
Abstract
Adult mental health challenges frequently stem from undiagnosed poor mental health earlier in life. With increasing levels of poor adolescent mental health and insufficient health care resources in low- and middle-income countries, mobile mental health may offer expanded service access. Little is known about mobile mental health interventions for adolescents in low- and middle-income countries. Our aim was to review the literature on mobile mental health intervention, development and use for low- and middle-income country adolescents. We searched APA PsycInfo, Web of Science, Psychiatry online, and Ebscohost databases using keywords and phrases. Screening of the 6953 retrieved articles, generated 6 articles that met the inclusion criteria. Arksey and O’Malley’s adapted framework was followed using rigorous inclusion criteria and screening by two reviewers. Studies showed high heterogeneity. Two studies used short message service text messaging platforms, one used phone call reminders, two used smartphone applications (WhatsApp or game-based), and one study compared different short message service, web-based and smartphone app offerings. Generally, adolescents had a positive perception of mobile mental health interventions. Helpline messages, peer group sessions, access to a counsellor and games set in real-life environments were some of the preferred contents of mobile mental health interventions. Noted barriers include low personal mobile phone ownership, leading to lack of confidentiality, data costs and limited internet access. While adolescents in low- and middle-income countries find mobile mental health interventions acceptable and supportive, challenges remain. Mobile mental health interventions can potentially overcome barriers associated with face-to-face care, such as high cost and stigma. However, more research is needed to overcome these challenges and build the evidence-base in low- and middle-income countries for this field to grow.
Introduction
The World Health Organization (WHO; 2022) defines mental health as ‘a state of well-being in which an individual realises his or her own abilities, can cope with normal stresses of life, can work productively and can make a contribution to his or her community’ (para 1). Mental disorders, which are health conditions that change one’s thinking, mood, or behaviour associated with impaired function, are common in adolescents and young people. It is estimated that mental illness, which refers to all diagnosable mental disorders, accounts for approximately 14% of the global burden of disease and main burden of disease in children and adolescents (Mokitimi et al., 2018; Yatham et al., 2018). Of the 970 million people living with mental health disorders globally, over 80% reside in low- and middle-income countries (LMICs), which typically have large youth populations (WHO, 2022, para 2; Yatham et al., 2018).
Approximately three-quarters of mental disorders that occur across the lifespan have their first onset during adolescence (Solmi et al., 2022). This stage (ages 10–19) is defined as a unique and formative time where multiple physical, emotional, and social challenges, including exposure to poverty, abuse or violence, can make adolescents vulnerable to mental health disorders (Chulani & Gordon, 2014). Poor mental health in adolescence can hinder optimal development and functioning (Mokitimi et al., 2018). Furthermore, mental health disorders negatively impact social relationships, physical health, and academic performance, resulting in low wage earnings in adulthood (Grist et al., 2017). Evidence shows that many mental health conditions in adulthood stem from undiagnosed mental disorders during childhood, impacting the ability of individuals to meaningfully contribute to their communities (Hatcher et al., 2019). Yet adolescent mental disorders in LMICs remain largely untreated due to reluctance from young people to seek help, services that are limited and often not tailored to youth or mental health or both, and other barriers such as cost, confidentiality concerns, stigma, and lack of mental health literacy (Ridout & Campbell, 2018; Seko et al., 2014). It is therefore important to identify innovative approaches for delivering sustainable mental health care in terms of reach and impact, particularly among populations at higher risk such as adolescents.
Over the last two decades, there has been a rapid advancement in digital technologies such as smartphones, mobile digital applications, and social media. Health care workers have leveraged these technologies to deliver health information and interventions in the form of mobile health (Seko et al., 2014). More recently, the adoption of mobile health technology for mental health has grown exponentially. Approaches to care using mobile technology offer an alternative to providing in-person care, and may improve the quality and availability of care, and reduce barriers to face-to-face help-seeking, such as stigma or concerns about talking about one’s mental health challenges (Ben-Zeev et al., 2017; Grist et al., 2017). The advantages of using mobile mental health (MMH) technology include accessibility, the potential for anonymity, timely feedback, and lower cost compared to traditional mental health service delivery (Liverpool et al., 2020). MMH interventions also have the potential to overcome language barriers by allowing users to use a language they are comfortable with – if they are developed in local languages (Noack et al., 2021).
