
Abstract
Background:
The aim of this study was to determine the relationship between post-COVID neurocognitive symptoms and interleukin-6 levels.
Methods:
This was a hospital-based cross-sectional study wherein patients complaining of forgetfulness post-infection with coronavirus disease-2019 (COVID-19) were taken up for study (n = 53) from February 2023 to June 2023. The forgetfulness was characterized using the memory subscale of Postgraduate Institute-Battery of Brain Dysfunction (PGI-BBD). In addition, sociodemographic data were collected from patients. After obtaining written informed consent, 3 mL of peripheral venous blood was collected from patients, and interleukin-6 levels were measured. Other inflammatory markers, like C-reactive protein (CRP), were also measured.
Results:
The mean age of participants was 46.11 ± 8.58 years. Twenty-nine (54.72%) respondents were female, and 24 (45.28%) were male. Most (62.2%) of the patients in the study suffered from mild-to-moderate severity of COVID-19 infection. Among these patients, 43.3% had impairment in recent memory, 32 patients (60.3%) had impairment in attention and concentration, 54.7% had impairment in delayed recall, and 33.9% had impairment in immediate recall. Impairment in delayed recall was associated with a raised level of interleukin-6 (P = .0048 [P < .05]).
Conclusion:
Patients with impaired recall on PGI-BBD post-infection with COVID-19 have raised levels of interleukin-6, suggesting the role of neuroinflammation in post-COVID neurocognitive symptoms. Interleukin-6 is a marker of neuroinflammation that has been linked to cognitive decline in various studies. It can be used to predict cognitive decline and also aid in diagnosis.
Cognitive abnormalities can be seen even after 12 months of severe acute respiratory syndrome coronavirus 2 infection. A positive relationship exists between inflammatory markers such as interleukin-6and post-COVID cognitive deficits.Key Messages:
The new coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV2), first identified in Wuhan, China, is the source of the contagious sickness known as coronavirus disease-2019 (COVID-19). 1 It is a multisystem disorder because of its impact on the pulmonary, vascular, osteoarticular, and multisystemic systems.1–3 COVID-19’s clinical manifestations might range from lethal to asymptomatic. 4 Apart from the indications that arise during the acute phase, many patients have complained about long-term sequelae even after recovery from the infection. 1 COVID-19’s long-term effects resemble those of other serious infectious diseases.5–8 The World Health Organization defines a post-COVID condition as an extended COVID-19 effect that manifests in a person with a history of suspected or confirmed SARS-CoV-2 infection, often 3 months after the onset of symptoms and persisting for a minimum of 2 months, and if any other diagnosis cannot explain these symptoms.8, 9 One of the neuropsychiatric consequences of the post-COVID state is cognitive impairment, which includes deficiencies in attention, executive function, memory, and learning. 4 This impairment is crucial in impeding patients’ ability to recover fully. 4 These cognitive symptoms can lead to considerable disability and affect people’s standard of living and day-to-day activities. 4 Subjective cognitive complaints and objective abnormalities in neuropsychological tests are both possible components of post-COVID cognitive dysfunction (PCCD). 4 Thus, patients with cognitive impairment might report problems while performing basic activities of daily living, decision-making, learning new things, and completing tasks requiring complex reasoning.10–14 The multisystem role of COVID-19 inflammation causes cognitive impairment after infection.10, 11 There is the rise of pro-inflammatory cytokines such as TNF-α (tumor necrosis factor-alpha), interleukin-6 (IL-6), and interleukin-1 (IL-1) and inflammatory mediators in the serum and Central Nervous System (CNS) because of the inflammatory insults, which in turn affect the blood–brain barrier permeability, resulting in oxidative stress, microglial activation, and synergistic cognitive impairment. 10 The direct psychological impact of the illness on susceptible populations has already been mentioned in various studies. However, the direct effects of SARS- CoV2 on the CNS and the role of psychoneuroimmunity are mainly unknown. Because of the emergence of new-onset cognitive symptoms post-COVID and the unexplored area of cytokine research, we examined the relationship of self-reported memory problems with inflammatory markers. We conducted a hospital-based cross-sectional study to determine the relationship between post-COVID neurocognitive disorder and IL-6 levels.
