
Abstract
The embedding of lived experience experts (LEEs) is increasingly recognized as important in research, but evidence from low- and middle-income countries (LMIC) remains sparse. This viewpoint aims to present and critically reflect on a model for integrating LEEs into the design of an artificial intelligence (AI)-based mental health (MH) study to develop an automated depression screening system in India. We report on the process of forming a diverse Lived Experience Advisory Panel (LEAP) and show how LEAP influenced methodology, system design, ethics, and language through a three-day workshop and co-design sessions. We also highlight the ethical, structural, and power-dynamic challenges encountered, demonstrating that meaningful LEE partnership is both feasible and essential for developing culturally grounded, safe, and clinically acceptable AI applications in LMIC settings.
Keywords
People with lived experience and their families develop a unique expertise in the condition they have endured over time, making them lived experience experts (LEE). 1 Many international funding agencies, including the UK’s National Institute for Health Research, Wellcome Trust, and the Canadian Institutes of Health Research, have guidelines on LEE involvement, and many high-impact journals (The Lancet, BMJ) require LEE participation in published articles. 2 By making research participatory, identifying and addressing inequities, and creating solutions that are truly useful to the end beneficiary, LEE involvement significantly improves mental health (MH) research. 3 Globally, there is increased recognition of the need to meaningfully involve these experts at all stages of MH research, rather than a tick-box approach. 3 Meta-research studying LEE involvement in MH research mostly comes from developed countries, with Pinfold et al. identifying only one study from Southeast Asia (multicentric). 4 Most government agencies funding MH research in low- and middle-income countries (LMIC) do not mandate LEE involvement. However, recent studies have shown that meaningful LEE engagement is challenging but possible and essential in non-Western settings, as well.5,6 Finally, while we strive for diversity, equity, and inclusion (DEI) in research participants, 7 this is rarely discussed in the context of LEE involvement. This omission is striking, as various intersectional identities, advantages, and disadvantages shape the experience of mental illness. 8
In this context, we report the key considerations, process, and outcomes of engaging LEEs in co-designing an artificial intelligence (AI)-based MH research protocol. This work was conducted at two tertiary-level MH institutes, one in South India and another in Northeast India. Both are government-funded teaching hospitals that provide subsidized treatment for mental and neurological illnesses. Researchers from the two centers submitted a joint concept proposal for a directed research grant to the Wellcome Trust—titled “Generative AI for Depression, Anxiety, and Psychosis”—proposing the development and testing of a multilingual human-in-the-loop (HIL) system to assist in the identification and assessment of depression, titled “Human-in-the-loop Evaluation of Assisted Depression Screening (HEADS).” The system aims to provide a diagnosis according to the Diagnostic and Statistical Manual of Mental Disorders and to assess depression severity using the Patient Health Questionnaire. Supplementary Figure S1 provides an overview of the research proposal. The Wellcome Trust supports this study under the MEXA—Accelerator Phase (Grant reference: MEXA2025-003a). The funder had no involvement in the study design, data acquisition, analysis, or manuscript preparation.
The overarching aim of this viewpoint is to present and reflect on the adaptation of an LEE integration model to the Indian context for AI-based MH research. We give a practice-based reflective account of participatory research in LMICs, in which the objectives are to: (a) Describe the research team’s conceptualization of the lived experience panel with multiple axes of representation, in line with DEI; (b) illustrate the recruitment process, co-design sessions and modifications to the research protocol made in collaboration with LEEs; (c) critically reflect on the ethical, structural, and power-dynamic challenges encountered during this partnership. We also briefly define the terminologies used in the article: “LEE involvement” refers to the overarching philosophy and mandate of integrating experiential knowledge into research. “Co-design” refers to the specific collaborative workshops and sessions undertaken along with LEEs to shape the study design. Finally, “partnership” denotes the equitable relationship and shared decision-making authority between the research team and LEEs.
Discussion
Defining the End Beneficiary: The Promise of Digital Mental Healthcare
The National Strategy for Artificial Intelligence, by the National Institution for Transforming India, asserts that AI applications are central to addressing the healthcare gap in India, especially in rural areas with poor connectivity and limited healthcare workers. 9 With cheap, almost universally available mobile phones and internet connectivity, a digital health system in the local language can significantly help close the healthcare gap for underserved populations.