Remote support utilising MMH has the potential to overcome geographical barriers to care and provides mental health support to hard-to-reach groups, such as adolescents who may not seek help through traditional care pathways (Grist et al., 2017). More importantly, MMH approaches have a great potential for impact in under-resourced and developing countries, such as in LMICs with limited access and poor quality of health care. Despite MMH’s potential to address the treatment gap in mental health care in LMICs, little is known about the use of MMH, its development and implementation, availability and acceptability, and barriers to use among adolescents. To address the gap in the literature, this scoping review was conducted to summarise existing work in adolescent MMH in LMICs and to provide steps for future developments of MMH interventions for adolescents.
Method
This scoping review process followed an adapted version of Arksey and O’Malley’s (2005) framework, which involves identifying the research question, identifying relevant studies, study selection, charting the data, and collating, summarising and reporting the results. In brief, the research question was: What is the availability and acceptability of MMH interventions for adolescents, and what has facilitated their successful implementation or acted as barriers to their use in LMICs?
MMH interventions included in the review were defined as: short message service (SMS) or text messaging, smartphone games, phone calls, and smartphone applications. Search terms and databases were determined in consultation with the authors. The following search string was adapted for each database: mobile health OR digital health OR mhealth OR text messag* AND design OR development OR intervention AND adolescent OR young people OR youth AND mental health. Searches were conducted in the following databases: PsycINFO, Ebscohost, Web of Science, and Psychiatry Online. In addition, an electronic search in Google Scholar and reference list checking of relevant articles were conducted to identify any additional articles missed during the initial search. Titles, abstracts and full-text articles were screened for relevance against the following inclusion criteria: (1) the article is a research study; (2) the focus of the study was mobile health, defined as medical and public health practice supported by digital technologies for mental health intervention; (3) the target population included adolescents aged 10 to 19 years; (4) the study was conducted in an LMIC; and (5) the article was written in English. Articles were excluded if they focused on adults or the general population. There was no restriction on publication dates. Grey literature, for example, dissertations and conference proceedings were excluded.
Screening process
Rayyan software (Ouzzani et al., 2016) was used to manage the process of screening and selecting research articles. Articles were screened by the author (SM) and research assistant (MM) between July and September 2022.
Charting the data
The final articles selected for data extraction were grouped according to the type of MMH intervention used. After reading the articles in full, key information was entered into a data extraction table and reviewed by the co-authors independently to cross-check the validity of the data characterisation. Following this process, three domains were identified using Braun and Clarke’s guidelines for thematic analysis (Terry et al., 2017).
Collating, summarising, and reporting the results
Data were extracted according to key characteristics, including author, year of publication, country, population, sample size, age of participants, the type of MMH intervention, and whether it was a development, evaluation, or feasibility and acceptability study. Key findings from each article were also recorded.
Study characteristics.
