
Abstract
Neuroendovascular procedures have led to breakthroughs in the treatment of ischemic stroke, intracranial aneurysms, and intracranial arteriovenous malformations. Due to these substantial successes, there is continuous development of novel and refined therapeutic approaches. Large animal models feature various conceptual advantages in translational research, which makes them appealing for the development of novel endovascular treatments. However, the availability and role of large animal models have not been systematically described so far. Based on comprehensive research in two databases, this systematic review describes current large animal models in neuroendovascular research including their primary use. It may therefore serve as a compact compendium for researchers entering the field or looking for opportunities to refine study concepts. It also describes particular applications for ischemic stroke and aneurysm therapy, as well as for the treatment of arteriovenous malformations. It focuses on most promising study designs and readout parameters, as well as on important pitfalls in endovascular translational research including ways to circumvent them.
Introduction
Neuroendovascular techniques are safe and effective for the treatment of acute ischemic stroke.1–3 Recently, these techniques proved to be effective even in an extended time window for selected patient populations,4,5 thereby substantially changing stroke treatment and research. 6 Moreover, recent technical advancements such as flow-diverting stents, intra-aneurysmal flow-diversion, and new liquid-embolic agents have widened opportunities for endovascular treatment of cerebral aneurysms and intracranial vascular malformations (AVMs). 7
However, preclinical research on endovascular technologies is more challenging as compared to conventional treatment opportunities. Rodent models offer numerous advantages such as wide-spread implementation, reproducibility, a broad spectrum of readout parameters and experimental imaging techniques, as well as the availability of transgenic animals.8,9 On the other hand, rodent models only allow to investigate basic aspects of neuroendovascular treatments due to size limitations and significant differences in brain and cerebrovascular anatomy. 10
Large animal models are available for preclinical neuroendovascular research and offer numerous advantages including larger vessel sizes, compatibility with clinical magnetic resonance imaging (MRI), 11 computed (CT) 12 or positron emission tomography (PET), 13 and a gyrencephalic brain with a gray-to-white-matter-ratio approximating that of humans. 14 Despite minor anatomical differences in some species, cerebral blood supply and cerebrovascular architecture are very similar to the human situation. 15 Large animal models are also feasible for long-term studies and extensive physiological monitoring. Behavioral tests for the assessment of functional outcomes are available, while international expert committees recommend confirmative research in large animal models prior to early stage clinical investigations.16,17 However, large animal models are not utilized widely yet, potentially due to special maintenance requirements, the necessity of for interdisciplinary research teams as well as profound knowledge on how to successfully employ these models, as well as some species-dependent anatomical differences to humans.9,10
Here, we review existing large animal models and their use in neuroendovascular research on stroke, aneurysms and AVMs. We also provide recommendations on most feasible study designs and readout strategies in order to capitalize on the advantages of large animal models while avoiding potential limitations.
Methodological approach
We conducted a systematic literature search for relevant publications according to the PRISMA guidelines. We accessed indexed and non-indexed Medline databases via Ovid search interface from Wolters Kluwer and Science Citation Index Expanded via Web of Science from Clarivate Analytics (Figure 1(a)). The Medline search strategy included 23 search steps of terms for the topic large animals and 37 search steps of terms for the topic cerebrovascular intervention. The databases were searched from 1990 up to the update status of the databases on November 24th 2017 (search date).
Study data. (a) PRISMA flow chart of selection process; systematic research in Medline and Web of Science databases, inclusion of studies that address neurointerventional research, test endovascular techniques and were performed in large animals (b) Study numbers show a continuous increase from 1990 until 2005, followed by a slight decline and a recent increase to all-time highs.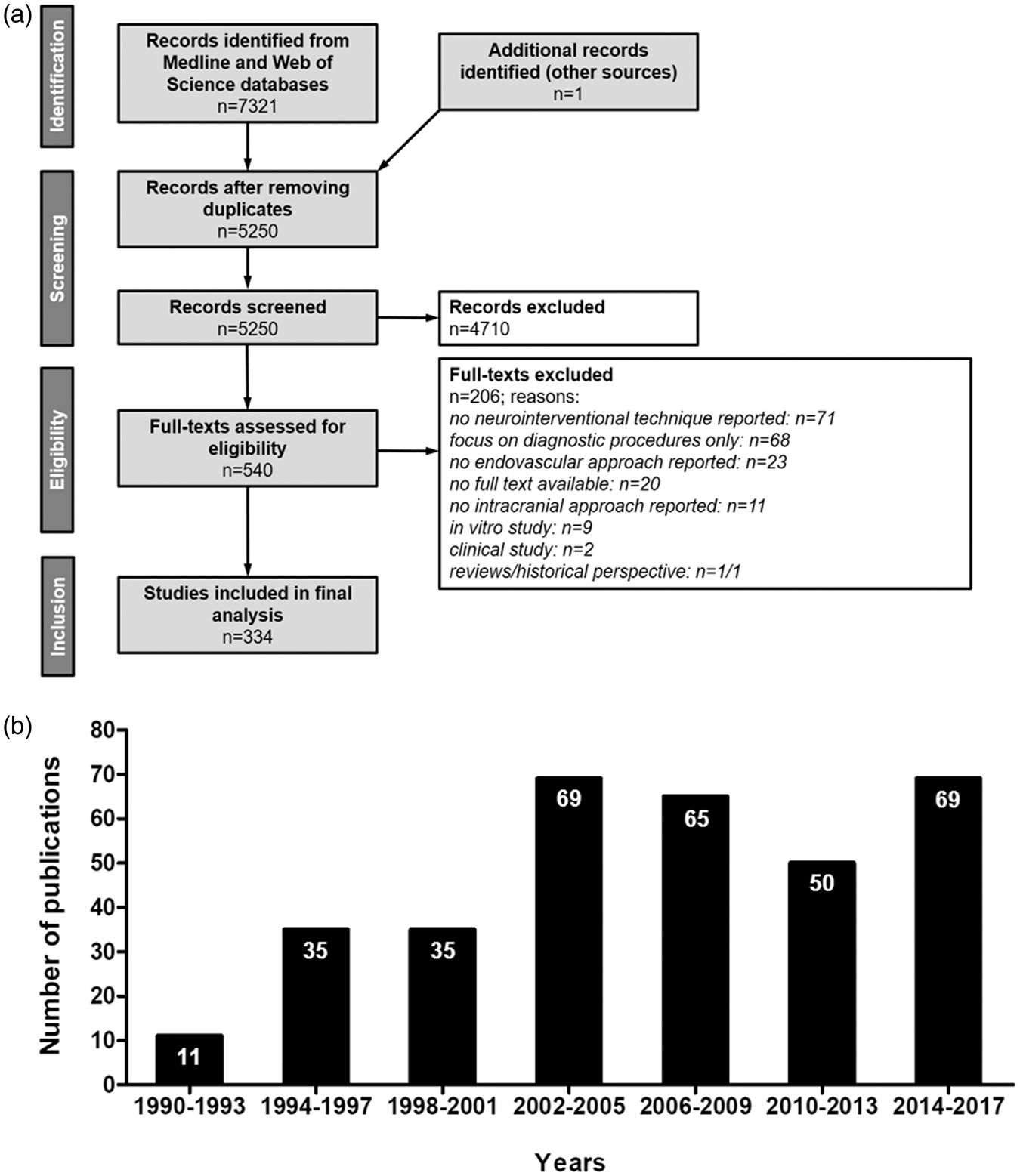
Search strategies combined the aspects “large animals” and “neurological intervention” with AND. We also used keywords with synonyms and, if available, controlled vocabulary terms for Medline (for detailed search strategies, please see Supplementary Tables 1 and 2). Only articles published in English were included.
