate the clinical significance of protocadherin-8 (PCDH8) promoter methylation in bladder cancer.
Methods
Methylation-specific polymerase chain reaction was used to examine the promoter methylation status of PCDH8 in tumour tissue samples obtained from patients with bladder cancer, and in normal bladder epithelial tissue samples obtained from age- and sex-matched control subjects. Methylation status was correlated with demographic, clinical and pathological parameters and disease outcome.
Results
PCDH8 promoter methylation was detected in 76/135 (56.3%) patients with bladder cancer and none of 34 (0%) control subjects. Methylation was significantly associated with advanced stage (T2–T4), high grade (G3), tumour recurrence, larger tumour diameter (>3 cm) and nonpapillary morphology. In addition, methylation was associated with significantly shorter survival time and was an independent predictor of overall survival.
Conclusions
PCDH8 promoter methylation is a common occurrence in bladder cancer, and is associated with malignant behaviour and poor prognosis. Determination of PCDH8 promoter methylation status in tumour tissue may assist in the identification of patients who require aggressive postoperative intervention in order to improve prognosis.
Introduction
Bladder cancer is one of the most common malignant genitourinary tumours worldwide, responsible for ∼145 000 deaths each year. 1 Histologically, >90% of bladder cancers present as transitional cell carcinomas, with 70–80% of tumours being nonmuscle invasive (stage pTa–pT1) and the remainder being muscle invasive (stage pT2–pT4).2,3 Around 50–70% of nonmuscle invasive tumours will recur, with 10–30% progressing to muscle-invasive cancer.2,3 Bladder cancer mortality increases with tumour invasiveness, despite advances in detection, treatment and surveillance strategies.2,3 New molecular biomarkers are needed to assist in outcome prediction and in the identification of high-risk patients who would benefit from aggressive postoperative therapy.2,3
The pathogenesis and development of bladder cancer is a multistep process involving genetic and epigenetic alterations.4–6 Epigenetic alterations (such as DNA methylation) are clinically interesting because it may be possible to reverse such changes and restore gene function.4–6 Epigenetic markers may be useful for the detection, outcome prediction and treatment of bladder cancer.4–6
Protocadherin-8 (PCDH8) functions as a tumour suppressor gene in several human malignancies.7–11 The inactivation of PCDH8 by promoter methylation has been observed in human tumours, and could serve as a tumour-specific biomarker.7–11 The promoter methylation status of PCDH8 and its clinical significance in bladder cancer remain unclear, however. The present study used methylation-specific polymerase chain reaction (PCR) to examine PCDH8 promoter methylation status in tumour tissue samples (from patients with bladder cancer) and matched normal bladder tissue samples from healthy control subjects. The clinical significance of methylation status was determined by correlation with demographic, clinical and pathological parameters and disease outcome.
Patients and methods
Study Population
Tumour tissue samples were collected intraoperatively from patients with histopathologically confirmed bladder transitional cell carcinoma who underwent surgery at the Department of Urology, The General Hospital of Jilin Chemical Group Corporation (CNPC), Jilin, China between March 2002 and March 2005. Inclusion criteria were: (i) histopathologically confirmed primary bladder transitional cell carcinoma; (ii) no history of other malignant tumours; (iii) no anticancer therapy prior to surgery; (iv) availability of sufficient tumour tissue and follow-up data. Tumour diagnosis, staging, therapy and follow-up were performed according to international standards. 12 Normal bladder epithelial tissue was collected from age- and sex-matched control subjects with bladder calculi and no prior tumour history, who were attending the same hospital department. Control tissues were histopathologically examined in order to exclude incidental tumours.
The study was conducted in accordance with the Declaration of Helsinki, 13 and approved by the Ethics Committee of The General Hospital of CNPC, Jilin, China. All study participants provided written informed consent prior to enrolment.
Follow-up and Study Definitions
Patients were followed up, according to guidelines on bladder cancer, 12 at intervals of 3 months to 1 year until death or the conclusion of the study. Overall survival was defined as the time from the date of diagnosis to the date of death from any cause, or last contact if the patient was still alive. Recurrence was defined as any evidence of tumour in a retained bladder ≥3 months after treatment.