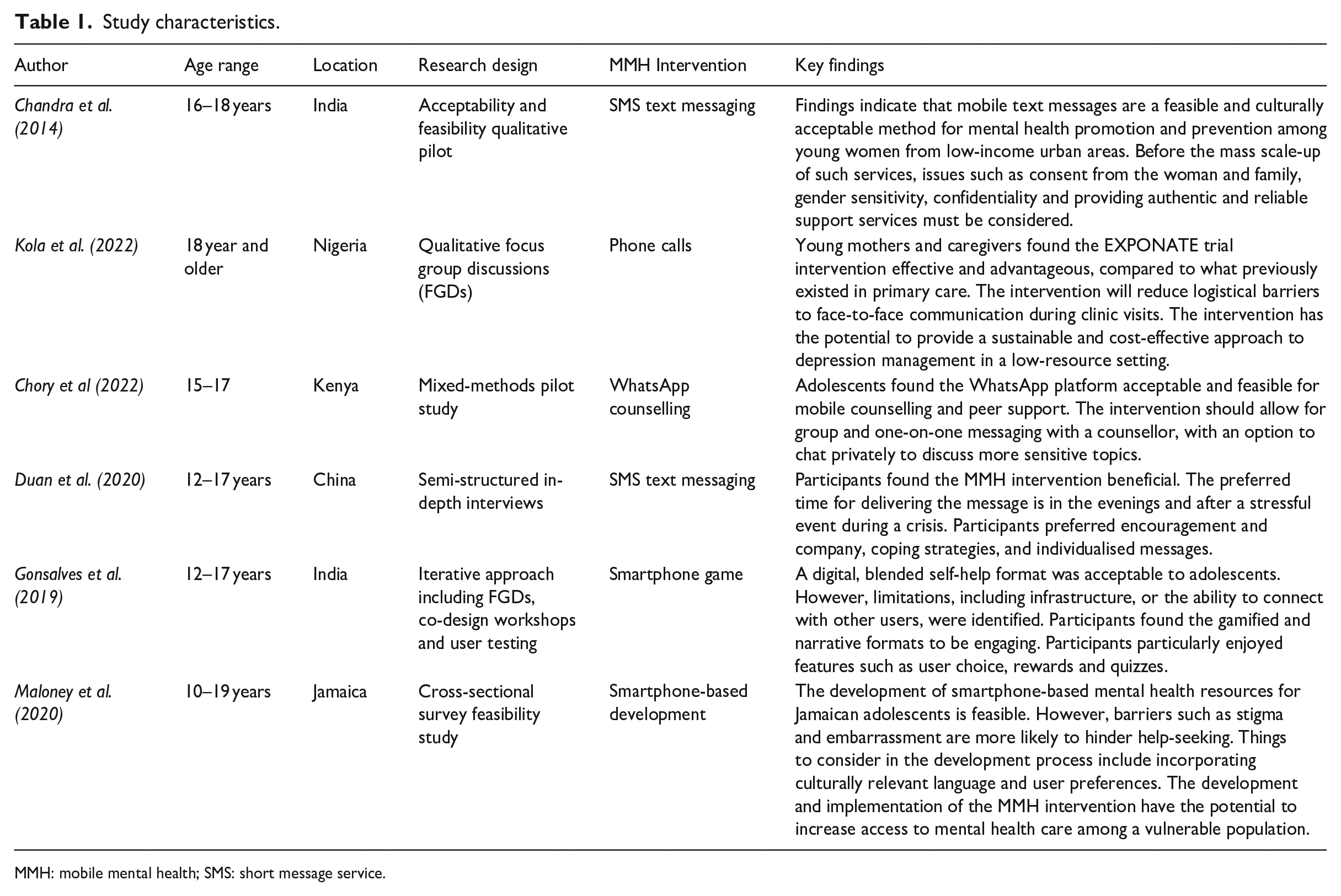
MMH: mobile mental health; SMS: short message service.
Ethical considerations
No ethical approval was required for this review article.
Results
Description of studies
Initially, 6953 articles were identified, and 624 duplicates were removed. Following this, 6329 articles were screened by title, and 6013 were excluded. The remaining 316 articles were screened by abstract, and 277 were excluded. Of the remaining 39 full-text articles assessed for eligibility, 33 did not meet the criteria due to the wrong population, age group, location, and/or grey literature. A total of six full-text empirical articles met the inclusion criteria. See the flow diagram in Figure 1 for the review process.
