
Abstract
Background:
Cognitive deficits in bipolar affective disorder (BPAD), particularly during manic episodes, are well-documented. However, research on domain-specific memory impairments in bipolar mania is limited, especially in the Indian subcontinent. This study aimed to assess memory impairments in individuals with bipolar disorder using the Postgraduate Institute Memory (PGI-Memory) scale and to highlight domain-specific deficits compared to healthy controls.
Methods:
This cross-sectional study was conducted at a tertiary care center in North India. Twenty subjects diagnosed with bipolar mania and 20 age, sex, and education-matched healthy controls between the ages of 18 and 40 were recruited. Memory functions were assessed using the PGI-Memory scale. Mental control and working memory were also evaluated.
Results:
Both groups were matched in terms of age, sex, and education. Individuals with bipolar disorder demonstrated significant deficits in various memory domains, including immediate (d = 1.47), recent (d = 0.93), remote (d = 1.58), long-term (d = 2.37), and associative memory (similar pairs: d = 1.4, dissimilar pairs: d = 1.84,), as well as in visual reproduction (d = 2.3) and recognition tasks (d = 1.54). In contrast, their working memory performance was comparable to that of the control group. The largest deficits were observed in long-term memory, visual reproduction, and associative memory.
Conclusions:
Bipolar mania is associated with widespread memory impairments, particularly in long-term and associative memory, which may contribute to difficulties in emotional regulation and daily functioning. These findings emphasize the importance of considering memory impairments in the diagnosis and management of BPAD. Further studies are required to investigate the neurobiological foundations of these impairments and to develop specific interventions.
There are significant domain-specific memory impairments in individuals with bipolar disorder, particularly in visual and verbal memory, episodic memory, mental control, and associative learning, emphasizing the cognitive challenges these individuals face. The findings underscore the importance of considering these cognitive deficits in both the diagnosis and therapeutic management of bipolar disorder, enhancing treatment precision and patient care.Key Messages
Bipolar affective disorder (BPAD) is a chronic, recurrent, and highly debilitating mental health condition characterized by alternating mood states—mania and depression—that vary in severity and duration.1,2 These fluctuations complicate both diagnosis and treatment. 2 The study on the worldwide burden of diseases estimates a 0.6% prevalence of BPAD in India, 3 with its global lifetime prevalence reaching up to 2.4%, 4 leading to significant emotional, social, and economic impacts. Individuals with BPAD may spend nearly half their lives in either manic or depressive episodes, underscoring the need for comprehensive clinical attention to both poles of the disorder. Mania, a defining feature of BPAD, is characterized by elevated or irritable mood, excessive energy, increased activity, and impulsive behavior. 5 These symptoms often lead to impairments in cognitive and emotional functioning, affecting work performance, academic pursuit, and social relationships. 6 Individuals experiencing mania may exhibit increased distractibility, impaired judgment, and disorganized thinking, all of which can complicate daily functioning.7–9
Cognitive impairments are commonly observed in BPAD, particularly during manic episodes.10–13 Studies have identified deficits in executive functioning, including cognitive flexibility and decision-making, that manifest during acute mania.14,15 Moreover, individuals with mania tend to show more pronounced impairments in verbal and working memory, executive functioning, reasoning, and problem-solving than those who are depressed or euthymic. 16 These cognitive deficits often correlate with the severity of the illness and the number of manic episodes experienced. 16 Although certain impairments—particularly in working memory—may persist into remission, 14 many other deficits improve once acute symptoms subside. 17 Nevertheless, about one-third of the individuals may continue to experience persistent cognitive dysfunction even during the euthymic phase. 17
Memory is not a unitary construct. Instead, it comprises multiple systems with varying storage durations and capacities.18,19 Research consistently shows impaired verbal learning and memory in both acute and remission phases of BPAD.20,21 During acute mania, working memory deficits are commonly reported and may persist during the period of remission, 14 while findings related to other cognitive domains have been mixed. Notably, verbal retrieval deficits appear to be stable vulnerability indicators, whereas encoding deficits seem specific to mania. 22 A meta-analysis found moderate-to-large impairments across cognitive domains in euthymic individuals, particularly in verbal learning and delayed memory. 21 Additionally, deficits in autobiographical memory and episodic specificity are observed in bipolar depression. 23 In contrast, mania may be associated with hypermnesia, wherein memories surface rapidly and in overwhelming qualities. 23
Despite these observations, our understanding of which specific memory domains are predominantly impacted during manic episodes remains incomplete. Clarifying the pattern of memory impairments could enhance insight into the underlying pathology and guide the development of targeted psychotherapeutic interventions. Therefore, this study aimed to investigate domain-specific memory impairments in individuals with bipolar mania (BM).
Methods
A cross-sectional study was carried out from January 2012 to April 2013 at Central Institute of Psychiatry, Ranchi, Jharkhand, India, using a convenience sampling approach. The study received approval from the Institutional Ethics Committee, written informed consent was obtained from all participants, and all procedures were conducted in accordance with the principles outlined in the Declaration of Helsinki. The study included 20 subjects diagnosed with BM and 20 healthy controls (HC) matched for age and sex. Individuals with bipolar disorder were recruited from the inpatient services of the hospital, whereas HC were selected from the general population. The control group consisted of age- and sex-matched healthy individuals without any personal or family history of psychiatric disorders. These participants were recruited from hospital staff, their family members who met the inclusion criteria, and bystanders unrelated to patients from inpatient or outpatient services.