Methylation-specific PCR
All tissue specimens were stored in liquid nitrogen until use. Genomic DNA was extracted from 500 mg of tissue using the DNeasy® Tissue Kit (Qiagen, Valencia, CA, USA), then treated with bisulphite to convert any unmethylated (but not methylated) cytosine residues to uracil (EpiTect® Bisulfite Kit; Qiagen). Methylation-specific PCR was performed as described, 11 using a GeneAmp® DNA amplification kit with AmpliTaq® Gold (both from PE Applied Biosystems, Foster City, CA, USA) and primers for methylated and unmethylated PCDH8. Primer sequences were: unmethylated, forward 5′-GGTGGTTATTGGTT ATTTGGTTT-3′ and reverse 5′-CCAAC AAACTCTAAAAACACACA-3′; methylated, forward 5′-CGGTTATTGGTT ATTCGGTTCC-3′ and reverse 5′-ACGA ACTCTAAAAACGCGCG-3′. The cycling programme involved preliminary denaturation at 95°C for 15 min, followed by 40 cycles of denaturation at 95°C for 30 s, annealing at 60°C for 30 s, and elongation at 72°C for 30 s, followed by a final elongation step at 72°C for 10 min. DNA from the nasopharyngeal carcinoma cell line CNE1 was used as positive control for PCDH8 methylation; water was used in place of DNA as negative control. 11 PCR products were separated via 2% agarose gel electrophoresis, stained with ethidium bromide and visualized under ultraviolet illumination. Samples were scored as methylation positive when bands were present in the methylated DNA lane and methylation negative when bands were present only in the unmethylated DNA lane. PCR was performed a minimum of three times per sample. 14
Statistical Analyses
Between-group differences in PCDH8 methylation status were compared using Fisher’s exact test, and the χ2-test was used to assess the relationship between PCDH8 methylation and clinicopathological features. Kaplan–Meier survival analysis and the log-rank test were used to assess differences in overall survival between methylated and unmethylated PCDH8 groups. Multivariate Cox proportional hazard analysis (controlled for tumour grade, stage, recurrence, diameter and number, and patient age and sex) was used to estimate the independent prognostic effect of PCDH8 methylation. Statistical analyses were performed using SAS statistical software, version 8.0 (SAS Institute, Cary, NC, USA) for Windows®. A P-value <0.05 was considered to be statistically significant.
Results
The study included tissue from 135 patients with bladder cancer (96 males/39 females; mean age 69.0 ± 6.7 years, age range 26.0–87.0 years) and 34 age- and sex-matched control subjects (24 males/10 females; mean age 66.0 ± 8.5 years, age range 22.0–83.0 years). Representative methylation-specific PCR findings are shown in Figure 1. PCDH8 promoter methylation was detected in 76/135 (56.3%) patients and none of 34 (0.0%) control subjects (P < 0.0001).