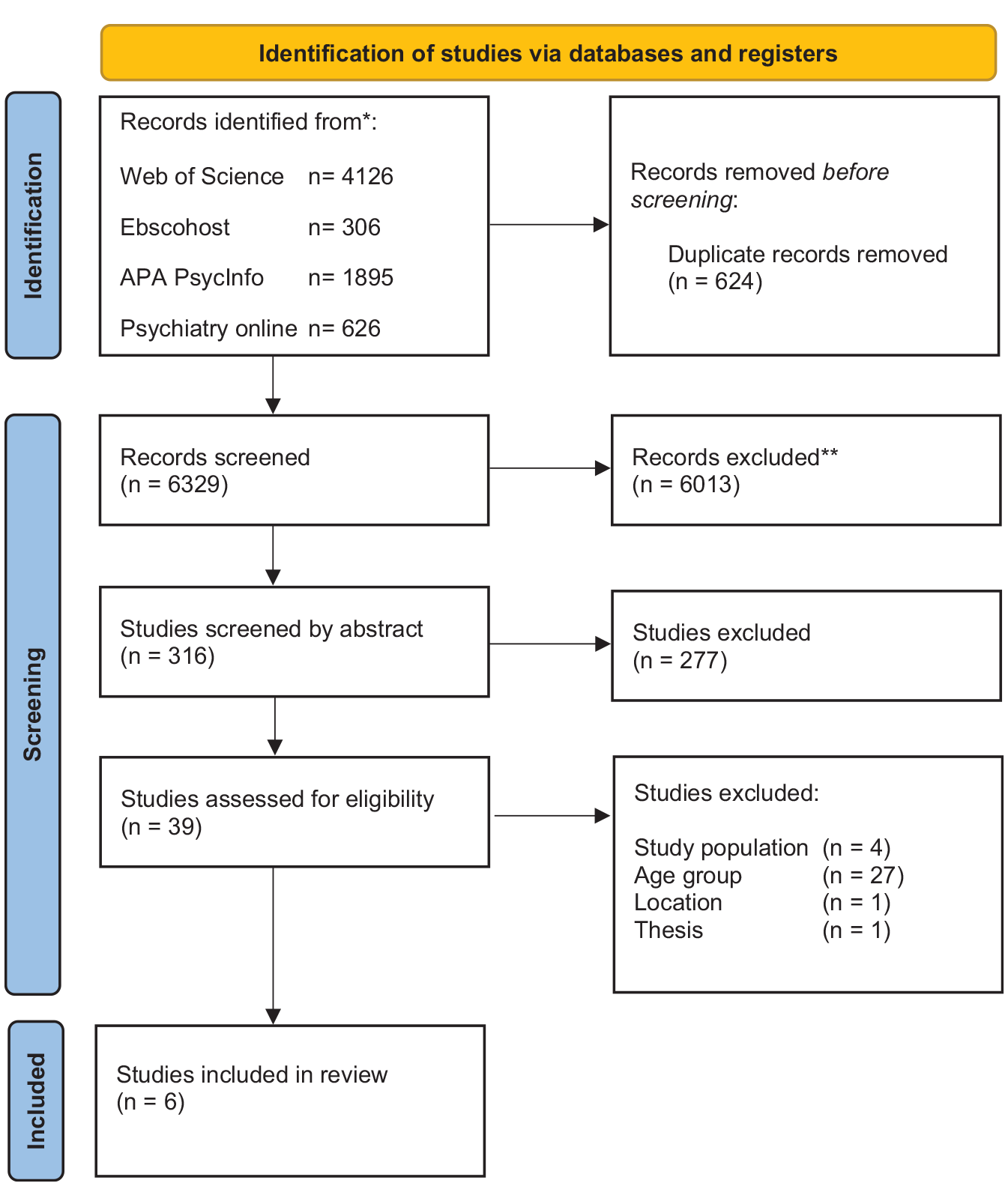
PRISMA flow diagram.
The six studies were published between 2014 and 2022, with the majority (five) published since 2019. There were three qualitative studies, one quantitative study, one mixed-method study, and one study that followed an iterative approach. The sample sizes of the studies ranged from 17 to 124 adolescent participants. Two out of the six studies included only female participants. The studies were conducted in Nigeria (1), Jamaica (1), China (1), Kenya (1), and India (2).
The six studies explored adolescent perceptions of using mobile health interventions for their mental health needs. Two of the six studies used short message service (SMS) text messaging platforms as an MMH intervention. One of the six studies focused on phone call reminders, while two others focused on smartphone applications such as WhatsApp and games. Finally, one was a feasibility study to determine the viability of using mobile health resources such as SMS communication, web-based and smartphone application. Three domains were identified from the six studies, namely: (1) Adolescents perceive MMH approaches as useful, (2) Access to mobile devices and other barriers impacting the use of MMH, and (3) MMH content preferred by adolescents.