The study initially aimed to include 42 participants to identify a large effect size (Cohen’s d = 0.80) with a statistical power of 0.80 and an alpha level of P < .05. This anticipated large effect size was based on prior literature indicating significant cognitive impairments in individuals with BM compared to HC.24–26 The software G*Power 3 was used for this sample size estimation.27,28 However, the final sample included only 40 participants. To evaluate whether this sample size was still sufficient to detect the anticipated effect size, a post-hoc power analysis was performed using the actual sample size and the observed effect size. This analysis yielded a statistical power of 0.81 with an alpha level of 0.05, confirming that the sample size remained adequate to detect the observed effect.
Individuals diagnosed with BPAD according to the International Classification of Diseases—Diagnostic Criteria for Research (ICD-DCR) criteria, 29 who were currently experiencing a manic episode lasting at least two months, with or without psychotic features, and had a Young Mania Rating Scale (YMRS) score greater than 15, were recruited for this study. While the diagnostic criteria specify a minimum duration of one week, we extended this duration to two months to ensure symptom stability and reduce the influence of rapid mood fluctuations on cognitive assessments, aligning with standard methodological practices.30,31 Both male and female participants were eligible if they met the following criteria: aged between 18 and 30 years; right-handed; with a minimum of 8–10 years of formal education; literacy in English or Hindi; and an Intelligence Quotient (IQ) above 70, as assessed by the Wechsler Abbreviated Scale of Intelligence (WASI). Additionally, participants were required to be on stable medication for the preceding month and were not using benzodiazepines.
The subjects were excluded if they had experienced more than one prior manic episode or presented with any other Axis I psychiatric disorder—including substance dependence (excluding nicotine)—intellectual disabilities, or identifiable neurological conditions such as epilepsy or dementia. Those with a history of head injury or who had received electroconvulsive therapy (ECT) within the past four months were also excluded to avoid confounding neurocognitive impairments. Multiple manic episodes were considered an exclusion criterion since an increased number of such episodes correlates with poorer cognitive performance, especially in verbal learning and memory.32,33
Individuals with bipolar disorder were assessed using the YMRS, 34 while HC were evaluated with the General Health Questionnaire–12 (GHQ-12). 35 The Edinburgh Handedness Inventory 36 was administered to both groups. IQ was assessed using the WASI, and only subjects with an IQ greater than 70 were included in the study. 37 This IQ assessment served strictly as a screening tool to ensure eligibility for the neuropsychological battery. All IQ and memory assessments were administered by registered clinical psychologists on the research team, ensuring standardized and professional evaluation. The Postgraduate Institute Memory (PGI-Memory) scale was used to assess multiple memory domains, including visual retention, immediate and delayed recall, recent memory, and remote memory, in accordance with the domains recommended by the International Society for Bipolar Disorders—Battery for Assessment of Neurocognition (ISBD-BANC). 38
The YMRS is widely utilized to assess the severity of mania and was developed by Young et al. 34 The YMRS is an 11-item instrument designed to assess the severity of manic symptoms in subjects already diagnosed with mania. It relies on the subjects’ self-reported clinical condition over the past 48 hours, supplemented by clinical observations made during the interview. The scale includes four items rated on a 0 to 8-point scale—irritability, speech, thought content, and disruptive/aggressive behavior—and seven items rated on a 0 to 4-point scale. The YMRS demonstrates strong criterion validity, evidenced by a correlation of 0.88 with the Mania Rating Scale, and displays a high inter-rater reliability of 0.93.
The PGI-Memory scale is a component of the Postgraduate Institute Battery of Brain Dysfunction (PGI-BBD), 39 which includes five batteries: the Performance Intelligence Battery, Verbal Intelligence Battery, Nahor Benson Test, and Bender Gestalt Test, and PGI-Memory scale. The PGI-Memory scale evaluates diverse memory dimensions, such as remote, recent, and immediate memory, using both verbal and non-verbal materials. It consists of 10 subtests that have been standardized for use in adult populations.