Additionally, we searched for large animal models that were developed to represent the vascular anatomy of humans as well as human neurovascular disorders. Studies utilizing extracranial vessels to simulate intracranial interventions and/or to establish a neurointerventional model were included, but discriminated from studies describing a neurointerventional procedure in the cerebrovasculature. Additionally, reference lists from identified papers of interest were screened to find other potentially relevant publications.
We further analyzed the application of these models in neurointerventional research focusing on endovascular approaches. Studies that (i) addressed neurointerventional research, (ii) tested endovascular techniques, and (iii) were performed in large animals were assessed.
We excluded articles due to the following criteria: no full text available (n = 20), focus on diagnostic procedures only (n = 68), no neurointerventional technique reported (n = 71), no endovascular approach (n = 23), clinical study (n = 2), review/historical perspective (n = 1/1), in vitro study (n = 9), and studies focusing on interventions in the peripheral circulation without modelling the cerebrovasculature (not intracranial, n = 11) (Figure 1(a)).
Results
Data set
We identified 5250 articles after removal of search result duplicates. From those, 4710 abstracts did not meet the inclusion criteria and were excluded. The full text of the remaining 540 articles was assessed, and data were finally extracted from 334 papers (Figure 1(a)).
For model description, 56 different large animal models using intracranial vessels were identified through full text assessment, and additional 18 models were derived by checking the reference lists of these papers. Moreover, we identified 26 models using extracranial vessels. One paper was excluded during the full text assessment due to an unclear methodological approach.
The number of publications reporting large animal trials in neurointerventional research continuously increased from the 1990s until 2005 (Figure 1(b)). The numbers of publications slightly declined thereafter, but increased from 2014 reaching all-time highs. This is potentially due to the recent breakthroughs in the neurointerventional field, prompting many academic and industry groups to intensify translational research on novel techniques and products.
Species and models
Large animal models for aneurysm, AVM, ischemic stroke, carotid siphon including models using extracranial vessels.
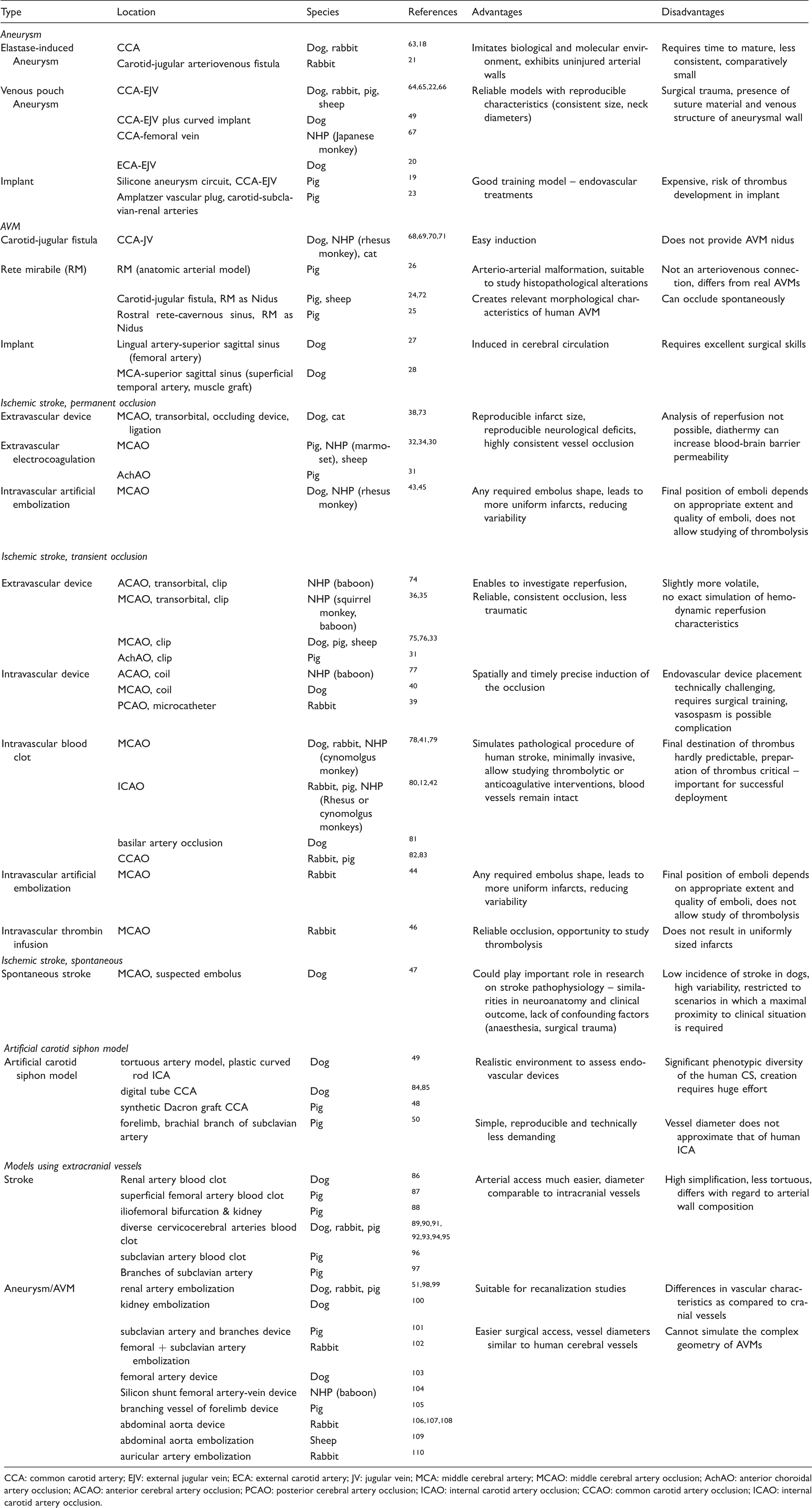
CCA: common carotid artery; EJV: external jugular vein; ECA: external carotid artery; JV: jugular vein; MCA: middle cerebral artery; MCAO: middle cerebral artery occlusion; AchAO: anterior choroidal artery occlusion; ACAO: anterior cerebral artery occlusion; PCAO: posterior cerebral artery occlusion; ICAO: internal carotid artery occlusion; CCAO: common carotid artery occlusion; ICAO: internal carotid artery occlusion.
Aneurysm models
Three different ways to induce an aneurysm in large animals are described (Figure 2(a)): elastase-induced aneurysms, venous pouch aneurysms, and use of artificial implants. Elastase-induced aneurysms imitate the biological and molecular environment of naturally occurring aneurysms and exhibit uninjured arterial walls.
18
On the other hand, they require time to mature,
19
are less reproducible in appearance,
20
, and comparatively small.