While designing the HEADS proposal (an automated system for non-psychiatrist healthcare workers to identify and assess depression in Indian languages), we defined the end beneficiary as an individual suffering from depression who would avail this service. This individual is most likely residing in a rural area, has a lower socio-economic status, is not highly educated, is not tech-savvy, cannot afford specialist doctors in the city, and has a linguistic barrier (i.e., limited English proficiency). We wanted to include these very end beneficiaries in our lived experience panel to reflect their perspectives. We obtained approval from the Institute Ethics Committee (No.: NIMHANS/EC (BEH.SC.DIV.)/2025 dated September 3, 2025) for this work.
Diversity, Inclusivity, and Meaningful Involvement in the Indian Context
At the beginning, a co-investigator with lived experience of depression was the only LEE involved. Having a diverse and representative panel of LEEs was our primary consideration. Other than the obvious axes—gender, age, sexual minorities, and diagnosis—we also wanted to ensure representation of education, linguistic diversity, depressed classes, socio-economic status, and urban versus rural residents. We believed the latter two to be more important diversity axes in the Indian context, where the healthcare gap is much higher in rural areas,
10
and nearly half of the healthcare expenditure is out-of-pocket,
11
severely disadvantaging poorer people. We considered partnering with patient support groups or registered advocacy groups (e.g.,
We concluded that only a ground-up, tailored approach would work. Most co-investigators on the project were primarily clinicians, and each invited LEEs, ensuring diversity across all aspects of the project. We cannot have LEEs solely from rural, impoverished backgrounds, as the significant power gap between highly educated, urban, affluent researchers and these LEEs may lead to socially desirable responses rather than honest feedback. Similarly, having all urban, tech-savvy LEEs from high socio-economic backgrounds is impractical, since they are less likely to depend on automated depression screening systems due to their access to quality healthcare. Therefore, balancing representation across different groups was the crux.
We planned a “partnership” approach, in which LEEs fully participated at every stage of the research (planning, conducting, interpreting, and dissemination), sharing decision-making responsibilities. Twenty LEEs were invited, and 15 agreed to become part of the Lived Experience Advisory Panel (LEAP). The remaining declined primarily due to time constraints.
Minimizing Information Asymmetry
We wished to immediately overcome the perceived hegemonic divide between the “academic clinician” and the “patient,” an inherent issue during LEE involvement in research. 12 We must also consider the sources of power imbalance—social dynamics and information asymmetry. 13 In LMICs, doctors frequently belong to the privileged class, while patients come from varied backgrounds. Furthermore, the research team is likely to know more than LEEs and can choose to share information selectively.
In this regard, a co-investigator had a ~60-minute discussion and onboarding process with each LEE in the language they were comfortable with. They explained the proposed study and the LEAP and LEE’s roles, emphasizing that LEEs would be equal partners. Flexible privacy options were also discussed, making it clear they could choose what to reveal and how much.
This LEAP had equal representation of men and women from diverse socioeconomic, linguistic, and educational backgrounds, as well as from various regions of the country (Southern, Northern, and Northeastern), spanning from engineers to individuals unfamiliar with even basic cell phones. All chose to identify themselves by name and meet in person with the research team and other LEEs; some also disclosed their professions, which were directly relevant to the study (human rights advocate, data scientist, engineer, management executive). Supplementary Table S1 and Figure S2 provide finer details on the LEAP formation and composition.
Co-design Sessions
We conducted a three-day workshop on responsible AI for psychiatry in India, where we invited domain experts from computer science, AI ethics and governance, psychiatry, community MH, and LEEs to deliberate on ethical considerations for the use of AI in mental healthcare (URL:
Ensuring Safety and Joint Reflection
In addition to the detailed onboarding process for each LEE before joining LEAP, we also did the following to ensure the understanding, safety, and comfort of all LEEs: During the workshop on responsible AI use, domain experts discussed topics related to ethics and safety. They also summarized their talk in an Indian language in the end. Moderators in both sites translated the summary into the LEE’s native languages. The co-design sessions involved almost as many non-researcher mental healthcare workers (translators, moderators, observers) as LEEs. These individuals themselves asked many questions about AI and the study, which made the sessions truly participatory and inclusive of all stakeholders.