Methods
This cross-sectional study was carried out in a North Indian tertiary care hospital’s postgraduate department of psychiatry after obtaining clearance from the Institutional Review Board (IRB). Patients of both genders, aged between 18 and 65 years, complaining of forgetfulness post-infection with COVID-19 were taken up for the study (n = 53) from February 2023 to June 2023. The memory subscale of PGI Battery of Brain Dysfunction (PGI-BBD) 15 characterized forgetfulness. In addition, sociodemographic data were collected from the patients. After obtaining written informed consent, 3 mL of peripheral venous blood was collected from the patient, and IL-6 levels were measured. Other inflammatory markers, like C-reactive protein (CRP), were also measured. The exclusion criteria for the cases were as follows: (1) history of neurocognitive disorder or any other psychiatric illness before COVID-19 and (2) other medical comorbidity or history of infections.
Assessment
All the patients who had presented to tertiary care with self-reported symptoms of forgetfulness after fulfilling the inclusion and exclusion criteria were subjected to neuropsychological assessment (PGI-BBD) by a postgraduate student. About 3 mL of venous blood was collected in a vial coated with Ethylenediamine Tetraacetic Acid (EDTA) to inhibit coagulation. Plasma was separated after immediate centrifugation, and the supernatant liquid forming the plasma was stored for the analysis of IL-6. Generally, IL-6 is not significantly detected in the systemic circulation. Normal levels of IL-6 can be considered 0.007 ng/mL or seven pg/mL, but they can also be up to 18 ng/mL and should be correlated with the patient’s clinical symptoms.
Instruments
PGI-BBD. 15 The PGI-BBD consists of tests to quantify cognitive dysfunction or impairment in clinical settings. Well-understood cognitive capacities of brain behavior, such as intelligence (both performance and verbal), memory, and perceptual acuity, are scaled by the PGI-BBD. Grounded on particular circumstances, the test can be utilized in parts and as a whole. It is easy to use these subscales autonomously, as each has separate norms. It also aids in assessing the degree of cognitive deterioration brought on by disease or trauma. Subscales of PGI-BBD include the following:
The PGI Memory Scale comprises 10 subtests: visual retention, retention for comparable pairs, retention for dissimilar pairs, mental balance, attention, remote memory, recent memory, delayed recall, immediate recall, and recognition psychometric properties.
Battery Performance Test of Intelligence: This consists of (1) a Koh’s block design test and (2) Pass-A-Long test.
Bender Visual Motor Gestalt Test evaluates the participant’s visual motor and perceptual abilities. Three main stages comprise the perceptual behavior of the Bender visual motor test: the sensory reception of the figures, the elucidation of the lines at the central nervous system level, and the motor performance of the figure.
Verbal Adult Intelligence Scale (VAIS): Verbal intelligence is developed through experiences, education, and social contact and continues to develop past physiological maturation. The assessment is divided into four smaller tests: information, digit span, arithmetic, and comprehension.
Nahor–Benson Test is an eight-card drawing test. The first five cards each include a pattern, while the remaining three cards have directions on drawing an item. The first five cards are based on development patterns, and the fourth and fifth cards evaluate the capacity to duplicate depth perception. These cards aid in determining the presence and severity of biological brain dysfunction.
Data Analysis
Following the compilation and entry of the recorded data into a Microsoft Excel spreadsheet, the data editor of the statistical package for social sciences (SPSS version 20.0, SPSS Inc., Chicago, Illinois, USA) was accessed. The categorical data were summed up as frequencies and percentages, whereas the continuous variables were reported as mean ± SD. Pearson’s chi-square was used for inferential statistics, and two-sided P-values were provided. A value of P < .05 was considered statistically significant.