21
Aneurysms created by venous pouches are commonly used, reliable aneurysm models
22
with reproducible characteristics such as consistent aneurysm size and neck diameters. Disadvantages are the surgical trauma required for induction, at least transient presence of suture threads, and the venous structure of the aneurysmal wall.
20
Aneurysms emerging from artificial implants provide good training opportunities for endovascular treatments such as coiling,
19
but are expensive
23
and come at the risk of thrombus formation within the implant. Hybrid models connecting an artificial vascular tree with multiple aneurysms to an animal’s circulation are also available for neurointerventional training purpose.
19
Illustration of the different techniques for model induction and utilization of clinical imaging procedures. (a) There are three different ways to induce an aneurysm model: elastase-induced aneurysms (aneurysm develops in a closed vessel by elastase infusion), venous pouches aneurysms (preparation of a venous pouch and suturing to artery, usually CCA) and use of artificial implants. Abbreviations: CCA: common carotid artery. (b) AVM models can be created by a carotid-jugular fistula (shunt between CCA and JV), use of RM in pigs and sheep, and use of autologous implants. Abbreviations: JV: jugular vein; ECA: external carotid artery. (c) Ischemic stroke models are based on transient or permanent occlusion of cerebral arteries. Extravascular and intravascular occlusion methods can be discriminated. Extravascular occlusion comprises electrocoagulation and the use of ligation, or occluding devices such as aneurysm clips. Intravascular occlusion can be induced by intravascular devices, such as aneurysm coils, blood clots, thrombin infusion or artificial emboli. (d) A major advantage of large animal models is the compatibility with clinical imaging technologies. Sample images were taken in a sheep after transient MCAO by a surgical clip (3-h occlusion time). Abbreviations: MTT: mean transit time; DWI: diffusion-weighted imaging; T2w: T2-weighted imaging. False color scale indicates MTTS from 0 (purple) to 10 s (red). All images were taken on standard clinical scanner during an in-house study (data not published).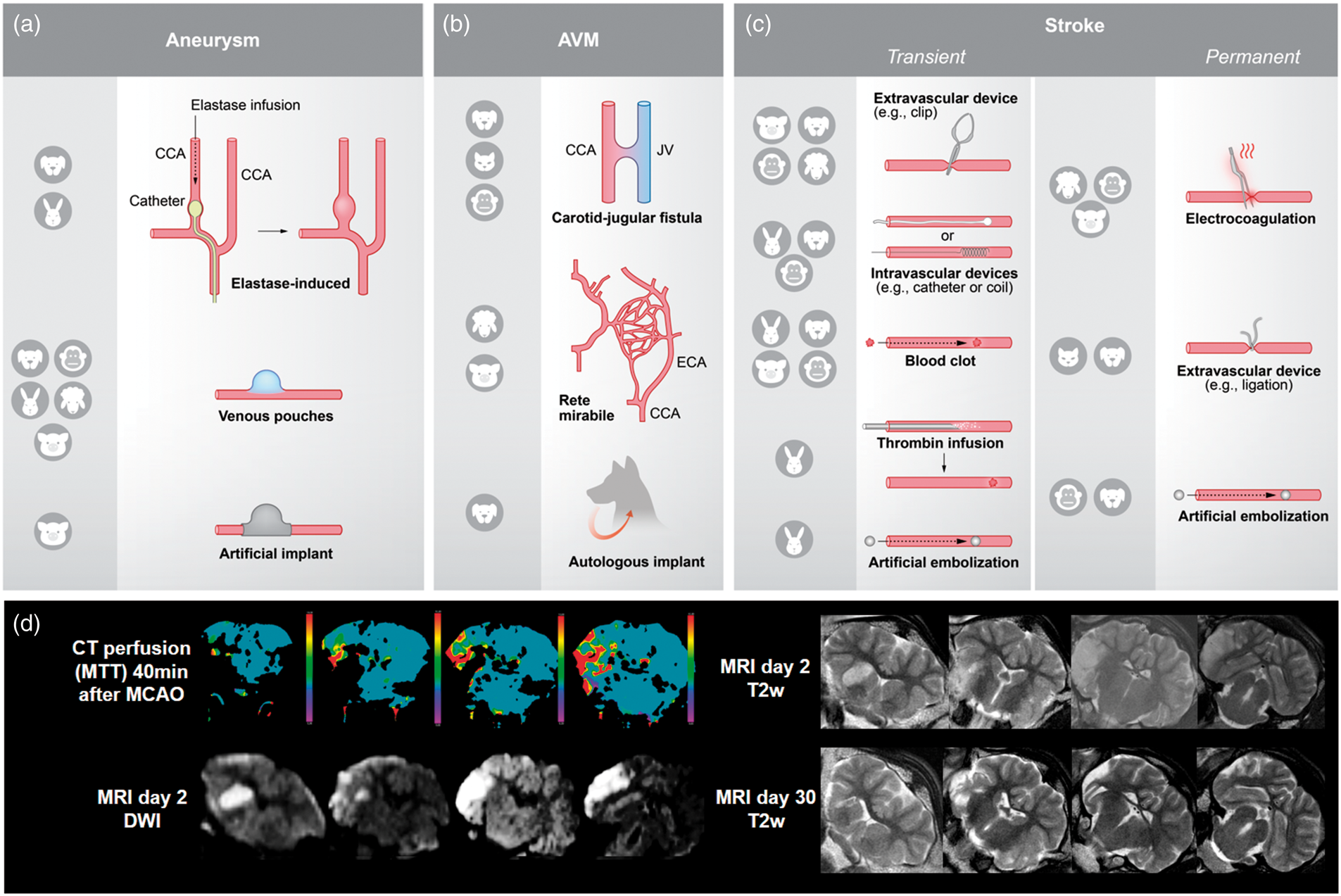
In the analyzed literature, therapies were tested immediately after aneurysm induction (30.4%, 68/224) or after a maturation time of up to two weeks (17.9%, 40/224), up to four weeks (38.4%, 86/224), up to eight weeks (4.4%, 10/224), or after more than eight weeks of maturation (1.3%, 3/224). Some studies (7.6%, 17/224) did not mention aneurysm maturation time.
Models of arterio-venous malformations
AVM models can be created by a carotid-jugular fistula, by using species exhibiting rete mirabile (RM), or by using autologous implants (Figure 2(b)). Carotid-jugular fistulas can be induced easily, but do not provide an AVM nidus. 24 The RM in pigs and sheep can be used alternatively. The RM is the branching of the maxillary artery into a network of fine arteries, which then reunite to the internal carotid artery. Although not an arteriovenous connection, 25 the RM is an often utilized natural AVM model and suitable to study post-interventional histopathological alterations. 26 Artificial arteriovenous shunts utilizing the RM as the AVM nidus provide relevant morphological characteristics of human AVM, such as feeding artery, interposed nidus, and draining vein. 24 However, they are prone to the risk of spontaneous occlusion. 25 Further, AVMs can be induced by an autologous implant in the cerebral circulation, such as an artery or a muscle graft with related artery. This procedure has immediate effects on cerebral circulation and provides a good simulation of pathophysiological conditions observed clinically.27,28 However, excellent surgical skills are required to consistently create such AVM models. 29
Therapy in AVM models is mainly tested immediately after AVM induction (72.7%, 24/33) or in some cases after a maturation time up to four weeks (18.2%, 6/33), and in rare cases even beyond that time (9.1%, 3/33).
