
Abstract
Intracerebral hemorrhage (ICH) is one of the most devastating forms of stroke. However, studies on ICH at high altitude are insufficient. We aimed to compare the initial manifestations, imaging features and short-term functional outcomes of ICH at different altitudes, and further explore the effect of altitude on the severity and prognosis of ICH. We retrospectively recruited ICH patients from January 2018 to July 2021 from two centers at different altitudes in China. Information regarding to clinical manifestations, neuroimages, and functional outcomes at discharge were collected and analyzed. Association between altitude and initial severity, neuroimages, and short-term prognosis of ICH were also investigated. A total of 724 patients with 400 lowlanders and 324 highlanders were enrolled. Compared with patients from the plain, those at high altitude were characterized by more severe preliminary manifestations (P < 0.0001), larger hematoma volume (P < 0.001) and poorer short-term functional outcome (P < 0.0001). High altitude was independently associated with dependency at discharge (adjusted P = 0.024), in-hospital mortality (adjusted P = 0.049) and gastrointestinal hemorrhage incidence (adjusted P = 0.017). ICH patients from high altitude suffered from more serious initial manifestations and worse short-term functional outcome than lowlanders. Control of blood pressure, oxygen supplementation and inhibition of inflammation may be critical for ICH at high altitude.
Keywords
Introduction
Intracerebral hemorrhage (ICH) is one of the most devastating forms of stroke characterized by bleeding in the brain parenchyma, 1 which results in substantial disabilities and high mortality (usually 50% at 30 days). 2 The incidence of ICH has been increasing over the past 40 years, and is higher in the developing countries than that in the developed countries.3,4 China has a vast territory, diverse geographical environment with various socioeconomic conditions, and the epidemiology of ICH at different altitudes is still unclear. It has been reported that the proportion of ICH in all stoke subtypes is the highest in Tibet (61.3%), comparing to that in the plain (less than 30%). 5 Despite the higher incidence of ICH in the plateau, the manifestations, radiological features and functional outcomes, especially the relationship between altitude and ICH, have been seldomly explored.
Several retrospective studies revealed that patients at high altitude have more risk factors of ICH (e.g. smoking, drinking, and hypertension), in-hospital complications and poorer prognosis.6 –8 Whether high altitude hypoxia and the higher levels of hemoglobin and blood pressure are associated with the unfavorable outcome need to be further investigated.9,10 On the other hand, the current guidelines and consensuses of prevention and treatment for ICH are based on the studies conducted in lowlanders, whether highlanders need special medical care remains unclear.
The aim of this study was to explore the differences in the manifestations and imaging features of patients from different altitudes. We also would like to analyze the role of altitude in the initial manifestations and short-term prognosis of ICH patients at high altitude.
Methods
Study design, population and data collection
This present study was an observational, retrospective analysis of data from consenting patients admitted at the Affiliated Brain Hospital of Nanjing Medical University (altitude at 20 m) and Yushu People’s Hospital (altitude at 4000 m) with latitude 32.2° in China, and followed the recommendation of Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 11 This was a retrospective study, so informed consent was not needed. Nanjing is a coastal city in Jiangsu Province in eastern China, while Yushu locates in the Qinghai-Tibet Plateau in Qinghai Province in west of China.
We recruited adult patients (≧18 years old) with the first-ever ICH or previous ICH without any sequelae admitted into hospital from January 2018 to July 2021. First-ever ICH was defined as the acute neurological deficits or other symptoms for the first time within 7 days of onset, confirmed by hyperintense area(s) on computed tomography (CT). Previous ICH without any sequelae was defined as the patient who had a history of ICH but did not develop any residual symptoms, and their mRS score was 0 before the onset of the current ICH.
The exclusion criteria include: (1) patients migrated to the local area within 5 years; (2) ICH due to vascular malformation, trauma or tumor; (3) subarachnoid hemorrhage; (4) hemorrhagic transformation of ischemic stroke, and (5) data scarcity. Information including age, gender, ethnicity, education, medical history, results of laboratory examinations (including complete blood count, C-reactive protein [CRP], random blood glucose, blood coagulation, renal function and blood lipids), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were collected when the patients were admitted. National Institute of Health stroke scale (NIHSS) and Glasgow Coma Scale (GCS) upon admission were also recorded to comprehensively assess the severity of symptoms. 12 In-hospital complications such as deep venous thrombosis (DVT), hydrocephalus, epilepsy, gastrointestinal hemorrhage, pulmonary infection, cardiac or renal dysfunction, as well as the patients’ outcome (in-hospital mortality, NIHSS, GCS and modified Rankin Scale [mRS] at discharge) were recorded.
Imaging
CT information was collected upon admission (baseline), 3 days and 7 days after symptom onset. The location of hemorrhage was classified as basal ganglia, thalamus, cerebral lobes (including frontal, parietal, temporal, occipital, and insular lobe), brain stem, cerebellum, and cerebral ventricles. We defined deep ICH as bleeding within the basal ganglia or thalamus, while lobar ICH as bleeding originating from the cortex or cortical-subcortical junctional areas. 13 Intraventricular (IVH) extension secondary to the hemorrhage of intracerebral parenchyma was recorded if present on the baseline CT. 14 The total volume of hematoma and perihematomal edema was calculated with ImageJ version 1.42q, based on the CT images as described previously. 15 The total hematoma volume was defined as parenchymal plus IVH hematoma volumes. Relative perihematomal edema (rPHE) was defined as the ratio of perihematomal edema to hematoma volume. 16 Evaluation was conducted by two experienced neuroradiologists blinded to the patients’ clinical information. Hematoma expansion was measured only for patients who had at least two CT scans and was defined as absolute growth ≥6 mL or a relative growth ≥33% from initial to the next CT.17,18
Outcomes
Primary outcomes were severe initial manifestation and unfavorable short-term outcome. Severe initial manifestation was defined as NIHSS > 15 when admitted. 19 Unfavorable short-term outcome was defined as mRS ≥ 3 at discharge. 20 Secondary outcomes were mRS at discharge, hematoma expansion, in-hospital mortality and complication.