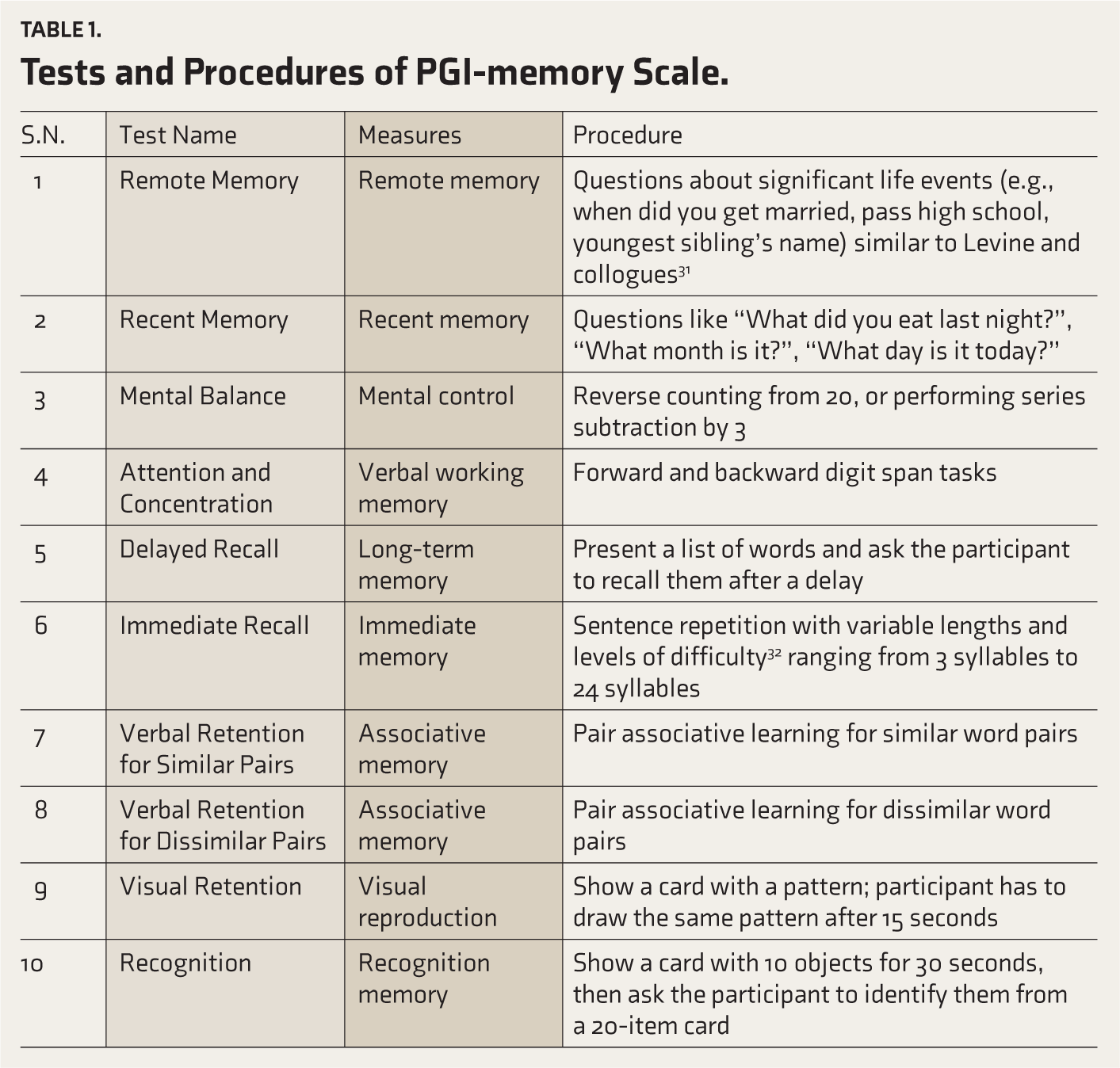
The scale has demonstrated robust reliability, with test-retest reliability over one week ranging from 0.69 to 0.85 for the individual subtests and approximately 0.90 for the total scale (both test-retest and split-half reliability). In addition, the PGI-Memory scale shows substantial concurrent validity, with a 0.71 correlation with the Boston Memory Scale and a 0.85 correlation with the Wechsler Memory Scale. Table 1 provides a summary of each subtest’s names and procedures in the PGI-Memory scale.
Tests and Procedures of PGI-memory Scale.
Statistical Analysis
All data were entered and analyzed using the SPSS 25.0 statistical software package. 40 Initially, the Shapiro–Wilk test was applied to assess the normality of data distribution, and Levene’s test was used to evaluate the homogeneity of variances. Results indicated that the data satisfied the assumptions necessary for parametric testing. Consequently, independent sample t-tests were employed to compare mean scores between the BM and control groups. Effect sizes were calculated using Cohen’s d, interpreted as small (d = 0.2), medium (d = 0.5), or large (d = 0.8). 41 For categorical variables, the chi-squared test examined any significant differences between groups. These statistical procedures ensured a rigorous comparison of neurocognitive performance across all examined domains.
Results
All the 40 participants (20 individuals in the BM group and 20 in the control group) successfully completed the clinical and neuropsychological assessments. The mean age of participants was 27.2 years (standard deviation (SD) = 4.14), reflecting a relatively homogeneous age distribution. The gender distribution was predominantly male, with 75% males and 25% females in both groups. Demographic and sociocultural characteristics for both groups are summarized in Table 2. Both groups were matched perfectly for sex (75% male and 25% female, P = 1.000), religion (85% Hindu, P = 1.000), and age (mean = 27.2 years, P = 1.000). No significant differences were observed in family type (P = .429), marital status (P = .519), or education level (mean years of education: 11.2 for the bipolar group and 10.67 for the control group, P = .951).
Comparison of Demographic and Sociocultural Variables Between Bipolar Mania and Control Groups.
