
Abstract
Background:
Functional impairment has been convincingly established in the euthymic/ remitted phase of bipolar disorder (BD). Though deficits in social cognition, especially theory of mind (ToM), predict functional impairment, the association has not been consistently proven.
Methods:
Thirty remitted subjects with BD (as per DSM 5) and 30 age- and gender-matched healthy controls were screened for eligibility and the sociodemographic details and ToM scores, that is, first-order ToM, second-order ToM, and Faux pas, were collected. In subjects with BD, functioning was assessed using Functioning Assessment Short Test (FAST) and illness variables were collected.
Results:
No significant difference was found in occupation or education between the groups. Remitted subjects with BD had statistically significant deficits in all domains of ToM, that is, first-order ToM (r = 0.65), second-order ToM (r = 0.69), and Faux pas (r = 0.75). Significant correlations existed between first-order ToM and FAST total score, as well as second-order ToM and FAST total score, but the correlations dropped after controlling for duration of illness and number of depressive episodes. Quantile regression analysis showed that the only factors which predicted global functional impairment was a higher number of episodes (βτ= –0.45, SE = 3.51, t = 0.13, P = 0.04), while all other illness variables and ToM failed to predict the global functioning.
Conclusion:
Though there seems to be an association between ToM and functioning, only illness variables predicted functional impairment in subjects with BD. We need prospective studies to delineate the contributors to functional impairment.
Subjects with BD continue to have significant ToM deficits even during the remitted phase; the only factor which predicted global functioning was a higher number of episodes; first-order ToM, second-order ToM, or faux pas did not predict global functioning.Key Messages:
ToM deficits were evident among individuals in all the three phases of bipolar disorder (BD), namely manic, depressive, and euthymic phases.2, 3 While one might expect relatively lesser ToM impairments in the remitted phase, the deficits observed were certainly not negligible. Three meta-analyses4–6 estimated the effect sizes of ToM deficits in the remitted state to be in the moderate range (0.5 < d <0.8), with no significant difference when compared to subsyndromal mood state, but lesser than the deficits seen during acute mood (mania) state (d =1.23). 4 Though the influence of illness variables over ToM vary across studies, in some studies, global cognitive impairment and history of psychotic symptoms seem to worsen the degree of ToM deficits.7–10
Multiple studies had consistently shown that the unemployment rate was as high as 55% in BD. 11 Functional outcomes in BD are affected by various factors such as personality, current level of depressive symptoms 12 as well as age, course, insight into positive symptoms, and lifetime substance use disorders. 13 However, there is increasing evidence indicating that social cognitive deficits contribute substantially to functional outcomes in individuals with schizophrenia, 14 but there is less research evidence in BD. While some studies have shown positive association 15,16 between ToM deficits and functional impairment in BD, others have not.17–20,21 Among ToM tasks, a strong association was found between poorer faux pas performance and lower Functional Assessment Short Test scores in one study, 22 but such association was not consistent in other studies.17, 23 It is also possible that the association was significantly influenced by subsyndromal depressive features. 24
Social cognition, especially ToM, seems to be under a substantial cultural influence. Individual cultural schemata and interpersonally shared cultural models determine how humans interpret each other’s experiences and guide their actions.25, 26 Functional magnetic resonance imaging studies demonstrate that, based on the cultural background of the test subject, neural correlates of ToM abilities may differ significantly.27, 28 As tools developed to assess social cognition in one culture may not be useful in another culture, assessment of ToM using culturally validated tools in the Indian population is necessary. 29
In view of multiple methodological issues like administration of different tests to assess functioning and social cognition, heterogeneous populations, low sample size, assessment at different stages of illness, presence of subsyndromal mood symptoms, and paucity of data on neurocognition, more research in this area will improve our understanding about ToM and its effect on functioning in remitted BD. 21 Thus, our primary aim was to compare the ToM abilities among remitted subjects with BD and healthy controls. The secondary aim was to find any association among illness variables, the ToM, and functioning in subjects with BD, and if any exist, then to find out which factors predict the functioning in BD. We hypothesize that subjects with BD have ToM deficits even during the remitted phase of illness and that ToM will predict functional impairment in BD.
Materials and Methods
This is a cross-sectional study with a control group, in which we recruited euthymic/remitted subjects with BD and healthy controls based on eligibility criteria.