Domain 1: adolescents perceive MMH approaches as useful
All six studies reported high levels of satisfaction from adolescents with MMH interventions. Maloney et al. (2020) reported that more than 50% of their participants indicated they would be interested in using a smartphone application to monitor their health. In Duan et al. (2020), most participants reported that the SMS text messaging intervention could benefit them, and they were willing to receive text messages. Positive experiences with WhatsApp chats were reported by Chory et al. (2022), where adolescents said these chats created a feeling of community and peer support among adolescents living with HIV. Similarly, according to Chandra et al. (2014), adolescents reported that they preferred receiving messages with quotes and brief phrases on positive well-being and felt that someone was there to care for them. Gonsalves et al. (2019) found that a digital blended self-help format was acceptable to school-going adolescents with or at risk of anxiety, depression, and conduct difficulties. Phone call reminders for adolescents with perinatal depression increased their capacity to engage with treatment and motivated clinic attendance (Kola et al., 2022). MMH treatment was an added opportunity for adolescent mothers to engage with care.
All the studies reviewed reported various benefits of using MMH identified by adolescents such as cost-effectiveness and confidentiality. For example, Chandra et al. (2014) highlighted that SMS texting is a low-cost method for adolescents, as it does not require mobile data or access to a smartphone device. This is particularly advantageous in settings where more advanced mobile technologies, such as smartphones, are not accessible and affordable. Using a MMH platform with pseudonyms allowed participants to share their experiences openly without any fear of revealing their real identity. Participants reported that they could talk about difficult topics that they would not be able to discuss in other settings, such as stigma and mental health challenges, such as depression and anxiety (Chory et al., 2022). This finding is similar to that of Gonsalves et al. (2019). The latter study, participants reported that they felt supported by a blended problem-solving mobile game and felt safe sharing their problems within the game. In addition, participants in the study by Duan et al. (2020) also found the SMS text-messaging intervention beneficial as the messages they received encouraged them to self-reflect and stay calm. In Kola et al. (2022), the use of the MMH intervention reduced participants’ logistic challenges of face-to-face communication during their clinic visits.
Domain 2: access to mobile devices and other barriers impacting the use of MMH
One study conducted in India reported a low level of individual phone ownership, with many adolescents sharing their phones with their families (Chandra et al., 2014). Also in India, Gonsalves et al. (2019) reported the sharing of smartphone devices, where adolescents used devices that belonged to a parent, mainly fathers. In contrast, Maloney et al. (2020) reported that all but one participant in Jamaica had access to a mobile phone. A small number of participants in China believed that the SMS text messaging intervention would not be helpful because their parents limited their use and access to their mobile phones during the day (Duan et al., 2020). Chory et al. (2022) did not report mobile device ownership challenges among adolescents in Kenya, as all participants were provided with a smartphone for the duration of the study. Participants were allowed to keep their mobile phones after the research ended.
Five out of the six studies highlighted concerns raised by adolescents regarding their use of MMH, such as a lack of confidentiality, for two primary reasons: (1) sharing their devices with parents and (2) parents having access to their mobile devices (Chandra et al., 2014; Duan et al., 2020). As a result, adolescents felt that they would not benefit from the MMH interventions. For example, in Duan et al. (2020), parents of adolescents kept their mobile phones for them during most of the day, making it difficult for them to access text messages. Moreover, there was no confidentiality for the adolescents. This lack of confidentiality limited how adolescents engaged with mobile platforms and what they shared on these platforms.