Subgroup analysis
To avoid the influence of ethnicity on the results of ICH, subgroup analysis was performed to explore the differences of initial manifestations, imaging features and functional outcomes of ICH in Han patients from plateau and plain areas.
Data availability statement
All supporting data for this analysis are available from the corresponding author upon reasonable request. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Ethics Committee of Xuanwu Hospital ([2018]071). The informed consents from patients were not required.
Statical analysis
Categorical variables are presented as frequencies or percentages, and differences between groups were analyzed using chi-square or Fisher’s exact tests. Continuous variables are expressed as mean ± standard deviation (SD) if normally distributed, while as median (interquartile range, IQR) if not. Kolmogorov-Smirnov tests are used to assess the distribution of continuous data. Differences between groups were detected using two-sided Student’s t-tests (normally distributed) or Mann-Whitney U test (non-normally distributed). Logistic regression was performed to investigate the relationship between altitude and initial severity or short-term prognosis, also to explore the risk factors associated with the initial manifestation and unfavorable short-term functional outcome. All statistical analyses were performed with IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, USA), with a two-tailed P value <0.05 considered as statistically significant.
Results
Baseline characteristics
A total of 724 patients were included in this study, with 400 from the plain and 324 from the plateau. Their demographical and baseline clinical characteristics are shown in Table 1. The median age of lowlanders was 63.0 (IQR: 53.0–69.0) years, with 257 (64.3%) male patients, and all the lowlanders were Han. The median age of highlanders was 60.0 (IQR: 51.0–72.0) years, with 204 male (63.0%) patients, and 293 (91.0%) of them were Tibetans. The median BMI of the lowlanders was 24.4 (IQR: 22.1–27.2) kg/m2, while that of the highlanders was 24.2 (IQR: 23.8–26.0) kg/m2. Age, gender and BMI of the ICH patients at different altitudes were similar. Only 48 patients (12.0%) didn’t receive any education in the plains, while 310 patients (95.7%) in the plateau were illiterate (P < 0.0001). Among the risk factors for spontaneous ICH, 1 the incidences of hypertension and polycythemia were higher in patients in the plateau than that in the plains (P < 0.0001), while the incidences of diabetes, dyslipidemia, ischemic stroke, coronary heart disease, and use of antiplatelet and lipid-lowering drugs were higher in lowlanders than that in highlanders (P < 0.05). The incidences of ICH, coagulopathy and use of anticoagulants were similar in the two populations.
Baseline characteristics of ICH patients from different altitudes.
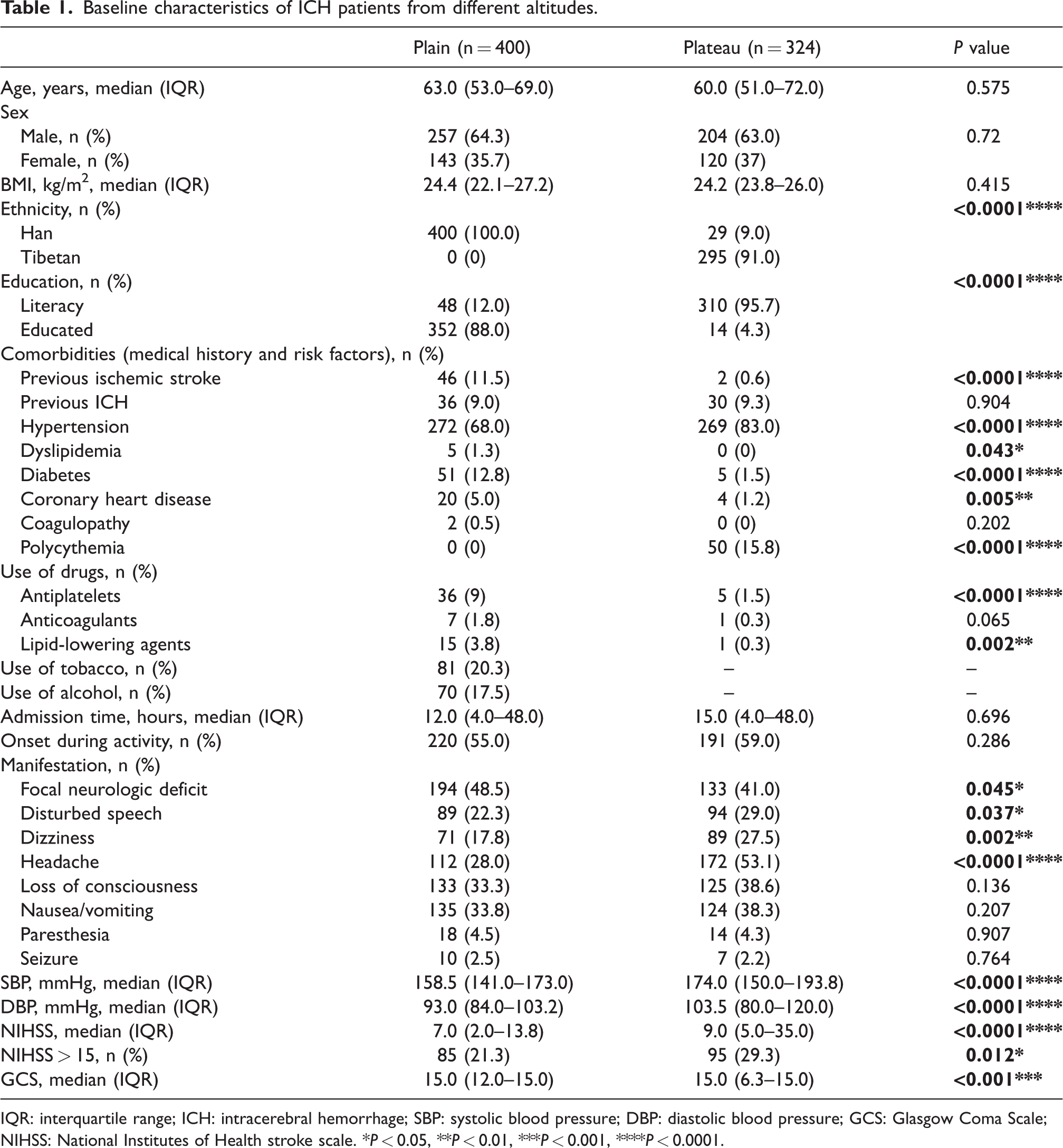
IQR: interquartile range; ICH: intracerebral hemorrhage; SBP: systolic blood pressure; DBP: diastolic blood pressure; GCS: Glasgow Coma Scale; NIHSS: National Institutes of Health stroke scale. *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001.