Recruitment of Participants
We recruited 30 subjects with BD (diagnosed by DSM 5) from the outpatient psychiatric services of a tertiary care medical college, during the period of May 2017 to September 2018, with prior informed written consent. We included subjects with BD who were 18 to 60 years old; of either gender; fulfilling DSM 5 criteria for bipolar affective disorder, either Type 1 or Type 2, using structured clinical interview for DSM5 (SCID 5); who are able to read and understand Tamil (local vernacular language) and who are currently in remission as defined by scores on the 17-item Hamilton Rating Scale for Depression (HAMD; score ≤8) and Young Mania Rating Scale (YMRS; score ≤ 6) for a period of eight weeks. We included this stricter definition of euthymia to minimize the influence of subsyndromal mood symptoms on the ToM tasks.21, 30 We excluded subjects with BD if they had history of psychotic symptoms during the episodes, substance use disorders (except nicotine), or other psychiatric axis I comorbidities (using Mini International Neuropsychiatric Interview, MINI plus 5.0); clinically determined severe cognitive impairment, mental retardation or neurodegenerative disorders; general medical illness that could impair cognitive performance; received electro convulsive therapy in the past six months, or severe visual or hearing impairment impairing test performance. Relatives of patients who were hospitalized for medical illness were screened for eligibility as controls. Age-, gender-, and education-matched healthy controls were included who did not have any lifetime psychiatric diagnosis (as established by MINI plus 5.0), neurological illness, or severe cognitive impairment that could impair the test performance. Ethics clearance was obtained from the Institutional Ethics Committee. The investigator (E.K) had undergone supervised three-day training organized by the authors of the culturally validated social cognition tool, The Social Cognition Rating Tools in Indian Setting (SOCRATIS), focusing on tool administration and scoring.
Assessments
With written informed consent, sociodemographic data and relevant illness variables were collected from the participants and cross-checked with the health records. Current mood symptoms were assessed using the 17-item HAMD and YMRS.