Results
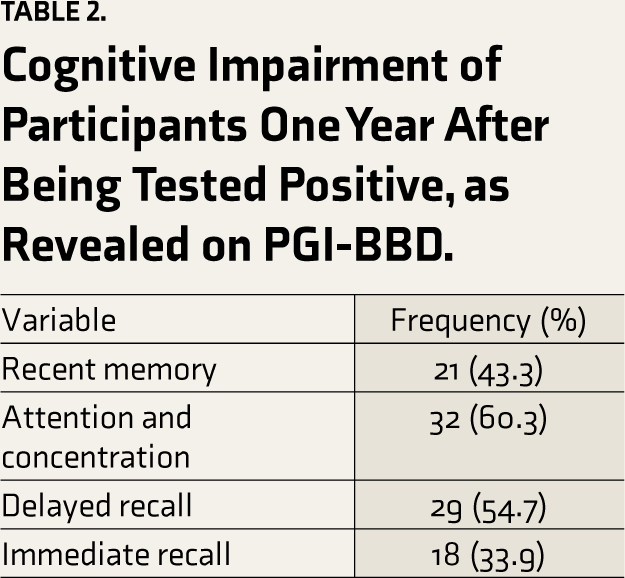
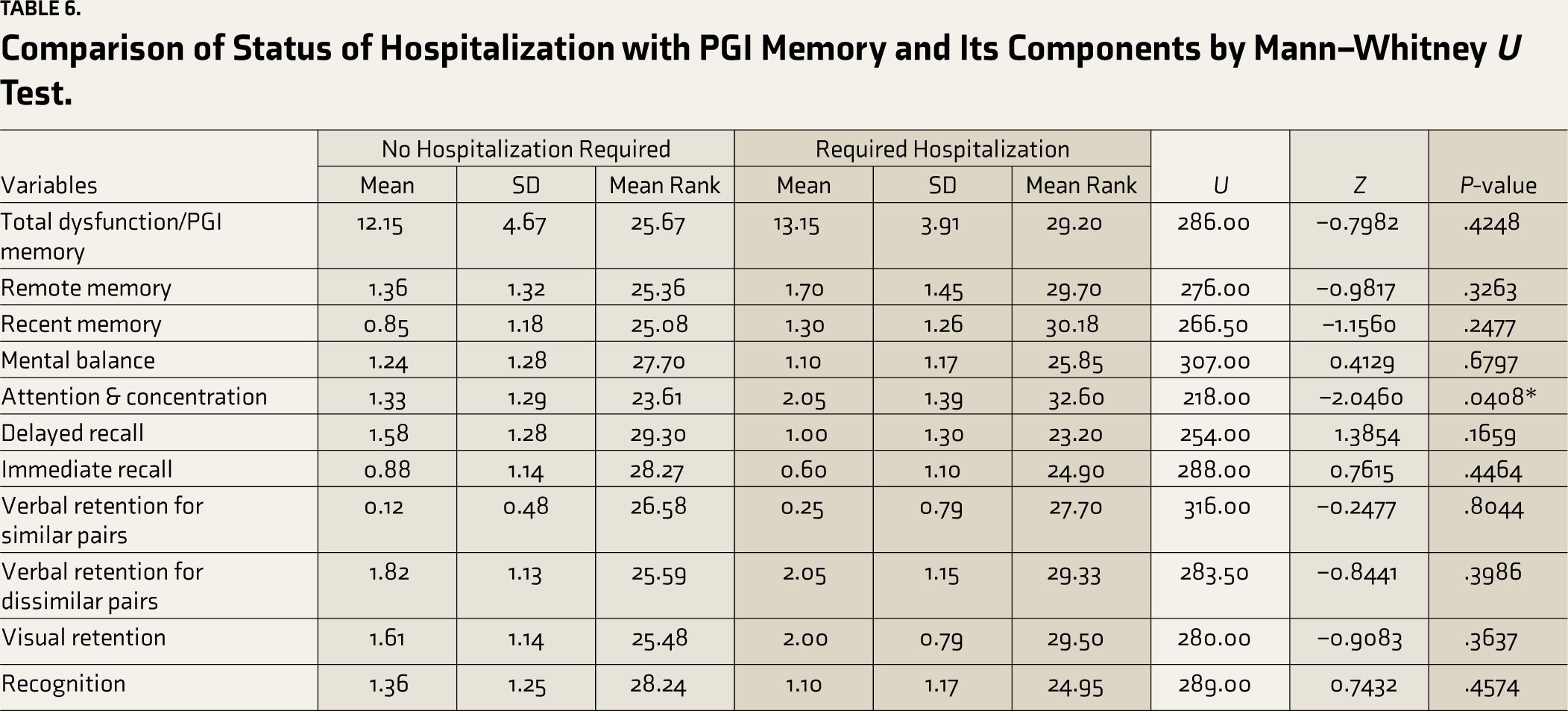
As shown in Table 1, 53 patients were recruited for the study. The sample included 24 males and 29 females with a mean age of 46.11 (SD ± 8.58) years. No statistically significant differences were observed in gender. Eighty-five percent of the study sample were educated and above high school. Most of the patients were married; the maximum number of them were employed. Two-thirds (62.26%) of the patients suffered from mild to moderate severity of the COVID-19 infection, whereas 37.74% had a severe COVID-19 infection and required hospitalization. The patients were assessed for cognitive impairment 1 year after their COVID-positive status with the help of PGI-BBD and its various subscales. As shown in Table 2, it was revealed that 43.3% of the patients had impairment in recent memory; 32 patients (60.3%) had impairment in attention and concentration; 29 (54.7%) had impairment in delayed recall; and 18 (33.9%) patients had impairment in immediate recall. Thirty-seven patients had difficulty performing the battery of performance tests of intelligence; 32 patients had dysfunction in the VAIS (Verbal Adult Intelligence Scale); 44 had produced the figures wrongly