
Abstract
Background:
In resource-limited primary care settings, Digital Mental Health Training (DMHT) programs have emerged as scalable solutions to bridge the mental health care gap. It is essential to consider the views and perspectives of trainers, as they play a crucial role in implementing these programs.
Methods:
This qualitative study was conducted within the “Mutistate Digital Mental Health Capacity Building Program for Primary Healthcare” and explored the perspectives of 15 trainers from various professional backgrounds regarding DMHT via a Focus Group Discussion (FGDs). The transcript of the FGDs was thematically analyzed to identify key themes.
Results:
The study highlighted the effectiveness of hybrid training models in delivering mental healthcare. Such models incorporate the benefits of in-person sessions along with the scalability of online platforms. However, some notable barriers to DMHT programs included limited digital literacy among primary care providers, unreliable infrastructure, and competing participant responsibilities. It was found that for DMHT’s success, there is a need for culturally adapted content, interactive teaching methods, and sustained administrative support. Other recommendations included improving digital infrastructure, offering pre-training sessions to enhance digital literacy, and addressing structural barriers through policy changes.
Conclusion:
The DMHT programs can be viable solutions to improve mental healthcare delivery in low- and middle-income countries if supported by strong infrastructure, culturally relevant content, enhanced digital literacy, and ongoing administrative support.
Keywords
DMHT programs should incorporate trainers’ perspectives to support effective design and ensure sustained implementationKey Message:
It has been found that mental health disorders account for a large portion of the global disease burden, affecting more than 450 million people globally, many of whom do not receive access to necessary care. 1 In India, around 10.6% of the population faces mental health challenges, with a treatment gap of more than 75%. 2 An additional challenge is the shortage of trained mental health professionals in the country, particularly in rural areas, which leaves millions of people without adequate care and support. 3
In resource-constrained settings, task-shifting and task-sharing have emerged as effective strategies over recent years. These strategies help redistribute healthcare responsibilities among non-specialist health workers, addressing unmet mental health needs in rural and low-resource areas. 4 However, traditional training programs often employed to support task-shifting and task-sharing strategies face several challenges, including logistical barriers, limited scalability, and difficulties in applying acquired skills to clinical practice without continued support.5,6
In light of these challenges, Digital Mental Health Training (DMHT) strategies have emerged as viable solutions, enabling healthcare providers to receive digital training in addressing mental health needs. The DMHT offers scalable, cost-effective solutions that address geographical and logistical barriers, making it particularly suitable for low-resource settings. 7 A recent randomized controlled trial comparing online and hybrid models for primary care physicians highlighted improved engagement and learning outcomes in the hybrid format. 8 By leveraging technology, accessible training for non-specialist healthcare workers can enable efficient skill transfer and adaptability in resource-limited scenarios.9,10 For example, randomized controlled trials in India that have implemented technology-based task-shifting initiatives to train Accredited Social Health Activists (ASHAs) have shown that digital tools efficiently empower community health workers to manage mental health conditions. 11 Similar studies have demonstrated that DMHT programs for community health workers significantly improve their ability to identify mental disorders, reduce stigma, and boost confidence. 12 Our study examined the perspectives of trainers who participated in the “Multistate Digitally Driven Capacity-Building Program for Primary Mental Healthcare,” a Corporate Social Responsibility (CSR) initiative led by a multinational company. The program successfully trained 42,192 primary healthcare workers—medical officers, staff nurses/Community Health Officers (CHOs), and ASHA workers—across eight Indian states: Karnataka, Maharashtra, Goa, Telangana, Uttarakhand, Kerala, West Bengal, and Bihar. 13
Although several studies have documented the benefits of DMHT, the perspectives of trainers, key contributors to a program’s success, remain underexplored. Trainers can offer valuable insights regarding the design of the training program, the implementation challenges, and the practical application of digital tools.10,14 Therefore, their involvement is crucial for ensuring that non-specialist health workers, such as community health workers, can effectively adapt to DMHT. This research addresses this gap by exploring trainees’ experiences of DMHT through Focused Group Discussions (FGDs). The findings aim to inform the design and policy development of scalable and resource-efficient mental health training programs, especially in Low- and Middle-Income Countries (LMICs).
Methods
Study Design
This qualitative study used FGDs to explore trainers’ perspectives on implementing DMHT within the Multistate Mental Health Digital Capacity Building Program for Primary Healthcare. FGDs were chosen for their ability to uncover group dynamics, shared norms, and collective narratives that individual interviews might overlook.
Development of FGDs Guide and Pilot Testing
A semi-structured FGDs guide (See Supplementary Material 1) was developed based on a review of existing literature and inputs from three experts. The guide included 10 open-ended questions covering digital engagement strategies, perceived effectiveness, and barriers in DMHT. The guide was initially pilot-tested with two trainers who were not part of the final sample, and minor refinements were made based on their feedback.