SOCRATIS, well-validated in Indian settings, 29 was used to measure three areas of social cognition, namely ToM, social perception, and attribution bias. The ToM task included two first-order and two second-order false belief picture stories, two metaphor-irony stories, and five faux pas recognition stories, which were presented as cartoon sequences. These story-based tasks examine the ability, at different complexity levels, to “meta-represent” mental states of others. Based on test performance, the tool scores ToM as first-order ToM (FOT) index (FOTI), second-order ToM (SOT) index (SOTI), and faux pas composite index (FPCI). If the subject scores less index scores, it suggests severe ToM deficits.
Functioning status was assessed in subjects with BD using Functional Assessment Short Test (FAST), 31 which assesses six specific areas of functioning: autonomy, occupational functioning, cognitive functioning, financial issues, leisure time, and interpersonal relationships, with higher scores indicating higher functional impairment.
Statistical Analysis
All calculations were performed using R software. The normality of data was checked using the Shapiro–Wilk test, which showed that the data were non-normally distributed. Between-group differences (BD vs. healthy controls) among sociodemographic variables were tested with the Mann–Whitney U test for continuous variables and Fisher’s exact test for discrete variables. Between-group ToM scores (FOTI, SOTI, FPCI) were tested for any statistically significant difference using Mann-Whitney U test, with the significance level set at P =0.05. Effect size (for nonparametric tests) 32 was calculated using Cohen r = z/√N. In order to understand the correlation among illness variables, ToM, and functioning (FAST domains and global), Spearman’s correlation was used. Partial correlation was used to find the degree of correlation between ToM and functioning (FAST scores) in subjects with BD, after controlling for illness variables of interest. Quantile regression was carried out with illness variables and ToM variables as independent variables while using FAST (individual and total scores) as the dependent variable. The goodness of fit of the quantile regression model was assessed by comparison with the null/base model (statistical significance set at P < 0.05). Based on βτ coefficients, the relative contribution of each independent variable over the FAST scores was deciphered.
Results
Sociodemographic and Illness Details
The mean age was not statistically different (U = 375, P = 0.27) between BD (35 ± 8.48) subjects (n = 30) and healthy controls (36.27 ± 7.01) (n = 30) (
Sociodemographic Profile of Subjects with BD (n = 30) and Healthy Controls (n = 30)
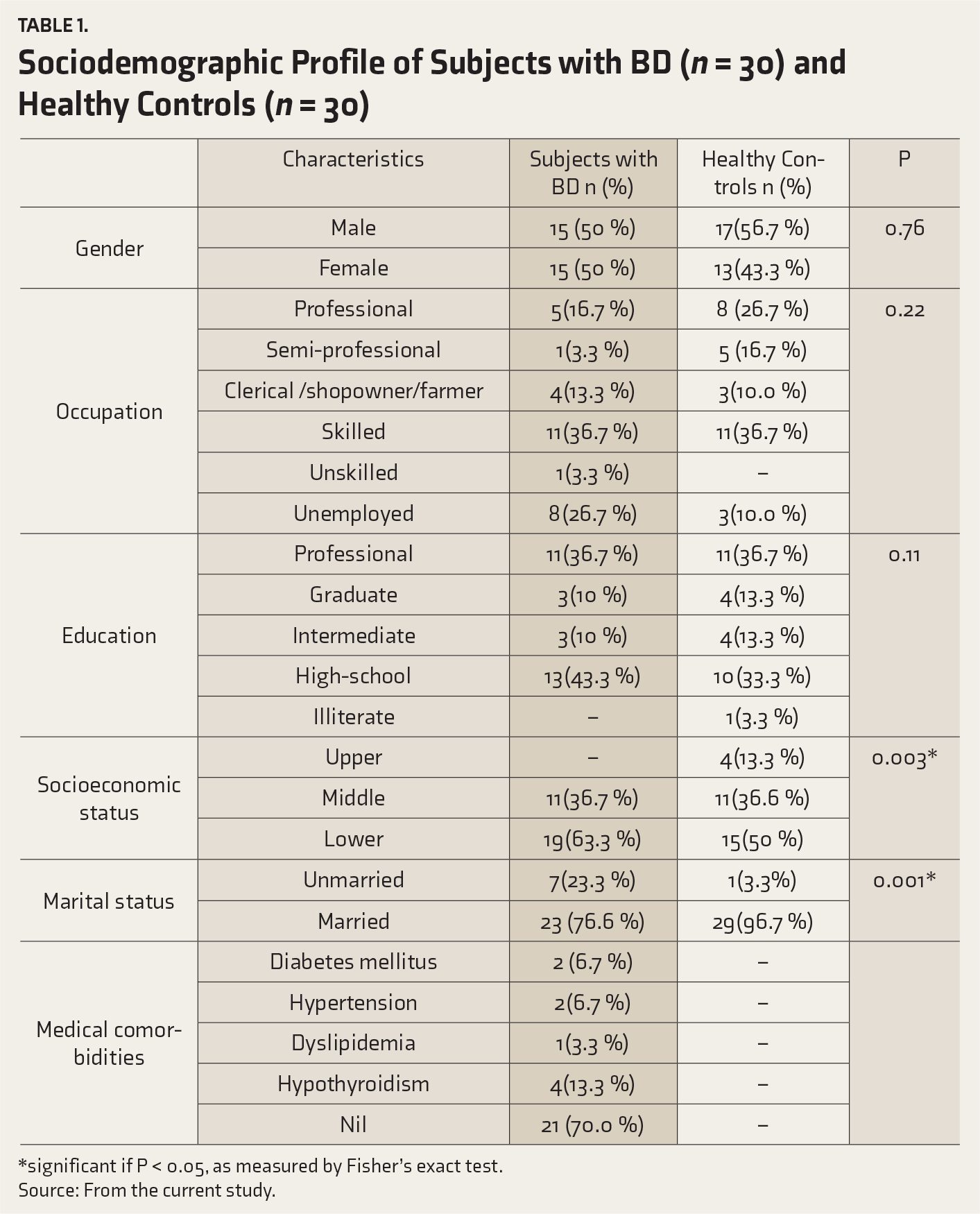
Source: From the current study.
Illness Variables in Subjects with BD (n = 30)
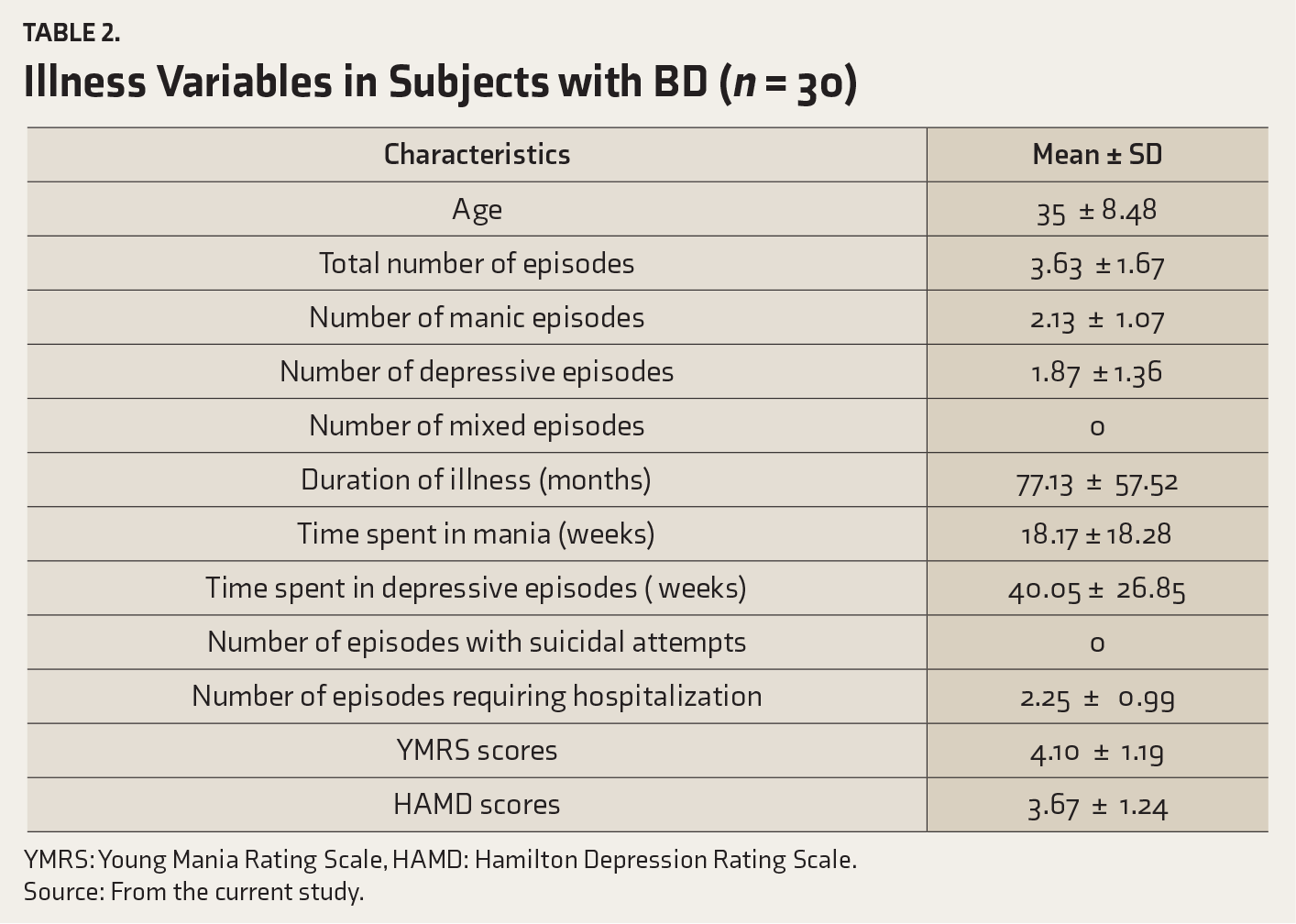
YMRS: Young Mania Rating Scale, HAMD: Hamilton Depression Rating Scale.