Ischemic stroke models
Stroke models are based on permanent or transient occlusion of cerebral arteries (Figure 2(c)), mainly the middle cerebral artery (MCA). Permanent occlusions models result in reproducible functional outcome and lesion size30,31 but do not allow analysis of reperfusion. 32 Transient occlusion models tend to produce more volatile results, but enable to investigate reperfusion. 33
Stroke induction can be discriminated into extravascular and intravascular occlusion methods. Extravascular occlusion involves neurosurgical access to the target vessel followed by ligation, electrocoagulation or occluding devices (e.g. aneurysm clips). Electrocoagulation is relatively easy to perform, leads to reproducible neurological deficits, 34 and highly consistent vessel occlusion. However, diathermy can increase blood–brain barrier permeability. 32 Vessel occlusion using clips or by ligation induces a reliable and consistent occlusion, which is less traumatic. 35 Transient vessel occlusion allows studying reperfusion effects, but hemodynamic characteristics are different from those seen in reperfusion. 10 Moreover, clip and thread handling can be challenging 36 and requires appropriate experimenter training. Extravascular occlusion needs transorbital access (mainly for the anterior or middle cerebral arteries 37 ) or craniectomy (all major arteries accessible). Transorbital access only requires a small craniotomy in the orbita, and manipulation of surrounding tissue is minimized. 38 Disadvantages of this approach are eye loss and related postoperative complications, including abnormal behavior caused by vision defects. 32 Craniotomy results in a larger wound and is technically more demanding, but preserves the eye. Craniotomy is avoided when using intravascular occlusion models.
Intravascular occlusion requires endovascular access to the target vessel. It is induced by devices such as coils, blood clots, artificial emboli, or thrombin infusion. Intravascular devices such as coils or catheters enable a spatially and temporally precise stroke induction, 39 but endovascular device placement is technically challenging and requires intensive training to generate reproducible results. Moreover, vasospasm is a possible complication, 40 effecting many relevant outcome parameters. Using blood clots for vessel occlusion perfectly simulates the pathological mechanism of human stroke, is minimally invasive, and allows studying thrombolytic or anticoagulative interventions. 41 Another advantage is that blood vessels remain physically undamaged after thrombus deposition. 42 The major disadvantage is that the occlusion site is hardly predictable, making the outcome highly heterogeneous. Another critical factor is preparation of the thrombus, which critically influences its characteristics. 41 Artificial emboli made of silicone rubber or silicone-coated filaments provide a standardized but artificial alternative. These emboli could be of any required shape, 43 helping to define occlusion site and thereby leading to more uniform infarcts. This reduces variability,44,45 but studying recanalization is not possible. Endovascular approaches are not applicable for species exhibiting an RM.30,32 Another possibility to produce a vessel occlusion also beyond the RM is thrombin infusion and subsequent thrombus formation. This method provides reliable occlusion and the opportunity to study recanalization, but induced infarcts are heterogeneous in size. 46
Spontaneous stroke occurrence is reported in dogs and might play an important role in the investigation of stroke pathophysiology. There are no experimental confounding factors such as anesthesia or surgical trauma. 47 However, the low incidence of stroke in dogs, along with a high variability, restricts this model to scenarios in which a maximal proximity to the clinical situation is required in spite of inter-subject variability.
Carotid siphon models
The human carotid siphon (CS) has unique anatomical bends which remain critical structures for endovascular catheter access to the intracranial vessels, in particular when using large-bore (5F or 6F) intermediate catheters for clot aspiration in acute stroke treatment or for facilitated navigation of flow-diverting stents in aneurysm therapy. In particular in elderly patients with increased CS tortuosity (Supplementary Figure 1), vascular access with these catheters may be impaired. On the other hand, too forceful manipulation during catheterization attempts may result into complications such as endothelial injury with vasospasm, dissection, thrombosis or even vessel perforation. Thus, new designs for intermediate cranial access catheters require testing using vascular models of the CS to evaluate important parameters like steerability/torquability, lubricity, stiffness, and durability under realistic in vivo conditions. Surgical CS models are created by using different implants and offer a realistic environment including pulsating blood flow and vascular responses for the assessment of endovascular devices in terms of vascular navigation. 48 However, there is a significant diversity in human CS anatomy 49 and each model can only represent one particular formation. Moreover, surgical implantation and creation of these models are technically challenging and require a recovery period before device testing. Alternatively, the human CS anatomy can be easily modelled by maximally flexing the porcine forelimb. 50 This creates a brachial artery tortuosity, resulting in an anatomical vessel configuration similar to that of the human CS. This method is simple, reproducible, and technically less demanding, but vessel diameter does not approximate that of the human ICA. 50
Models using extracranial vessels
Animal modeling of large vessel occlusion exclusively in the extracranial circulation has informed the thrombectomy device design (Table 1), leading to efficient and effective technologies for treating stroke patients. For instance, research on thrombolysis and thrombectomy is sometimes performed on renal arteries, the superficial femoral artery, the iliofemoral bifurcation, the subclavian artery or its branches (mainly in pigs), and on different cervicocerebral arteries. The latter includes the lingual artery, maxillary artery, cervical arteries, external carotid artery (ECA), or ascending pharyngeal artery (APA). Aneurysm or AVM therapy is often simulated using renal arteries, which are suitable for recanalization studies. 51
Simple metrics such as the angiographic evidence of recanalization are used to assess device efficacy. Importantly, the trauma caused to the vessel wall can be studied as well as the consequence of distal 52 emboli to a downstream organ (e.g., renal artery vascular occlusion models 53 ). However, there are important limitations to these models that must be appreciated when interpreting the data. The first obvious point is that arteries of the brain have significant differences in structure, 54 mechanics 55 and function as compared to systemic arteries. Importantly, intradural arteries are not tethered or constrained in the perivascular environment. Additionally, the tortuosity of the human intracranial circulation is not seen in existing animal vascular occlusion models. It is for these reasons that an important complement to animal modeling includes in vitro vascular occlusion modeling in phantoms of patient-specific or population-based vascular replicas.56–61 This combined approach has led to the development and ultimate regulatory approval of highly effective thrombectomy devices such as stent-retrievers and aspiration catheters.
However, the lack of the target organ of interest, namely the brain, is a critical limitation for the next evolution in stroke care. 10 Perhaps the optimal treatment will involve pre-thrombectomy neuroprotection, 62 direct to angiosuite mechanical thrombectomy for emergent large vessel occlusions, catheter-based delivery of thrombolytics to treat shed microemboli or other agents to further limit/alter the course of neuronal injury. When considering such a complex treatment solution, the variables are further compounded when considering dose of each treatment or route of delivery.
Benefits and challenges of large animal models in neurointerventional research
Advantages of large animal models for neurointerventional research.
