
Abstract
Background:
Caregivers play an important role in children’s development. Therefore, they need to recognize the learning difficulties that their children face and support them to ensure learning gains and prevent secondary complications. Nevertheless, supporting a child with a learning disability can be challenging for caregivers in many ways. 1 This study investigated caregivers’ knowledge of dyslexia, their challenges when raising children with dyslexia, and the support they seek to raise such children.
Methods:
Ten individual in-depth interviews (IDIs) and four focus group discussions (FGDs) were conducted among 30 caregivers in Sri Lanka. Initial codes were generated using open coding from the transcripts, leading to sub-themes and themes.
Results:
Thematic analysis revealed a lack of knowledge of dyslexia-type difficulties among caregivers and in society, giving rise to misconceptions, leading to labeling and abuse of children. Caregivers feel emotionally pressured, helpless, stressed, and depressed in bringing up children with dyslexia, creating family disputes. Further, as a family, they have a sense of rejection and discrimination from school and society. Caregivers receive insufficient support from the education and health sectors due to multiple complexities such as myths, misbeliefs, inadequate knowledge and skills, unavailability of resources, and inaccessibility to services.
Conclusions:
Caregivers and families of children with learning disabilities demand more attention to improve their mental health and family harmony, which in turn improves children’s educational and health status. Sri Lankan health, educational, and social services should be optimized to reach the families of children with dyslexia-type difficulties.
Caregivers of children with dyslexia in Sri Lanka face many challenges related to identifying and supporting their children’s condition. Caregivers and families feel rejected, discriminated and pressured to raise their children with learning difficulties due to lack of social support. Caregivers of children with learning difficulties face parenting stress and depression, which in turn give rise to family conflicts and abuse, but no attention is given to their mental health status.Key Message:
Primary caregivers are the first observers of child development. Therefore, they need to understand the development process and delays to identify unusual development patterns or the challenges their children face. When knowledge of child development is not easily available to caregivers, misbeliefs and myths about developmental delays arise.
Even though research evidence is scanty in the country, a study in 2015 revealed that 22.5% of Sri Lankan school children needed help with reading, spelling, and related activities in the Sinhala language. 2 On this ground, raising and supporting children with dyslexia can be challenging in many ways. 1 First, identification may be difficult if caregivers need more understanding. Even if identified, caregivers may not know how to support such children. Support services may also not be widely available, and lack of such support makes caregivers exhausted, frustrated, and stressed. 3
Caregivers’ Ability to Identify Dyslexia-Type Difficulties
Dyslexia has a neurobiological origin that mainly affects decoding ability and language phonological processing. 4 It is possible for children with dyslexia to show signs at an early stage of their life. Therefore, one can assume that caregivers may be able to notice them. However, according to research evidence, caregivers may immediately identify initial signs if the condition is familial. Other caregivers may not be able to recognize them.5-7 An Indian study reported that 70 out of 100 (70%) parents had inadequate knowledge, and the mean overall knowledge score was below 50 out of 100 (50%). 5 Further, a qualitative study conducted in Turkey also revealed that parents do not have adequate knowledge of dyslexia. 6 Another recent study highlighted that caregivers’ inadequate knowledge leads to delays in diagnosing dyslexia. 7
With this evidence, it is understood that parents’ awareness and knowledge of dyslexia are not optimal. Hence, they may depend on dyslexia interventions that are not scientifically proven. 8 In Germany, it was found that only a minimal number of parents go for evidence-based therapy. 9 Caregivers whose children have reading difficulties make them extensively practice reading and writing at home. 10 Parents hesitate to seek professional help because they feel embarrassed to admit their children have learning difficulties. 11 In light of the above evidence, a Sri Lankan study shows that caregivers’ involvement in the education of a child with learning difficulties could be minimal and even inappropriate due to their lack of knowledge and the support needed. 12
Impact on Children
Lack of caregiver knowledge may also bring negative consequences to children. A report from Namibia highlights how a mother scolded and beat her son out of frustration when the child struggled to read and write. 13 A mother in China scolds and beats her child for lower exam scores and writing characters incorrectly. 14 Parents in China pressurize children struggling with learning to achieve higher grades. 15 Caregivers’ reactions may also vary based on cultural context. Especially in Asian cultures, social expectations play a demanding role in one’s education. Hence, caregivers may try hard to educate their children with learning difficulties to meet those expectations without realizing what they can achieve.16,17
When caregivers get to know that their children have learning difficulties, it can create frustration. Mostly, the initial reaction is denial, 18 and they reject the evidence that their children are having learning difficulties while blaming themselves. 19 In India, 76 out of 100 (76%) mothers who have children with learning difficulties are anxious. 20 In Turkey, most mothers (85 out of 100) in their cohort are overly emotional. 21 Studies also show that these caregivers suffer from depression and excessive parenting stress compared to those without children with dyslexia.22,23 Families of children with dyslexia are negatively affected because of continuous disagreements on parenting matters among parents.15,23 All these can lead to emotional pressure for children and their caregivers. This is where support services have a vital role to play.