Source: From the current study.
ToM Scores
In subjects with BD (
Comparison of ToM Scores Among Subjects with BD (n = 30) and Healthy Controls (n = 30)
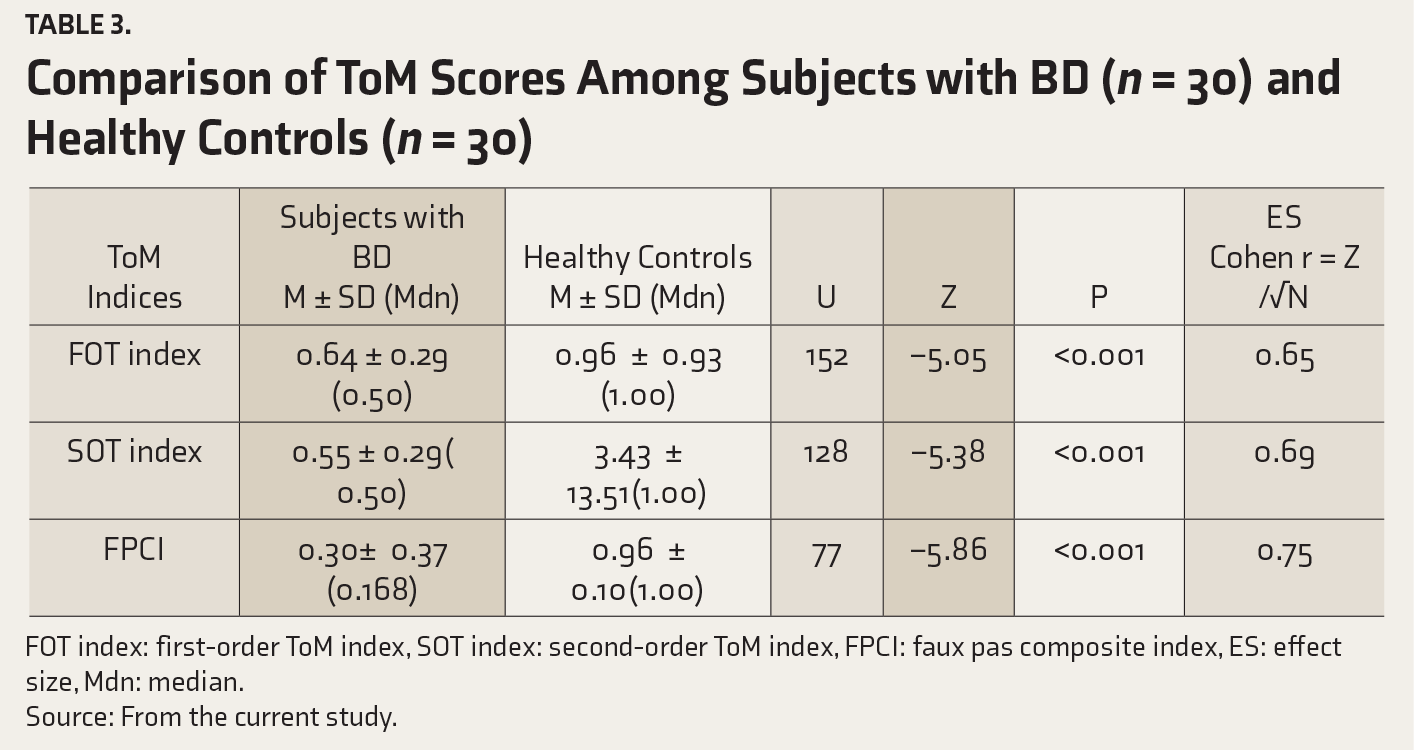
FOT index: first-order ToM index, SOT index: second-order ToM index, FPCI: faux pas composite index, ES: effect size, Mdn: median.
Source: From the current study.