The onset form and most common manifestations of lowlanders and highlanders were similar, including focal neurological deficits, nausea/vomiting, loss of consciousness, headache, and disturbed speech. However, compared to patients in the plain, initial manifestations of patients in the plateau were more severe, with higher NIHSS (7.0 [IQR: 2.0–13.8] vs. 9.0 [IQR: 5.0–35.0], P < 0.0001) and lower GCS scores (15.0 [IQR: 12.0–15.0] vs. 15.0 [IQR: 6.3–15.0], P < 0.001), though the admission time from ICH onset was similar (P = 0.696). The median admission time of the lowlanders was 12.0 (IQR: 4.0–48.0) hours, while that of the highlanders was 15.0 (IQR: 4.0–48.0) hours. A total of 85 patients (21.3%) in the plain while 95 patients (29.3%) in the plateau suffered from severe ICH (P = 0.012). In addition, patients in the plain showed significantly lower SBP than those in the plateau (158.5 [IQR: 141.0–173.0] mmHg vs. 174.0 [IQR: 150.0–193.8] mmHg, P < 0.0001).
Laboratory examinations and neuroimaging
The results of laboratory examinations and characteristics of neuroimaging are shown in Table 2. Patients at high altitude had more RBC, higher levels of hemoglobin and hematocrit than those in the plain due to high altitude hypoxia exposure (P < 0.0001). In addition, compared to patients in the plain, those resided in the plateau bared more severe inflammation, with more WBC and higher CRP level (P < 0.001). Other biochemical parameters were normal in both populations, though most with differences.
Laboratory tests and imaging of the ICH patients at different altitudes.
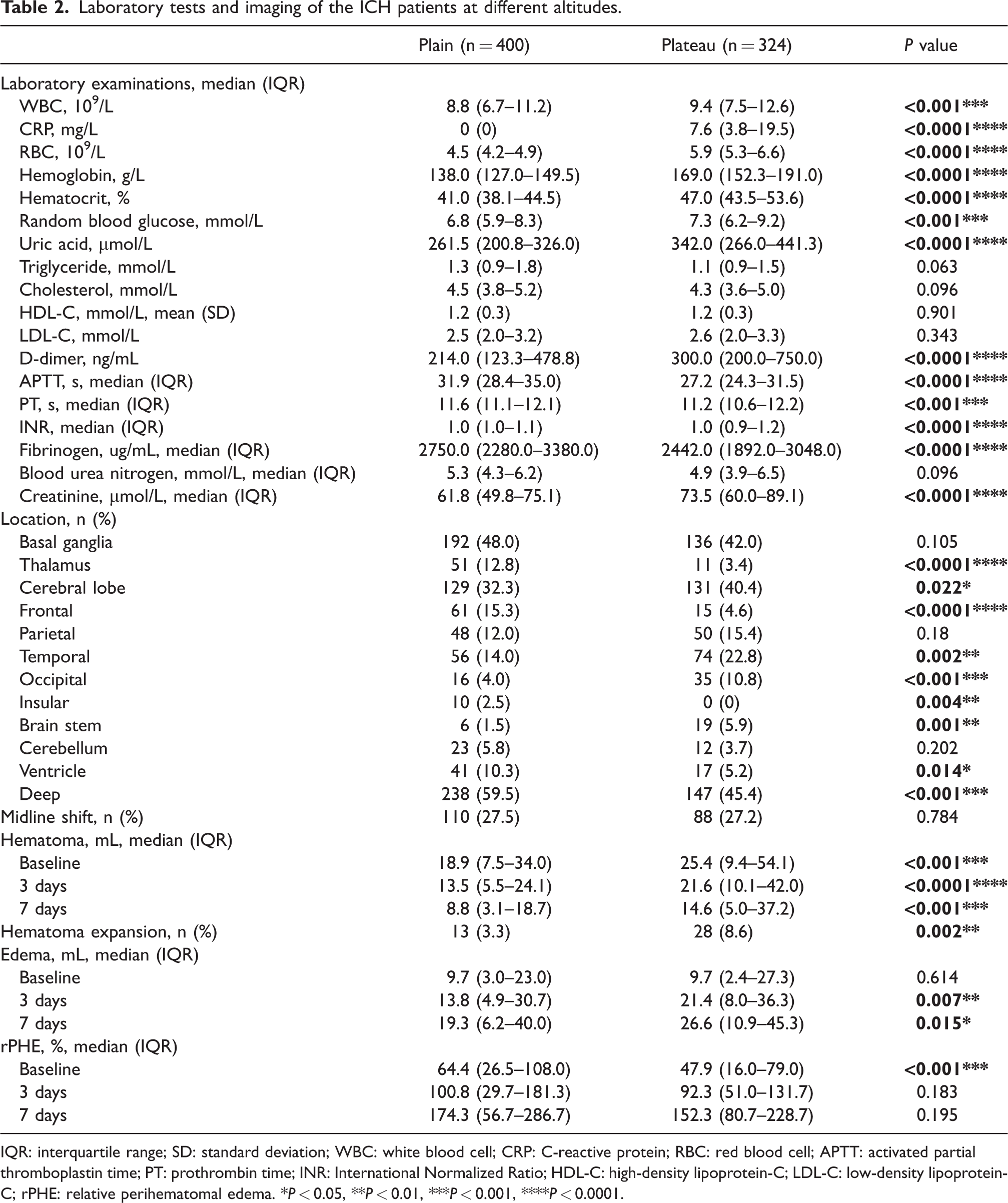
IQR: interquartile range; SD: standard deviation; WBC: white blood cell; CRP: C-reactive protein; RBC: red blood cell; APTT: activated partial thromboplastin time; PT: prothrombin time; INR: International Normalized Ratio; HDL-C: high-density lipoprotein-C; LDL-C: low-density lipoprotein-C; rPHE: relative perihematomal edema. *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001.