Sessions began with investigators and moderators introducing themselves in Indian languages, omitting their titles or affiliations to reduce hierarchy. A dual expert LEE (identifying as a psychiatrist and depression survivor) and a few other LEEs (with higher education backgrounds, who had agreed to greater disclosure) introduced themselves first. This set an example for openness and greater participation for hesitant members. Conducting the sessions in Indian languages itself broke down hierarchy barriers. We also used storyboards and group discussions, following a cycle of working in smaller groups and coming together for evocative, reflective discussion.
Taking the LEAP into True Co-research
We give some illustrative examples of how LEAP co-designed the study protocol. We asked the following question: While designing an automated system, what should research focus on—diagnosis or treatment? LEAP chose diagnosis, highlighting that they felt a correct diagnosis is the most important, as it is the first step toward treatment.
About collecting audio recordings of patient interviews, four approaches were considered: (a) Avoiding audio recording altogether due to privacy risks, (b) censoring personally identifiable information in participants’ presence, (c) employing in-house transcribers and translators to ensure data safety, (d) using third-party services only under strict non-disclosure agreements (NDAs). The LEAP endorsed a combination of (b) and (d)—censoring recordings in front of participants and obtaining NDAs from all transcribers and translators, whether internal or external. The theme, however, was the common good of the peer community versus the sacrifice of some individuals’ rights. In such a context, they would be willing to give their time and allow researchers to record long interviews with much personal detail, and they were confident that other peers would as well. However, there were limits—subsequent deidentification was mandatory, and video recording was certainly intrusive and out of question.
Communication of uncertainty was paramount. While the automated system for depression diagnosis gives its inference, it must also convey its level of certainty to the healthcare worker, giving the HIL enough agency to take their own decision; otherwise, it could lead to over- or underdiagnosis. The language of communication was of most importance. Some LEEs said they would choose a well-trained automated system that understood and communicated in their language over a human doctor who did not. Additionally, audio recording and automatic transcription would help prevent doctors from taking notes during interviews. Doctors writing during conversations often gave the impression that they were not paying attention to the patient. Table 1 lists the other suggestions from the LEAP.
Suggestions by LEEs Incorporated into Various Aspects of Study Design.
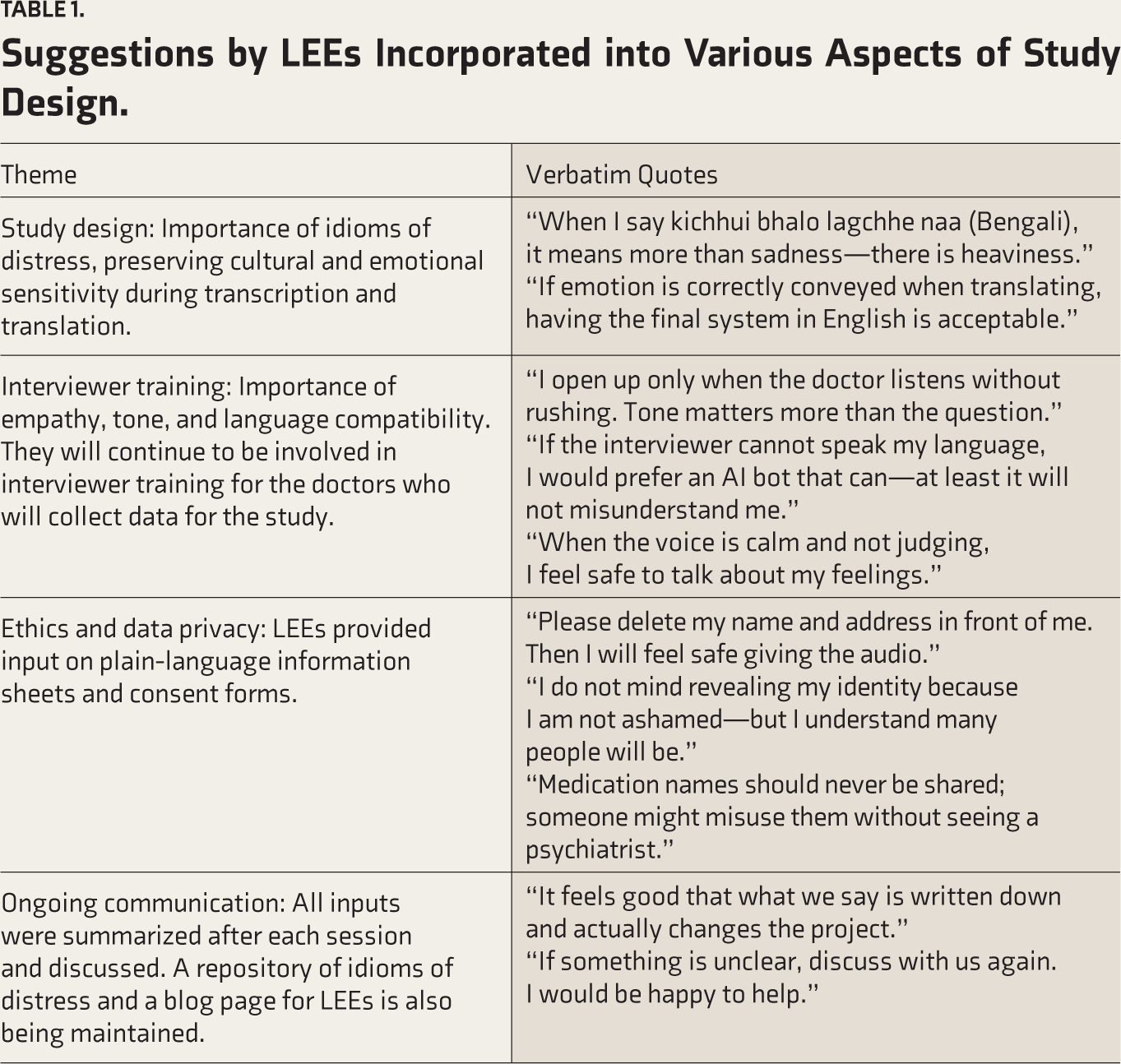
