
Abstract
Purpose of the Review:
Repetitive transcranial magnetic stimulation (rTMS) has emerged as a promising alternative therapeutic modality for bipolar depression. Theta Burst Stimulation (TBS) a novel variant of rTMS is currently evolving as an effective and safe therapeutic tool in the management of bipolar depression, although it is still in the initial phase. In the present systematic review and meta-analysis, data from various studies investigating the effectiveness and tolerability of TBS in individuals with bipolar depression were synthesized.
Data collection and analyses:
Eight studies assessing the efficacy of TBS as a treatment for bipolar depression were included after a systematic search. The quality of the included studies was assessed using standard methods. Synthesized data included three uncontrolled clinical trials (non-randomized controlled trials [RCTs]; n = 48) and five RCTs (n = 201). While four studies used intermittent TBS, two studies used continuous TBS and bilateral TBS, each. Data from the five RCTs meta-analyzed using the random effects model showed the pooled odds ratio and effect size for response in the active group compared to the sham group were 1.01 (95%CI: 0.56, 1.83) and 1.64 (95%CI: –0.46, 3.74), respectively. Although both models showed no/minimal heterogeneity or publication bias, they were not statistically significant. A supplementary trial sequential analysis confirmed the need for more studies and suggested that the total sample required for drawing meaningful inferences was 918 samples.
Conclusion:
The available evidence suggests that more studies are required to draw conclusive inferences for the efficacy of TBS in the therapeutic management of bipolar depression.
Bipolar disorder is a mood disorder with cyclic clinical representation, marked by alternating episodes of mania and depression, and is considered a severe mental illness. Depression remains the predominant polarity of the clinical progression of the illness in many cases and is associated with characteristic cognitive, physical, and behavioral symptoms affecting approximately 1%–3% of the population.1–4
Despite growing evidence for the use of conventional treatment (both pharmacological and non-pharmacological) approaches for bipolar disorder,5,6 a number of patients with acute phase bipolar depression either report poor response or develop intolerant side effects, 7 leading to poor adherence and deteriorating quality of life.8,9 In light of these limitations, it becomes pivotal to probe for new and possibly more effective treatment options for patients suffering with bipolar depression in order to experience prolonged periods of stability.
Repetitive transcranial magnetic stimulation (rTMS) is a new non-invasive neuro-modulatory approach that has received approval from the United States-Food and Drug Administration (US-FDA) for patients with major depressive episodes who do not show satisfactory response to pharmacotherapy or psychotherapy. 10 While excitatory stimulation (high-frequency rTMS) to the left dorsolateral prefrontal cortex (DLPFC) is US-FDA approved, many off-label studies have found inhibitory stimulation (low-frequency rTMS) to the right DLPFC also to be effective, in both unipolar and bipolar depression. 10
Theta burst stimulation (TBS), is a quite potent and innovative variation of TMS that applies short bursts of TMS pulses at a frequency of 50 Hz. The two types of TBS are continuous TBS (cTBS) type and intermittent TBS (iTBS) type. cTBS delivers uninterrupted 300 or 600 pulses and has inhibitory effects. In contrast, iTBS delivers 30 pulses lasting 2 seconds and repeated every 10 seconds, which has been shown to have excitatory effects.11,12 TBS has been shown to exert long-lasting post-stimulation effects and to exhibit comparable strengths and direction of post-effects to rTMS while requiring lower stimulation intensity and lesser stimulation time.13,14
The latest research has focused on investigating the therapeutic effectiveness of TBS as a management technique for bipolar depression, using iTBS or cTBS. In the present systematic review and meta-analysis, data from various studies investigating the effectiveness and safety (or tolerability) of TBS in bipolar depression were synthesized.
Method
The systematic review has been registered on PROSPERO (CRD42023362608).