Availability of Identification Practices, Tools, and Support Services
Research on the support services available for individuals with dyslexia-type difficulties from 195 countries shows that they need to be more adequate in most contexts. 24 On the one hand, caregivers may need to be made aware of what is available. For example, a study done in Sri Lanka among primary school teachers found that 58 out of 100 (58%) participants were not aware of any dyslexia identification practices in the country, and 75 out of 100 (75%) teachers were not aware of any place where dyslexia identification and evaluation take place. 25 If teachers are unaware of such services, it is possible to assume that caregivers may have even less awareness. Another research report is a lack of knowledge among teachers in Sri Lanka, 26 which can make dyslexia identification more difficult because they cannot lead caregivers to relevant support services or educate them on their children’s educational needs.
Even if support services are available, their ability to adequately support parents is another issue worth investigating. When teachers are not knowledgeable, caregivers feel abandoned and helpless. 1 In such a context, blaming one another for incompetency, inadequacy, and frustration occurs. 15 Caregivers feel that they are discriminated against by the educators due to the knowledge gap when going through assessment and planning for their children with dyslexia, just because caregivers do not understand specific terms that the professionals use. 27 This can become a power gap and make caregivers feel less confident in parenting and supporting their children’s education. 27
Positive results have also been demonstrated when support services are available for caregivers. For example, a mixed-method study in Greece among 299 parents of children with autism spectrum disorder who were already receiving care through support groups found that they perceived less child-related stress and felt accepted after they had joined support groups. 28 Further, caregivers learned about normal and abnormal development, growth patterns, new teaching strategies, and how to reach funding mechanisms after joining various support groups. 29 Another Chinese study reveals that parents request social support and more information to support their children with special needs. 30 A quantitative study in Sri Lanka among 200 primary caregivers of children with cerebral palsy found that, whether formal or informal, perceived social support acted as a protective factor of caregivers’ psychological well-being, which in turn improved family dynamics and responsive and responsible caregiving, in line with other research.31,32
Rationale
According to available research evidence, children with learning difficulties may demonstrate different behavioral patterns, emotional development, and cognitive growth. In such situations, caregivers must identify those differences, understand what they mean, and know how to support children with difficulties. However, research also shows caregivers do not have a sufficient understanding of these aspects, support services available for such caregivers are inadequate in most contexts, and the existing support services may also be unable to provide the service that caregivers require. Although the studies discussed above provide some indication of their struggle in the process of diagnosing children with learning difficulties and the provision of parental support, they are scarce, particularly in the Sri Lankan context, according to available local evidence. More systematic investigations are needed to examine caregivers’ perceptions of their struggles, how the challenges influence their health and the family, and what support they need in a developing country where a proper system is not yet established. Such investigations can provide insights into how health services can be uplifted and how education services can assist caregivers. This study investigated these aspects in depth based on the following research questions.
Research Questions
RQ1: To what extent are Sri Lankan primary caregivers knowledgeable of dyslexia-type difficulties?
RQ2: What challenges do primary caregivers of children with dyslexia face in Sri Lanka?
RQ3: According to primary caregivers’ perceptions, what resources and services are needed in Sri Lanka to support children with dyslexia?
Methods
A qualitative phenomenological study was conducted to answer the research questions.
Context
There are two distinct settings for dyslexia identification in Sri Lanka: private (paid) and public (free) service providers. Therefore, the study settings were purposefully selected to recruit participants representing both services. Lady Ridgway Hospital, Department of Child Psychiatry, Faculty of Medicine, Colombo, and Faculty of Medicine, Kelaniya were selected to represent the public sector, and three private hospitals in Colombo, Gampaha, and Kandy districts were selected to represent the private sector. They represent the limited places available to provide regular dyslexia identification services in the country. As the diagnosing mechanism for learning disabilities is still developing in the country, children already diagnosed with “probable dyslexia” were included in the research.
