
Abstract
Rapid and selective therapeutic hypothermia is a promising neuroprotective method for acute ischemic stroke. A recent study developed a simple but efficient technique of transnasal cooling, in which air at ambient temperature was passed through standard nasal cannula to induce evaporative cooling of the brain. Selective brain temperature decrease was achieved within 25 minutes in piglets. It is a major step forward to initiate early brain cooling. However, it is still necessary to devise a more comprehensive strategy to enhance the benefits of selective brain cooling in the era of effective reperfusion.
Keywords
Therapeutic hypothermia (TH) is one of the most promising neuroprotective treatments for acute ischemic stroke (AIS). 1 Selective brain cooling has gradually gained researchers’ interest to avoid side effects and retain benefits of TH. 2 However, multiple clinical trials failed to replicated the success of selective brain cooling in pre-clinical experiments. Cooling helmets, the most common method of selective cooling, can hardly reach the recommended mild hypothermic status (34–36°C) within a short period after AIS onset. 3 Intra-arterial selective cooling infusion (IA-SCI) can cool the brain rapidly to mild hypothermic status (34–36°C) in minutes, but the invasive operation discourages many patients. 4
Another promising selective brain hypothermia approach, which avoids invasive surgery while guarantees cooling efficiency, is transnasal cooling. A recent study by Koehler et al. proved the safety and feasibility of transnasal cooling in a piglet model. 5 Air at ambient temperature was passed through standard nasal cannula with an open mouth to produce evaporative cooling of the nasal passage. Brain temperature was decreased by 3 °C within 25 minutes and lasted over 6 hours. However, how to combine this approach with common clinical therapy to achieve better outcomes remains still unknown. We want to pursue a discussion concerning how to prolong the duration of the therapy and apply it to adult AIS patients.
The neuroprotective protocol of AIS has been revolutionized by the development of reperfusion therapy. 6 Thus, a great deal of advantages of transnasal cooling make it stand out in the era of effective reperfusion. First and foremost, the conditions of operation for the procedure are so simple that it can be used quickly in patients to achieve early induction of hypothermia. 7 Secondly, this feasible method has been demonstrated to be safe with no reduction of blood flow to the nasal turbinate or nasal mucosa injury. Moreover, air at ambient temperature is chosen to be the cooling medium instead of other coolants, in which case, this strategy does not have to worry about the risk of local frostbite, but also achieves economic benefits. Last but not least, only a standard nasal catheter is used so that it does not interfere with any procedures the patient receives in the hospital.
Therefore, this transnasal cooling method can be applied in various clinical scenarios. When patients miss the time window for reperfusion therapy, TH in prehospital care will be a possible remedy to extend the time window of recanalization treatment. Moreover, the supplies used in this method are easy to assemble and suitable for use in ambulances. Thus, transnasal cooling can become a powerful complementary therapy of thrombolysis and thrombectomy. Besides, airway support and ventilatory assistance are recommended by STAIR XI for the treatments of patients who have decreased consciousness or who have bulbar dysfunction that causes compromise of the airway.8,9 If oxygen in nasal cannula could be combined with evaporative cooling to induce brain hypothermia, transnasal cooling will the preferred neuroprotective therapy during and after recanalization.
Transnasal cooling has been demonstrated to be effective in exerting neuroprotective functions in animal experiments. 10 The device can be further optimized to improve simplicity while maintaining cooling rates, thus enabling it to operate from the AIS onset to reperfusion treatment in first aid. Besides, this approach needs to be considered for extended cooling time and applied in awake patients in order to achieve neuroprotection from before imaging assessment to after reperfusion therapy. Thus, further exploration of the full-time use of intranasal cooling therapy may be a development direction for the adjuvant therapy of reperfusion therapy (Figure 1).