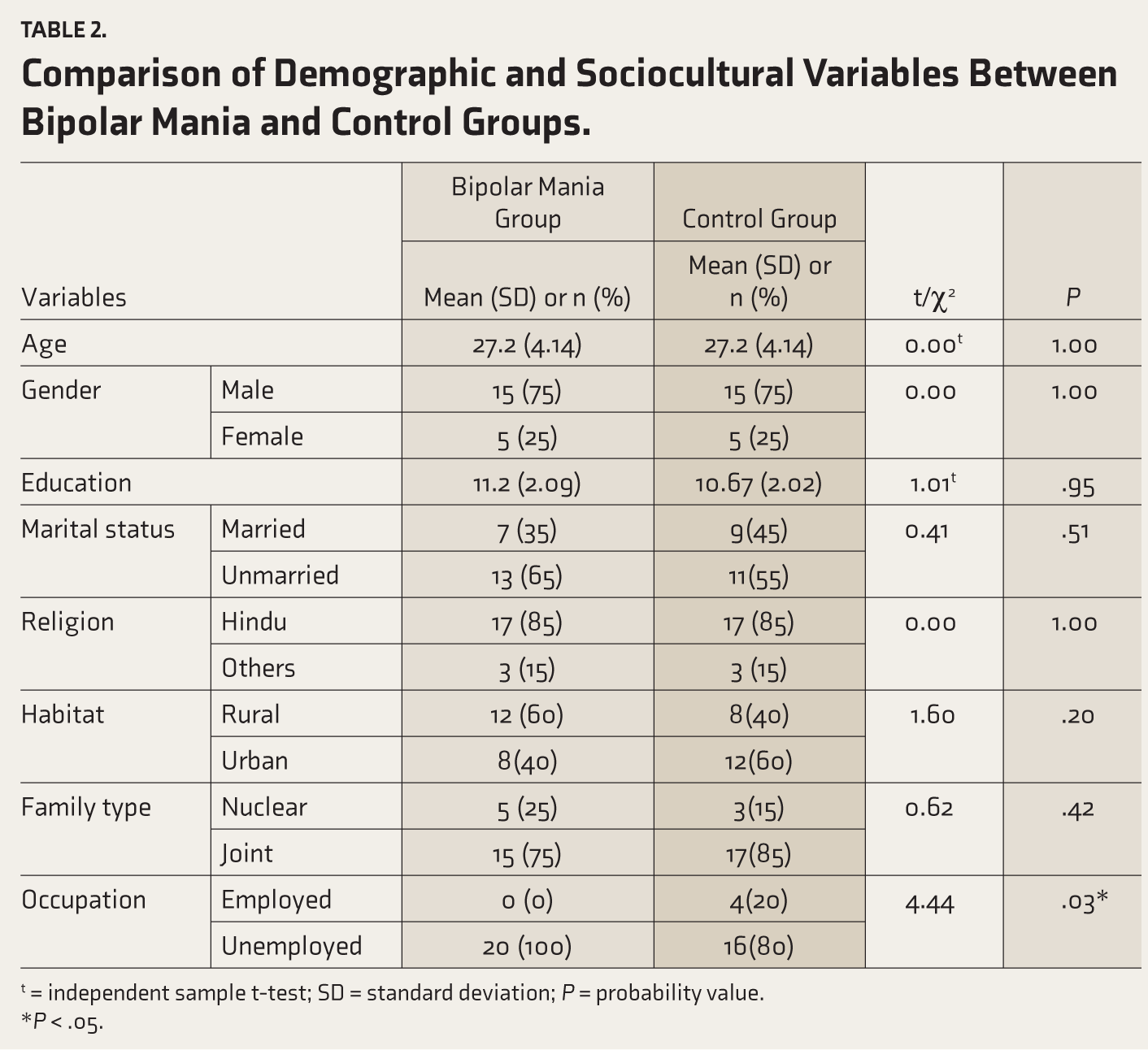
t = independent sample t-test; SD = standard deviation; P = probability value.
*P < .05.
A significant difference was observed in occupational status. All participants in the BM group were unemployed, while 20% of the control group were employed (P < .05), suggestive of a potential association between BM and unemployment. In contrast, the distribution of rural and urban residences was relatively similar between the groups: 60% of the bipolar group and 40% of the control group lived in rural areas, with no significant difference (P > .05).
The mean age of the participants was 27.2 years (SD = 4.14), with most experiencing the onset of bipolar disorder in early adulthood (mean = 22.46, SD = 2.97). Three subjects reported a history of depression before the current manic episode. Participants had experienced an average of 3.2 mood episodes (SD = 1.2), comprising 2.8 depressive episodes, 0.2 mixed episodes, and zero manic episodes. Nine participants (45%) had a history of psychotic symptoms, and 12 subjects (60%) exhibited psychotic symptoms during the current episode. The average number of suicide attempts was 0.7 per subject (SD = 1.1). The average duration of manic episodes was 4.04 months (SD = 3.48), and the mean illness duration was 6.12 months (SD = 2.54). The YMRS scores averaged 23.21 (SD = 4.38), indicating moderate manic symptoms. 34 Only two subjects were on mood stabilizers, while the remaining 18 were prescribed atypical antipsychotics.
Table 3 summarizes the neurocognitive performance differences between the BM group and the control group across various memory domains. In immediate, recent, and remote memory, the bipolar group showed significantly lower scores compared to the control group. For remote memory, the bipolar group scored 4.45 (SD = 1.39), significantly lower than the control group’s 6.00 (SD = 0.00), with a large effect size (Cohen’s d = 1.58, P < .001). Similarly, recent memory performance in the bipolar group (M = 4.35, SD = 0.99) was significantly lower than the control group (M = 5.00, SD = 0.00), with a medium effect size (Cohen’s d = 0.93, P = .006). Immediate memory deficits were also notable in the bipolar group (M = 6.05, SD = 2.39) compared to the control group (M = 9.30, SD = 2.00), with a large effect size (Cohen’s d = 1.47, P < .001).
Comparison of Memory Domain Performance Between Bipolar Mania and Control Groups.