Recruitment and Participants
Fifteen trainers, all actively engaged in a CSR initiative led by a multinational company, participated in the study. These trainers came from diverse professional backgrounds within the mental health field. Recruitment took place through targeted emails and invitations within the program’s network. All participants provided informed consent. Ethical approval was obtained from the Institutional Ethics Committee (IEC) at [Institution Blinded].
Data Collection
FGDs were conducted on May 6, 2024, and lasted approximately two hours. Participants provided informed consent and completed a socio-demographic questionnaire detailing their professional background, experience, and familiarity with digital training. Discussions were audio-recorded and transcribed verbatim. The lead author reviewed transcripts to ensure accuracy. Data saturation was assessed continuously and was reached when no new codes emerged during the final stages of transcription analysis.
Data Triangulation and Analysis
Data triangulation was achieved through investigator triangulation, where three coders independently reviewed and interpreted the data, resolving any discrepancies through discussions to reach a consensus. Inter-rater reliability was not formally calculated. Thematic analysis, guided by Braun and Clarke’s six-phase framework, identified explicit and implicit patterns, providing a detailed understanding of factors influencing DMHT effectiveness. 15
Results
Table 1 displays the participant demographics.
Participant Demographics.
*Mental health professionals included psychiatrists, clinical psychologists, psychologists, psychiatric social workers, medical social workers, and psychiatric nurses.
Qualitative Findings
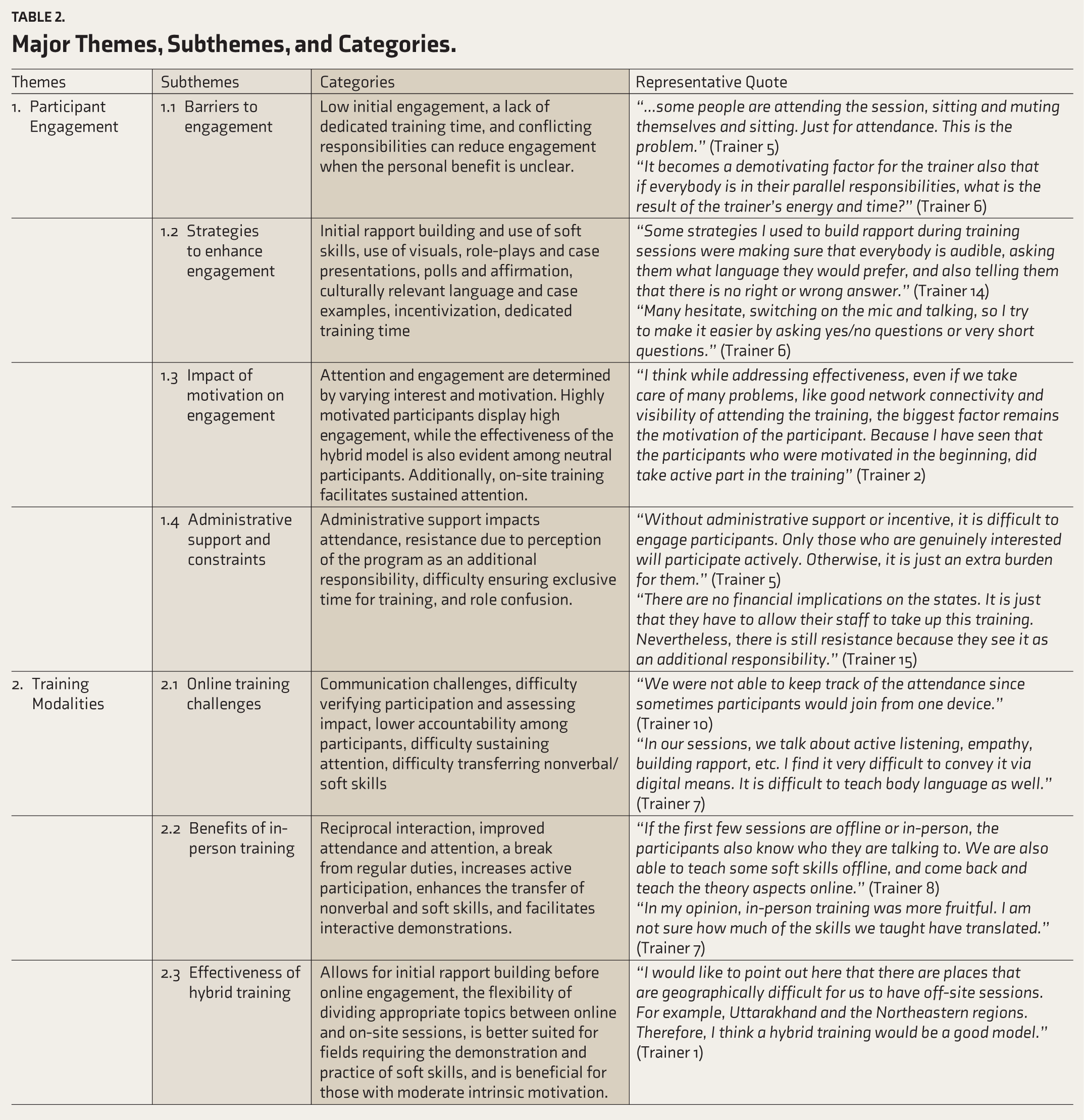
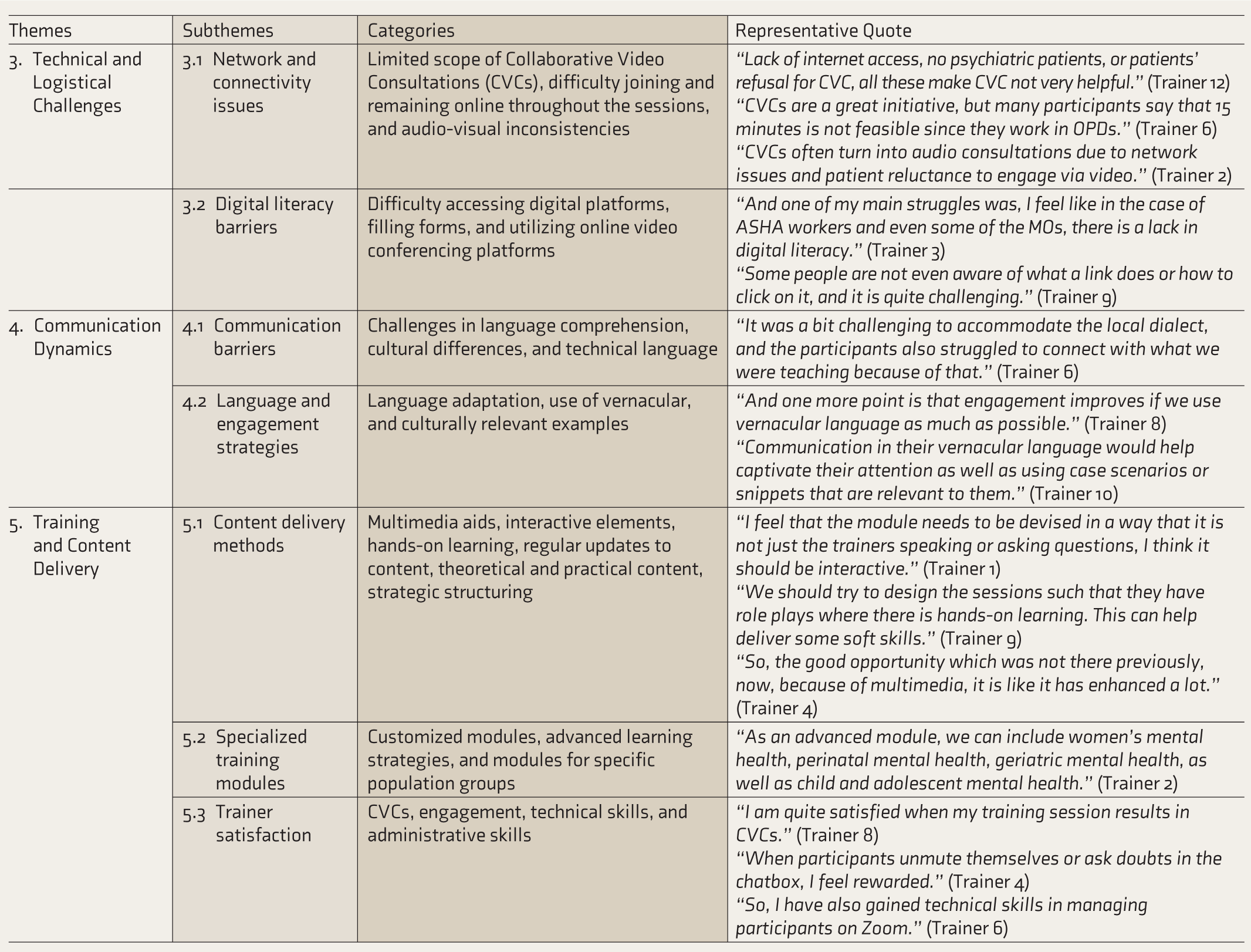
The findings revealed five major themes: participant engagement, training modalities, technical and logistical challenges, communication dynamics, and training and content delivery, as listed in Table 2.
Major Themes, Subthemes, and Categories.
Theme 1. Participant Engagement
Participant engagement emerged as a key theme, encompassing attendance, active involvement in discussions, sustained attention, and practical application of skills. Personal, contextual, and systemic factors influenced engagement.