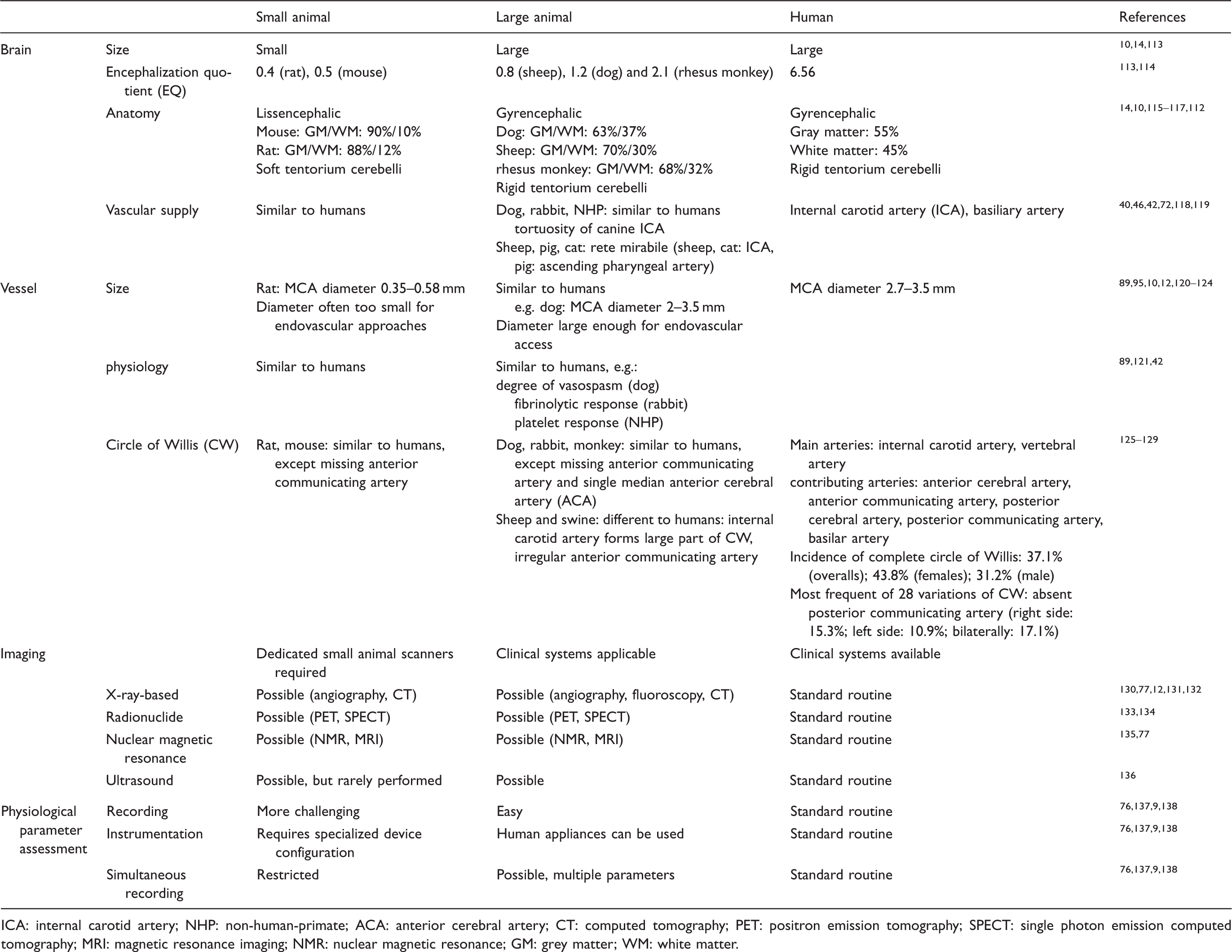
ICA: internal carotid artery; NHP: non-human-primate; ACA: anterior cerebral artery; CT: computed tomography; PET: positron emission tomography; SPECT: single photon emission computed tomography; MRI: magnetic resonance imaging; NMR: nuclear magnetic resonance; GM: grey matter; WM: white matter.
In contrast to the situation in rodents, large animal and human brain anatomy share many similarities. Large animal brains are mostly gyrencephalic and exhibit higher white matter content. This is important since white matter is more resilient to ischemia and therapeutic approaches targeting white matter are believed to have a wider therapeutic time window. 111 Moreover, white matter is important for higher brain function and plasticity. Another example is the comparatively rigid tentorium cerebelli in most large animal species, as compared to the soft structure in rodents. This plays a crucial role in the effects of edema and can aggravate consequences of intracerebral pressure 112 in humans and large animals alike. Moreover, large animals models can be used easily with clinical imaging equipment (Figure 2(d)).
Individual anatomical variations can impair model induction or the therapeutic approaches. Large animal strains are often outbred, increasing the likelihood of such variances. For instance, collateral vasculature or tortuous blood vessels as observed in pigs, 76 dogs, 75 and cats 139 can cause challenges in experimental interventions. Moreover, some species-specific anatomic prerequisites must be taken into consideration, the most prominent one being the RM.
Large animal experiments are often more complex than small animal studies. Training and pilot studies are therefore warranted to optimize the results of the main trial. The time and resource “loss” caused by such pilot experiments are often compensated by increased reliability and decreased variability in the main trial. This is of particular importance because large animal stroke models, such as the situation in human patients, tend to be more variable in outcome than their rodent counterparts. Pilot studies are also important to reveal at least basic information on effect sizes and thus required group/sample sizes in cases where small animal data are not available. This also helps to balance the number of required animals per group to maintain sufficient statistical power against ethical and financial constraints.
Pilot studies can further reveal whether model optimization can increase the amount or quality of information derived from the main experiment. In cases where an entirely new technical field is entered, pilot studies, together with consulting expert colleagues in large animal experimentation, help to select the appropriate large animal model.
Some genetically modified large animal strains exist and can be used to address special research questions. For instance, transgenic NHPs 140 or pigs 141 expressing green fluorescent protein have been reported. Transgenic large animal models are also available for other neurological disorders. 142
Types of interventions and therapies in the literature
Experimental aneurysm therapies were reported by two-third (67.0%; 224/334) of all studies, 19.5% (65/334) assessed stroke therapies, and 9.9% (33/334) AVM treatments. This is reasonable because aneurysm, stroke and AVMs are frequent and severe neurological disorders. Figure 3(a) to (c) provides detailed information on investigated approaches; 2.4% (8/334) of studies investigated conditions that were not defined in more detail; these included “intracranial lesions,” “abnormalities in central nervous system” or “brain injury” (referred to as “unspecified conditions” in Figure 3(c)); 1.2% (4/334) simulated carotid artery occlusive diseases.