Literature Search and Screening
A comprehensive literature search was carried out in various databases such as PMC, MEDLINE, Google Scholar (advanced search), and EMBASE covering articles available from the inception of related research up to January 2023. We pinpointed and extracted studies pertaining to TBS and bipolar disorder by employing relevant keywords and Boolean operators—AND and OR. The keywords were identified following the PICO framework. 15 The keywords were—Population—(“bipolar disorder,” “Bipolar Depression”), Intervention (“TBS,” “Theta Burst Stimulation,” “cTBS,” “Continuous Theta Burst Stimulation,” “iTBS,” “Intermittent Theta Burst Stimulation”), Comparator (“Sham”) and Outcome (“response,” “remission”). We followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to methodically screen and filter studies. In addition to uncontrolled studies (without sham treatment), randomized controlled studies (with sham treatment), open-label studies, and case series of TBS in bipolar depression were identified and screened. Two reviewers independently screened all the retrieved studies to determine and authenticate them to meet the eligibility. To solve any differences while reviewing the previous studies, reviewers work out together and reach an agreement with the help of a third reviewer. Subsequently, all prospectively relevant studies underwent analyses to confirm alignment with eligibility criteria, and the findings were duly reported.
Studies utilizing stimulation methods other than TBS for control comparison, for instance, rTMS or tDCS were excluded. We also excluded studies that had subjects with manic symptoms; protocol papers; review articles; conference abstracts/posters; consensus guidelines; and studies where TBS was co-initiated with any other modality of treatment, such as cognitive control training. Studies starting new pharmacotherapy with TBS protocol were also excluded. See the PRISMA chart (see Figure 1).
Depicting the PRISMA Flow Chart.

Method of Reaching Consensus
Assessment of Risk of Bias
The risk of bias in each study was autonomously conducted by two researchers. In the case of any discrepancies or differences, a third researcher intervened to resolve them through 100% consensus. For assessment, the studies were categorized into randomized control studies and non-randomized studies. The Cochrane Risk of Bias assessment tool (ROB) as recommended by the Cochrane Collaboration was employed to evaluate the randomized control studies. 16 The results of this assessment were synthesized using RevMan 5.4.1, a software developed by The Nordic Cochrane Centre, in collaboration with The Cochrane Collaboration, Copenhagen. This synthesis involves graph creation and a summary reflecting the authors’ judgment of each included study. In our analysis, we took into account several criteria to evaluate the risk of bias. These criteria encompassed aspects such as allocation concealment (selection bias), blinding of participants and personnel (performance bias), random sequence generation (selection bias), incomplete outcome data (attrition bias), selective outcome reporting (reporting bias), and blinding of outcome assessment (detection bias). We employed the Newcastle–Ottawa scale to assess the quality of non-controlled studies.
Outcome Measures and Data Extraction
The rates (numbers) of cases that showed response within the active and sham groups, where available, were retrieved along with the sample size. Similarly, the mean (±standard deviation [SD]) scores on the standard rating scales for depression (i.e., MADRS and HDRS) at baseline and post-treatment at two/three weeks were retrieved/extracted. Where values were depicted in graphs and not in terms of values, values were extracted from graphs using an open-source platform ( √((SDpre-intervention)2 + (SDendpoint)2 – 2 × r × SDpre-intervention × SDendpoint), we considered r (correlation coefficient) = 0.4 as a conservative estimate.
From different articles data were extracted by the researchers and the following items were noted: stimulation type (iTBS, cTBS, B/LTBS), gender ratio, study type and design, mean age of study participant, diagnosis, rating scale, brain target method, TMS equipment make, type of coil, site of stimulation, stimulation protocols (stimulation frequency, current intensity, total number of stimuli delivered).