Functioning in Subjects with BD
Mean FAST scores indicated that interpersonal (9.17 ± 4.2), occupational (7.37 ± 4.38), and cognitive (7.40 ± 4.28) domains of functioning were more affected than financial (1 ± 1.11), autonomy (1.30 ± 1.91), and leisure (1.30 ± 1.02) domains of functioning. Correlation between illness variables, ToM variables, and FAST (individual item based and total) scores was evaluated using Spearman’s rho correlation (
Correlation Among Illness Variables, ToM Scores and Functioning (Individual Item and Total–FAST Scores) Among Subjects with BD (n = 30)
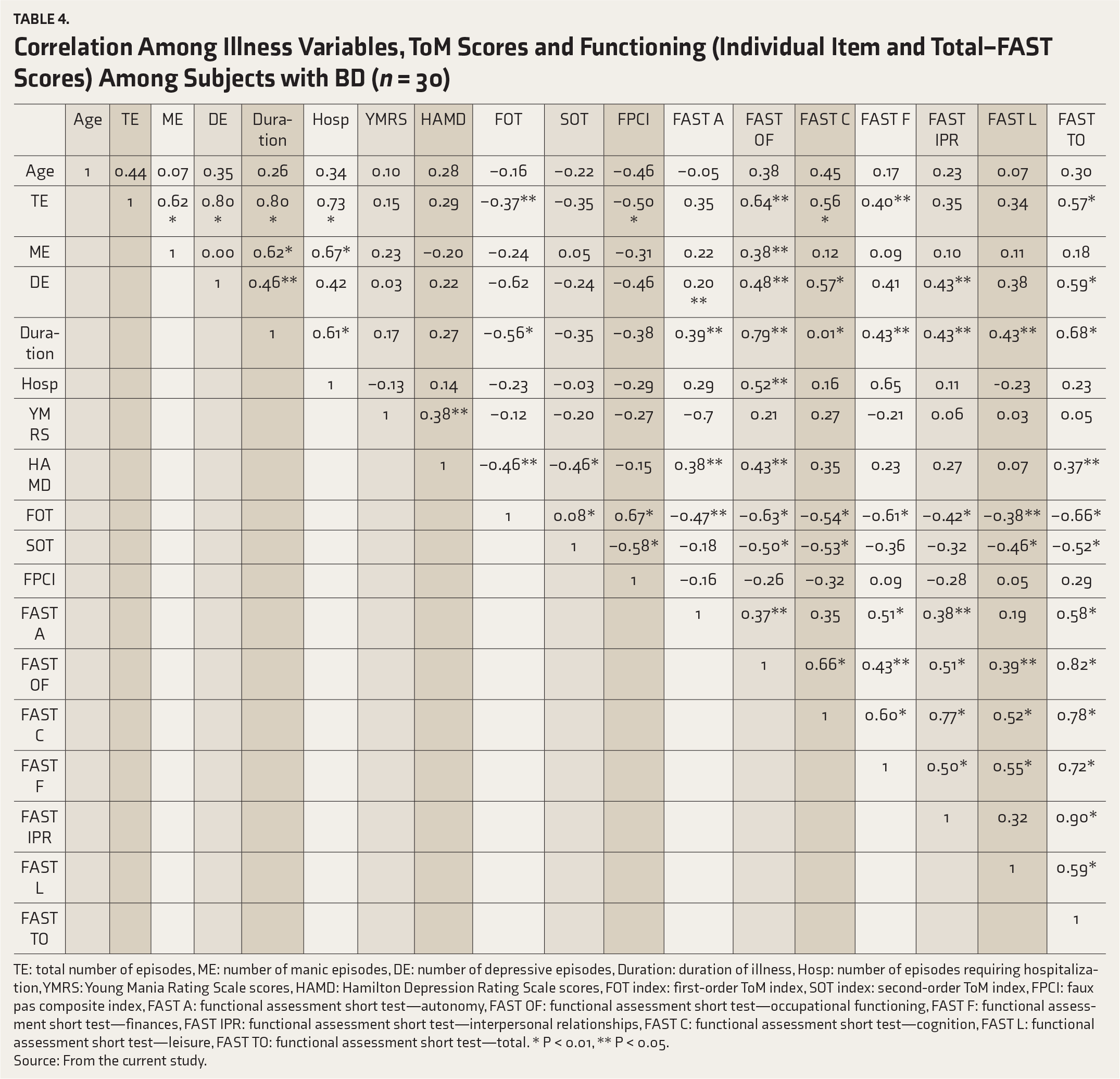
TE: total number of episodes, ME: number of manic episodes, DE: number of depressive episodes, Duration: duration of illness, Hosp: number of episodes requiring hospitalization, YMRS: Young Mania Rating Scale scores, HAMD: Hamilton Depression Rating Scale scores, FOT index: first-order ToM index, SOT index: second-order ToM index, FPCI: faux pas composite index, FAST A: functional assessment short test—autonomy, FAST OF: functional assessment short test—occupational functioning, FAST F: functional assessment short test—finances, FAST IPR: functional assessment short test—interpersonal relationships, FAST C: functional assessment short test—cognition, FAST L: functional assessment short test—leisure, FAST TO: functional assessment short test—total. * P < 0.01, ** P < 0.05.