Adolescents in the study by Gonsalves et al. (2019) speculated that concerns might arise from parents and teachers with the amount of time spent on their mobile phones. Adolescents also reported their caregivers as potential barriers to using MMH interventions as some caregivers did not understand why the participants were using their phones for longer periods (Chory et al., 2022). Participants identified household chores and school responsibilities as further barriers to MMH intervention participation. With household chores and schoolwork, adolescents had limited time to engage with the MMH interventions. Another common barrier to using MMH identified across all studies was data costs and/or access to the internet. Maloney et al. (2020) speculated, with no direct evidence, that adolescents might be unwilling to exhaust their mobile phone data on MMH resources. Rural participants had less frequent access to Wi-Fi compared to their peers in urban areas (Maloney et al., 2020). Participants in the study by Gonsalves et al. (2019) recommended that the MMH interventions should be accessible offline and available independent of internet access.
Domain 3: MMH content preferred by adolescents
Four out of the six articles reported specific preferences that the participants held for MMH interventions. In an SMS text messaging intervention, most participants preferred helpline messages rather than positive mood-lifting messages (Chandra et al., 2014). The helpline message encouraged them to call or text back if they felt angry, sad, or anxious. Many participants used the helpline to send text messages or calls when upset or angry (Chandra et al., 2014). The opportunity to text back or call someone was strongly preferred because it gave adolescents a sense of support and care. In a game intervention, participants preferred games with stories set in various real-world environments, with choices that could be explored (Gonsalves et al., 2019). Moreover, some participants indicated that online group sessions may help provide a sense of togetherness among users. This finding is consistent with Chory et al.’s (2021) study, where participants reported that WhatsApp group chats offered a feeling of community and peer support among adolescents. However, for more severe problems, participants preferred private chat functions as an option for counsellor support (Gonsalves et al., 2019). Similarly, participants reported that private chats with a counsellor helped them to discuss sensitive topics (Chory et al., 2021). Encouragement and company, meeting and communicating with friends online, providing coping strategies, and receiving individualised or tailored messages were some of the additional preferred content of participants in the study by Duan et al. (2020).
Discussion
This scoping review aimed to report on current evidence for MMH design, development or intervention for adolescents in LMICs. The scarcity of published research on this topic reflects the limited focus on adolescent mental health interventions in LMICs, despite increased mobile phone ownership and use in these countries (International Telecommunications Union [ITU], 2022). This also reflects that the field of MMH is a small but growing research area that dramatically increased due to the coronavirus pandemic, which required rapid advances in the use of MMH to deliver and ensure continuity of care (Bantjes, 2022). Nonetheless, the three domains identified provide insight into the perception and usefulness of MMH interventions. Adolescents in LMICs perceive MMH approaches as useful and a viable alternative to accessing mental health care, using various approaches for delivering and improving their mental health. However, barriers such as not owning or sharing a mobile phone, access to phones by parents, and mobile data and internet access may hinder adolescents from using MMH approaches. Adolescents’ perceptions of MMH approaches and barriers to MMH implementation, use, and acceptability will be explored in this section.
Adolescent users reported mobile health interventions to be beneficial in all of the research studies included in this review, though the reported benefits varied, based on the mobile health intervention used. Our review found that MMH interventions have the potential to overcome service access barriers, such as treatment costs and long waiting hours at clinics because they provided continuous low-cost access to care outside clinical settings. While adolescents perceive MMH interventions as useful, studies have reported high dropout rates in MMH interventions (Hall et al., 2022). Research by Välimäki et al. (2017) found that participants in the intervention group dropped out more often, showing that they may not have been fully engaged with the web-based interventions. User engagement was also reported as a critical challenge for mental health digital applications (apps), reporting a 4% user retention rate 2 weeks after the first download (Melcher et al., 2022). Bauer et al. (2020) reported limited downloads and poor retention in mental health apps, particularly outside of clinical trials and research settings.
The benefits reported by adolescents highlight the potential of MMH interventions to overcome not only access-related barriers but also confidentiality and stigma concerns associated with face-to-face treatment. Therefore, MMH interventions should ensure anonymity and confidentiality – for example, users should have the option to hide their identity. However, they should be able to consent to being identified by a professional counsellor if there is a suspected emergency or the user is in danger, for example, suicidal thoughts. Our findings are consistent with those of studies conducted in non-LMIC countries. In Seko et al. (2014), confidentiality and privacy were the youths’ commonly stated concerns. Similarly, 74% of US college students listed data privacy as their top concern for mental health apps (Melecher et al., 2022). While MMH shows potential for use in adolescents, challenges persist. For the MMH potential to be fully realised, critical issues, such as data protection and appropriate ethics and safety frameworks specifically for MMH still need to be considered.