Data Analysis
Meta-analyses were done using the Review Manager (RevMan)-Version 5.4.1. Data were grouped by outcome (risk ratio and standardized mean difference [SMD]) and pooled using the random effects models. The random effects model was used to address heterogeneity across studies, specifically with respect to stimulation parameters in our study, and is assumed to be universally present in intervention studies, in general. The inverse variance method and the Mantel–Haenszel test and were used for pooling SMDs and odds ratios, respectively. The odds ratio of >1 was considered to increase the chances of response in the active group. SMD values of 0.2–0.5, 0.5–0.8, and >0.08 were considered small, medium, and large effects, respectively. Heterogeneity assessment was done using the I2 statistic. Funnel plots were studied to assess publication bias.
Sensitivity analysis, which re-meta-analyze the findings after excluding data from studies showing a high risk of bias, was not conducted as the exclusion of such studies resulted in study numbers lower than the recommended for conducting a meta-analysis.
To calculate the required information size and improve the validity of all the meta-analyses of effect sizes, we conducted trial sequential analyses (TSAs).17,18 TSA was carried out by using an open-source software TSA-Version 0.9.5.10 Beta. The cumulative Z-curve’s eventual breach of relevant trial sequential boundaries—conventional, monitoring, and futility, was assessed based on a type I error of 5%, a power of 90%, and the standard error of supplementary random effects meta-analysis based on the SMD of change of severity scores.
Results
Selection and Characteristics of Studies
Following the search criteria, our initial search gave 64 results among which three records were identified as meta-analyses. All pertinent studies from the review on rTMS in bipolar disorder by McGirr et al. 19 were included. Further, we search the review by Chu et al. 20 on TBS as a therapeutic modality for unipolar or bipolar depression. Discarding non-specific and incomplete studies, duplications, consensus and guidelines, abstracts of meetings, and editorial pages, 15 studies were narrowed down for a diligent screening of eligibility. Consequently, eight studies fulfilled the eligibility criteria for evaluating TBS as the treatment option for bipolar depression.21–28 The complete process for study selection and exclusion criteria is illustrated in Figure 1.