Predictors of Functioning in Subjects with BD During the Remitted Phase
In order to improve the model accuracy and prevent dilution of the model, we used the significantly correlated variables (total number of episodes, number of depressive episodes, duration of illness, FOTI, SOTI) as independent variables and FAST (total and sub-items) as a dependent variable into the final models (
Predictors of Global and Interpersonal Functioning (FAST) in Subjects with BD (n = 30)
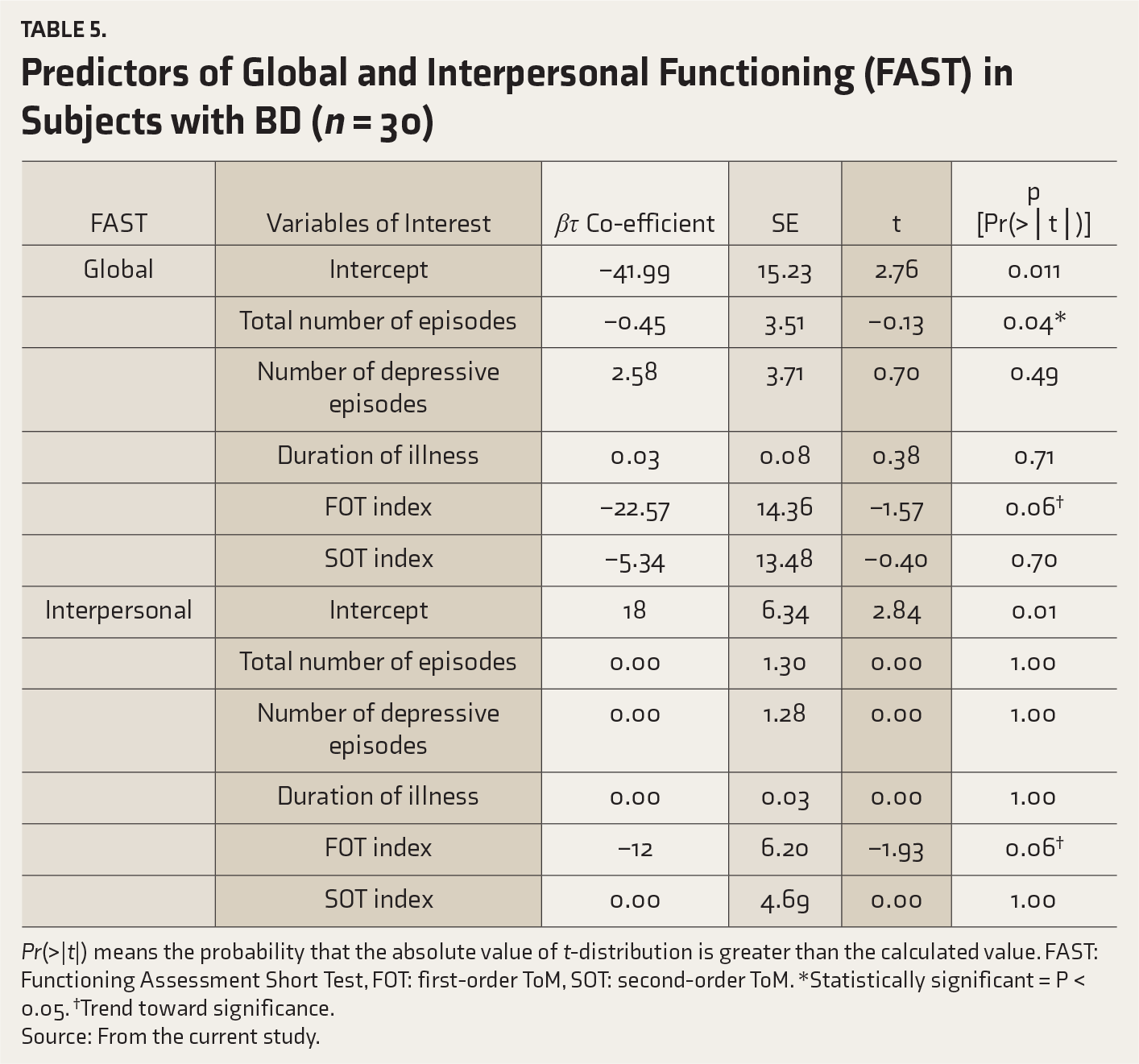
Pr(>|t|) means the probability that the absolute value of t-distribution is greater than the calculated value. FAST: Functioning Assessment Short Test, FOT: first-order ToM, SOT: second-order ToM. *Statistically significant = P < 0.05. †Trend toward significance.
Source: From the current study.