Participants and Sampling
Twenty primary caregivers who received services from the public sector and ten who received services from the private sector were selected for the study. As the public sector is widely distributed in the country and provides the majority of the services available, more participants from the public sector were chosen. Criterion sampling was used to select participants. The criterion was: “primary caregivers of children aged between five and ten years who were screened within Sri Lanka for reading difficulties and identified as having probable dyslexia.” This method was devised based on the sampling methods used in similar studies. 5 To arrange interviews, the participants were prior contacted over the phone by the author as a PhD student. Among the participants were 19 mothers, two fathers, and nine other primary caregivers (grandparents, uncles, and aunts). Participants’ education qualifications varied from grade ten to postgraduate qualifications, their ages varied from 26 to 68 years, and they came from various occupations representing different social statuses. Initially, 35 participants were contacted, but after exclusion and consenting procedures, only 30 participants were recruited. Caregivers with children who had partially gone through the process of identifying learning issues and were fully or partly evaluated in another country were excluded.
Data Collection Methods
Interviews are considered the most suitable method to collect in-depth content-rich information on personal experiences. 33 Focus group discussions allow information gathering and participants to discuss their personal experiences in common with others who are interested. 34 This also allows for the exploration of their views in an integrated manner, giving rise to different perspectives of the experienced event. 35 Therefore, face-to-face FGDs were conducted among caregivers representing the public sector due to their personal preference. Face-to-face in-depth interviews were conducted among caregivers who represented the private sector as they preferred IDIs over FGDs due to logistic and personal issues in timing and setting.
Data Collection Instruments
Open-ended questions in a semi-structured interviewer guide were used in IDI and FGDs. Three experts and three caregivers validated the questions. The questions covered aspects such as caregivers’ knowledge of dyslexia, their beliefs, thoughts, and perception of dyslexia, dyslexia identification processes in Sri Lanka, challenges caregivers face during dyslexia identification and remediation, and their views on how to improve the current status of services in the country. The first author (NP) herself acted as the primary data collector after receiving training while she was a PhD student after completing her MPhil.
Data Collection Procedure
Data was collected from June 2021 to March 2022. As Sri Lanka is a multiethnic country, Sri Lankans use Sinhala, Tamil, and English for communication. Therefore, interviews and FGDs were conducted in all three languages separately. The interviews lasted for about 30–45 minutes, and FGDs lasted for about 60–90 minutes, and all of them were audio recorded. Ten caregivers participated in IDIs, and among them, six were Sinhala speakers, two were Tamil speakers, and two were English speakers. Twenty caregivers participated in three FGDs. Seven participants were there at the FGD, which was conducted in Sinhala; another seven participants attended the FGD conducted in Tamil, and six participants attended the FGD, which was conducted in English. Field notes were taken during data collection by the main data collector and the moderator as well. All data collection sessions were smoothly conducted and audio recorded. Data collection was terminated successfully, and data saturation was observed during the last two interviews.
Data Analysis
The first author did data analysis. First, the recordings were transcribed word for word, and filed notes were added and anonymized. The transcripts were checked with the participants before translation. Then, Sinhala and Tamil texts were translated into English by professional translators. The software ATLAS.ti.8 (from ATLAS;
Ethical Considerations and Credibility
Data collection took place after obtaining ethical clearance, necessary institutional approvals, and also after written informed consent from the participants. The information sheet given to participants before obtaining consent contained all the necessary details the participants should know in understandable language in all three languages used in SL. There was no prior relationship of any sort between participants and researchers that would have influenced their voluntary participation. Participants were asked to use the “identifiers” given at the beginning of the interview to identify themselves. Information was anonymized by replacing their names with coded identifiers when transcribing. Audio recordings were securely stored until transcribing took place and then discarded. The relevant participants checked interview transcriptions before data analysis took place to ensure their accuracy, credibility, and trustworthiness. The first author, as the main data collector and data analyzer, tried to have a neutral mindset about the research area, practiced bracketing, and maintained a reflective diary throughout the process to minimize biases. There were no conflicts of interest, and the project was self-funded.
Results
The results are reported based on the three themes that were generated with seven subthemes (ST).