The reviewed articles showed a trend in the use of text messaging and smartphone application interventions. Quotes and brief messages on positive well-being, encouragement and coping strategies are the types of messaging that adolescents seem to prefer in LMIC contexts. This can be attributed to the fact that SMS text messages would not require internet access. This is evident in the study by Kola et al. (2022). In the latter study, over 50% of adolescents indicated that they preferred receiving mental health information as text messages, while very few preferred such information as videos on cell phone apps. Similarly, Akinfaderin-Agarau et al. (2012) found that adolescents preferred SMSs. The most frequently cited reason by adolescents was that it is cheaper. Moreover, adolescents stated they can still receive SMS texts with a poor network connection. Adolescents highly rated a sense of community from a group chat, but they equally appreciated being able to chat with a counsellor privately. This is consistent with the finding from Liverpool et al. (2020). The latter study found that adolescents’ willingness to use the MMH intervention was influenced by the ability to connect with others. They found that adolescents were more likely to engage with the MMH intervention if it facilitated conversations with others because they wanted to know that others had similar experiences. While acceptability was generally favourable, the findings of this review highlight that implementing MMH interventions is not a ‘one size fits all’ process but rather requires a nuanced understanding of adolescent needs in particular communities. The design and development of MMH interventions should involve the end-users, paying attention to their preferences. Watson et al. (2023) emphasise the importance of engaging young people in making decisions for their health. Watson and colleagues recommend that young people should be included in all stages of the deliberative priority-setting process. Organisations such as WHO and the United Nations International Children’s Emergency Fund also acknowledge the importance of involving young people in making decisions concerning their health (Watson et al., 2023).
It is important to note that only one of the six studies designed and developed an MMH intervention. The rest of the studies used existing platforms such as WhatsApp or a short messaging service platform to deliver the intervention. The limitation of a different range of MMH interventions in LMICs is also evident when compared to literature from non-LMICs. For example, a review conducted by Liverpool et al. (2020) on engaging children and young people in MMH interventions in high-income countries identified six different interventions such as (1) apps, (2) virtual reality, (3) websites, (4) game and computer-assisted programmes, (5) robots and digital devices, and (6) text messaging, while our review only identified three, namely, SMS text messages, smartphone apps and digital games. This finding highlights a need for organically developed platforms tailored explicitly for adolescents and specific to their socioeconomic and cultural contexts. For this field to grow in LMICs, researchers need to explore adolescents’ preferences for MMH interventions in conjunction with a range of platforms.
Recent studies report widespread mobile phone ownership and use among young people (Nwaozuru et al., 2021). According to ITU’s (2022) latest report, 65% of individuals in LMICs own a mobile phone. According to a survey assessing mobile phone ownership in 24 developing nations, more than half of the population in each of the 24 countries owns a cell phone (Feroz et al., 2021). However, cell phone ownership, meaning full ownership with control of when and who gains access, is not reflected in our review, and this may partly be due to affordability (Chandra et al., 2014). Evidence from previous reviews of adolescent MMH has shown that mobile phone ownership overcomes privacy concerns, which is an important factor for adolescents (Feroz et al., 2021). In contrast, our findings show that phone ownership may actually be low among adolescents in LMICs and particularly among those who might benefit from MMH interventions. Sharing phones with family members or parents, and guardians having access to the adolescent’s phone was a common finding in our review, resulting in limited privacy for the adolescent. The privacy issue highlights the challenges adolescents may face with little autonomy and confidentiality in their homes. The issue of privacy is not unique to LMICs. These findings highlight the importance of MMH interventions being discrete and easy to hide to avoid the potential stigma attached to experiencing mental health. A review conducted by Grist et al. (2017) appraising the efficacy of MMH apps for adolescents, all developed in high-income countries, also reported privacy concerns, not related to parents but their peers having access to their mobile phones. According to Ben-Zeev et al. (2017), mobile health apps can be password protected and automatically log out after minutes of no use. Again, the importance of involving adolescents in the design and development of the MMH intervention is evident. The role of parents and caregivers should also be considered in overcoming these challenges. Adolescents value anonymity and confidentiality, and these must be considered, but there needs to be careful consideration of safety issues in case of an emergency, for example, a user showing signs of suicidal intentions. Sufficient IT resources are needed to handle, securely, such cases while maintaining anonymity and confidentiality where possible. Moreover, a dedicated counsellor should be available to offer support through counselling and provide important information to help users cope while waiting for a referral to mental health professionals.