Finally, in total eight eligible studies were incorporated into the systematic review. Among these studies, five were randomized, sham-controlled,21,23,25–27 two were case series,22,24 and one was open-label. 28 These eight studies address the role of TBS in bipolar depression, the term “Bipolar depression” was used in six studies,21,23–26,28 and “Mixed state” in two studies.22,27 A dataset consisting of a total 249 patients having bipolar depression was assessed for the effectiveness of TBS in treating bipolar depression. Among these individuals, 145 were undergoing active TBS treatment. The specific characteristics of these studies can be found in Table 1.
Studies and Their Respective Characteristics Investigating the Effects of TBS in Bipolar Depression.
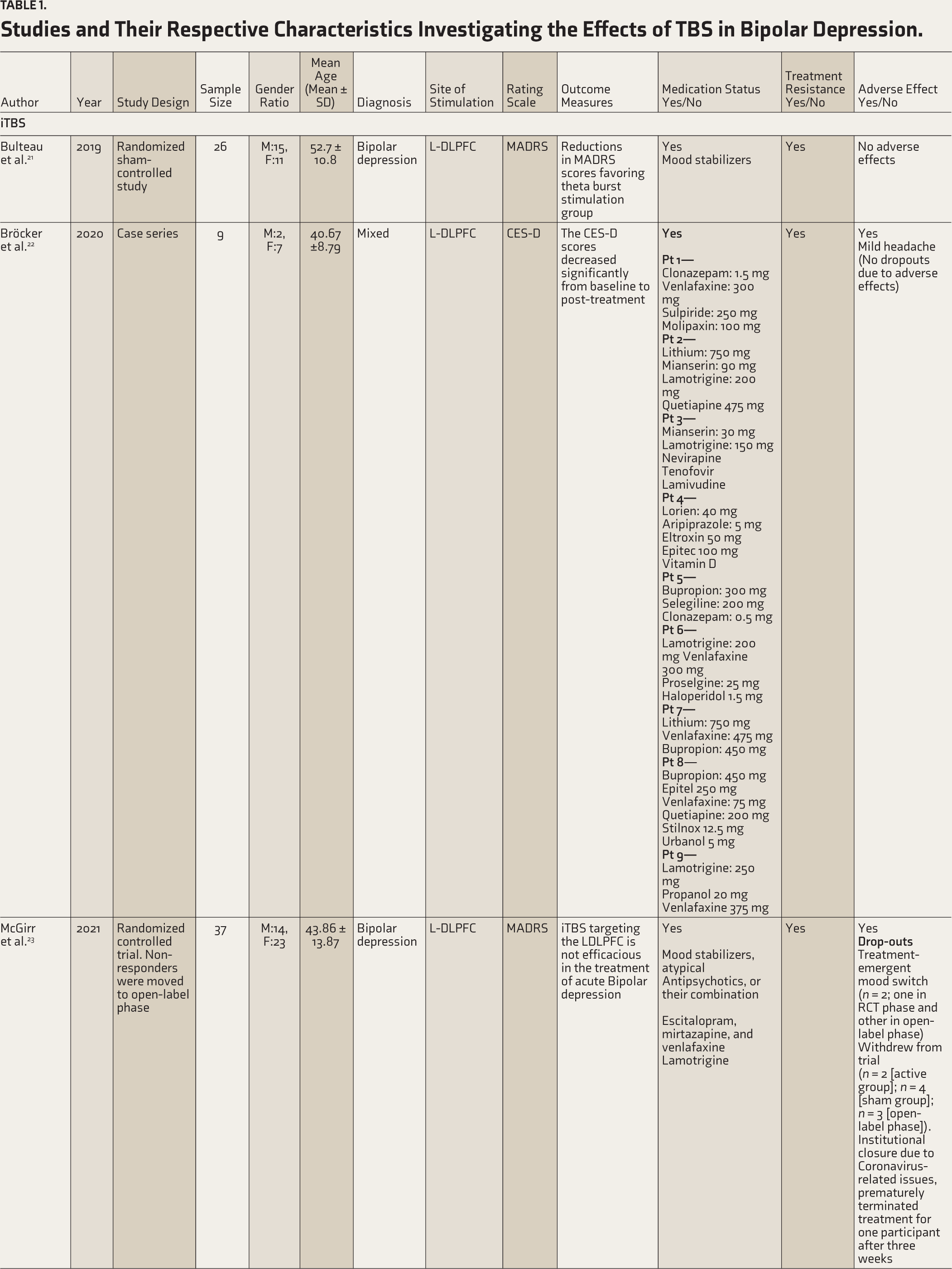

iTBS = intermittent theta burst stimulation; cTBS = continuous theta burst stimulation; BLTBS = bilateral theta burst stimulation; aMT = active motor threshold; CES-D = Centre for Epidemiological Studies Depression Scale; HDRS = Hamilton Depression Rating Scale; MADRS = Montgomery-Asberg Depression Rating Scale; MT = motor threshold; N/A = not available; rMT = resting motor threshold; R-DLPFC = right dorsolateral prefrontal cortex; L-DLPFC = left dorsolateral prefrontal cortex; CANMAT= Canadian Network for Mood and Anxiety Treatment.
We noted the given variables related to treatment: type of coil used for active and sham procedure, data extracted from used treatment protocol (iTBS, cTBS, or bilateral TBS [BLTBS]), location of coil placement, stimulation frequency (Hz), stimulation intensity (in percentage), the total number of pulses delivered, and number of treatment sessions (sessions per day, total sessions). The number of sessions per day was not specified in some studies or had varied numbers and duration of sessions each day.
In different studies, the approaches employed to locate the cortical sites varied significantly across various studies, and the locations were determined either by neuronavigation, according to the international electroencephalographic system, or by the 5-cm rule. There were broad differences in the type of coil used for active stimulation across studies, with most of them using a figure of eight type coil, while some of the studies use Cool-B65 A/P coil/Cool-B70 coil, and butterfly coil for the study. However, the studies included employed an array of sham approaches. Some sham coils mimicked the auditory effects of TBS without delivering the actual pulses. Some would place the coil on the scalp surface angled at 45 or 90 degrees or tilted resulting in the sham coil producing a minimal degree of intracortical activity. Characteristics of the TBS protocol of each included study are shown in Table 2.