in the Nahor- Benson test; and 48 had dysfunction in the Bender–Gestalt test. During the presentation to the hospital, a venous blood sample was taken for the levels of IL-6, and it was revealed that among 29 patients who had impairment in delayed recall, seven patients (24.13%) had raised IL-6 levels, which was also statistically significant (P = .0048) as shown in Table 3. Table 4 shows that impairment in the performance test (Bender–Gestalt test) was also positively correlated with the raised levels of IL-6 (R = 0.30, P = .02). As shown in Table 5, multiple linear regression analysis for various cognitive function variables for the prediction of cognitive dysfunction, the combined effect of age on the PGI memory scale was found to be positive and significant (R = 0.33, P = .0413); however, for other cognitive function variables, age and IL-6 were not significant predictors. Also, no significant difference was observed between hospitalized and non- hospitalized patients with cognitive dysfunction. However, hospitalized patients had more impairment in attention and concentration, as shown in Table 6 (P = .04).
Demographic Characteristics of Patients.
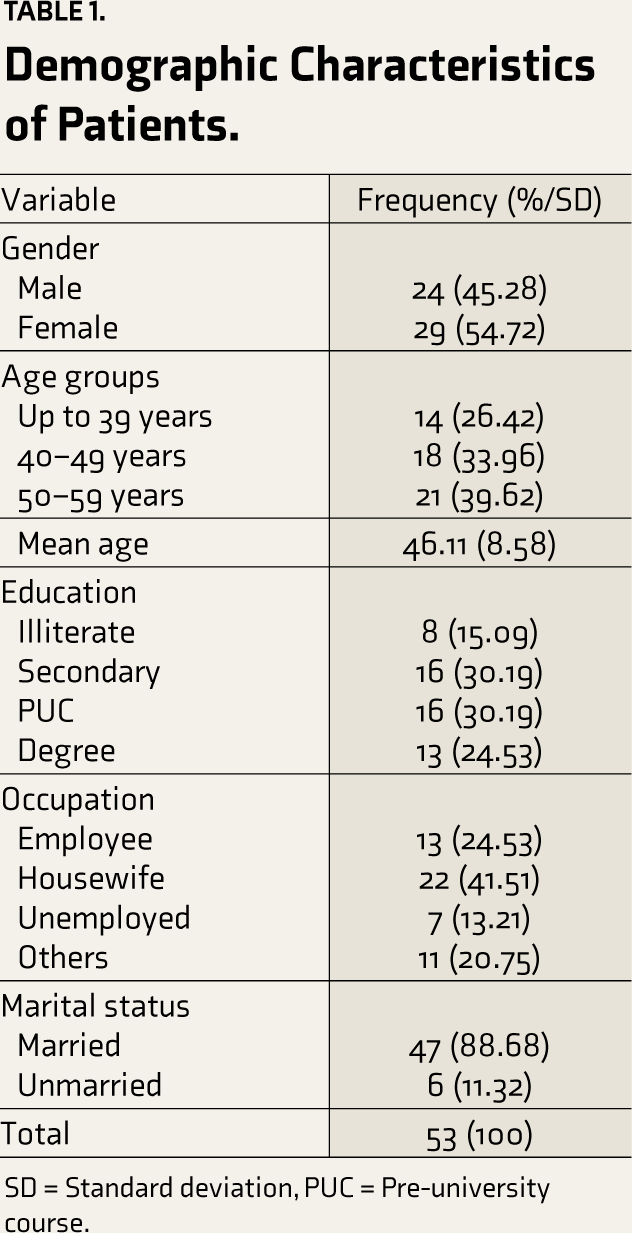
SD = Standard deviation, PUC = Pre-university course.