Applied therapies in analyzed studies. (a) Aneurysms: main focus was on coils, stents and flow diverter stents (b) stroke: dominant therapy was mechanical thrombectomy, a recognized alternative to intravenous thrombolysis (c) AVMs: majority of studies investigated liquid embolic agents; unspecified conditions (e.g. “intracranial lesions,” “abnormalities in central nervous system” or “brain injury”): focus was on hypothermia and endovascular devices; carotid occlusive diseases: all studies investigated stents. Information about animals: (d) Number of animals: almost half of the studies used only up to 10 animals. (e) Occurrence of different species: most commonly used species were pigs and dogs, followed by rabbits (f) Animal characteristics: only a minority of studies reported all four items – strain, weight, sex and age.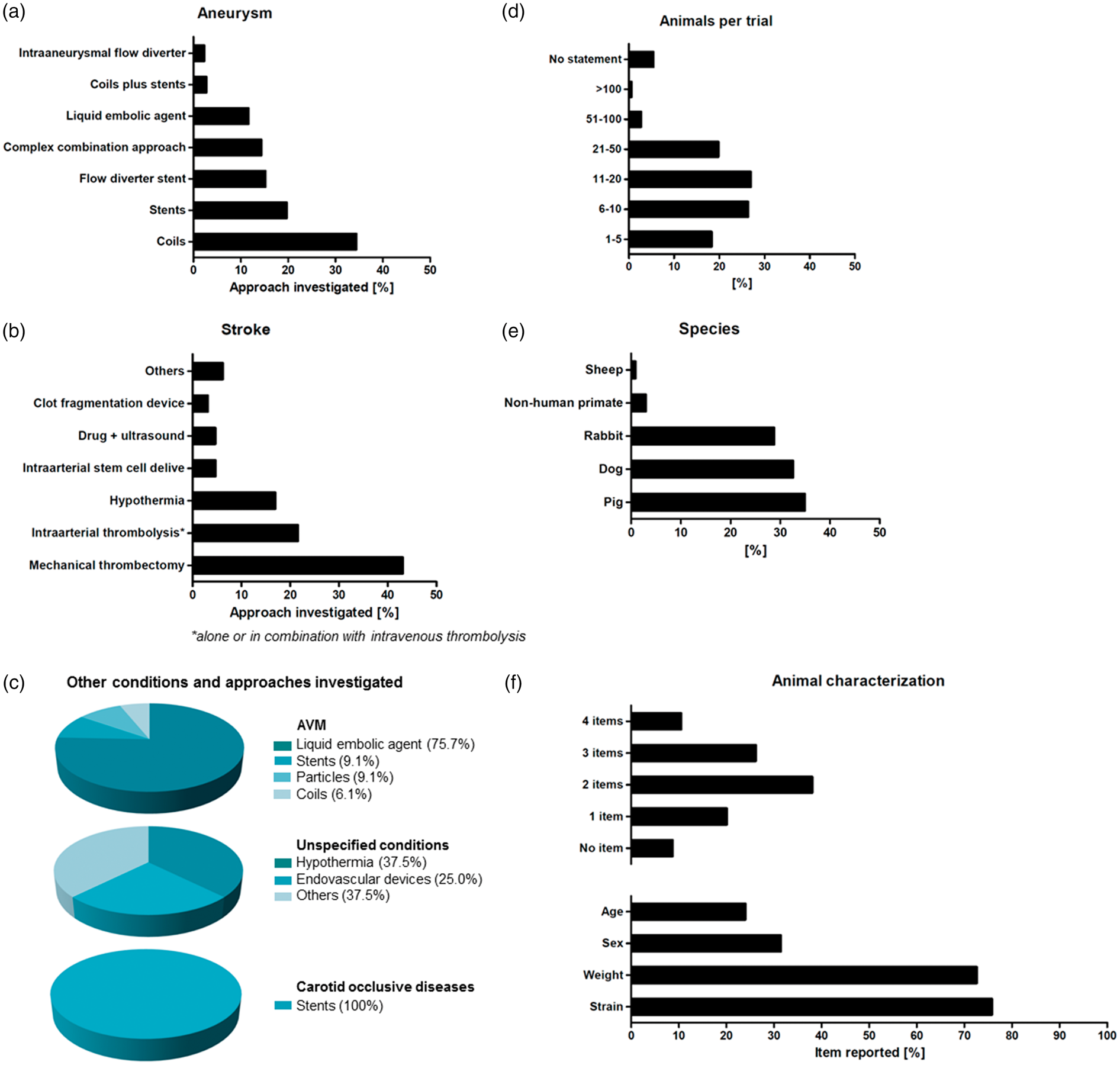
Most interventional aneurysm therapies focused on coils (34.4%, 77/224), followed by stents (19.6%, 44/224) and flow diverter stents (15.2%, 34/224). Studies also investigated liquid embolic agents or intraaneurysmal flow diverters, reflecting the technical progress in aneurysm therapy. Some therapeutic studies on aneurysms reported combined approaches. Those, for instance, comprised coils or stents in combination with additional effector substances (such as Onyx or fibroblasts,143,144 6.3%, 14/224), combined approaches using neck bridging devices (1.8%, 4/224), and microcatheter-based delivery of stem cells, 145 hydrogels, 146 and other biomaterials 147 (5.4%, 12/224). Some combination approaches were only employed by very few studies, as is the case with unconventional approaches such as magnetic microparticles 148 (0.9%, 2/224).
Liquid embolic agents were primarily investigated in AVM therapy studies (75.8%, 25/33; Figure 3(c)). Expectedly, mechanical thrombectomy was the predominant technique investigated in stroke therapy studies (43.1%, 28/65; Figure 3(b)). Intraarterial thrombolysis was investigated by 21.5% (14/65) of the studies. A significant proportion of all studies on stroke therapy investigated hypothermia (16.9%, 11/65), which may improve the results of recanalization by neuroprotective effects. 76 Only a small part of the studies investigated the effects of intraarterially administered stem cells (4.6%, 3/65), an approach believed to promote neurological regeneration.
Interestingly, we also identified one paper that reported the off-label use of a stent-retriever to remove a misplaced stent. 149 This represents an innovative complication management approach that deserves further testing in animal studies for proving and refinement prior to use in patients.
Study design
Therapeutic efficacy was the most important endpoint assessed either alone or in combination with secondary endpoints. Almost one-third of all studies focused solely on efficacy (29.6%, 99/334), directly followed by studies assessing safety and efficacy (24.2%, 81/334), or feasibility and efficacy (17.7%, 59/334). The minority of studies focused on feasibility (11.1%, 37/334) or safety (6.9%, 23/334) alone, some studies assessed safety and feasibility (7.5%, 25/334). The minority of studies (3%, 10/334) investigated the triad of feasibility, safety and efficacy simultaneously.
Some papers (23.7%, 79/334) reported acute studies (no reawakening and survival of experimental subjects), 70% (234/334) reported survival studies, and 6.3% (21/334) featured both, non-survival and survival experiments. The follow-up periods were up to one day (1.2%, 3/255), up to three days (0.4%, 1/255), up to one week (2.7%, 7/255), up to two weeks (9%, 23/255), up to one month (21.2%, 54/255), between one and two months (15.7%, 40/255), between three and six months (36.5%, 93/255), and over six months (10.6%, 27/255). Some studies did not report the follow-up period (2.7%, 7/255).
Study objectives define study duration and follow-up periods. For instance, acute studies are adequate for feasibility and safety assessments, as potential adverse events such as tissue damage can be investigated immediately. On the other hand, survival studies allow observation of short- and long-term effects including possible disadvantages of an approach that emerge at later stages. The stroke academic and industry round table (STAIR) expert consortium generally recommends long-term studies in efficacy-oriented stroke research. 16 The situation may slightly differ in neurointerventional studies in which for instance successful recanalization may serve as the major efficacy endpoint. Long-term observation is nevertheless advantageous when identifying delayed effects or complications such as aneurysm recanalization in experimental aneurysm therapy, 150 and provide a more complete context of effects. Life span of large animals allows for observation times of a year or even more.