One of the main subthemes that emerged in the data under this theme was caregivers’ limited knowledge of dyslexia (ST1). The majority (20) of caregivers interviewed did not know what a reading disability was until their children were identified and explained by assessors. However, most (15) of the caregivers mentioned that they could see that “something was wrong with their child,” but did not know exactly what that was, what to do, and where to go for support. Prior experience with dyslexia has helped some caregivers notice difficulties demonstrated by their children. The overall findings showed that the participants could not identify when their children demonstrated difficulties. Only those who had prior experience with such difficulties had some understanding.
This limited knowledge had led to several negative consequences (ST2), which was identified as the second subtheme. There were misconceptions among the caregivers, and they needed to be made aware of the appropriate support that they should provide for their children. Almost all participants agreed that their lack of knowledge had led to late diagnosis as well as hindered caregivers’ ability to stand up for their children’s rights and well-being, which they later regretted. It had also been apparent that caregivers received conflicting information from others once the child was identified as having dyslexia, which had led to confusion.
Overall, findings showed that caregivers lacked knowledge and mostly relied on others or their experience. Further, they either relied on assessors/teachers/doctors or did not believe them. This led them to develop misconceptions, leading to sub-optimal caregiving.
According to the participants, one of the main challenges that caregivers face is discrimination and emotional pressure (ST3). In general, there were negative attitudes toward such children in the school community. All the participants from both the private and public sectors brought up the issue of rejection. Discrimination at school has given rise to new behavioral issues in their children. Another issue highlighted was the discrimination faced by the caregivers against other parents of neurotypical children. Some parents of neurotypical children did not seem to like having children with learning difficulties in the same classroom as their children. Further, the school was getting pressured by such parents, which seemed to affect the functioning of the classroom.
Another challenge that emerged as a subtheme was caregivers’ helplessness, stress, and depression (ST4). The participants highlighted that they felt lost, left out, and lonely. Due to these challenges, they felt more parenting stress, and some were depressed affecting family harmony. They had punished their children, ended up in family separations, and experienced mental disorders related to stress.
An additional challenge caregivers faced, which was identified as a subtheme, was the lack of support they and their children with learning difficulties receive (ST5). The participants explained about occasions in which teachers blamed caregivers for not supporting their children at home. The lack of support from schools has also negatively impacted children. Caregivers were never looked after by either social or health services.
Overall, the participants’ perceptions revealed three main challenges children with dyslexia and their caregivers face. One was the discrimination against such children and their caregivers by the school community, including teachers, peers, and caregivers of other children. Then, the lack of support provided by the school has led to negative educational consequences. Lastly, caregivers also felt helpless, stressed, and depressed because they did not receive any attention and support.
One of the main subthemes that emerged was the lack of facilities for diagnosis, remediation, and accommodation (ST6). Nearly all participants were unhappy that their children were not identified early. For most of the caregivers, the diagnosis had made a positive impact on their lives, clearing doubts. They mentioned that their first reaction to diagnosis was denial and stress; however, with time, they realized the benefit of having a diagnosis. Most participants (18) also valued having a diagnosis as a means of fighting against discrimination at school. The diagnosis helped them to advocate for their children’s rights, as highlighted below.
The next subtheme that emerged was the need for support services for caregivers (ST7). Caregivers were automatically considered fit and able to assist their children by educational and healthcare providers. Some caregivers were not able to give necessary support to their children due to financial constraints. There was no mechanism to provide financial assistance because it was not identified as a disability. In the private sector, services were limited and expensive. In the government sector, services still needed to be improved and distributed. Multidisciplinary services could have been more varied due to a lack of personnel, limited knowledge, affordability, and several other reasons.
Overall, the data revealed two main service requirements: more opportunities for early and proper diagnosis and support services for caregivers to understand how to help their children with dyslexia and themselves. Table 1 summarizes the findings.
Primary Caregivers’ Experiences of Children with Dyslexia.