Cognitive Impairment of Participants One Year After Being Tested Positive, as Revealed on PGI-BBD.
Correlation Between IL-6 with Cognitive Functioning and Its Component Scores by Spearman’s Rank Correlation (
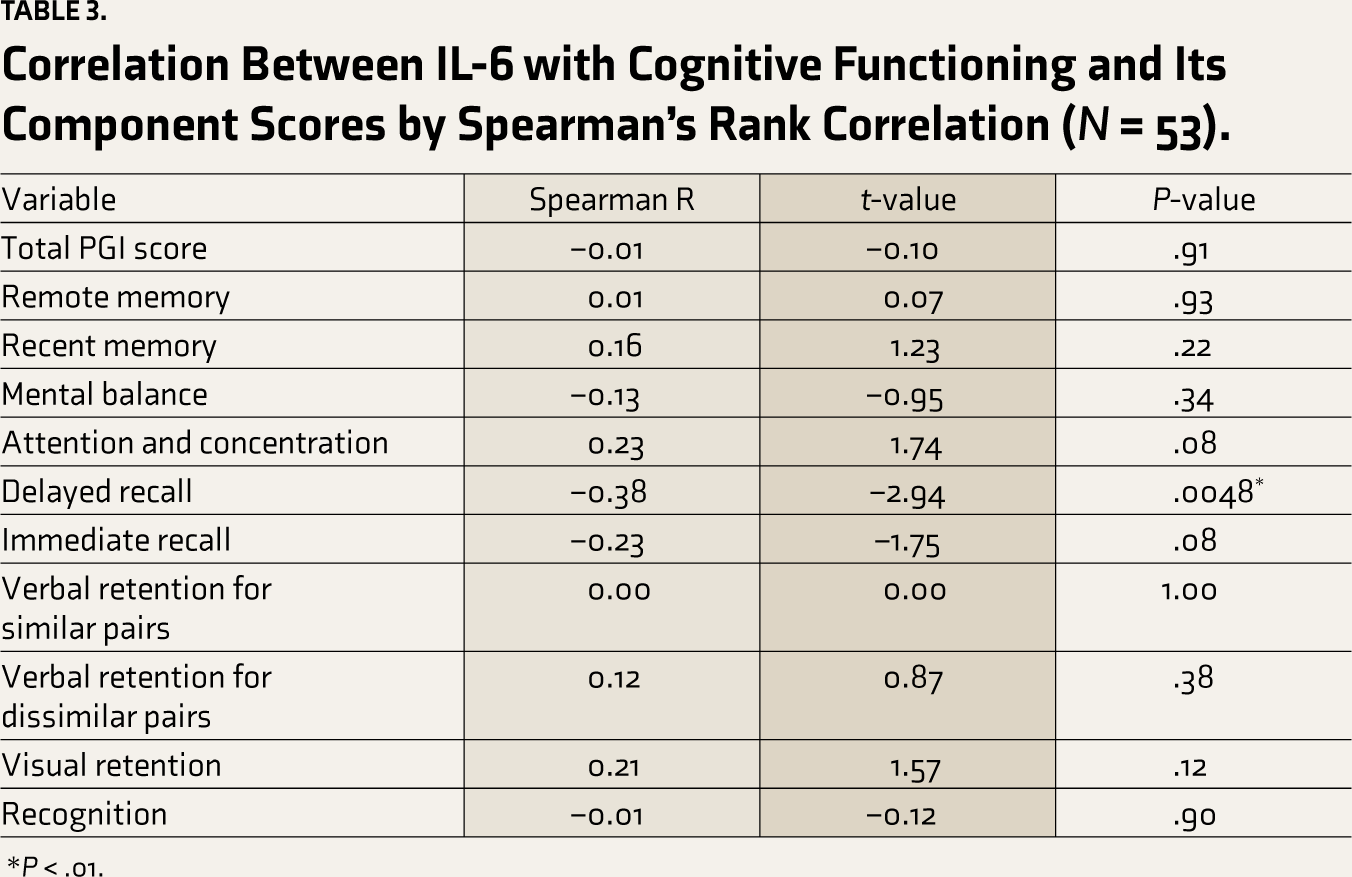
*P < .01.