Data costs appear to be the most common barrier to adolescents using MMH interventions in LMICs; this was reported across all six studies in our review. It is important to note that limited access to the internet may deter users from engaging with the MMH interventions. Ben-Zeev et al. (2017) found that participants may only engage with mobile health services if they are free or have Wi-Fi access. On the other hand, internet access was not reported as a barrier in high-income countries. Instead, young people in Australia, the United States and Hong Kong reported that they are online almost constantly (Ridout & Campbell, 2018). This finding warrants further research to develop context-specific interventions that understand local implementation challenges by involving adolescents across all stages of the design and development of any MMH interventions where they are end-users. Furthermore, while adolescents’ mobile phone use would allow access to MMH, constant mobile phone use has risks. Research by Girela-Serrano et al. (2022) investigating the impact of mobile phone use on children and adolescents shows an association between mobile phone use and depression, anxiety and behavioural problems. They add that ‘problematic smartphone use’ may be responsible for poor mental health (Girela-Serrano et al., 2022, p. 2). Future research is needed among LMIC adolescents to evaluate if the potential benefits of greater smartphone access for adolescents, including access to health services and support, outweigh the potential risks observed in high-income countries.
Strengths and limitations
A strength of this study was that we followed established guidelines for scoping reviews by Arksey and O’Malley (2005). Two independent reviewers were involved in the appraisal of the research studies and the findings contribute to the limited research available on MMH for adolescents in LMICs. One limitation of this research is that it is possible that other relevant publications were not included because only four electronic databases were searched for peer-reviewed sources. Moreover, sources written in languages other than English and grey literature were excluded. Therefore, our conclusions are based on a very small set of studies, and any conclusions offered are tentative.
Implications for future research
There is a lack of research on adolescent MMH in low-income countries. All six studies in our review were conducted in middle-income countries. Overall, the review points to the need for more research on adolescent MMH in LMICs. New theoretical and conceptual frameworks are needed to guide the design and development of MMH interventions. Future research should clearly state what was used and consider the medicolegal and ethical frameworks needed to support implementation. The studies included in the review were very brief, and thus, the results provided were based on short-term outcomes. Therefore, future research should focus on longitudinal studies to assess the long-term effects of MMH interventions. While MMH is a promising tool for improving adolescent mental health, there are potential risks associated with its use. Therefore, more attention should be devoted to minimum safety standards and data protection.
Conclusion
This review identified only six studies from five LMIC countries that reported the development or use of mobile health interventions for adolescent mental health. The results indicate that mobile technologies for adolescents are a promising tool in LMICs. However, the results highlight the importance of involving adolescents in the design and development process of MMH interventions, particularly around issues of access and privacy. Future research needs to broaden the scope to include preferred content highlighted by adolescents and consider the different aspects of mental health literacy, encouraging messages, and coping tools, among others. While MMH interventions are promising and show potential for addressing gaps in mental health care, they should not be considered the only solution for addressing the global burden of mental disorders. Instead, they should be used in combination with existing ways of providing care to complement and reinforce the services provided by therapists and trained health care professionals.
Footnotes
Acknowledgements
The authors would like to thank Mimi Mhlaba at Wits Health Hubb for her assistance with the screening of the articles.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received financial support for the research, authorship, and/or publication of this article from the National Research Foundation of South Africa (NRF) and the DSI-NRF Centre of Excellence in Human Development (CoE-Human) at the University of the Witwatersrand.