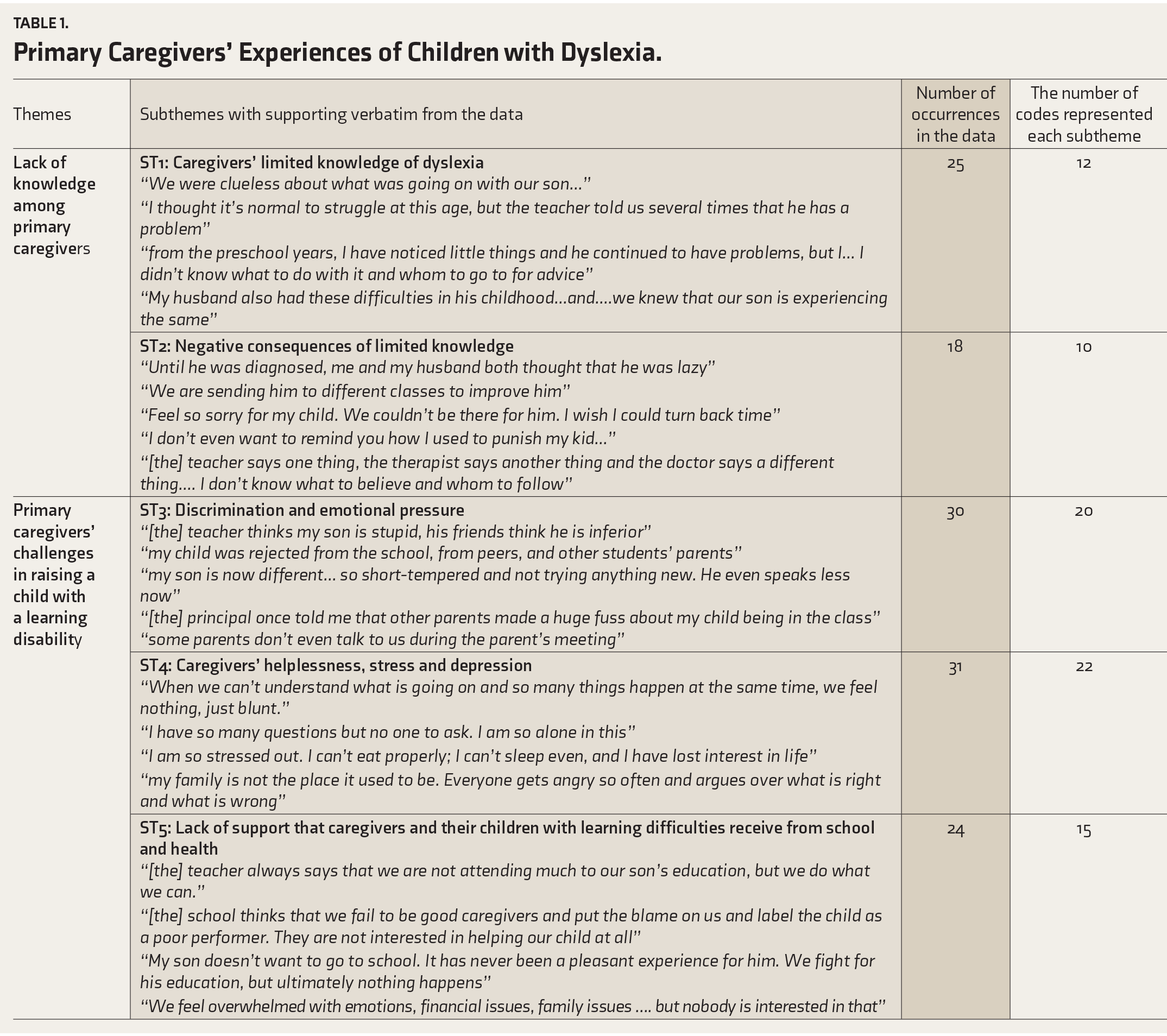
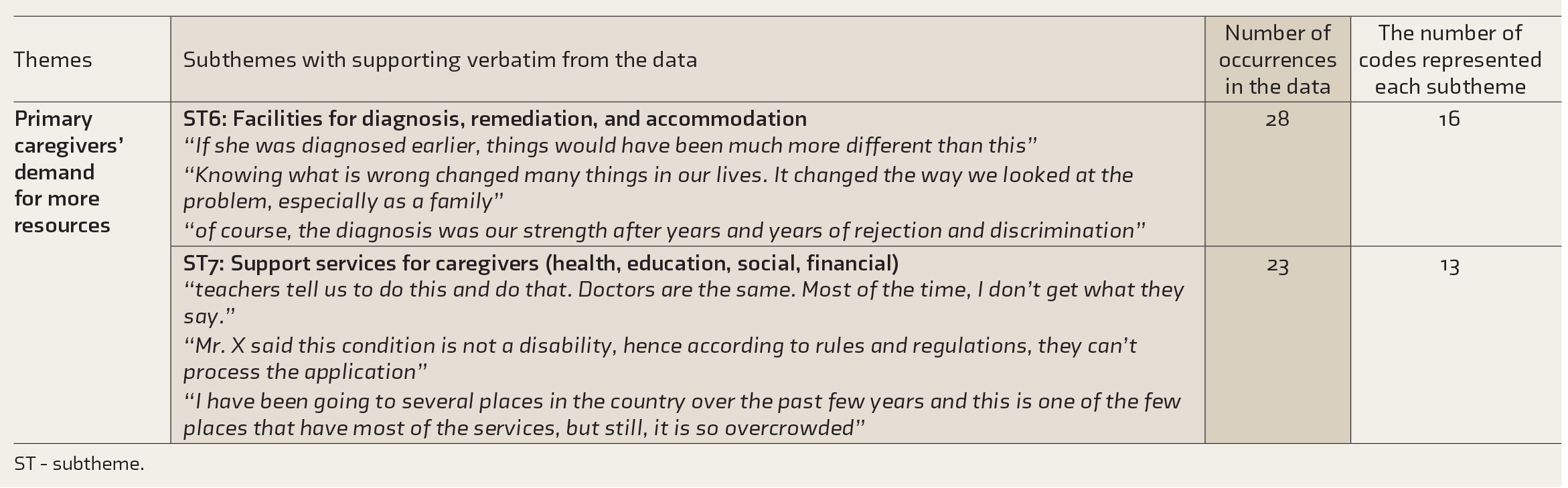
ST - subtheme.
Discussion
One of the important findings of the study was that, in Sri Lanka, caregivers, in general, do not have sufficient knowledge about learning difficulties such as dyslexia and might not even be able to notice difficulties that their children face. On the other hand, parents who have prior experience with dyslexia-type difficulties might be able to notice symptoms. This aligns with the findings of research done in India and Turkey, which showed that, due to lack of knowledge, children and families get affected in several ways, such as delays in identification and minimal appropriate support on time.5,6,7,8
It was well noted that caregivers’ lack of knowledge of dyslexia-type difficulties delayed the early diagnosis. However, a more important finding in this study was the continuing lack of knowledge among caregivers even after a diagnosis was made. The need for more professional support services for caregivers and the knowledge discrepancy between caregivers and professionals can explain this. In the South Asian context, teachers play an important role when it comes to raising caregivers’ awareness of children’s educational practices. However, previous studies revealed that teachers in this region do not have a sufficient understanding of learning difficulties such as dyslexia.15,25,26,30 In this study, caregivers revealed that they did not receive sufficient support and accurate information from schools. This situation seems to have affected the caregivers most because school may be the most accessible, relevant, and only available support that the caregivers have for the time being. This implies the importance of enhancing the awareness and knowledge among caregivers as well as educators.