Barriers to Engagement
Trainers identified various barriers to fostering active participation in DMHT, including logistical constraints, competing professional responsibilities, and participant attitudes. The digital format often exacerbates these challenges by making it more difficult to sustain attention and verify participation. Participants frequently struggled to balance training with their existing responsibilities, resulting in minimal engagement. In some cases, attendance was seen as a formality rather than an opportunity for professional growth.
“The difficulty I have faced mostly is engaging in a conversation. If it is face-to-face, it’s easier to have a conversation, clear up doubts, or address any other issues. However, in an online platform, I feel like it is difficult to engage the participants.” (Code 2)
“In a batch of 25–30, around 2–3 would join after repeated messages, after calling the district coordinator or the doctors. And multiple calls later, 2–3 would also be doing some other work.” (Code 9)
Strategies to Enhance Engagement
Trainers implemented innovative strategies to foster engagement and bridge the gaps created by digital formats. These included interactive techniques such as tele-mentoring with role-plays and case presentations, the potential use of virtual reality, and adapting communication to participants’ preferences, such as using short questions via chat.
“Using tele-mentoring for more role plays and more case presentations works in engaging people more.” (Code 33)
“Many hesitate, switching on the mic and talking, so I try to make it easier by asking yes/no questions or very short questions.” (Code 70)
“Some strategies I used to build rapport are ensuring they are comfortable with the language, emphasizing there are no wrong answers.” (Code 73)
“There is no small or silly doubt they can feel free to ask questions, so that helps in making the sessions interactive.” (Code 74)
Administrative Support and Constraints
Administrative challenges were seen as significant barriers to DMHT implementation. Inconsistent support from state agencies, resistance from officials, and competing priorities at the district level were recurring issues.
“There are no financial implications for the states. It is just that they have to allow their staff to take up this training. Nevertheless, there is still resistance because they see it as an additional responsibility.” (Code 114)
“So, there has been some amount of problem where exclusive time for training is not being given due to competing priorities at the district level.” (Code 115)
Confusion over roles, such as expectations for institutions like [Institution Blinded] to implement state policies, further complicated administrative processes.
“In continuation with that, sir, I mean, now there is an expectation from Karnataka that [NIMHANS] should come and implement these state policies, which is creating a bit of role confusion.” (Code 238)
Systemic challenges extended to clinical settings, characterized by a lack of patient privacy during consultations and insufficient incentives for participants.
“There was one more concern from CHOs during the consultation, as patients were uncomfortable discussing their personal history because of a lack of privacy.” (Code 239)
“I think it is normal human nature. First of all, they think what is in it for them, and if it is just a certificate, it does not work much.” (Code 247)
Administrative Support and Constraints
Administrative support or constraints were found to influence participant engagement significantly. Trainers observed that participant motivation and attendance improved when district health officers or hospital administrators were actively involved in prioritizing mental health training for community healthcare workers, such as by providing protected time for training or temporarily relieving them of duties. However, in several instances, the absence of such support led to scheduling conflicts and a diminished perceived importance of the training.
“Only when the DHO told them, they came.” (Code 260)
“We had to call the medical officer and ask them to relieve the staff for training.” (Code 262)
The findings underscore the importance of implementing robust administrative strategies, including more effective resource allocation, clearer roles, and tangible incentives, to support the development and implementation of effective DMHT programs.
Theme 2: Training Modalities
Training modalities explore the diverse delivery methods of DMHT, including online, in-person, and hybrid formats. Each modality presents distinct benefits and challenges that influence the effectiveness of training.
Online Training Challenges
Online training poses significant challenges, particularly in communication and participant engagement. Trainers often find it challenging to resolve doubts and provide effective feedback when face-to-face interaction is absent.
“Face-to-face training allows easier communication and doubt resolution compared to online.” (Code 3)
“Struggles with conveying tone and feedback in online training, leading to perceived harshness.” (Code 4)
The inability to assess participant engagement due to muted audio and video further limits interaction and accountability.
“Challenge of verifying participant engagement due to muted audio and video during online sessions.” (Code 19)
“Lack of personal connection reduces participant accountability, impacting the quality of the training.” (Code 22)
While online training offers flexibility and accessibility, trainers note that attention tends to drift more frequently in online formats compared to in-person sessions.
“Attention tends to drift during online training, a challenge not as prevalent in offline sessions.” (Code 150)
Benefits of In-person Training
In-person training provides several advantages, particularly in fostering interaction and immediate feedback. It enables dynamic engagement and is effective for teaching soft skills and interview techniques.
“Offline training enables real-time demonstration and practice of skills, improving understanding of diagnosis and screening tools.” (Code 139)
Additionally, in-person settings offer participants a break from routine duties and the incentive of travel allowances, increasing their appeal.
“On-site training provides participants with a break from regular duties, increasing appeal through time away and travel allowances.” (Code 95)
Role plays and real-time demonstrations, which are less effective in online setting, tend to be more engaging and informative in in-person formats.