With regard to interpersonal functioning (FAST), the model showed goodness of fit (∆F (5, 24) = 5.18, P = 0.002), in which all independent variables lost significance, except FOTI, which showed trend towards significance (βτ = –12, SE= 6.2, t = –1.93, P = 0.06). Among other models, the models which showed goodness of fit were FAST occupational (∆F (5, 24)= 6.60, P = 0.0005), FAST cognitive (∆F (5, 24) = 12.26, P = 0.0003), and FAST leisure (∆F (5, 24) = 6.18, P = 0.0008) as dependent variables, in which none of the independent variables showed a significant contribution (
Predictors of Occupational, Autonomy, Cognitive, Financial, and Leisure Components of Functioning in Subjects with BD (n = 30)
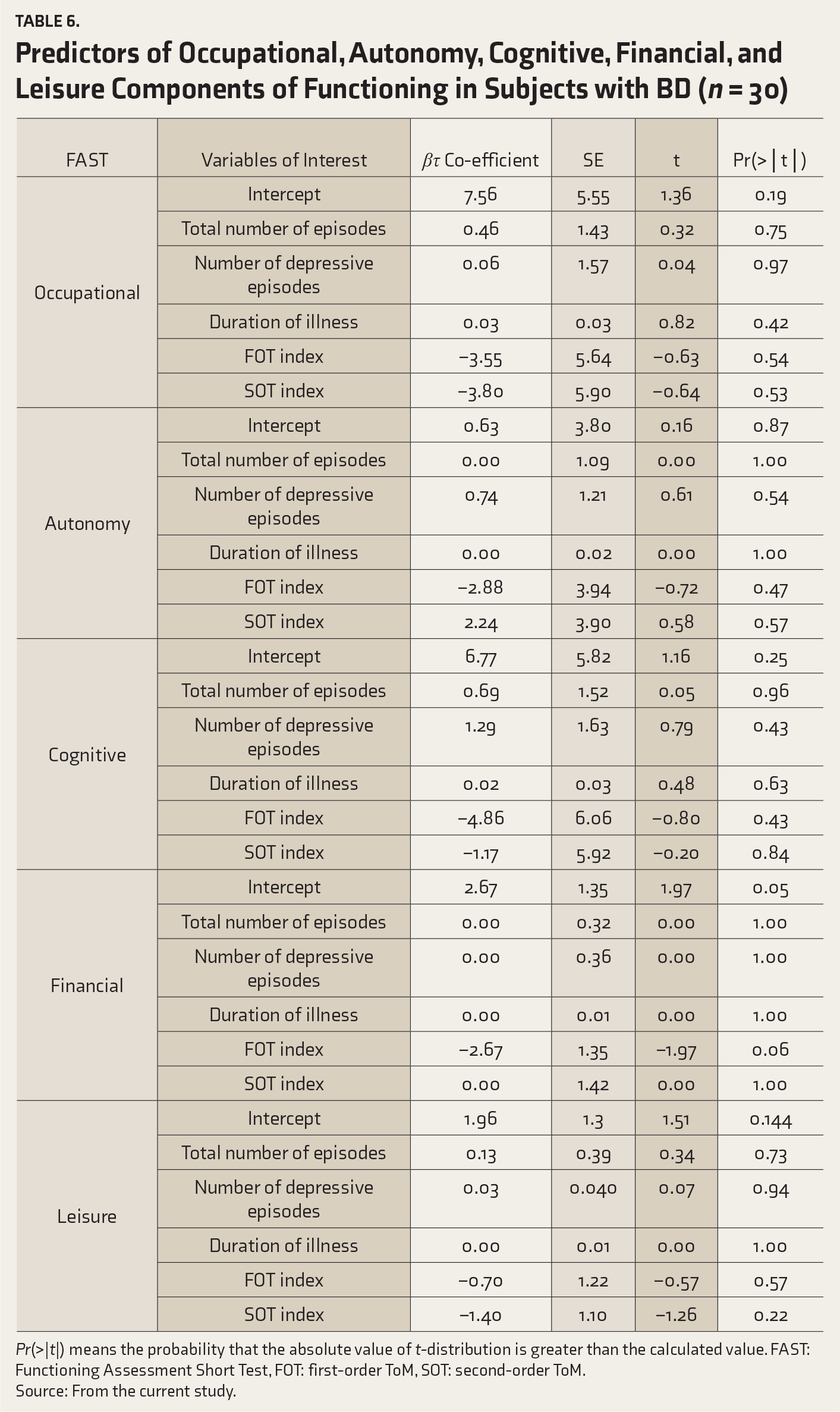
Pr(>|t|) means the probability that the absolute value of t-distribution is greater than the calculated value. FAST: Functioning Assessment Short Test, FOT: first-order ToM, SOT: second-order ToM.
Source: From the current study.
Discussion
Our findings suggest that significant ToM deficits (FOT, SOT, and faux pas) are present during euthymic/remitted state of BD when compared to healthy controls. A significant association existed between global functioning (FAST–Total) and most of ToM variables, that is, with FOT (P < 0.001), SOT (P = 0.003), but not with faux pas (P = 0.17). A higher number of episodes predicted poor global functioning, while ToM did not predict global functioning in subjects with BD during the remitted phase.
ToM (first-order, second-order, and faux pas recognition) deficits seem to persist even during the remitted phase of the BD. This is in line with multiple metanalyses4–6 that had also shown that ToM deficits persist irrespective of the form (cognitive or affective) and type of assessment tools.