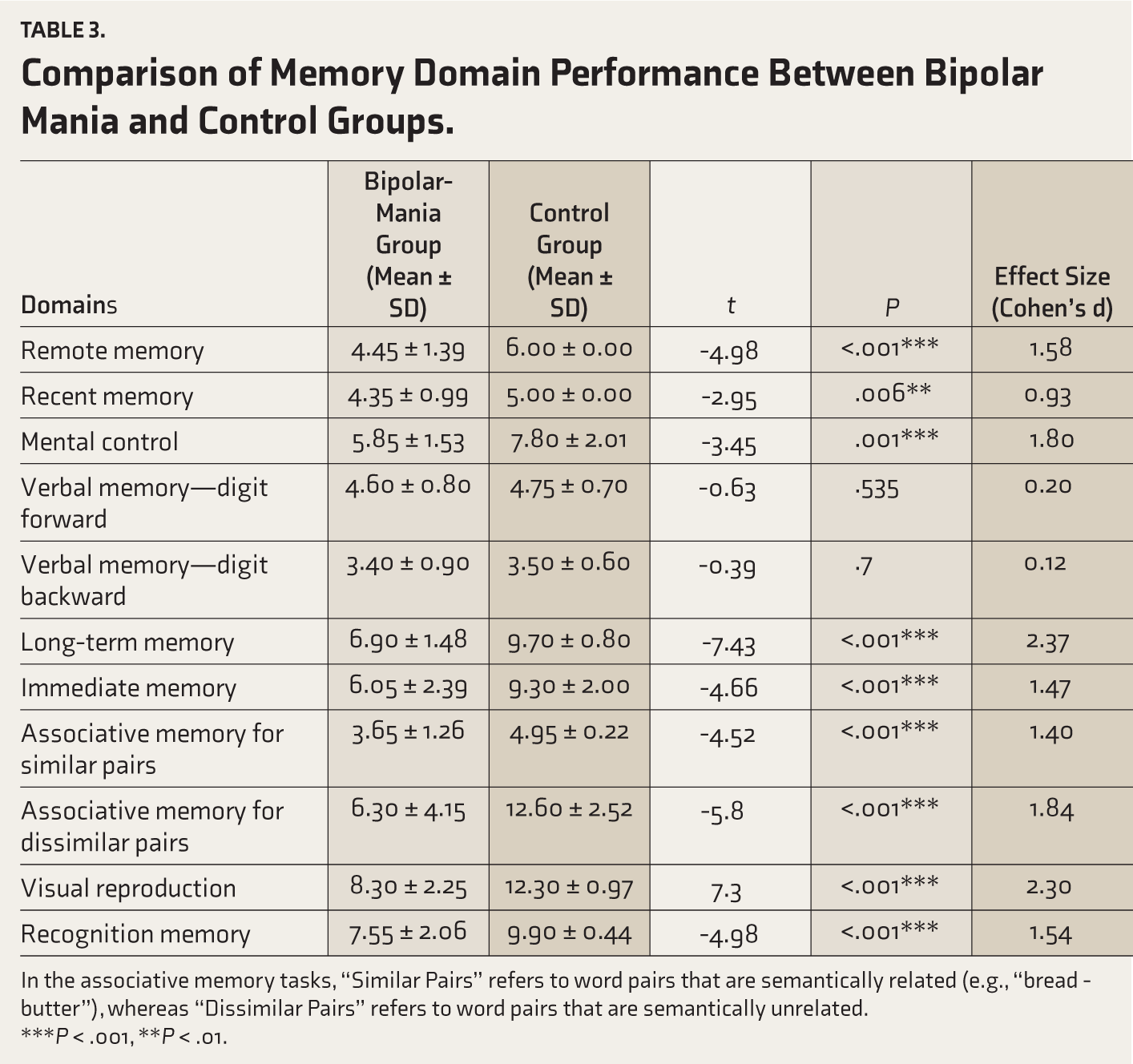
In the associative memory tasks, “Similar Pairs” refers to word pairs that are semantically related (e.g., “bread - butter”), whereas “Dissimilar Pairs” refers to word pairs that are semantically unrelated.
***P < .001, **P < .01.
In the domains of mental control and working memory, the bipolar participants demonstrated significant impairments in mental control but performed comparably to controls in working memory. Specifically, mental control scores were lower in the bipolar group (M = 5.85, SD = 1.53) than in the control group (M = 7.80, SD = 2.01), with a significant difference (Cohen’s d = 1.80, P = .001). In contrast, no significant differences were found in verbal working memory: the bipolar group scored 8.00 (SD = 1.21), and the control group scored 8.25 (SD = 0.96) with a small effect size (Cohen’s d = 0.23, P = .476). When verbal working memory was assessed separately for forward and backward components, scores were comparable. For digit forward, the bipolar group scored 4.60 (SD = 0.80), while the control group scored 4.75 (SD = 0.70) (Cohen’s d = 0.20, P = .535). For digit backward, the scores were 3.40 (SD = 0.90) for the bipolar group and 3.50 (SD = 0.60) for the control group (Cohen’s d = 0.12, P = .700).
In the domains of learning and associative memory, significant deficits were observed in the bipolar group. Long-term memory scores averaged 6.90 (SD = 1.48) in the bipolar group, significantly lower than the control group (M = 9.70, SD = 0.80), with a very large effect size (Cohen’s d = 2.37, P < .001). Associative memory was also impaired in the bipolar group, with scores of 3.65 (SD = 1.26) for similar pairs and 6.30 (SD = 4.15) for dissimilar pairs, compared to 4.95 (SD = 0.22) and 12.60 (SD = 2.52) in the control group, respectively. Both comparisons showed large effect sizes (Cohen’s d = 1.40 and 1.84, both P < .001).