The imaging characteristics of ICH at different altitudes were different, with higher frequency of hemorrhage in cerebral lobes, and larger volumes of hematoma and perihematomal edema for patients at high altitude (Table 2). The hematoma volumes of patients in the plain were significantly smaller at baseline (18.9 [IQR: 7.5–34.0] mL vs. 25.4 [IQR: 9.4–54.1] mL, P < 0.001), 3 days (13.5 [IQR: 5.5–24.1] mL vs. 21.6 [IQR: 10.1–42.0] mL, P < 0.0001) and 7 days (8.8 [IQR: 3.1–18.7] mL vs. 14.6 [IQR: 5.0–37.2] mL, P < 0.001), with less frequent hematoma expansion (3.3% vs. 8.6%, P = 0.002) when compared to those resided at high altitude. The volumes of perihematomal edema of the lowlanders were also smaller at 3 days (13.8 [IQR: 4.9–30.7] mL vs. 21.4 [IQR: 8.0–36.3] mL, P = 0.007) and 7 days (19.3 [IQR: 6.2–40.0] mL vs. 26.6 [IQR: 10.9–45.3] mL, P = 0.015). However, baseline rPHE of lowlanders was larger than that of highlanders (64.4 [IQR: 26.5–108.0] % vs. 47.9 [IQR: 16.0–79.0] %, P < 0.001), though no statistical significance was observed between the two groups at 3 days and 7 days. No significance was observed in midline shift between the two groups as well.
Complications and short-term outcomes