Another result was caregivers’ un- pleasant behavior towards their children who showed learning difficulties. This study revealed that before the diagnosis, caregivers had punished children for showing learning difficulties despite multiple efforts, and their children did not improve. Some caregivers had expected such children to demonstrate educational gains like those shown by neurotypical children. This is similar to the observations made in several contexts, including Namibia, 13 , and China.14,15 The findings revealed that some caregivers sent their children with dyslexia for additional classes that were not designed to help such children. It is also similar to the results of another previous study, which revealed how caregivers would make children practice reading more when they demonstrate reading difficulties, with the belief that extra activities may help children overcome the issues. 10 It is also evident that caregivers demonstrated self-blame for not being able to support their children adequately.19,20 By improving caregivers’ knowledge, these negative consequences can be mitigated.
Another major finding was caregivers’ unwillingness to depend on scientific practices. According to the study results, some caregivers were unwilling to accept professional advice even after the diagnosis was made, which is similar to the results of a German study. 9 Although other research indicates that parents seek alternative support due to feeling embarrassed that their children have learning difficulties, 11 this study revealed different reasons for caregivers seeking alternative support, which were poor knowledge, limited awareness, inaccessibility to resources, discrimination, power gap, and helplessness. In the Sri Lankan context, there seems to be a knowledge gap between caregivers and professionals, which leads to a disparity, ending up with discrimination against caregivers of children with disabilities.27,28 Rather than in a tug-a-war, service providers and caregivers should be on the same team, and the caregivers should be supported in the best interests of the child. For that, their skills must be updated, and accessibility should be improved. As service availability has become a challenge, making diagnosing facilities and other support services widely available can ensure better service delivery.