In terms of visual reproduction and recognition memory, the bipolar group exhibited significant deficits. For visual reproduction, the bipolar group scored 8.30 (SD = 2.25) compared to 12.30 (SD = 0.97) in the control group, with a very large effect size (Cohen’s d = 2.30, P < .001). Recognition memory scores were also lower in the bipolar group (M = 7.55, SD = 2.06) than in the control group (M = 9.90, SD = 0.44), showing a large effect size (Cohen’s d = 1.54, P < .001).
Overall, we found that memory impairments were evident across all domains in the BM group, except for working memory, which showed no significant difference between groups. As depicted in Figure 1, our study found that long-term memory exhibited the greatest impairment, followed by visual retention. Recent memory showed the least impairment, highlighting domain-specific variability. Despite these widespread cognitive deficits, working memory was relatively unaffected compared to controls.
Cohen’s d Values for PGI-Memory Subtests Comparing Bipolar and Control Groups.
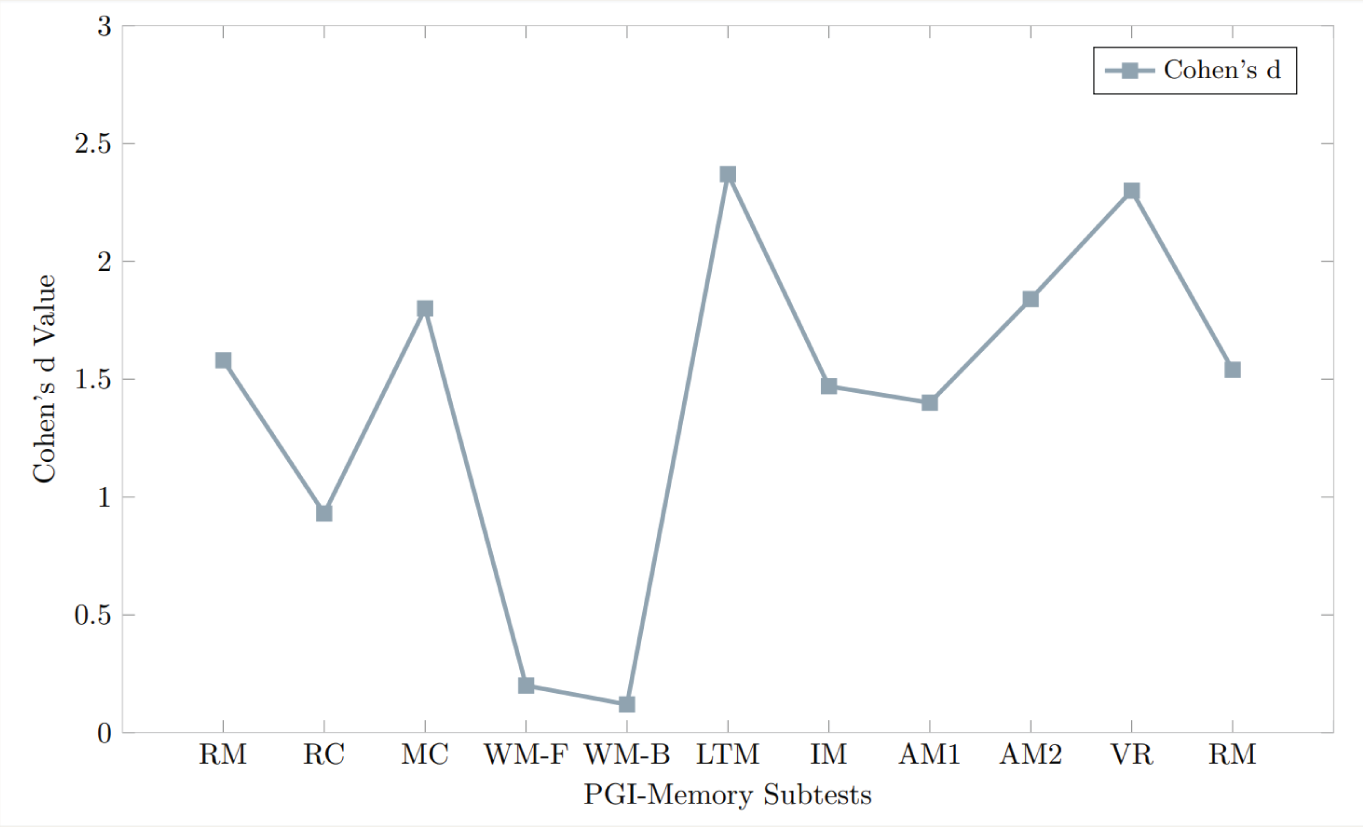
The following abbreviations represent the memory domains assessed using the PGI-Memory Scale: RM = Remote Memory; RC = Recent Memory; MC = Mental Control; WM-F= Working Memory-Digit Forward; WM-B= Working Memory-Digit Backward; LTM = Long-Term Memory; IM = Immediate Memory; AM1 = Associative Memory for Similar Pairs; AM2 = Associative Memory for Dissimilar Pairs; VR = Visual Reproduction; RN = Recognition.
Discussion
This study investigated domain-specific memory impairments in individuals with BPAD experiencing a current manic episode, utilizing the PGI-Memory scale. While previous research has explored cognitive functioning in various phases of BPAD—depression, euthymia, and mania—domain-specific memory impairments during mania remain underexplored. Our findings revealed significant deficits across multiple memory domains, including immediate, recent, remote, associative, long-term memory, visual reproduction, and recognition memory, in individuals with BM compared to HC. Interestingly, working memory appeared unaffected, suggesting that memory impairments during mania are domain-specific and tied to the unique cognitive profile of the manic phase.