The link between ToM and functioning has been explored in all the symptomatic phases of BD, that is, depressive,18,33–35 manic,18, 33, and mixed phases. 35 Studies that explored the association between ToM and functioning in euthymic/remitted BD had shown mixed results, with some reporting significant association15,16,18,22,24,36 and others not.17, 20 A possible link exists between depressive symptomatology and global functioning, where depressive symptoms explain 17%–35% of the variance in the global functioning.18, 33
Our results show that FOT is most consistently correlated with all the domains of functioning (autonomy, financial, occupational, cognitive, interpersonal, and leisure). But there was no consistent correlation with higher-order ToM such as faux pas stories and SOT tasks in our study. These results are in line with existing literature that shows that out of 12 studies, only two16,22 showed a positive association between faux pas (higher-order ToM) and functioning, especially social functioning. 21 In our study, the only illness variable which significantly predicted global functioning was a higher number of episodes, while all other illness variables and ToM tasks (FOT, SOT, faux pas) lost their contribution to variance in global functioning impairment. The interesting question which arises now is which factor(s) mediates the influence of illness variables over functional impairment in BD. The absence of any significant prediction of functional impairment by ToM17, 23 makes us wonder whether alternate mediators like neurocognition would mediate the influence of illness variables on functioning. 37 On the contrary, a recent study has shown that social cognition moderates the effect of neurocognitive deficits over community functioning. 38 In view of the mixed results, prospective studies looking into the association of illness variables, social cognition, neurocognition, and functioning needs to be done.
Recently, social cognition and interaction training (SCIT) has been investigated in schizophrenia39, 40 and has shown promising preliminary results. But to our knowledge, only two studies exist in BD.41, 42 The study which compared the effects of SCIT and treatment as usual on social cognition in outpatient subjects with BD 42 had shown that SCIT caused small but significant improvement in ToM, facial emotional recognition, and hostility attribution biases, but not in social functioning. The authors proposed that improvement in BD may be better if SCIT is modified by including tasks involving comprehension of more complex social situations rather than lower order facial emotional recognition.
Though many studies had shown that subsyndromal depressive symptoms influence the social and occupational functioning,16,17,33 our study did not show such a correlation (FAST-interpersonal or FAST-occupational), possibly because of our stricter definition of euthymia and the higher HAMD scores in other studies. In one such study, 22 low functioning (FAST > 11) and high functioning (FAST ≤ 11) remitted bipolar groups were compared for verbal social cognition using comprehension faux pas test, which showed that verbal social cognition and subsyndromal depressive symptoms significantly predicted poor functioning in the low functioning group but not in the high functioning and control groups. Such an association between subsyndromal depression and functioning was not universally proven in all studies.43, 44 At the same time, though subsyndromal depressive symptoms may have a lesser influence on ToM tasks, in many studies it has been found that subsyndromal depressive symptoms have a mediating effect between emotional perception deficits and social functioning.22–24,33,36,43–45
Based on the correlation between functional impairment and illness variables like longer duration of illness, 30 higher number of episodes, especially depressive episodes, and longer time spent in depressive episodes in our study, we hypothesize that functional impairment could be a consequence of the progressive nature of the illness rather than subsyndromal depressive symptoms. There is some evidence in the short- or long-term (3 to 10 years) prospective studies that the severity and frequency of bipolar depressive episodes contribute to cognitive decline and poor psychosocial functioning, 46 possibly through dysregulated neuroinflammation. 47 Similar inconsistent evidence also suggests that the frequency and severity of manic episodes may lead to poor psychosocial functioning and cognitive impairment, 48 but our study did not find such association. It is possible that this causal relationship could not be established with the cross-sectional nature of the current study and thus, it may need longitudinal studies using more objective rating scales rather than subjective, self-report scales like FAST. 33
Limitations
This study was less powered to detect a statistically significant association, and this could have influenced our statistical interpretations. Second, confounding variables such as intelligence, which could influence the social cognition scores, were not formally assessed. This could have been partly mitigated by the use of SOCRATIS, which assesses intellect and memory by use of control questions, which are scored during the final scoring of the tool. This is also mitigated by a careful, clinical evaluation of premorbid intelligence. Third, we did not evaluate the neurocognitive variables like processing speed, attention, and verbal recall which could interfere or influence the social cognition task performance. Fourth, the above findings are restricted to patients in the remitted phase of bipolar I disorder without a history of psychotic symptoms. Though subjects with BD with a history of psychotic symptoms have been known to have more ToM deficits when compared to those without a history of psychotic symptoms,8, 9 we intentionally excluded them to avoid contamination of results and thereby to find the deficits that are exclusive to BD. Thus, the generalization of our findings to other types/phases of BD may not be possible and that would require a study that looks into differential social cognition findings across other bipolar diagnoses/phases. Finally, it is known that accurate predictions cannot be guaranteed in a cross-sectional study and rather should be based on a longitudinal study. Temporality assumption (dependent variable has to occur after the independent variable) cannot be assured in a cross-sectional study. But still, findings of a cross-sectional study can pave the way for testing those variables in later longitudinal cohort studies.
Conclusions
There seems to be an association between ToM deficits and global functioning in subjects with BD during the remitted phase, but they lose their ability to predict when illness variables such as a higher number of episodes are taken into account. Caution needs to be exercised in interpreting our findings, in view of the cross-sectional nature of the study and the low sample size. Thus, prospective studies on the effect of ToM deficits on functioning are needed to understand the role of preexisting social cognition deficits, especially ToM deficits, if any, in BD.
Footnotes
Acknowledgements
We would like to thank Dr. Merlin Veronika, Visiting Faculty, PSG Center for Research and Bioethics, for her profound support in analyzing and interpreting the data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.