The outcomes of ICH patients at different altitudes are shown in Table 3. The short-term functional outcome of patients in the plateau was worse than that in the plain, with higher NIHSS (8.0 [IQR: 3.0–14.8] vs. 4.0 [IQR: 0.0–9.0], P < 0.0001) and mRS scores (4 [IOR: 2–5] vs. 3 [IQR: 1–5], P < 0.0001). The mRS distribution at discharge is shown in Figure 1. A total of 238 patients (73.5%) in the plateau while only 206 patients (51.5%) in the plain required assistance (mRS 3–6) in daily life (P < 0.0001). The in-hospital mortality of patients at high altitude was also significantly higher than that at sea level (9.9% vs. 2.0%, P < 0.0001). In addition, there were significant differences in the incidence of gastrointestinal hemorrhage between the two groups (plateau: 5.2% vs. plain: 0.5%, P < 0.0001). No significance was observed in the occurrence of pulmonary infection and heart/kidney adverse events between the two groups.
Complications and short-term functional outcomes of ICH patients at different altitudes.
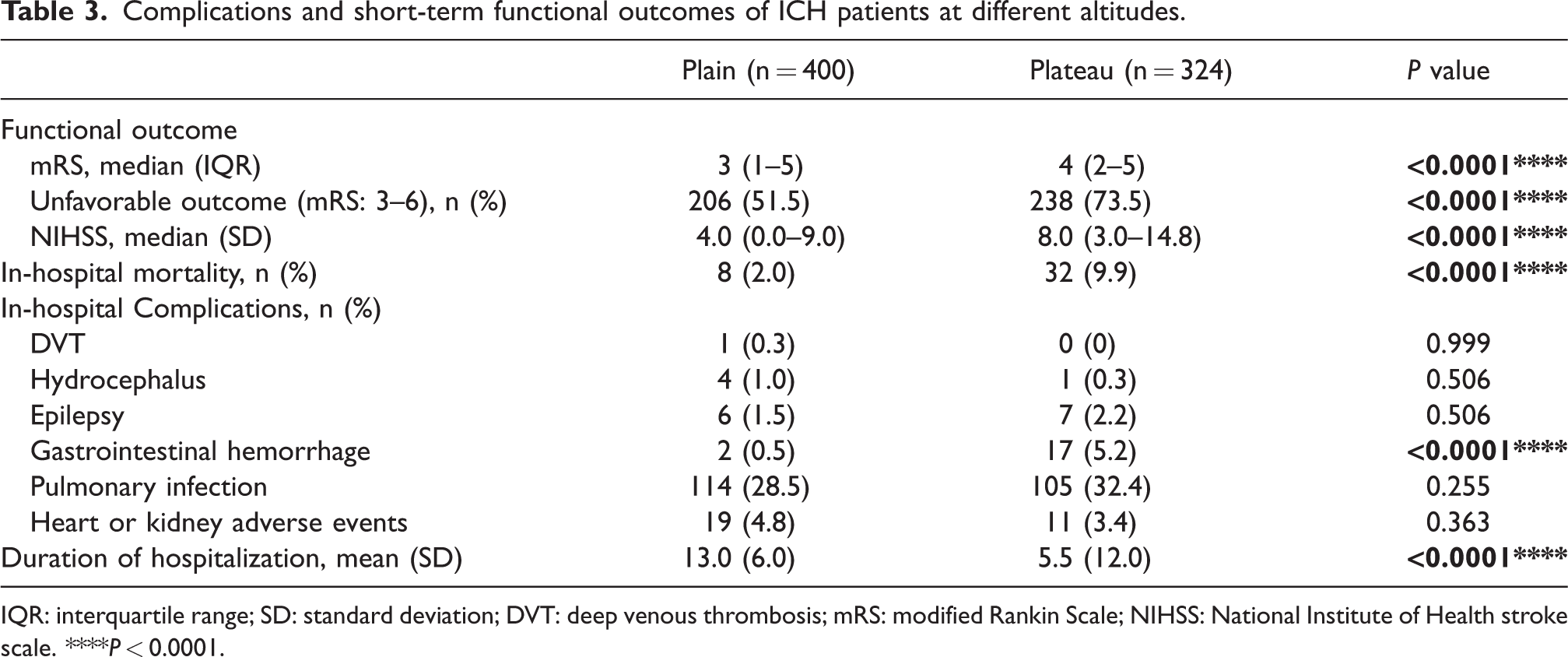
IQR: interquartile range; SD: standard deviation; DVT: deep venous thrombosis; mRS: modified Rankin Scale; NIHSS: National Institute of Health stroke scale. ****P < 0.0001.
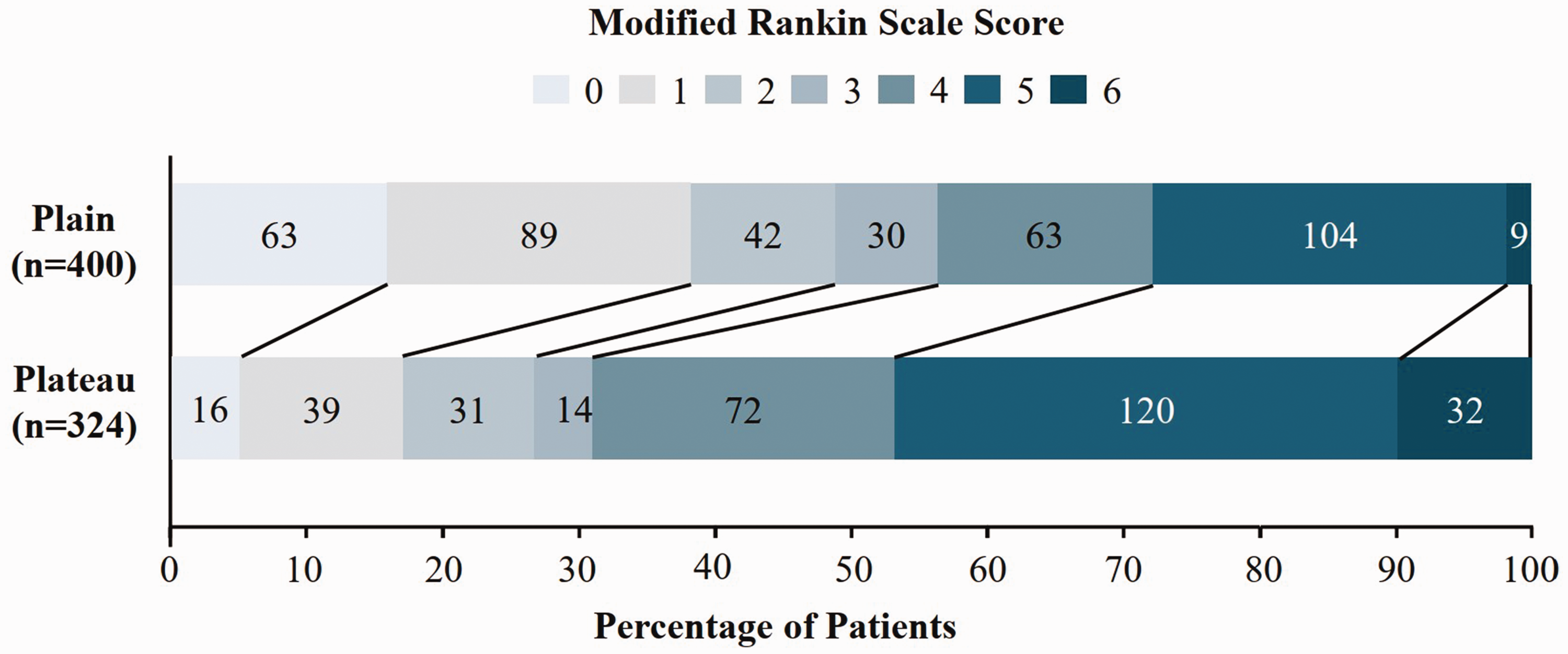
Distribution of modified Rankin Scale at discharge in each group.