Representative methylation-specific polymerase chain reaction results for protocadherin-8 (PCDH8) promoter methylation in tumour-derived DNA samples from five patients with bladder cancer. M, methylated; U, unmethylated. Cases T 91, T 92 and T 94 exhibited PCDH10 promoter methylation. DNA derived from the nasopharyngeal carcinoma cell line CNE1 was used as positive control.
Correlations between protocadherin-8 (PCDH8) promoter methylation in tumour-derived DNA, and demographic, clinical and pathological characteristics of patients with bladder cancer (n = 135).
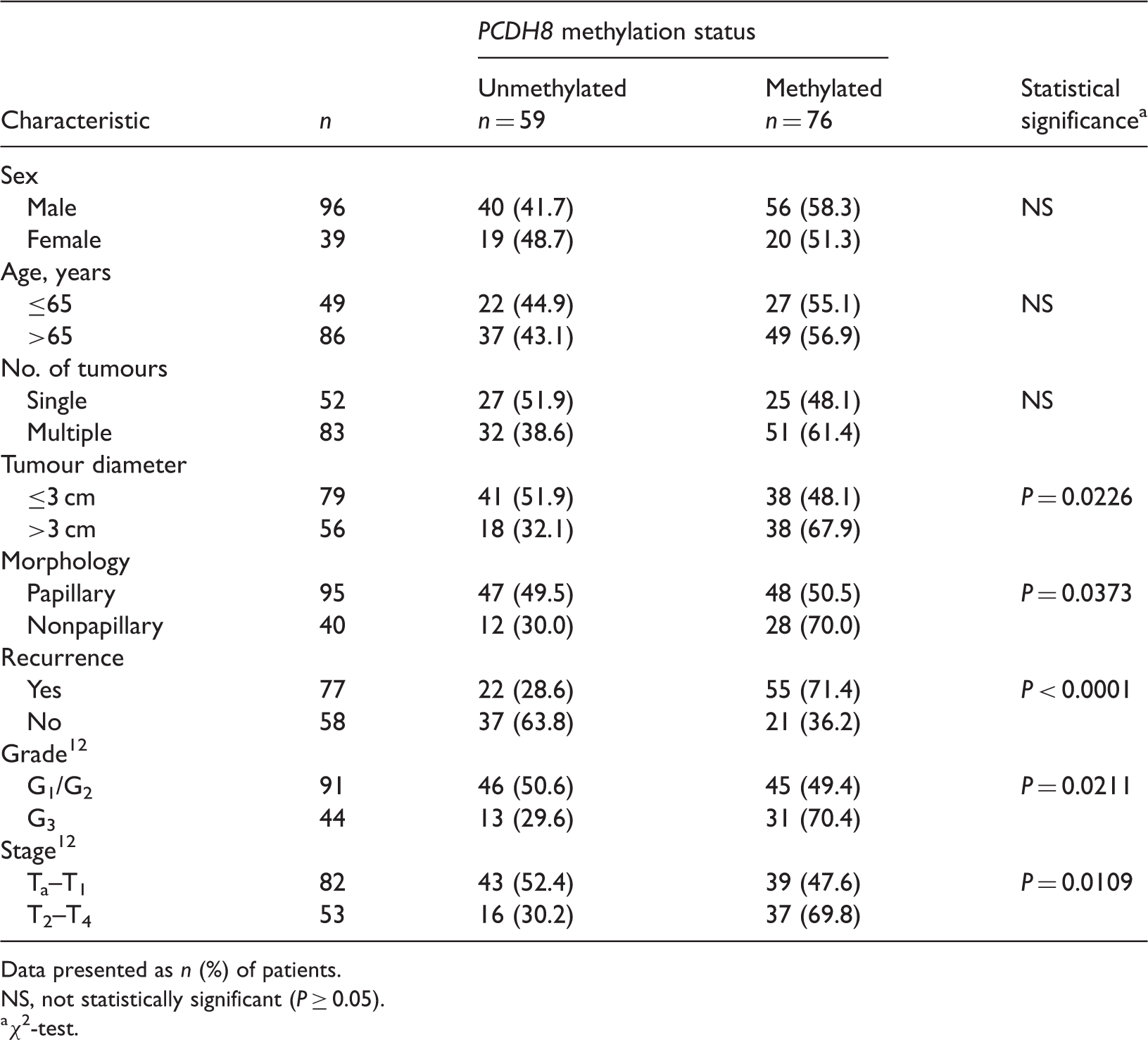
Data presented as n (%) of patients.
NS, not statistically significant (P ≥ 0.05).
χ2-test.
Overall survival was assessed in patients with bladder cancer. Patients with PCDH8 promoter methylation had significantly shorter survival times than those without methylation (P = 0.0004, Figure 2). Multivariate regression analysis revealed that PCDH8 promoter methylation (hazard ratio [HR] 3.972; 95% confidence intervals [CI] 1.761, 8.934), tumour recurrence (HR 2.978; 95% CI 1.023, 7.964), high grade (HR 3.134; 95% CI 1.017, 8.036) and advanced stage (HR 3.704; 95% CI 1.458, 8.687) were independent predictors of overall survival in bladder cancer (Table 2).
Kaplan–Meier survival curves for patients with bladder cancer (n = 135), stratified according to protocadherin-8 (PCDH8) promoter methylation status assessed in tumour-derived DNA. P = 0.0004; log-rank test. Multivariate Cox proportional hazard analysis of independent predictors of overall survival in patients with bladder cancer (n = 135), controlled for tumour grade, stage, recurrence, diameter and number, and patient age and sex. PCDH8, protocadherin-8.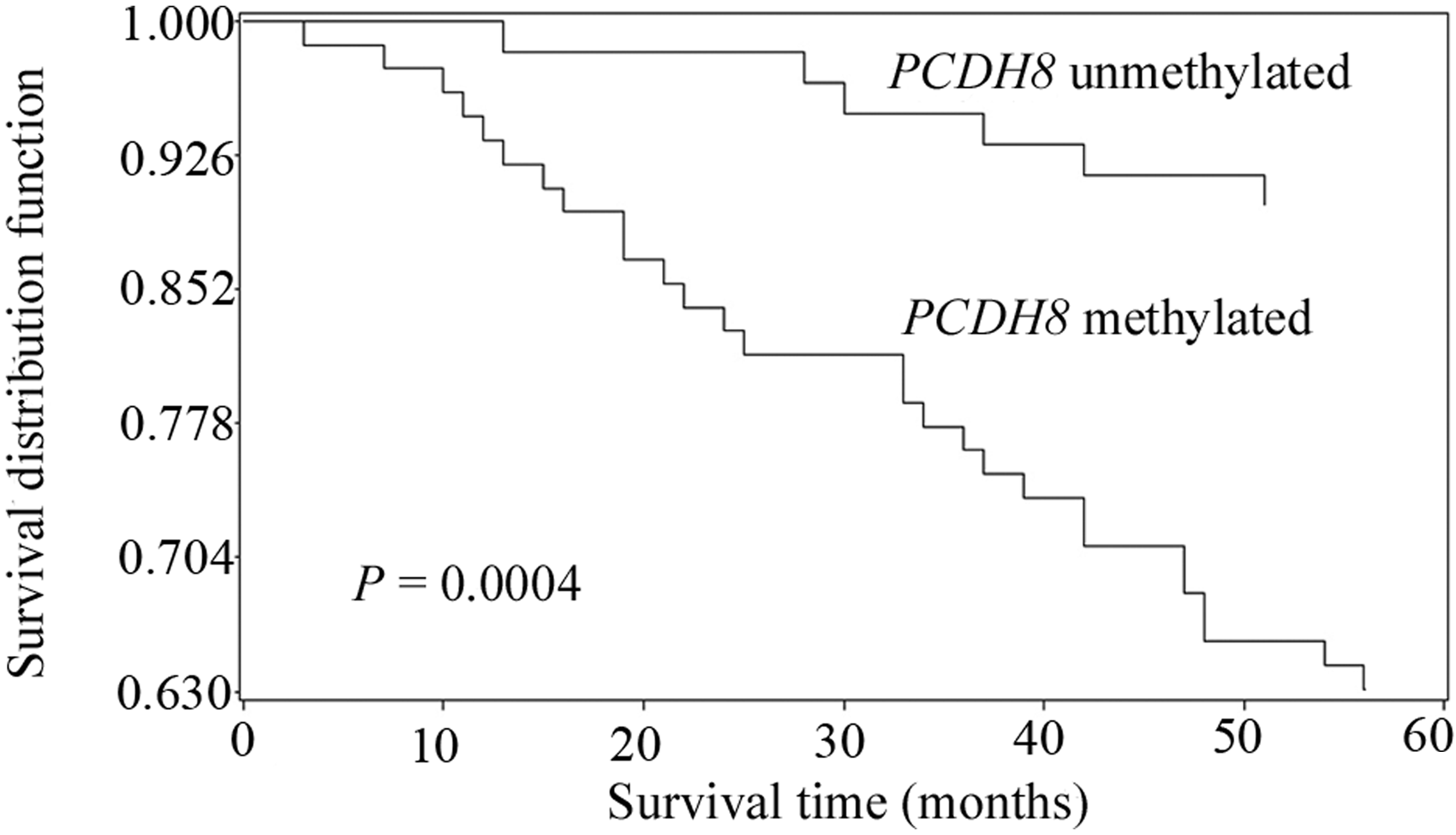

Discussion
Protocadherin-8 acts as a tumour suppressor in human cancers.7–11 PCDH8 is downregulated in tumours, and exogenous PCDH8 expression can suppress tumour cell proliferation and migration.7–11 DNA methylation is an enzyme-induced chemical modification whereby a methyl residue is transferred onto the 5′ position of cytosine molecules. This mainly occurs in cytosine–guanine dinucleotide-rich areas (CpG islands) in gene promoter regions.15–17 The majority of CpG islands are unmethylated in humans, and aberrant methylation in promoter regions can permanently inactivate tumour suppressor genes.15–17 Promoter methylation is a useful biomarker for cancer diagnosis, surveillance and outcome prediction, especially in the case of tumour suppressor gene inactivation.18–20