The BM group and the control group were well-matched across most sociodemographic variables, including sex, religion, habitat, family type, marital status, age, and education level. This comparability minimizes the likelihood of confounding effects of these factors. However, a notable difference was observed in employment status; none of the subjects in the BM group were employed, while 20% of the control group were employed. This disparity underscores the functional challenges faced by individuals with BM, which may stem partly from the observed cognitive impairments. Memory deficits can significantly affect occupational functioning by impairing the ability to learn, retain, and apply new information, thereby reducing overall task efficiency.10,42 Consistent with our findings, previous studies have shown that cognitive impairments, including memory deficits, are strong predictors of occupational recovery and employment status, highlighting the importance of addressing these deficits to improve vocational outcomes and quality of life in individuals with BM.43,44
Mood state at the time of encoding, whether manic, depressed, or euthymic, plays a significant role in influencing the ability to recall events later. We hypothesized that individuals in a manic state would exhibit poor recollection of remote events, and our findings confirmed impairments in immediate, recent, and remote memory. Prior research on autobiographical memory—a subset of remote memory—has highlighted similar deficits, particularly in episodic memory.23,45 One of the studies found that individuals with mania demonstrated greater impairments in episodic memory compared to euthymic or depressed individuals, whereas semantic memory remained relatively unaffected. 23 Consistent with these findings, our results indicate that remote memory was more impaired than recent memory in individuals with BM, suggesting a particular vulnerability in episodic memory during manic episodes. The remote memory subtest questions of the PGI-Memory scale primarily assess episodic memory, as they require recall of personally experienced past events. This specificity further supports the pattern of episodic memory impairment observed in our study.
Impairment in immediate and recent memory observed in our study is suggestive of encoding difficulties, consistent with existing literature.45–47 Although working memory appeared intact in our study, as assessed by the Digit Span test—a measure primarily evaluating the ability to hold and manipulate simple information—deficits emerged in tasks requiring immediate and recent memory subtests, which better reflect real-world encoding demands. This pattern suggests that while individuals with mania may retain the ability to encode simple information, encoding deficits become apparent as the complexity of information increases. Furthermore, the significant deficits observed in long-term memory likely stem from impaired encoding, given the critical role of encoding in memory consolidation. However, these findings should be interpreted with caution, as memory deficits in mania likely involve an interplay of encoding, storage, and retrieval processes. Further research is needed to clarify these mechanisms and their implications for cognitive functioning in bipolar disorder.
Structural and functional abnormality in the hippocampus has been consistently implicated in individuals with BPAD, particularly during manic episodes,48–50 which may explain the memory impairment observed in this study. According to the multiple trace theory, the hippocampus is essential for both encoding and retrieving events, especially episodic memory. 51 This theory posits that the hippocampus acts as a pointer, directing attention to relevant information during memory recall. In contrast, semantic memory retrieval is less reliant on the hippocampus. 52 Our findings, which show greater impairment in episodic rather than semantic memory, align with this theory. Neuroimaging studies have corroborated these results, demonstrating disrupted hippocampal activity in individuals with BPAD during memory tasks, which likely contributes to the observed encoding and retrieval deficits.53–56
In our study, individuals with BM exhibited impairments in mental control but retained intact working memory, as measured by the Digit Span task. Mental control involves regulating cognitive processes such as attention and task-shifting while working memory reflects the temporary storage and manipulation of information. 19 The absence of working memory impairments in our study contrasts with prior research reporting deficits in BPAD.21,57–60 However, studies considering inhibitory control suggest that working memory may appear intact when attention and inhibitory mechanisms are well-managed. This indicates that the preserved working memory in our sample may reflect compensatory mechanisms, while the observed deficits in mental control could stem from impaired inhibitory control, particularly during mania. 61 Further research is necessary to delineate the distinct contributions of inhibitory control to different cognitive domains in BM.
Baddeley’s Hedonic Detector theory 62 provides additional insight into these findings, emphasizing the role of emotional states in modulating cognition. According to this theory, emotional dysregulation during mania may interfere with tasks requiring self-regulation and flexibility, leading to specific deficits in mental control. In contrast, basic working memory capacity, which is less reliant on emotional regulation, remains unaffected. This framework suggests that emotional interference, rather than fundamental deficits in working memory, underlies the impairments observed in mental control.
Our findings align with prior research demonstrating broad-based memory deficits in mania, with the most pronounced impairments in long-term memory and recognition memory.20,57–59,63,64 Subjects in our study showed significant difficulties in verbal recall, visual, immediate reproduction, and visual recognition, indicative of compromised encoding and retrieval processes during manic episodes. Similar results have been reported in studies using the California Verbal Learning Test (CVLT) and Rey-Osterrieth Complex Figure Test (ROCF), where individuals with BPAD exhibited poor performance on verbal and visual memory tasks. 63 These deficits may reflect dysfunctions in the hippocampus and prefrontal cortex, 65 regions critical for memory consolidation and retrieval, which contribute to the broader cognitive impairments observed in mania.