Subgroup analysis
The results of subgroup analysis of baseline characteristics of Han ICH patients from the different altitudes are shown in Table S1. The median age of Han patients from the plateau was 52.0 (IQR: 46.5–57.5) years old, which was much younger than that from the plain (P < 0.0001). Compared to male in the plain, those resided at high altitude were at higher risk of ICH (P = 0.043). The level of DBP of ICH patients in the plain was lower than that in the plateau (93.0 [IQR: 84.0–103.3] mmHg vs. 102.0 [IQR: 93.0–116.0] mmHg, P < 0.001), though no significance was observed in the level of SBP between the two groups. The admission time of Han patients in the plateau was much shorter than that in the plain (5.0 [IQR: 2.0–24.0] hours vs. 12.0 [IQR: 4.0–48.0] hours, P = 0.024). Consistent with overall results, Han patients in the plateau suffered from higher NIHSS scores (11.0 [IQR: 4.0–35.0] vs. 7.0 [IQR: 2.0–13.8], P = 0.018), with more severe ICH ones (11 [37.9%] vs. 85 [21.3%], P = 0.037) than lowlanders.
The subgroup analysis results of laboratory examinations and imaging features of Han patients from different altitudes are shown in Table S2. In line with overall results, Han patients in the plateau had higher level of RBC, hemoglobin, hematocrit and CRP than those in the plain (P < 0.0001). Han patients in the plateau showed higher frequency of hemorrhage in brain stem, while lower in cerebral lobe, when compared to those in the plain. However, baseline volume of perihematomal edema and rPHE of Han patients at high altitude were smaller than those in the plain. No significant difference was observed in other neuroimages due to the small sample size in the plateau.
The results of short-term functional outcome and complications are shown in Table S3. The functional prognosis of Han patients in the plateau was worse than that in the plain, with higher NIHSS (8.5 [IQR: 3.0–12.8] vs. 4.0 [IQR: 0.0–9.0], P = 0.014) and mRS scores (5.0 [IQR: 2.0–5.0] vs. 3.0 [IQR: 1.0–5.0], P < 0.001). A total of 72.4% Han patients in the plateau while only 51.5% in the plain were disabled at discharge (P = 0.029). Consistently, the in-hospital mortality and gastrointestinal hemorrhage incidence of Han patients at high altitude was also significantly higher than that at sea level. No significant difference was observed in other adverse events between the two groups.
High altitude associated with worse initial severity
The univariable logistic regression showed that high altitude was associated with the initial severity of ICH (OR [95% CI], 1.54 [1.10–2.16], P = 0.013). Besides, age, sex, polycythemia, level of SBP, concentration of WBC, CRP, random blood glucose, uric acid, hemorrhagic location, baseline volume of hematoma and perihematomal edema also associated with the initial severity of ICH (Table S4). However, no statistical significance was observed between high altitude and initial severity of ICH after adjustion for the above factors (adjusted OR [95% CI], 0.72 [0.35–1.50], P = 0.379) (Table 4).
Logistic regression for relationship between high altitude and the initial severity or outcome of ICH.
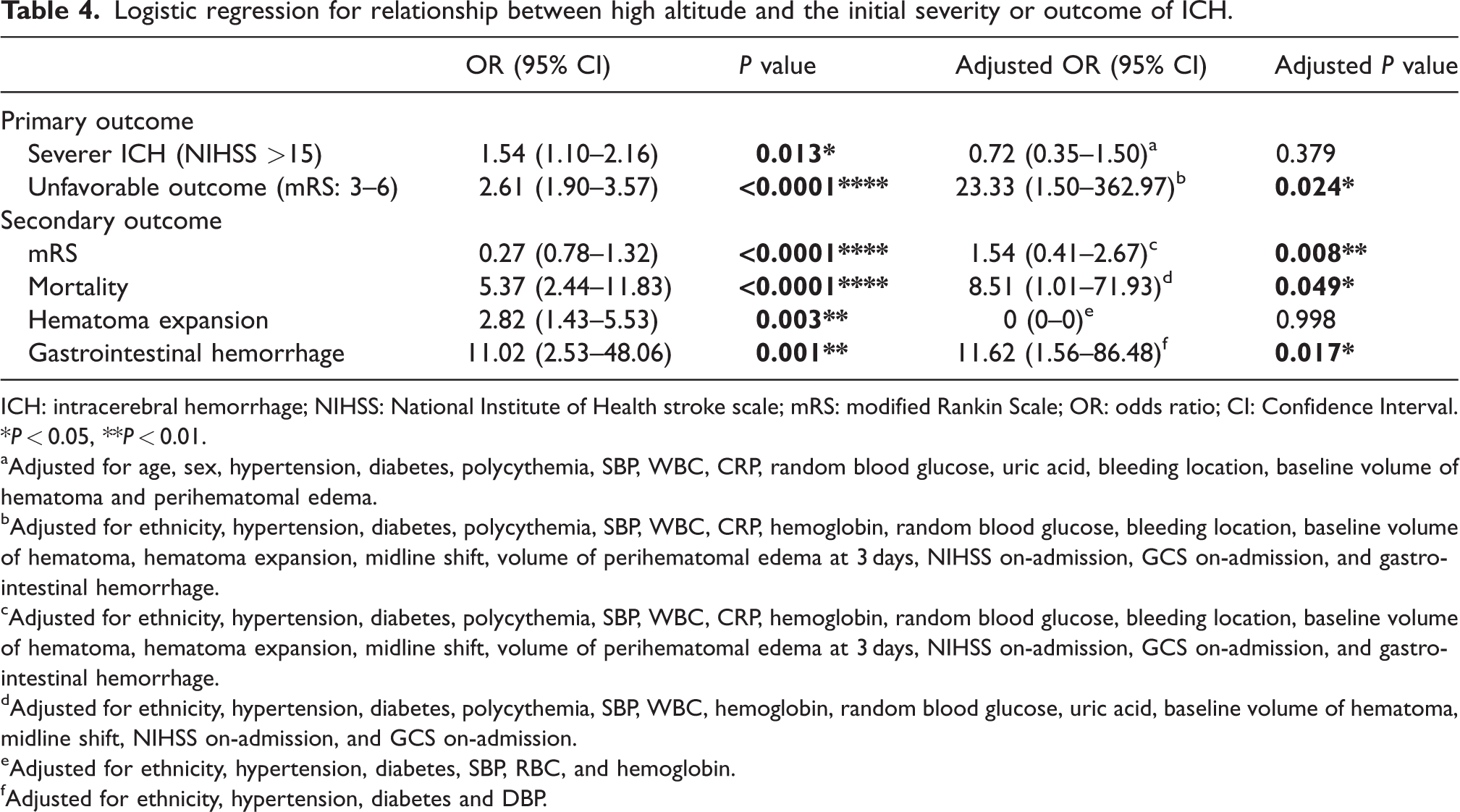
ICH: intracerebral hemorrhage; NIHSS: National Institute of Health stroke scale; mRS: modified Rankin Scale; OR: odds ratio; CI: Confidence Interval. *P < 0.05, **P < 0.01.