Characteristics of the Stimulation Protocol of the Included Studies.

aMT = Active motor threshold; BA = Brodmann area; MT = motor threshold; rMT = resting motor threshold; R-DLPFC = right dorsolateral prefrontal cortex; L-DLPFC = left dorsolateral prefrontal cortex.
Side/Adverse Effects
Most of the studies included in this review reported no significant side effects except mild headache and scalp discomfort associated with the intervention. However, in two studies, one using iTBS 23 and the other BLTBS, 27 reported cases of TMS-induced manic switch and worsening of depression. Four patients also reported worsening of suicidal ideation. 27 All these cases dropped out. One study reported of a dropout due to local scalp discomfort reported. 28 Only one trial reported (albeit nil) statistical difference between the drop-out rates of active and sham groups 27 (see Table 1).
Risk of Bias
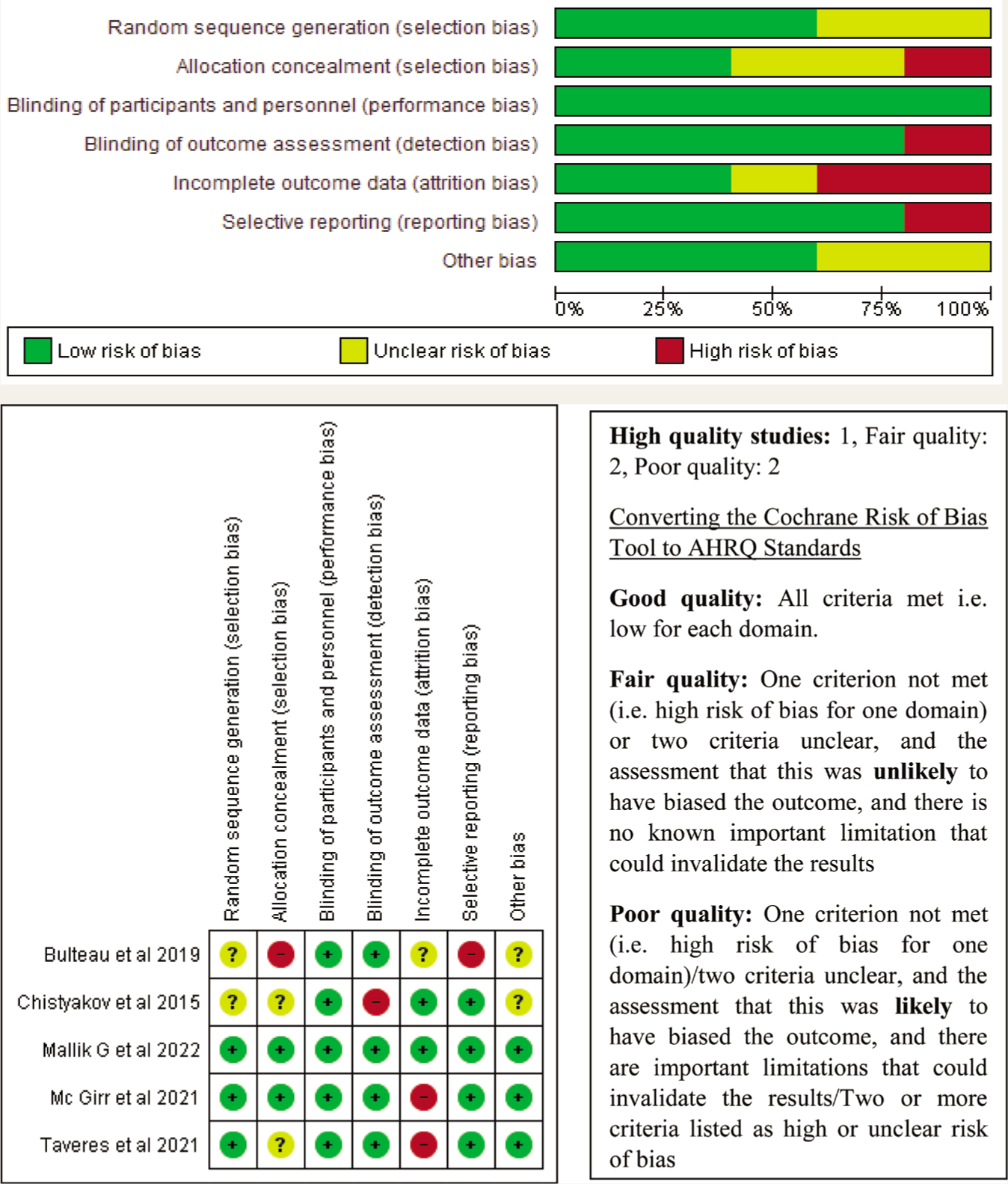
There was a significant bias in the methodological quality of the included randomized, non-randomized, open-label trials or case series. Out of the five randomized control trial studies, one study was considered to have a low risk of bias, 26 two studies had a moderate risk23,27 and the remaining two studies reported a high risk of bias.21,25 The summarized result in percentage form is represented in Figure 2a and b using RevMan 5 software. Among non-randomized studies, two were determined to have a moderate quality24,28 while one study had low quality. 22 This information is presented in Table 3.