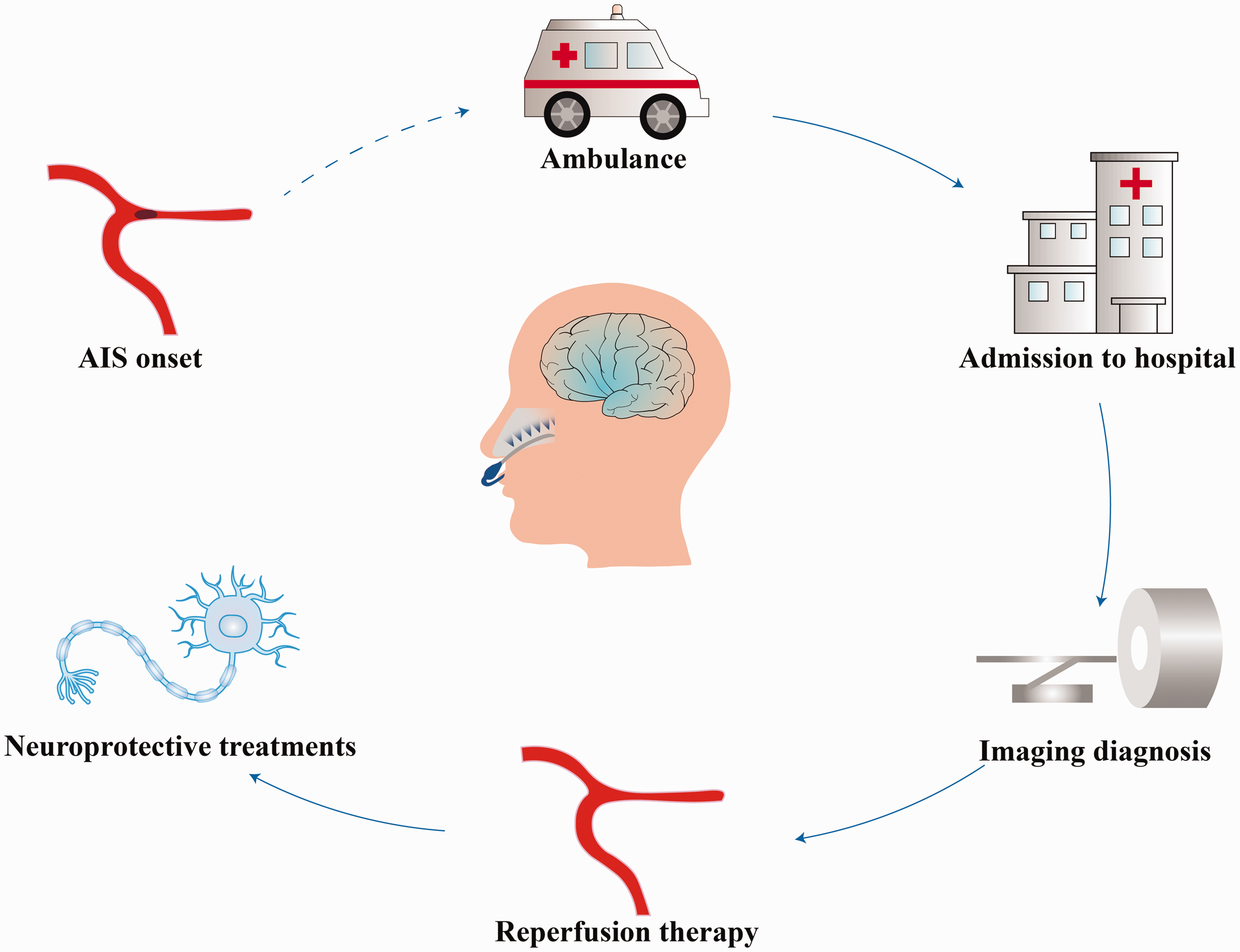
The schematic exhibits a new temperature management strategy by utilizing selective transnasal cooling. Potential clinical scenarios for transnasal cooling include pre-hospital transit, in hospital transfer, imaging diagnosis, and reperfusion therapy.
Transnasal cooling, as a promising selective therapeutic hypothermia, will maximize hypothermic benefits and minimize side effects related to hypothermia in the future. More clinical trials are needed to provide evidence that transnasal cooling therapy as an adjunct treatment could provide tangible clinical benefits by protecting salvageable tissue.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China grant (82071466, 82027802, 82102220); Beijing Municipal Science and Technology Project grant Z181100001918026.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.