Promoter methylation of PCDH8 was detected in 56.3% of bladder cancer tissues in the present study but was completely absent from normal bladder epithelial tissue, suggesting that PCDH8 promoter methylation is tumour specific. Methylation was significantly associated with high tumour grade, advanced stage, nonpapillary morphology and large tumour diameter (>3 cm), all of which are known risk factors for progression and poor prognosis in bladder cancer.2,21–23 In addition, PCDH8 methylation was significantly associated with tumour recurrence during follow-up. The high recurrence rate in bladder cancer is a major factor that is known to influence prognosis. 24 Findings of the present study indicate that PCDH8 promoter methylation may be a useful biomarker for bladder cancer malignancy.
The outcome of bladder cancer varies widely, as tumours with similar morphology behave differently. 2 Prognostic biomarkers are vital for the accurate prediction of outcome and to determine which patients need more aggressive postoperative intervention.25–27 PCDH8 methylation was present in a high proportion of bladder cancer tissues in the present study, and was associated with malignant behaviour. PCDH8 promoter methylation may therefore represent a useful prognostic biomarker in bladder cancer. Patients with PCDH8 methylation had significantly shorter survival times than those without methylation, in the present study. In addition, methylation was an independent prognostic indicator. Aggressive postsurgical intervention should be performed in patients found to have PCDH8 promoter methylation, in order to achieve better outcomes.
In conclusion, the present study indicates that PCDH8 promoter methylation is a common occurrence in patients with bladder cancer and is significantly associated with malignant behaviour and poor prognosis. Determination of PCDH8 promoter methylation status in tumour tissue may assist in the identification of patients who require aggressive postoperative intervention. As PCDH8 methylation was present in 56.3% of bladder cancers in the present study, it is possible that around half of the clinical management could be optimized. The present study was limited by its small sample size, and larger-scale prospective studies are required in order to confirm these findings.
Footnotes
Declaration of Conflicting Interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.