Research done in China with 368 families having children with disabilities also illustrates that one-third of the parents investigated emphasized the need for more professional involvement to provide training to parents on their children’s difficulties. 30 Teacher training and policy decisions can be used to minimize the gap and improve the harmony between them. To achieve that, it is important to make professionals more willing and flexible to work with caregivers in collaboration when raising children with learning difficulties. This can be facilitated by providing adequate training and resources.
According to the results, there was psychological pressure on caregivers having children with dyslexia-type difficulties, which supports other research findings from India 20 and Turkey. 21 Family support is vital for caregivers of children with disabilities to share emotions and problems faced while parenting. 32 However, there is evidence that their parenting styles are criticized even by extended family and friends in social gatherings because of the behavioral problems that children with learning difficulties show. 15 Not only family and friends but also teachers may humiliate caregivers for not being responsible in making their children a good “fit” for the competitive school education. 15 The data also revealed that caregivers got frustrated and depressed mainly when they were not supported by the school, teachers, and service providers. As an important implication of the study, at least basic training for all schoolteachers should be provided to ease the pressure on caregivers to some extent.
When the relevant parties are not knowledgeable and aware, it affects society as well. When people in society are unaware of learning difficulties, they may develop negative attitudes towards those who demonstrate such difficulties, and, as a result, these children and their caregivers may experience social pressure and exclusion. 15 The study revealed that negative attitudes that prevailed in society harmed the caregivers and children, as there was a tendency to reject children with learning difficulties along with their families. Social awareness is crucial to overcome these challenges, which will also create more positive attitudes and acceptance from society.30,31,32 Since social media is widely used now, they could be suitable platforms to reach large numbers of people without much delay or financial cost for social awareness programs. Although establishing support services is a responsibility of the government or other responsible authorities, the general lack of awareness in society affects how governments and other regulatory bodies react to social issues. Therefore, it is possible to claim that the main problem lies in the country’s lack of societal understanding of learning difficulties.
Due to all these challenges, the psychological status of caregivers is directly and indirectly affected. Hence, it should be evaluated and supported as a part of the holistic approach to managing learning disabilities in children.
We would also like to acknowledge some of the limitations of this study. The caregivers that we investigated had children who were identified as having dyslexia-type difficulties. Therefore, they had some understanding of such difficulties and some experience working with the available support services. There can be other caregivers who have yet to access these services and perhaps rely on alternative support. In addition, there can be caregivers who have not done anything to support their children because they have not noticed their difficulties. More research is needed to provide a comprehensive picture of caregivers’ knowledge, challenges, and support they need.
Conclusions
To conclude, according to caregivers’ perception, the study highlights that there is a lack of understanding of learning difficulties in Sri Lanka among themselves, as well as a lack of understanding among teachers, other children, health service providers, and society in general. This has created negative attitudes towards those who show learning difficulties and their families, and thus, they are discriminated against in schools and society. The children also face negative outcomes due to parenting styles used by caregivers with a lack of knowledge of learning difficulties and delaying the diagnosis. According to participants, the resources needed to identify, remediate, and accommodate children with learning difficulties are highly limited in both the private and public sectors and are expensive in the private sector. The caregivers demand more social and financial support, but a lack of social awareness may have also contributed to a lack of support services. In this context, primary caregivers and the families of children with learning difficulties face psychological issues disrupting their peace of mind and family harmony, and they seek emotional support. Hence, targeted interventions are needed to improve knowledge, awareness, attitudes, resources, and social services for caregivers, teachers, service providers, and society in general. Mental health services should target their interventions not only to the child but also to caregivers of children with learning disabilities to ensure optimum health of the child, caregivers, and the family as a whole.
Supplemental Material
Supplementary material for this article is available online.
Footnotes
Acknowledgements
We would like to acknowledge the Faculty of Graduate Studies, University of Colombo Sri Lanka for Ethical Clearance, Supervision and guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Ethical approval was obtained from Ethics Review Committee, Faculty of Graduate Studies, University of Colombo, ERC ID: FGS/ERC/2018/028 and Lady Ridgeway Hospital, ID: LRH/DA/o5/2019.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Patient informed consent was taken for data collection up to publication and knowledge dissemination during recruitment to the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.