Depicting Quality Assessment of Non-randomized Intervention Studies Using Newcastle–Ottawa Scale.

Quality scoring as per scale (low quality: 0–3; moderate quality: 4–6; high quality: 7–9). One study has low quality, while remaining two studies have moderate quality. * Indicates that the assessment domain was satisfactory for the particular study.
(a) Findings from the Reviewing Authors Regarding Each Risk of Bias Item (Presented as Percentages Across All The Studies): Risk of Bias Graph Using the Cochrane Risk of Bias Assessment. (b) Findings from the Reviewing Authors Regarding Each Risk of Bias Item (Presented as Percentages Across All The Studies): Risk of Bias Summary Using the Cochrane Risk of Bias Assessment.
Meta-analyses
Out of eight studies comprising 249 participants, only 201 participants belonged to the five randomized controlled trials (RCTs) with sham control groups. Further, although severity scores were available for all 201 participants, odds ratios could be calculated for only 200 participants (for one study, 25 frequency of responders was available for one participant less in the sham group).
Odds of Response (Risk Ratio)
A total of 200 patients from five studies were engaged in the odds ratio analysis. Results of the random effects meta-analysis of odds risk ratio data revealed that the pooled odds ratio of response in the active arm compared to the sham was 1.02 (95%CI: 0.71–1.46; k = 5; I2 = 0%; Z = 0.09; p = .93) (see Table 4 and Figure 3).
Meta-analyses (Risk Ratio) of TBS in Bipolar Depression.