All such suggestions have been incorporated into the final study proposal, including guidelines for interviewing, audio recording, transcription, and translation (Supplementary Tables S2 and S3 provide examples). To reflect on the co-design process, we collected anonymous feedback from the LEAP members after the sessions. The sessions were described as respectful, inclusive, insightful, and essential, with everyone expressing interest in participating in subsequent sessions (Supplementary Figure S3 and Table S4). Additionally, the depth of involvement and interest is further illustrated by the fact that two members of the LEAP are co-authors on this article.
Challenges, Learnings, and Unanswered Questions
We faced various challenges during this work: Explaining technical AI-related and methodology concepts in simplified language was challenging and required detailed conversations. Discussions during sessions often occurred simultaneously in Hindi, Kannada, Assamese, Bengali, and English—we had to ensure that we communicated to every LEE in their own language without fail. However, there was an advantage—LEEs discussed in great detail and compared “idioms of distress” across various Indian languages, providing insight into the different expressions of psychiatric phenomenology in these languages. Although we strived to include all marginalized groups, we could not find LEE representation from some groups, such as the transgender community (we had one LEE who was of homosexual orientation), in spite of active efforts. Despite varied educational, socio-economic, and linguistic backgrounds, every LEE understood the study design and its ethical considerations and provided clear, detailed feedback on design modifications at each step. In addition, we faced another challenge. Guesthouses in academic institutions are reserved for academic faculty. In one case, administrative permission was not granted for an LEE’s institute accommodation, nor for financial compensation to accommodate them outside. As a result, a co-investigator hosted the LEE at their own residence. This reflects a deeper structural and policy issue, which can only be remedied by systemic change that views LEEs as equal partners.
We also faced a systemic dilemma regarding ethical oversight, that is, informed consent and ethics committee approvals for this process. Although these were technically interactions with “patients,” the engagement was a partnership—a “co-researcher” rather than a “participant.” Is this not akin to inviting a colleague to be a co-investigator in a project? There are no clear answers to such questions, which highlights a gray area in current frameworks for ethics committees in India. Because LEEs were technically individuals with a history of mental illness, the existing framework considered them as study participants from whom qualitative data was being extracted. Even though the true nature of engagement was that of a co-researcher, this ethics framework led us to obtain traditional informed consent from LEEs. As collaborative methodologies become widespread, future guidelines for ethics committees in India may change to include provisions for LEEs as co-researchers, rather than just participants. That said, provisions such as a separate informed consent form for LEEs will ensure protection and autonomy, and it is worthwhile to follow all procedures required to protect human participants in research, specifically modified for LEE involvement.