Lack of randomization and blinding is believed to account for a significant proportion of false-positive study results. 151 Surprisingly, most large animal studies we assessed were neither designed in randomized nor blinded fashion (65.9%, 220/334). Only 12.6% (42/334) randomized experimental subjects and only 4.1% (14/334) featured a completely blinded study design; 17.4% (58/334) studies only blinded analysis of selected endpoints.
Since more investigators are usually required to perform large animal studies, complete blinding might indeed be challenging. A potential solution is to separate model induction from testing the diagnostic or therapeutic paradigm, for instance by randomization right after stroke induction, as well as to strictly separate the experimenters acquiring data from those who perform data analysis.
Animal numbers and animal characterization
Almost half of the studies only used up to 10 animals in total (44.6%, 149/334), making inter-group comparisons statistically challenging. In contrast, only a minority used more than 50 animals (3.3%, 9/334) (Figure 3(d)). Very few studies described details of animal housing and care (5.7%, 19/334). More than four fifths (82%, 274/334) of all studies reported some details on the applied anesthesia protocol. The majority gave precise information about used anesthetics (63.4%, 212/334), but some studies only provide unspecific or basic information (18.6%, 62/334). Nearly 20% of studies did not provide any information on medication at all, including anesthesia (18%, 60/334). Not even 10% of all studies (9.3%, 31/334) did report details on the use of analgesics.
Animal strain was reported most frequently (75.8%, 253/334), followed by weight (72.2%, 241/334) and sex (31.4%, 105/334) (Figure 3(f)). Age was reported by less than a fourth of all studies (24%, 80/334), and from those about one-third (27/80) only provided an unspecific classification (e.g. “adult” or “juvenile”). More than half of the studies reported one to three characteristics (60.2%, 201/334), but only 10.5% (35/334) reported all four items (strain, weight, sex, age), while 8.7% (29/334) did not provide any of such information. Information about the animals is not only essential for reproducibility of a study, but also of relevance for study result interpretation since strain, age and sex can influence both the model and the intervention. 16
No studies reported the use of subjects exhibiting comorbidities. This can be explained by the fact that comorbidities in large animals are not genetically induced, but naturally occur with age, distress, malnutrition, and other factors as is the case in humans. Therefore, comorbid large animals exhibit extremely heterogeneous phenotypes and subjects require a long time to develop these comorbidities, impairing their use.
Selection criteria
Only very few studies applied a priori defined selection criteria (4.8%, 16/334). Of these, 50% (8/16) reported specific inclusion criteria, 37.5% (6/16) reported the use of inclusion criteria but did not specify them, and 12.5% (2/16) reported exclusion criteria. None of the studies used both inclusion and exclusion criteria. Similarly, just a few studies mentioned post hoc exclusion of animals (11.1%, 37/334) with all, but one study providing the specific reason for subject exclusion. Some studies reported animal death prior to study conclusion, but inclusion of these cases into analysis (2.1%, 7/334). Information on inclusion and exclusion criteria is essential to ensure reproducibility. These criteria should be determined at the beginning of the study and mentioned in the publication. Animal health condition should be covered by inclusion criteria.
Endpoint assessment and readout parameters
Imaging endpoints dominated the evaluation process (95.1%, 318/334; referred to as “study endpoints” in Figure 4(a)), what reflects the uncomplicated use of clinical imaging modalities with large animal models as well as the high importance of imaging technologies and imaging-based endpoints in clinical neurointerventional routine and research. Imaging has been used in most cases to prove therapeutic (and sometimes model) efficacy (73.9%, 235/318; referred to as “process surveillance” in Figure 4(b)), for instance to detect revascularization after vessel occlusion or occlusion of an aneurysm. More than two-third of studies using imaging for outcome assessment have also used imaging to control for model performance, adequate model handling, and lesion induction (75.2%, 239/318; referred to as “procedural process” in Figure 4(b)). Angiography is particularly suitable for endovascular procedures, as it can be used to visualize blood flow and hemodynamic changes in the blood vessel, while simultaneously allowing potential interventions. Hence, it is not surprising that angiography was by far the most frequently used imaging procedure (96.5%, 307/318). Other modalities were used with much lower frequency. Examples comprise MRI (6.9%, 22/318), CT (5%, 16/318), ultrasound (4.4%, 14/318), or conventional X-rays and fluoroscopy (1.9%, 6/318; Figure 4(b)). The lower number of studies using such modalities can be explained by the fact that MRI and in particular diffusion weighted imaging may be important in some areas such as stroke research and treatment, but are less important for aneurysm or AVM assessment as the major domains of large animal models in neuroendovascular research. There is still a lack of data reporting variability of imaging endpoints such as ischemic volume on MRI following MCA occlusion. However, such information is important for defining sample sizes for efficacy endpoints.
Overview of endpoint assessment in analyzed studies. (a) Evaluation process: frequent use of imaging (reflecting uncomplicated use in large animals) and histology. Only 16.5% evaluated physiological parameters. Behavioral tests are applied in stroke research (b) Data about imaging: clearly dominated by angiography (well qualified for use in neurointerventional research). Most common use for imaging was to prove efficacy and for procedural process. (c) Presentation of physiological parameters: dominated by blood pressure, temperature, heart rate and electrocardiogram. CT: computed tomography; MRI: magnetic resonance imaging; OCT: optical coherence tomography.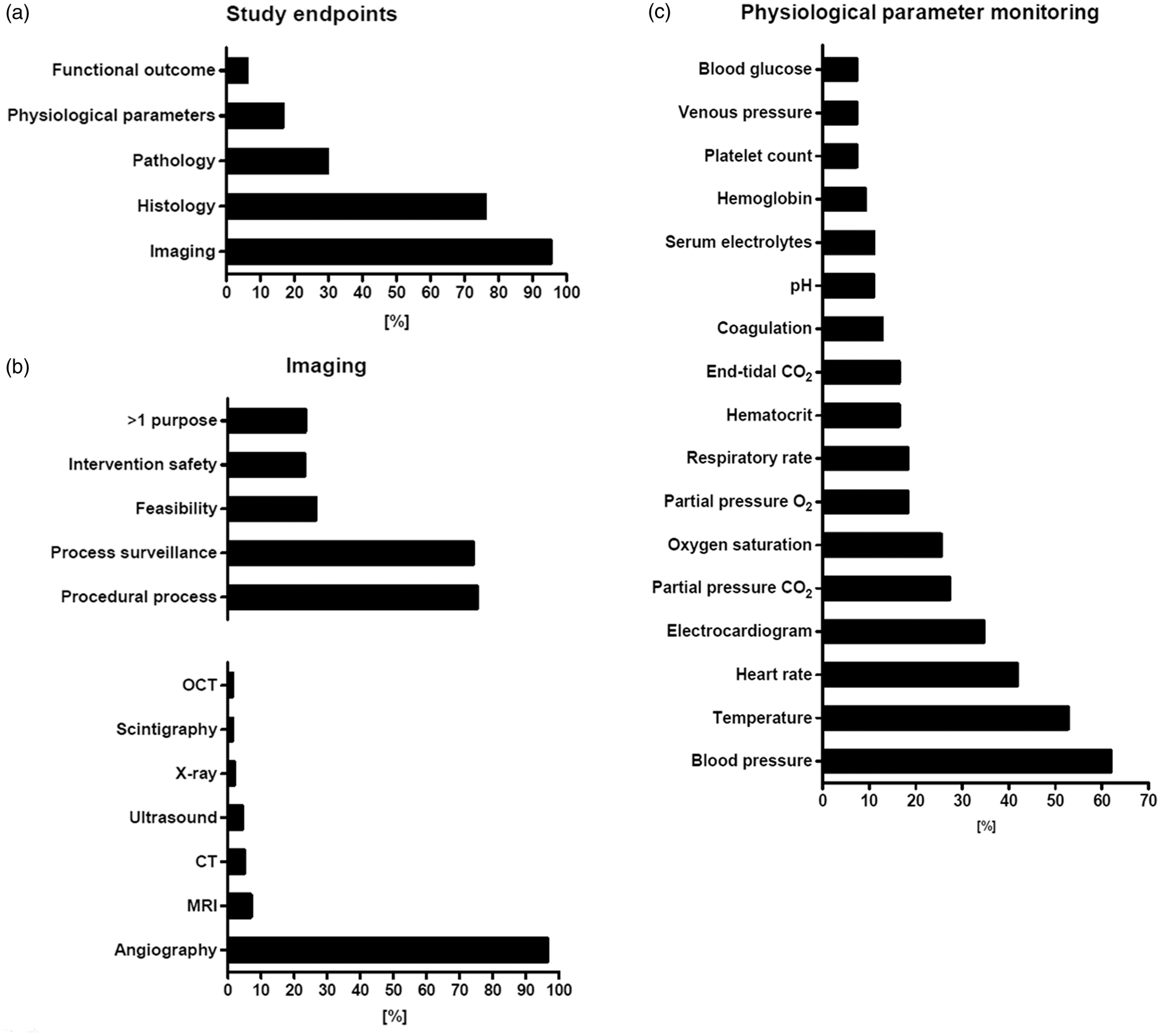