Effect Size-change in Severity Scores
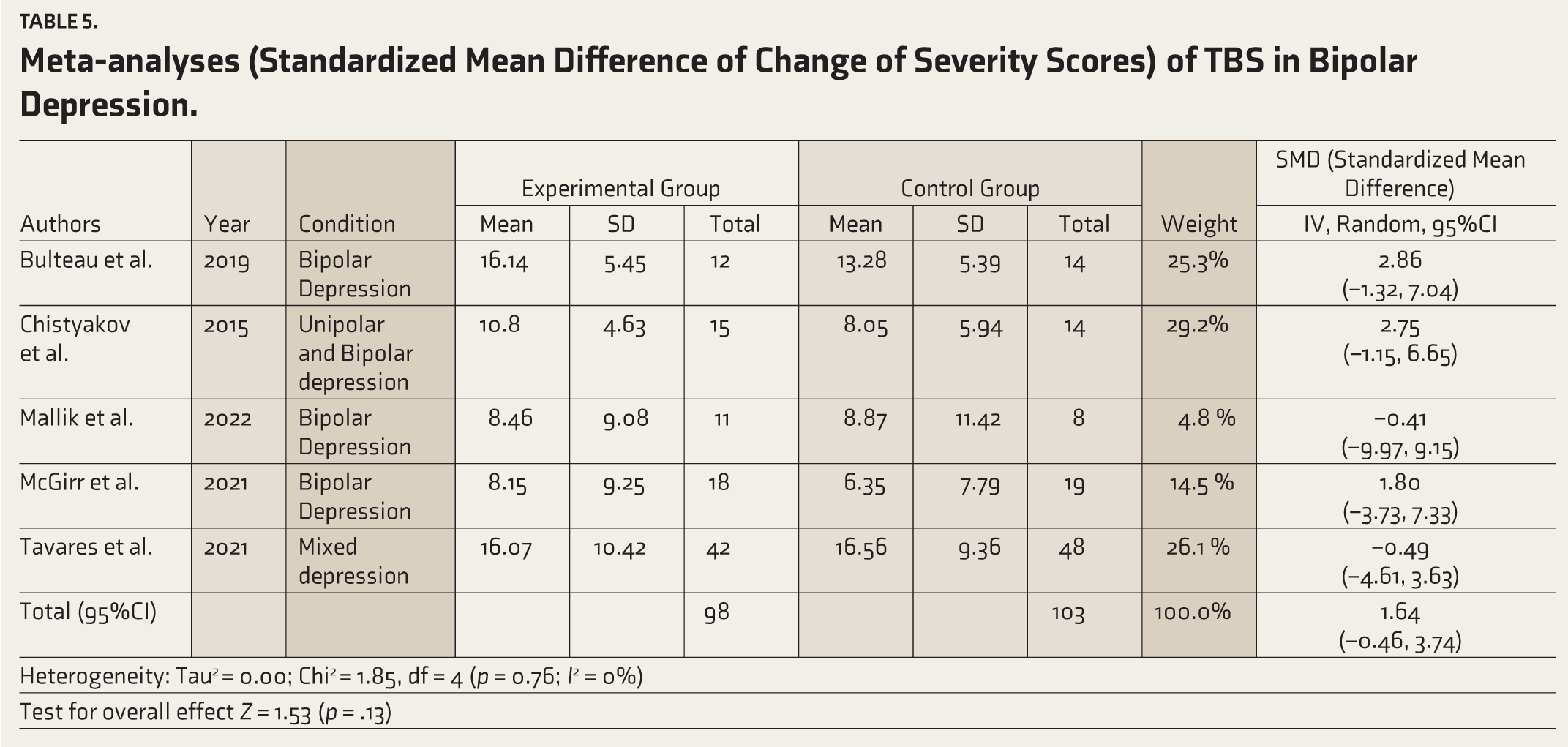
Results of the random effects model meta-analysis of mean difference in the change in severity scores revealed a pooled SMD of 1.64 (95%CI: –0.46 to 3.74; k = 5; I2 = 0%; Z = 1.53; p = .13) (see Table 5 and Figure 3).
Meta-analyses (Standardized Mean Difference of Change of Severity Scores) of TBS in Bipolar Depression.
Meta-analyses Indicating the Risk Ratio and Standardized Mean Differences of Theta Burst Stimulation (TBS) to Dorsolateral Pre-frontal Cortex (DLPFC) in Modulating Bipolar Depression.

The funnel plots for both analyses suggested no publication bias (Supplementary Figures 1 and 2).
TSA
The cumulative Z-curve was seen to end on the side favoring active TBS but did not breach any of the trial sequential boundaries—conventional; monitoring; and futility, suggesting an inconclusive nature of the findings and a need for more studies to confirm increased risk. The diversity-adjusted required information size was estimated as 918, which was greater than the current information size of 201. See Figure 4 for the TSA graph.