Correlation Between IL-6 with a Battery of Performance Test of Intelligence (Dysfunction) Scores by Spearman’s Rank Correlation.

VAIS = Verbal Adult Intelligence Scale, BGT = Bender–Gestalt test.
*P < .05.
Multiple Linear Regression Analysis of Cognitive Function Variables by Age and IL-6.
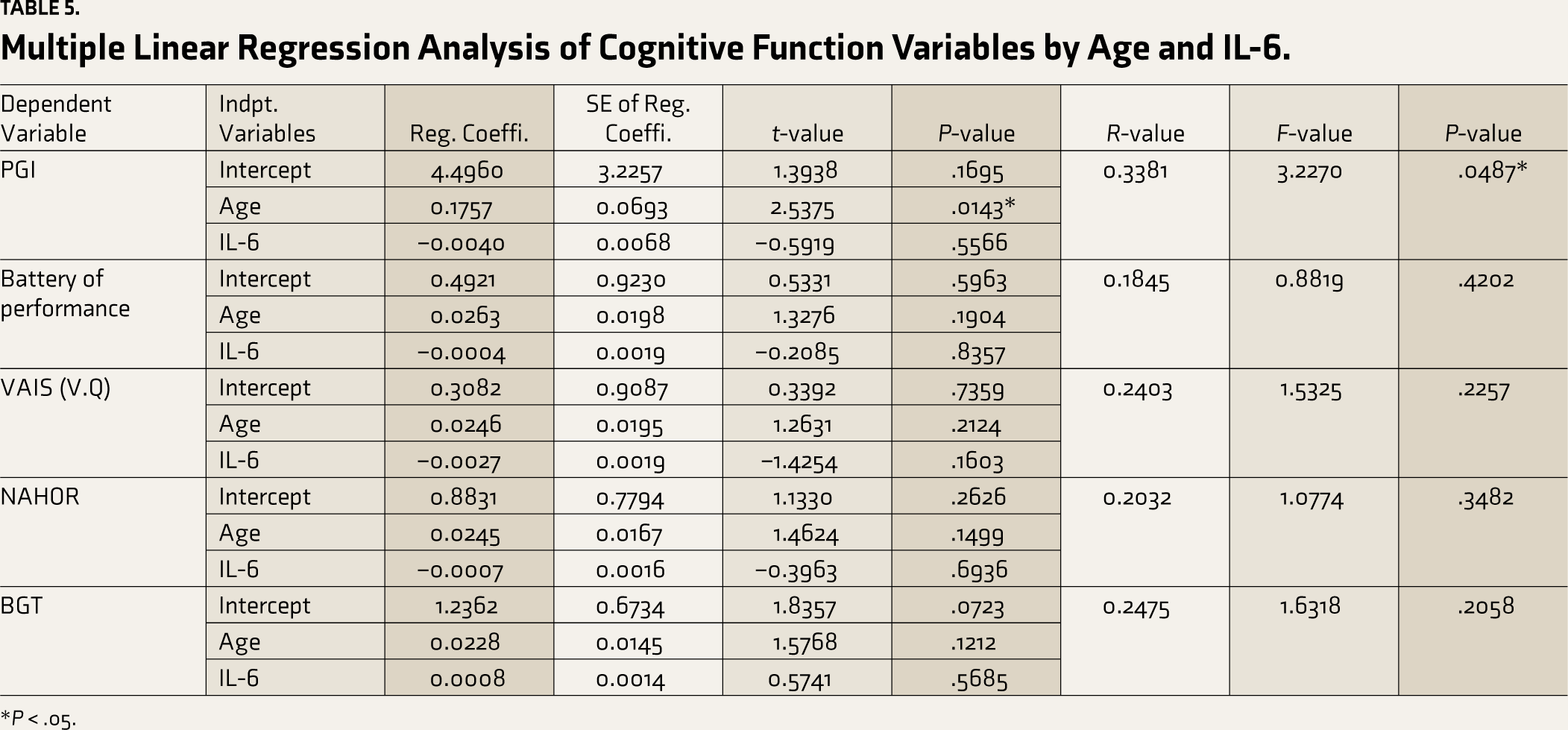
*P < .05.