Histological examination was the second most frequent method employed for evaluation (76.1%, 254/334; Figure 4(a)). Histology is useful for safety assessment, for example to evaluate the inflammatory response or vessel wall damage, and almost half of the studies (41.6%, 139/334) indeed assessed safety alone or in combination with other endpoints. Moreover, histology can assess efficacy aspects such as endothelialization or neointima formation after coil placement.
Behavioral tests can be performed on pigs, 31 dogs, 152 rabbits, 153 NHPs, 154 and sheep. 30 However, only a small proportion of the studies used behavioral endpoints (6%, 20/334; Figure 4(a)). Interestingly, all of these studies focused on stroke. In turn, almost a third of studies focusing on stroke included behavioral tests (30.7%, 20/65). Behavioral tests are a valid option to investigate functional effects of stroke lesion induction and therapy. The STAIR committee16,17 recommends at least two outcome measurements allowing both functional and morphological assessment in stroke research, what shall also account for large animal models.
Some studies measured brain temperature (3.9%, 13/334) or intra-aneurysmal pressure (1.5%, 5/334), while others specifically investigated mortality and morbidity (1.2%, 4/334). Only few studies reported special aspects such as radiation dosimetry (0.6%, 2/334), coil insertion pressure, stereographic photography, liquid scintillation counting (0.3% each, 1/334), drawing blood samples (0.6%, 2/334), pressure transducers in the RM, cerebrospinal fluid sampling, or cerebral blood flow (0.3% each, 1/334).
Not even one-fifth of all studies evaluated physiological parameters (16.5%, 55/334). This is surprising, because recording of physiological parameters in large animal models is even less complicated than in rodents, and a broad spectrum of physiological parameters may be recorded easily, and simultaneously. Blood pressure was the predominant parameter recorded (61.8%, 34/55), followed by temperature (52.7%, 29/55), heart rate (41.8%, 23/55), and electrocardiogram (34.6%, 19/55; Figure 4(c)). End-tidal isoflurane, end-tidal O2, body weight, cardiac output, intracranial pressure, electroencephalogram, d-dimer (3.6% each, 2/55), hemograms, renal function during surgery, motor-evoked potentials, and auditory brain stem response (1.8% each, 1/55) were investigated rarely. Some studies 5.5% (3/55) reported measuring of physiological parameters, but without any further details including the particular parameters monitored.
STAIR16,17 recommends rigorous physiological monitoring to control for potential side effects of surgery, and to reduce or at least explain infarct size variability. This recommendation can be extended to neurointerventional research using large animals. Reporting of some core physiological parameters such as blood pressure, temperature, and heart rate should be mandatory. Recording of additional physiological depends on the respective study objective. For example, in studies featuring hypothermia, monitoring of blood gases is essential as these are influenced by body temperature. 155 Any study should record physiological parameters not only at the beginning and the end of an experiment, but also in the meaningful intervals throughout the procedure. Measuring physiological parameters is an elegant way to derive the maximum of information from a single experimental subject, facilitating result interpretation and, if necessary, providing a thorough basis for subject exclusion.
Only 0.6% (2/334) of the studies clearly defined study endpoints, but these featured both primary and secondary end points. This is nevertheless a surprisingly low number. Large animal models are primarily used in confirmative and translational research, often as the last experimental step prior to clinical application, and thus critically depend on a clear definition of study objectives and, thereby, primary and secondary endpoints.
Conclusion
Large animal models offer many important benefits – foremost to mention their similarities to human brain and vascular anatomy – that make them attractive for neurointerventional research. New endovascular approaches can be developed and refined in large animal experiments, which may improve minimal-invasive neurointerventional therapy for patients in future. On the other hand, large animal studies are laborious and expensive. Careful study planning, deriving maximum information from each study subject, and transparently reporting negative data or pitfalls are therefore essential. Tapping the full potential of large animal models critically requires careful outweighing the individual advantages and disadvantages of animal models, carefully selecting the model best suitable to answer the research question, and implementation of improvements where required, as well as maximally precise study design.
Supplemental Material
Supplemental material for Large animals in neurointerventional research: A systematic review on models, techniques and their application in endovascular procedures for stroke, aneurysms and vascular malformations
Supplemental Material for Large animals in neurointerventional research: A systematic review on models, techniques and their application in endovascular procedures for stroke, aneurysms and vascular malformations by Andrea M Herrmann, Stephan Meckel, Matthew J Gounis, Leona Kringe, Edith Motschall, Christoph Mülling and Johannes Boltze in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: only intramural funds were used for this work.
Acknowledgements
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SM: consultancy and honoraria as member of the scientific advisory board (Acandis GmbH); travel support (Covidien/Medtronic; Microvention; Stryker); study grant (money paid to institution; Bracco S.p.A.); JB: consultancy and honoraria (Acandis GmbH). All other authors declare that they have no conflict of interest.
Availability of data and material
The datasets generated and/or analyzed during the current study are available from the corresponding author on request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.