Adjusted for age, sex, hypertension, diabetes, polycythemia, SBP, WBC, CRP, random blood glucose, uric acid, bleeding location, baseline volume of hematoma and perihematomal edema.
Adjusted for ethnicity, hypertension, diabetes, polycythemia, SBP, WBC, CRP, hemoglobin, random blood glucose, bleeding location, baseline volume of hematoma, hematoma expansion, midline shift, volume of perihematomal edema at 3 days, NIHSS on-admission, GCS on-admission, and gastrointestinal hemorrhage.
Adjusted for ethnicity, hypertension, diabetes, polycythemia, SBP, WBC, CRP, hemoglobin, random blood glucose, bleeding location, baseline volume of hematoma, hematoma expansion, midline shift, volume of perihematomal edema at 3 days, NIHSS on-admission, GCS on-admission, and gastrointestinal hemorrhage.
Adjusted for ethnicity, hypertension, diabetes, polycythemia, SBP, WBC, hemoglobin, random blood glucose, uric acid, baseline volume of hematoma, midline shift, NIHSS on-admission, and GCS on-admission.
Adjusted for ethnicity, hypertension, diabetes, SBP, RBC, and hemoglobin.
Adjusted for ethnicity, hypertension, diabetes and DBP.
High altitude associated with unfavorable short-term outcome
The univariable logistic regression showed that high altitude (OR [95% CI], 2.61 [1.90–3.57], P < 0.0001), ethnicity, diabetes, level of WBC, CRP, RBC, hemoglobin, hematocrit, random blood glucose, SBP and DBP, hemorrhagic location, baseline volume of hematoma, hematoma expansion, midline shift, volumes of perihematomal edema (baseline, 3 days and 7 days), NIHSS and GCS at admission, and gastrointestinal hemorrhage were associated with unfavorable functional outcome (mRS ≥ 3, Table S2). After adjustion for confounding factors mentioned above, the multivariable logistic regression model showed that high altitude has a critical negative role on the short-term functional outcome of ICH (adjusted OR [95% CI], 23.33 [1.50–362.97], P = 0.024) (Table S5). Consistently, the univariable linear regression model showed that high altitude (β [95% CI], 0.27 [0.78–1.32], P < 0.0001), ethnicity, dyslipidemia, diabetes, polycythemia, level of WBC, CRP, RBC, hemoglobin, hematocrit, random blood glucose, uric acid, SBP and DBP, hemorrhagic location, baseline volume of hematoma, hematoma expansion, midline shift, volume of perihematomal edema at baseline and 3 days, NIHSS and GCS at admission, and gastrointestinal hemorrhage were associated with functional outcome. Furthermore, high altitude positively related to mRS (adjusted β [95% CI], 1.54 [0.41–2.67], P = 0.008) after adjusting for confounding factors (Table S6).
High altitude (OR [95% CI], 5.37 [2.44–11.83], P < 0.0001), ethnicity, polycythemia, level of WBC, RBC, hemoglobin, hematocrit, random blood glucose, uric acid and SBP, baseline volume of hematoma, midline shift, baseline volume of perihematomal edema, NIHSS and GCS at admission were associated with in-hospital mortality. High altitude also related to in-hospital mortality after adjustion for the associated covariables (adjusted OR [95% CI], 8.51 [1.01–71.93], P = 0.049) (Table S7).
The univariable logistic regression showed that high altitude (OR [95% CI], 2.82 [1.43–5.53], P = 0.003), ethnicity, level of RBC, hemoglobin, SBP and DBP were associated with hematoma expansion. However, no statistical significance was observed between high altitude and hematoma expansion after adjustion for the above factors (OR [95% CI], 0 [0–0], P = 0.998) (Table S8).
Moreover, high altitude (OR [95% CI], 11.02 [2.53–48.06], P = 0.001), ethnicity and level of DBP were associated with the incidence of in-hospital gastrointestinal hemorrhage (Table S9). After adjustion for the confounding factors, high altitude also independently related to the incidence of in-hospital gastrointestinal hemorrhage (adjusted OR [95% CI], 11.62 [1.56–86.48], P = 0.017).
Discussion
In this study, we found that residents in the plateau exhibited more severe initial manifestations, larger hematoma and perihematomal edema, and worse short-term outcome than those in the plain. Dependency at discharge, in-hospital mortality and gastrointestinal hemorrhage resulted from high altitude independently.