Comparison of Status of Hospitalization with PGI Memory and Its Components by Mann–Whitney U Test.
Discussion
The SARS-CoV2 infection, even in its mild and moderate forms, can cause brain damage in the long term, with a potential effect on cognition. 16 The pathogenesis of such symptoms and the link between these impairments and inflammatory markers have yet to be studied in detail. In our study, we included the patients with self-reported memory problems who had developed COVID-19 infection in the past (all the patients on average presented after one year) with no history of such symptoms before the infection, no other psychiatric diagnosis, and excluding all the medical comorbidities. Thus, this study enhanced our comprehension of what is known as post-COVID neurocognitive dysfunction by emphasizing two primary patterns of findings:
First, the study revealed that the patients presenting to tertiary care for post-COVID forgetfulness had impairments in various memory components. Forty-three percent of patients had impairment in recent memory, 55% had impairment in delayed recall, and 34% had difficulty in immediate recall. This was consistent with the study of Zhao et al., 17 where 53.5% of patients had cognitive slowing in post-COVID-19 conditions. Another study by Qing et al. 18 also revealed that memory loss and concentration difficulties were seen in 37% of the COVID-19 survivors. The Nahor–Benson and Bender–Gestalt tests, two of the PGI-BBD’s most crucial sections, measure a subject’s ability to comprehend and replicate gestalt figures using the biological concept of visuomotor movement. The capacity to reproduce gestalt figures was severely affected in the patients with a raised level of inflammatory cytokines, which was statistically significant (P < .05) in our study.
Cognitive decline post-COVID infection is because of the multisystem role of COVID-19 inflammation. There is increased regulation of pro-inflammatory cytokines such as IL-1, IL-6, and TNF-α and other inflammatory mediators in the serum and Cerebrospinal Fluid (CSF)7, 8 Thus, in the study population, a venous blood sample was taken for IL-6 levels to determine the relationship between neurocognitive dysfunction and IL-6 levels, and it was revealed that among 29 patients who had impairment in delayed recall, seven patients (24.13%) had raised IL-6 levels. CRP was also done to rule out other causes of inflammatory conditions, and it was negative in all the patients. This finding was statistically significant, with a positive correlation between impairment in delayed recall and raised levels of IL-6. This was in line with another study, which concluded that an inflammatory source is responsible for post-viral physical and mental affective disorders. 19 The demographic variations were also seen in our study, where the majority (62.26%) of the patients presenting with neurocognitive symptoms had developed mild-to-moderate severity of COVID-19 infection. 20 However, this differed from the study by Hosini et al., 21 where only hospitalized patients were included, and memory issues were seen in 31.5% of the study population. Also, compared with another study by Philippe et al., 22 it was discovered that the group with severe infections fared worse on long-term episodic memory tests. The demographic disparity was not statistically significant in our study because of the small sample size.
Limitations
It is important to acknowledge the limitations of this study, such as the relatively small sample size, uncontrolled study design, and potential influence of other confounding factors. Additionally, quality of life and daily functioning were not assessed. The study focused on a specific population in the Kashmir region, and the findings may not be directly generalizable to other geographic or demographic contexts. Moreover, the study population’s COVID-19 vaccination was not considered. These factors may have influenced the cognitive deficits observed in this group.
Conclusion
In conclusion, the research paper shows that cognitive abnormalities can be seen even after a 12-month SARS-CoV2 infection and provides valuable insights into the relationship between IL-6 and cognitive impairments, particularly in delayed recall. These findings contribute to our understanding of COVID-19’s long-term consequences and underscore the need for comprehensive rehabilitation strategies and potential therapeutic interventions targeting inflammatory pathways. Further research is warranted to explore the underlying mechanisms and develop effective strategies to mitigate the cognitive impact of COVID-19 on affected individuals and communities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Ethical approval was obtained and clearance was taken from institutional review board (IRB) with reference number: IRB GMC/PSY 344 on 25th January 2023.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.