“On-site training allows better engagement through role plays, which is lacking in online formats.” (Code 67)
Effectiveness of Hybrid Training
Hybrid models combine the strengths of online and in-person formats, enabling rapport-building through in-person sessions followed by flexible, scalable online components.
“Hybrid model allows rapport-building in-person, followed by online theoretical training.” (Code 135)
This approach is efficient for fields that require an understanding of emotions and behaviors, which cannot be fully addressed through online learning.
“Hybrid training better suits fields requiring understanding of emotions and behaviors, which cannot be diagnosed solely through symptoms.” (Code 136)
Hybrid models also enhance the teaching of practical skills, such as interview techniques, and allow for strategic division of content across formats.
“Different skills and knowledge should be divided between online and on-site formats to maximize effectiveness.” (Code 142)
Training modalities must be tailored to the curriculum’s specific requirements and participants’ learning styles. While online training offers scalability and convenience, in-person formats enhance interpersonal skill development. Hybrid models effectively balance these strengths, making them a promising approach for delivering impactful DMHT programs.
Theme 3: Technical and Logistical Challenges
Technical and logistical challenges significantly impact the effectiveness and accessibility of DMHT. These challenges, including network issues and digital literacy barriers, disrupt learning processes and hinder participant engagement, highlighting the need for adaptive strategies to ensure effective training delivery.
Network and Connectivity Issues
Network instability is a significant technical barrier that compromises the potential benefits of DMHT. Collaborative Video Consultations (CVCs), designed to facilitate interactivity and real-time learning, are often degraded or rendered infeasible due to poor network infrastructure.
“CVCs are not in those great numbers.” (Code 7)
“CVCs often turn into audio consultations due to network issues and patient reluctance to engage via video” (Code 201)
Despite their limitations, audio consultations remain valuable for developing interviewing skills by exposing participants to professional interactions with distressed patients.
“Even audio consultations can be effective if the patient is willing to engage. These interactions allow patients to connect with professionals and also provide an opportunity for the healthcare provider, such as the CHO or doctor, to learn new skills indirectly.” (Code 202)
Participants frequently face difficulties joining or staying connected to training sessions due to unreliable networks, which are compounded by poor audio quality that reduces engagement and interaction.
“Cannot join or stay in sessions due to network issues.” (Code 249)
“Cannot hear clearly and engage due to network issues.” (Code 250)
Digital Literacy Barriers
Digital literacy gaps, particularly among community health workers, such as ASHA workers, CHOs, and some medical officers, present another critical barrier. Limited familiarity with digital tools and basic functionalities significantly hinders effective participation.
“And one of my main struggles was, I feel like in the case of ASHA workers and even some of the MOs, there is a lack in digital literacy.” (Code 63)
Instances of participants struggling with basic tasks, such as activating links, further highlight the challenges posed by limited digital proficiency.
“Some people are not even aware of what a link does or how to click on it, and it is quite challenging.” (Code 64)
This lack of proficiency often results in hesitancy to engage actively, particularly in sessions requiring interaction, such as medical officer guidance sessions.
“Whereas, coming to the engagement of the participants, they are hesitant in asking questions even during medical officer guidance sessions.” (Code 68)
The combination of network connectivity issues and digital literacy barriers underscores the multifaceted challenges in deploying effective DMHT programs. Addressing these issues through infrastructure improvements and foundational digital literacy training is essential to ensure that DMHT is accessible and impactful for all participants.
Theme 4: Communication Dynamics
Communication dynamics examines the challenges and strategies involved in fostering effective communication in DMHT. Barriers such as language proficiency, communication styles, and the absence of non-verbal cues can impact engagement and understanding, necessitating thoughtful and inclusive strategies to enhance interaction.
Communication Barriers
Communication barriers in DMHT significantly hinder engagement and effectiveness. Complex technical language in tele-mentoring settings often alienates participants, reducing their involvement.
“We learn in adult learning that these realistic scenarios should be there, but again, if it is becoming too technical, people tend to disengage.” (Code 30)
Language proficiency issues further complicate communication, with participants’ varying levels of proficiency impacting their ability to comprehend and engage.
“It was a bit challenging to accommodate the local dialect, and the participants also struggled to connect with what we were teaching because of that.” (Code 58)
Written communication often leads to misinterpretation due to the inability to convey tone or intent, a common challenge in digital settings.
“Even when we are not training them to that level, sometimes they misinterpret what we write because they cannot see our face or hear our tone.” (Code 119)
Differences in communication styles between trainers and participants, along with the absence of non-verbal cues, create additional barriers to effective learning and interaction.
“Picking up, making a diagnosis, and recommending a course of action – all these are difficult without non-verbal cues.” (Code 131)
Cultural differences also influence the effectiveness of communication, impacting how messages are perceived and understood.