Consistent with previous studies, ICH patients showed more severe initial manifestations in the plateau than those in the plain, although high altitude was not an independent risk factor for the initial severity. This may be due to the aggravation of high altitude hypoxia on inflammation and larger baseline volume of hematoma. 21 Chronic high altitude hypoxia may induce pro-inflammatory microenvironment and immune hypersensitivity, 22 and augment existed inflammation mediated by ICH. 23 Besides, the increased level of uric acid of highlanders may be caused by increased urate generation and relatively impaired renal excretion secondary to chronic systemic hypoxia,24,25 and was thought to be an independent predictor of early neurological deterioration and death.26,27 Moreover, a larger volume of baseline hematoma and a higher incidence of brain stem involvement in highlanders may also contribute to the worse preliminary manifestations of ICH. 28
In this study, we found a higher incidence of ICH in cerebral lobes in highlanders than patients in the plain. This may affect the initial degree of severity. 29 One of the reasons for the high incidence of cerebral lobe hemorrhage in the highlanders is vascular amyloidosis. 30 An in vitro experiment demonstrated that chronic hypoxia can inhibit the metabolism of amyloid precursor protein in cerebral microvascular smooth muscle cells. 31 Another reason could be the small cerebral vascular disease. Microbleeds, white matter hyperintensities, and perivascular space enlargement were detected in the mice brain after chronic high altitude hypoxia exposure, resulting in amyloid protein disposition and neuroinflammation.32 –34 Moreover, hypertension, more prevalent and poorly controlled in highlanders, 35 may also increase the probability of vessel rupture in cerebral lobes by causing arteriolosclerosis in leptomeningeal and cortical vessels. 30
Consistent with previous studies, ICH patients in the plateau were found to exhibit worse outcomes and higher in-hospital mortality than those in the plain. Firstly, we revealed the independent role of high altitude on the unfavorable short-term functional outcome. Secondly, the more severe initial manifestations of highlanders also related with the worse prognosis in this study, resulting of the larger mass effect of hematoma and perihematomal edema in highlanders.36 –38 The declined rate of hematoma resolution in the plateau may aggravate the mass effect of ICH, due to the decreased phagocytosis of microglia/macrophages and meningeal lymphatic function in chronic inflammatory circumstances.39 –42 Furthermore, the larger volume of perihematomal edema may also induce the more serious blood-brain-barrier impairment,43,44 erythrocyte rupture and iron release 45 due to intensive inflammation and chronic hypoxia. Thirdly, the much higher level of SBP also resulted in an unfavorable outcome directly, 46 though no independent negative effect was observed in the initial severity. Fourthly, hematoma expansion may also contribute to the poor functional outcome significantly,47,48 which may be associated with the acute hypertensive response, blood pressure variability and inflammation.49,50 Finally, in line with previous research, ethnicity influenced the outcome of on ICH.51,52 The implications of ethnicity encompass various factors, including genetic polymorphisms, 53 differences in healthcare processes 54 and variations in health insurance coverage. 55 The prognostic effect of hemorrhagic locations is controversial.47,56 –58 In our study, lobar ICH acted as a positive role in short-term functional outcome, which needs further exploration.
In this study, we found high altitude and baseline hematoma volume were independently associated with in-hospital mortality. This may be due to activated inflammation and cerebral hernia induced by large volume of hematoma. 22 In addition, we also found that high altitude was independently associated with higher incidence of gastrointestinal hemorrhage after ICH. This may be due to vagal hyperactivity and gastric acid hypersecretion induced by serious inflammation and intracranial pressure. 59
There are some limitations in this retrospective study. First, smoking and drinking have been associated with hematoma growth and worse clinical outcomes, including increased mortality rates.60,61 However, the alcohol and tobacco use data of patients at high latitude was absent, we only exhibited those in the plain. In the future, we will conduct prospective studies to compare the consumption of alcohol and tobacco among ICH patients in different altitudes, and further explore the effect of altitude on the severity and prognosis of ICH after adjustion for smoking and drinking. Second, examinations related to the etiology of ICH were not conducted and explored in this study. Therefore, rigorous prospective studies should be carried out in the future to clarify the risk factors for etiology and prognosis of ICH at different altitudes and to further investigate more accurate prevention and treatment. Third, the volume of perihematomal edema at 7 days was not included in multivariate analysis due to limited data. The results of the difference of rPHE between two groups was inconsistent with that of the volume of perihematomal edema. The volume of perihematomal edema demonstrated a stronger association with hematoma surface area rather than hematoma volume, such as shape and distribution. 62 Therefore, further studies are needed to explore the impact of altitude on perihematomal edema, including volume of perihematomal edema, rPHE, and rate of perihematomal edema. Finally, in the overall comparison, we mixed the effect of altitude and ethnicity. While in the subgroup analysis of this study, the sample size of Han patients at high altitude was relatively small. Therefore, large observational studies are needed in the future to clarify the impact of high altitude and ethnicity on the severity and outcome of ICH.
Conclusion
In China, ICH patients in the plateau suffered from more serious initial manifestations and worse short-term functional outcome than those in the plain. High altitude was independently associated with hematoma expansion and unfavorable outcome. Hypertension, inflammation, and vascular lesions resulted from high altitude hypoxia may be the critical reasons. Oxygen supplementation, blood pressure regulation, inhibition of inflammation and prevention of complications are important for ICH patients at high altitude.
Supplemental Material
sj-pdf-1-jcb-10.1177_0271678X231201088 - Supplemental material for More severe initial manifestations and worse short-term functional outcome of intracerebral hemorrhage in the plateau than in the plain
Supplemental material, sj-pdf-1-jcb-10.1177_0271678X231201088 for More severe initial manifestations and worse short-term functional outcome of intracerebral hemorrhage in the plateau than in the plain by Xiaoyin Wang, Haochen Sun, Xian Wang, Jing Lan, Yong Guo, Weiguo Liu, Lili Cui and Xunming Ji in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Project No. 82027802, 81620108011, 82001258 and 82101389).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
XMJ, LLC and WGL designed and supervised the study. XW, YG and JL collected the data. XYW and HCS drafted and finalized the manuscript. LLC edited the manuscript. All authors read and approved the final manuscript.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.