Our study found significant impairments in pair association learning in individuals with mania, indicating a marked deficit in their ability to form and retrieve associations between stimuli. This finding highlights disruptions in the consolidation and retrieval of associative memories—a process reliant on the hippocampus and prefrontal cortex.66,67 Friston’s free energy principle68,69 offers a theoretical framework for these findings, positing that dysregulated neural activity in these brain regions disrupts the brain’s ability to minimize uncertainty by forming sensory-stimuli associations. In mania, the dysregulated neural activity in these key brain regions may disrupt this process, leading to difficulties in associative learning.
This study highlights a broad range of memory impairments in BM, which are crucial for emotional regulation, decision-making, and daily functioning. One of the strengths of our study is the careful matching of the BM group and the control group for age, sex, and education. This matching minimizes potential confounding variables and enhances the validity of our findings. These findings can enhance clinicians’ ability to conduct mental status examinations and improve diagnostic accuracy by focusing on how memory details are generated across different mood states. For example, our findings indicate that memory impairments during mania are primarily associated with difficulties in the encoding stage of memory processing. In contrast, depression appears to affect the retrieval stage, leading to recall abilities that produce memories with fewer perceptual details and fragmented timelines. 23 These observations underscore the importance of distinguishing between the different stages of memory—encoding, storage, and retrieval—when interpreting memory impairments. Notably, impairments in recall can result from deficits in encoding, short-term memory retrieval, transfer to long-term memory, or long-term memory retention rather than solely from issues in long-term memory storage. 70 Therefore, our results must be analyzed with caution, as the memory deficits observed during mania may result from initial encoding failures that subsequently impact retrieval. Conversely, the retrieval impairments seen in depression suggest that while the encoding and storage of information may remain relatively unaffected, the ability to access that information is compromised.
This distinction is important in clinical assessments, particularly when asking subjects about the sequence of events, as it can guide more tailored diagnostic and therapeutic approaches. Episodic memory, a unique neurocognitive system enabling recall of past experiences, 71 plays a crucial role in adaptive decision-making and problem-solving. may lead individuals to repeat maladaptive behaviors because they struggle to recall past experiences and learn from them. 72 Similarly, impairments in mental control—the ability to regulate one’s thoughts, attention, and responses—can result in impulsive reactions. Recognizing these specific deficits could provide clear clinical provide and guide the development of targeted interventions to improve memory consolidation and executive control in individuals with bipolar disorder. Understanding the precise memory impairments in BM can also lead to more effective clinical interventions for managing cognitive dysfunctions.
One limitation of this study is the relatively small sample, which may limit the generalizability of our findings. We also utilized convenience sampling, which could influence the study outcomes due to potential selection bias. However, the groups were matched, and no significant differences were found in sex, religion, habitat, family type, marital status, age, or education level, suggesting that these demographic factors are unlikely to confound the cognitive outcomes observed. Additionally, while we employed the GHQ-12 as a screening measure for HC, it is not a comprehensive diagnostic instrument. To ensure a more accurate determination of the absence of psychiatric disorders, a semi-structured diagnostic interview, such as the Structured Clinical Interview for DSM-5 (SCID-5), 73 or Mini-International Neuropsychiatric Interview (MINI), 74 should have been administered. Implementing such a tool in future research would provide a more reliable basis for categorizing participants as “healthy controls” and strengthen the validity of the study’s findings. Future research should aim to replicate these results with larger and more diverse populations, including individuals in depressive and euthymic states, to enhance the applicability of the conclusions. Additionally, the cross-sectional design limits our ability to determine whether cognitive impairments persist across mood states or vary with symptom severity. Longitudinal studies are needed to track cognitive changes over time in bipolar disorder. Although we used an Indian neuropsychological battery, future studies should consider employing more comprehensive cognitive assessment tools. Lastly, the study did not account for possible confounding variables such as medication status, the presence of comorbid conditions, or affective states such as anxiety and depression, which are known to influence neuropsychological test performance. These were not assessed or employed as covariates in the analysis, which represents another limitation of the study.
Conclusions
In conclusion, this study identified significant domain-specific memory impairments in individuals with bipolar disorder, particularly in visual and verbal memory, episodic memory, mental control, and associative learning, while working memory remained unaffected. These findings suggest that cognitive dysfunction in BPAD is selective and linked to underlying neural abnormalities, particularly in the hippocampus and frontal-subcortical circuits. Understanding these impairments provides valuable insight into the cognitive challenges faced by individuals with bipolar disorder. It underscores the importance of developing targeted interventions to improve memory and executive functions in this population. Further studies are needed to investigate the neurobiological mechanisms that contribute to these deficits and to assess the effectiveness of cognitive interventions in addressing these impairments.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Note
This manuscript is a revised version of a preprint previously posted on medRxiv (DOI:
Acknowledgements
We sincerely thank our mentor’s Basudeb Das, and D. Ram for their invaluable guidance throughout this study and Shashank Nadkarni our expert advisor for his insightful contributions to the writing of this manuscript.
Consent to Participate
Written informed consent was obtained from all study participants.
Data Availability
Data of the current study will be shared on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors assume full responsibility for the entire content of this manuscript. While no part of the manuscript was created using artificial intelligence tools, artificial intelligence (AI) was used to enhance its clarity and language.
Ethical Considerations
Approval was obtained from the Institute Ethics Committee (Approval No. IEC/M.Phil/48/2011 dated 14-11-2011), Central Institute of Psychiatry, Ranchi, Jharkhand, India.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Prior Presentations
This study has not been presented at any seminar or conference, nor has it been published in any journal.
Simultaneous Submission
This study is not being submitted to any other journal or resource for publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.