“So, I think through them, we are somewhere tackling cultural differences as well.” (Code 128)
Language and Engagement Strategies
To overcome these barriers, trainers have implemented strategies that focus on inclusive and adaptive communication. Using vernacular languages makes content more relatable and accessible, improving engagement.
“And one more point is that engagement improves if we use vernacular language as much as possible.” (Code 103)
Learning basic local languages helps trainers connect better with participants, especially community health workers.
“Just like my colleague, even I started learning a bit of Marathi, which has helped me connect better with ASHA workers.” (Code 222)
Tailoring content to reflect participants’ cultural contexts and language preferences significantly enhances understanding and engagement.
“So, something that I have realized is, one thing that has worked is using culturally relevant examples.” (Code 220)
Effective communication is pivotal to the success of DMHT programs. Addressing language barriers, adapting to diverse linguistic and cultural contexts, and using thoughtful communication strategies enhance participant engagement and improve training outcomes. These approaches ensure that digital training is inclusive, impactful, and aligned with participants’ needs.
Theme 5: Training Content and Delivery
Training content and delivery examines how training materials are structured and presented in DMHT programs. This theme highlights the influence of delivery methods, specialized training modules, and trainer satisfaction on learning outcomes and the overall training process.
Content Delivery Methods
Effective content delivery is critical for engaging participants and ensuring knowledge retention. Multimedia tools enhance understanding by presenting information in diverse, accessible ways.
“So, the good opportunity which was not there previously, now, because of multimedia, it is like it has enhanced a lot.” (Code 28)
Interactive elements, such as quizzes, diagrams, and collaborative tasks, further boost engagement and participation.
“Okay, I am working here as a trainer, engaging them with some quizzes, some videos.” (Code 39)
Trainers also structure content to maintain interest, segmenting material into manageable parts based on participant feedback to refine their methods.
“One thing I did was, like, I noted down the points where people seemed to lose interest and restructured the content.” (Code 69)
“If you are starting only with the complicated aspects, it might not work. So, incorporating their feedback has been key.” (Code 76)
Real-life case studies and hands-on simulations are integrated to provide practical insights, making the training more relevant and enhancing retention.
“But rather tell like, list out one, even if it is just one real-life case study, which is very interesting.” (Code 71)
“This is not just me teaching. They can also learn by doing, which is through simulations.” (Code 77)
Balancing theoretical knowledge and practical application ensures the content meets diverse learning preferences and needs.
“We focus on building a strong foundation in patient communication through theory, but balancing this with practical application is also important. Online mock drills can support diverse learning needs, though conveying body language and non-verbal cues remains a challenge in virtual settings.” (Code 84)
Specialized Training Modules
Specialized training modules cater to specific skills and knowledge areas, such as domestic violence and adolescent mental health, fostering deeper learning.
“Regarding the content of the training program, it should be customized for specific skills.” (Code 233)
“As an advanced module, we can include women’s mental health, perinatal mental health, geriatric mental health, as well as child and adolescent mental health.” (Code 236)
Tailored content aligns with participant needs, ensuring relevance and effectiveness. Advanced strategies address unique demands across diverse groups, enhancing engagement and learning outcomes.
“The comment from the MOHFW was, Karnataka needs more advanced strategies in these modules.” (Code 237)
“So, the attitude just kept being different from the traditional methods, which was tailored according to their needs.” (Code 245)
Trainer Satisfaction
Trainer satisfaction is influenced by the effectiveness of training delivery and the level of participant engagement. Successful learning experiences, such as effective CVCs, contribute significantly to trainer motivation.
“I am quite satisfied when my training session results in CVCs.” (Code 48)
However, challenges like low attendance, participant disengagement, and distractions can lead to frustration.
“And in the terms of a trainer, frustration would occur when, despite all the efforts, there is no proper engagement.” (Code 51)
“It might as well become a demotivating factor for us as trainers when they are distracted by other responsibilities.” (Code 112)
Trainers gain satisfaction from developing digital platform management and administrative skills, which enhance their ability to deliver training effectively.
“So, that will be very beneficial. So, I have also gained technical skills in managing participants on Zoom.” (Code 218).
“Adding to that, another important skill I would say is administrative skills by interacting more with healthcare officials.” (Code 219)
Training content and delivery are crucial to the success of DMHT programs. Integrating multimedia tools, interactive elements, and tailored modules can enhance participant engagement and learning outcomes. Addressing challenges that affect trainer satisfaction is equally important to maintaining the quality and effectiveness of these programs.