Trial Sequential Analyses of the Effect of TBS in Reducing Depressive Symptoms in Bipolar Depression. DARIS: Diversity-adjusted Required Information Size.

Discussion
Our review and meta-analysis were the first to aim to explore the existing literature on the efficacy of TBS in treating bipolar depression. Moreso, we were the first to run the TSAs to determine the validity of all the meta-analyses of effect sizes and to calculate the required information size. We did not find any significant difference in the improvement of depressive symptoms between active TBS and sham stimulation. Likewise, the overall response rate difference between groups was also found to be non-significant.
Our study selection criteria focused solely on studies where TBS was the exclusive treatment modality. Studies involving other treatment modalities were not included in our review.
TBS is a type of patterned TMS modality and is preferred over conventional rTMS citing stronger and prolonged neuroplastic effects over human cortices. Moreover, TBS’s shorter duration of session time per TMS protocol invites pragmatism to the treatment options. 10 Interestingly, conventional rTMS protocols (HF-rTMS over left DLPFC) have gained recommendations in bipolar depression, acute phase. 10 Therefore, it became even more relevant to determine the current evidence base of TBS protocols in acute phase bipolar depression.
Though the effect size (SMD) was reported to be large (>0.8) in our meta-analysis, but this change in severity scores remained statistically insignificant which is in accordance to our additionally calculated insignificant risk ratio. Recent metanalysis by Cai et al.29,30 have supported our findings of lack of evidence of cTBS efficacy in bipolar depression. Interestingly, they have reported iTBS to have a greater response in treating major depressive than sham stimulation. 30 But the population they have recruited has heterogeneous mix of both unipolar and bipolar depression. Possible reasons for the inconsistent reasons across the available reviews could be trial design, variations in stimulation site, method of localization (10/20 EEG electrode placement vs. rule of 5 vs. neuronavigation), number of sessions (& pulses) per day, motor threshold considered, and follow up period. The use of heterogeneous assessment tools (HAM-D, MADRS, CES-D) for outcome measures in studies included for review helps to assess variability across studies and to make comparisons.
It is essential to highlight that the studies included in our review exhibited variation in sample sizes, with five studies having a small sample size (<30). This aspect should be considered as it may potentially restrict the generalizability of the findings.
The majority of the studies testified minimal side effects like headache and scalp discomfort and that too transient. Only one study systematically reported the dropout rates and the reasons between active and sham groups and not surprisingly found no statistical difference. 27 There were a couple of studies reporting iTBS treatment emergent switch in four patients till date and had to discontinue the trial for the same.
The TSA, however, suggested that for a confident inference of a positive effect of TBS in bipolar depression, we need more studies that total to sample size of 918.
The strength of this study is that it is the only up-to-date overview of studies (including RCT, case series, open-label, and pilot studies) for the effectiveness of TBS in the depressive phase of bipolar disorder. Also, our methodology acknowledges and empowers us to identify the available evidence and map where the evidence base is tough or fragile.
Several limitations shall be noted. First, as mentioned most of the RCTs had limited sample sizes, which would limit the statistical power. Second, the limited duration of treatment (one to six weeks) was a limiting factor. Third, the parallel use of psychotropics which could have had additional antidepressant effects was not standardized either. Fourth, we did not calculate and compare the adverse effect and dropout rates profile among the RCTs. Finally, the dearth of head-to-head trials comparing the effectiveness of standard rTMS and of TBS and in bipolar depression was an important limitation.
Conclusions
In this meta-analysis, active TBS and sham TBS did not differ in efficacy for depressive symptoms in bipolar depression. The available evidence suggests that more studies are required to draw conclusive inferences for the efficacy of TBS in the therapeutic management of bipolar depression. Future multi-center RCTs with larger sample sizes and longer treatment duration are needed to determine the clinical use of TBS.
Footnotes
Acknowledgements
Nil.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.