A shift from the paternalistic, deficit-based, “vulnerable individual” approach to a strength-based approach may be warranted. 12 Along these lines, we faced a practical challenge. While providing honorarium for one LEE, a survivor of depression and alcohol use disorder, there was a concern that they would relapse to alcohol on getting access to a large sum of money (access to money had been a contributory factor for relapse in the past). We took a paternalistic approach and handed the amount to a family member. We list out other practical dilemmas we faced in Supplementary Table S5. By adopting a reflective decision-making approach and acknowledging the inherent power imbalance, we may be able to navigate these ethical dilemmas effectively. 12
What is the Way Forward?
This work demonstrated that LE involvement in the LMIC context is not only feasible but invaluable, even in niche areas such as the application of AI in MH research. LEEs are experts in their own right and can contribute directly to the scientific process through their experience. All clinicians personally know highly educated and accomplished LEEs. The real task is to encourage these LEEs to bring in peer LEEs who may not otherwise participate in such work. Notwithstanding this, training and capacity building for LEEs is an important opportunity, allowing for active participation in practical aspects such as data collection, quality control, analysis, and writing. 14 This recognizes them as co-researchers, not merely passive advisors. 15 We plan to adopt a similar stance, where LEEs will be trained to review transcripts and translations for cultural and emotional sensitivity, forming Language Evaluation Groups, and evaluating the automated system for bias through Bias Evaluation and Mitigation groups.
Conclusion
This viewpoint aims to provide a rich, descriptive, experiential account of integrating lived experience into MH research. Also, we specifically report on some aspects of the co-design sessions and methodology using the Qualitative Research Checklist for MH Studies. (Supplementary Table S6). Valuing LEE contribution and true integration requires systemic change, such as including LEE work in long-term budgets and plans of institutes, giving true decision-making authority through memberships of ethics committees and monitoring panels. While the MH policy in India is making a move in the right direction by incorporating two members with mental illness as part of the MH review board. Most Indian universities have yet to include lived experience in research. At a larger level, there is a pitfall: Funding agencies often fund community engagement programs but do not specify LE involvement. National and international funding agencies have enormous power to foster this culture and must consider LE integration as a primary component while evaluating study proposals. By shifting from tokenism to a true partnership with LEEs, researchers can ensure their work is culturally and ethically grounded, with greater benefit to end users.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We thank Mr Surajeet Verma, Ms Jupitora Kakoti, Dr Hemanta Dutta, Dr Binita Talukdar from LGBRIMH Tezpur; Ms Meghana GB, Dr Lakshmanan Sethuraman, Ms Sanchitha from NIMHANS Bengaluru; Dr Sachin Barbde from Ekjut Foundation; Mr Kamaruz Hoque from Satra, Sipajhar, Assam; Dr Rayna and Mr Nanjappa from Institute of Public Health (IPH), Bengaluru for their support and suggestions. We thank all our lived experience experts for their time, energy, expertise and enthusiasm in making this a truly productive and successful engagement.
Reporting Guideline (Supplementary online material)
Name: Qualitative research checklist for mental health studies
Citation: Beg MJ. Qualitative methods in mental health research: Standards for ethical inquiry, research practice, and peer review. Indian Journal of Psychological Medicine. 2025;0(0). doi:
Data Availability Statement
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethical Approval
Name of the Institutional Ethics Committee/Independent Review Board: The study was approved by the Institute Ethics Committee of NIMHANS Bengaluru. Approval Ref. No.: NIMHANS/EC (BEH.SC.DIV.)/ 2025. Date: September 3, 2025.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This pilot project is supported by an award from Neuromatch, Inc. as part of the Generative AI for Mental Health Research Accelerator, funded by Wellcome Trust Limited. [Grant number: MEXA2025-003a].
Informed Consent
Informed consent was obtained from all participants included in the study.
Citation Diversity Statement
We are committed to equitable citation practices and have made conscious efforts to include work from authors of diverse genders, geographic regions (including the Global South), career stages, and historically marginalized groups. We aim to support a more inclusive and representative scholarly record.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.