Discussion
The current study’s findings offer a novel perspective on DMHT for primary care providers in resource-limited settings. Although short-term mental health training programs for community health workers have been shown to improve knowledge, attitudes, and skills and boost their confidence, leading to better clinical practices and patient outcomes, they also present significant challenges that must be addressed. 16 These findings are consistent with previous studies, such as the MANashanti Sudhar Shodh Trial, which demonstrated the effectiveness of training lay health workers in delivering mental health interventions in Indian primary care settings. 17
One significant barrier to DMHT programs that emerged during the FGDs was the challenge for participants (community health workers) in balancing their professional responsibilities with the demands of digital training. This was particularly challenging when training sessions overlapped with their active-duty or OPD hours, often limiting their ability to fully engage in the training sessions. This aligns with the Unified Theory of Acceptance and Use of Technology framework, which suggests that effort expectancy and facilitating conditions can significantly affect user engagement with digital tools. 18 Among these, digital literacy-related challenges stood out as the most significant impediment. Trainers reported that several participants, especially those from rural regions, were unfamiliar with basic digital functions, such as logging into the platform and accessing online resources. Some of them did not have personal email addresses or smartphones, making it difficult for them to log in during training. These gaps made them dependent on peers, affecting independent engagement. These findings are consistent with prior research indicating that digital literacy is a critical step in ensuring that rural communities are not left behind in the digital era. 19 Therefore, solutions must be tailored so that participants are offered flexible timings or asynchronous options, ensuring that the training hours do not coincide or interfere with their essential professional duties. 20 Dedicated pre-training digital orientation sessions, easy-to-use interfaces, and support systems that can guide participants through digital platform setups and navigation are the need of the hour. Future programs must invest in scalable digital literacy modules that are tailored to the needs and constraints of frontline workers.
Although DMHT programs can provide the flexibility and accessibility that traditional training programs lack, they can be an effective training strategy only when the training content aligns with participants’ immediate needs and long-term professional goals. This highlights the need to develop training programs that are context-sensitive and participant-focused. Incorporating interactive and multimedia content in the local language, along with the integration of realistic case studies and role-play exercises into the training material, can provide participants with practical insights into mental health disorders while promoting active participation. According to the Technology Acceptance Model, perceived usefulness plays a significant role in determining whether users accept and engage with digital platforms. 21 Trainers also noted that participants who perceived the training as relevant to their clinical duties were likely to engage more actively. Participant motivation can further be amplified through certificates, recognition, and institutional encouragement, highlighting the role of extrinsic incentives in digital learning environments. 22 Institutional or organizational support is another essential component that needs to be considered while overcoming challenges, such as time constraints and overlapping priorities. These findings align with the “Inner Setting” domain of the Consolidated Framework for Implementation Research. This highlights the importance of organizational readiness and support for successful implementation. 23 Therefore, organizations and institutions must actively support training initiatives by providing access to technology and resources, as well as incentives (such as certificates and financial rewards), and flexible training schedules to enhance participant engagement.
Additionally, hybrid training programs that integrate in-person and online sessions were seen as a promising solution for improving the effectiveness of DMHT. Studies have highlighted the flexibility and effectiveness of hybrid formats, which include initial in-person sessions to build rapport with participants, followed by flexible and accessible online components for continued learning. 13 The trainers in our study stressed the importance of hybrid mental health training sessions. Besides imparting theoretical knowledge, hybrid training models facilitate skill transfer through role-plays and soft skills training, enabling participants to apply their learning effectively in real-life settings. 24 While in-person sessions encourage collaboration and peer learning through group discussions, teamwork, and immediate feedback from the facilitator, the online component provides a platform for participants to stay connected and continue learning via online forums, webinars, and other digital tools. Feedback-informed modifications have been found to enhance both participant engagement and trainer delivery quality concerning digital training programs. 25 This blended approach helps sustain engagement and strengthens the overall learning experience. Moreover, hybrid training addresses other contextual challenges, such as limited time, space, or resources, as it minimizes the need for continuous in-person attendance. This can be particularly advantageous for community health workers and primary care providers in resource-constrained areas, where travel and time constraints often hinder participation, as is commonly seen in traditional training formats. Emerging Indian research reports positive outcomes from blended models that combine in-person training and tele-mentoring to upskill CHOs and MHLPs. 26 The trainers also highlighted the technical and logistical challenges, such as poor connectivity and gaps in digital literacy, that hinder participants’ full engagement in DMHT programs. These highlight the systemic inequities in accessing digital training content. Such challenges are especially pronounced in rural and resource-limited settings where necessary infrastructure is lacking, making it difficult for community healthcare workers to participate effectively. This barrier is especially evident among nursing staff and frontline health workers from rural Primary Health Centres (PHCs) who struggle with basic platform use and login procedures. Peer learning, culturally localized tutorials, and straightforward onboarding guides can be effective support strategies. Such challenges reflect a broader issue across India’s healthcare sector, where more than 50% of healthcare workers report having no formal training in digital health. Additionally, rural areas frequently experience power cuts and poor internet connectivity, which negatively impact digital service delivery. 24 Initiatives like Chhattisgarh community mental healthcare tele-mentoring program (CHaMP) have demonstrated that technology-based task-shifting programs can effectively address gaps in mental healthcare delivery when supported by adequate infrastructure and training, particularly for non-specialist healthcare workers.25,27 Several studies on ASHA training programs have emphasized the importance of improving digital literacy among community health workers to enhance engagement and effectiveness. 11 Systemic interventions, such as investments in digital infrastructure and incorporating digital literacy training into the DMHT curriculum, are essential in addressing these inequities. These efforts align with global initiatives aimed at closing the gap in healthcare education. 23
The study also highlighted other systemic issues affecting trainer satisfaction, such as the lack of institutional recognition and support. Trainers can experience frustration and demotivation when their efforts fail to yield meaningful outcomes. This underscores the need for reforms at the administrative level that prioritize trainer well-being. Institutional support, including dedicated training time and incentives provided by administrators, can encourage participation. Programs that clearly outline the roles and responsibilities of trainers and participants, along with continued administrative support, are more likely to achieve higher levels of engagement and effectiveness. 25
Communication strategies also emerged as a crucial factor in DMHT’s success. Incorporating vernacular language and culturally relevant examples into training sessions can enhance inclusivity within the training content, particularly in a multicultural country like India. Several studies that have integrated local languages and culturally specific case studies in their programs have underlined the need for tailored training content that is culturally and linguistically relevant to enhance its impact. 12
Last, trainer satisfaction was closely linked to the long-term success of DMHT programs. Insights from the FGDs suggest that incentives, such as certifications and skill development opportunities, enhance trainer motivation. 28 Along with providing tangible rewards that can help boost trainer morale, it is also important to establish feedback loops where trainers can share challenges and collaboratively develop solutions with administrators, which can, in turn, build a supportive training ecosystem. Such systemic changes are crucial for maintaining the long-term effectiveness of these programs. Moreover, trainers emphasized the importance of designing sustainable and low-cost programs for long-term impact, leveraging existing government e-learning platforms (e.g., National Health Mission (NHM) modules), ensuring content compatibility with low-bandwidth scenarios, and using a rolling trainer model to minimize recurring expenses. These suggestions also align with an Indian pilot case study assessing digital training costs, which found that 62% of the expenditures went into human resources, underscoring the value of scalable and cost-efficient strategies. 29
Limitations
The study offers valuable insights into the perspectives of trainers involved in a national DMHT program; however, several limitations must be acknowledged. The sample was limited to15 trainers from a specific CSR-driven implementation program, which limited the transferability of the findings across different contexts in India. Given the diversity of India’s healthcare landscape, it is possible that perspectives from underrepresented regions have not been adequately captured. Another limitation that needs to be highlighted is the absence of inter-rater reliability measures. While the researchers conducted multiple discussions to reach consensus on the themes, formal inter-rater reliability was not conducted. Future studies could strengthen the methodological rigor by incorporating inter-rater checks.
Conclusions
This study offers novel insights into the potential of DMHT programs from the perspective of trainers, highlighting their role in bridging gaps in mental healthcare delivery, particularly in low-resource settings. The findings demonstrated both the opportunities and challenges of digital health education, aligning with global experiences during the COVID-19 pandemic. Effective DMHT programs require a comprehensive approach that integrates advanced digital tools for interactive learning, adopts inclusive communication strategies to address cultural and linguistic diversity, and establishes strong systemic support to sustain engagement and application. It is also crucial to address barriers such as digital literacy gaps and inadequate infrastructure through targeted investments and pre-training modules, ensuring equitable access. Additionally, prioritizing training well-being and recognition is equally important for the success of DMHT programs. Offering incentives, professional development opportunities, and resilient feedback mechanisms are also important factors to consider in maintaining trainer motivation and improving DMHT program outcomes. DMHT programs can overcome the limitations of traditional in-person digital training by adopting a holistic approach and ensuring that the skills acquired are translated into better health practices and patient outcomes. The current study contributes to the growing body of evidence supporting DMHT as a scalable solution for enhancing mental healthcare in resource-constrained settings.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
Same as the “Introduction ” article of this issue (Indian J Psychol Med. 2026;48(1 suppl)).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Author Channaveerachari Naveen Kumar is the Principal Investigator of this project and supplemental issue. The author did not take part in the peer review or decision-making process for this submission and has no further conflicts to declare.
Declaration Regarding the Use of Generative AI
During the preparation of this work, the authors used ChatGPT, a language model developed by OpenAI, and Grammarly, a digital writing assistant, to assist with drafting, refining, and proofreading the manuscript. After using these tools, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Ethical Approval
The study was approved by the IEC (Approval No. NIMHANS/ 43rd IEC (BEH.SC.DIV) 2023, dated 8th December 2023) and registered with the Clinical Trial Registry of India (Registration No. CTRI/2024/02/062906).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The pan India training program was funded by a multinational company’s CSR grant.
Informed Consent
Informed consent was sought from all participants – including the primary healthcare workers and patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.