
Abstract
Background:
The coronavirus disease (COVID-19) pandemic, associated with the economic consequences of non-pharmaceutical interventions such as lockdown, has led to mental health consequences among people worldwide. Protecting the mental well-being of populations is an imperative component of fighting the COVID-19 pandemic. This scoping review attempts to present an overview of the existing tools to measure COVID-19-related mental health problems.
Methods:
Literature search was conducted in the PubMed electronic database using developed key search terms. Reference lists of the identified eligible articles were reviewed to locate relevant articles missed from the electronic database search. Fifteen scales measuring COVID-19-associated mental health problems, validated among diverse populations across the world, were included in this review.
Results:
The majority of these scales were validated among middle-aged adults in Turkey. Only a few validated scales encompass the negative socioeconomic consequences of COVID-19. None of the available scales focused on the aspects of suicidal ideation or behavioral responses/coping strategies, neither were they inclusive of participants from diverse age, geographic, and COVID-19 exposure groups.
Conclusion:
This scoping review highlights the need for future research to develop and validate comprehensive psychometric tools to assess COVID-19-associated mental health problems. Also, in view of the vulnerable nature of healthcare professionals for developing mental health concerns in the course of providing services for COVID-19-affected individuals, future psychometric research needs to concentrate on the development of measures specific for these professionals.
Various validated tools are available to measure the mental health implications of COVID-19. The available psychometric instruments must be used in an informed manner in different settings to comprehend the psychological burden posed by COVID-19 on populations. Identification of COVID-19-associated mental health problems with an informed use of the available psychometric tools facilitates a thorough preparation of healthcare systems in dealing with the psychological aftermath of COVID-19.Key Messages:
Materials and Methods
This scoping review was conducted to examine the available psychometric tools to measure COVID-19-related mental health problems. While the primary purpose of a scoping review is to provide an overview of the available evidence by summarizing the available literature pertaining to a concept, there exists no concrete consensus on the indications for the conduct of a scoping review. 17 Besides comprehending the fundamental characteristics of a phenomenon, identification and analysis of knowledge gaps, which forms the basis for this study, is purported to be one of the key indications of scoping reviews. 18 The framework proposed by Arksey and O’Malley for scoping reviews was adopted in this study. 19
Identification of the research question: Since the scoping review attempts to comprehensively document the existing literature, a broad question that facilitates the inclusion of different constructs relating to mental health are warranted. The research question for this review was identified as: In spite of a preliminary scan of the results showing predominant emphasis on the constructs of anxiety and fear, “What are the existing scales to measure COVID-19-related mental health problems?”.
Formulating the search strategy to identify relevant studies: A literature search was conducted in the PubMed electronic database after a series of consensus building among the investigators for identification of key search terms. The following key terms were included in the search for eligible studies: Coronavirus*, COVID-19, COVID, “COVID 19”, “SARS CoV-2”, “SARS CoV 2” for coronavirus disease; “mental health,” anxiety, fear, phobia, stress for mental health problems; and scale, tool, instrument, questionnaire for scale. The final search string was (Coronavirus* OR COVID-19 OR COVID OR “COVID 19” OR “SARS CoV-2” OR “SARS CoV 2”) AND (“mental health” OR anxiety OR fear OR depression OR stress OR phobia) AND (scale OR instrument OR questionnaire OR tool). Those studies measuring the constructs related to mental health specific to COVID-19, published in the English language in peer-reviewed journals in the year 2020, after the emergence of the COVID-19 pandemic, were included in the review. The search was inclusive of all the relevant publications available till June 10, 2020.
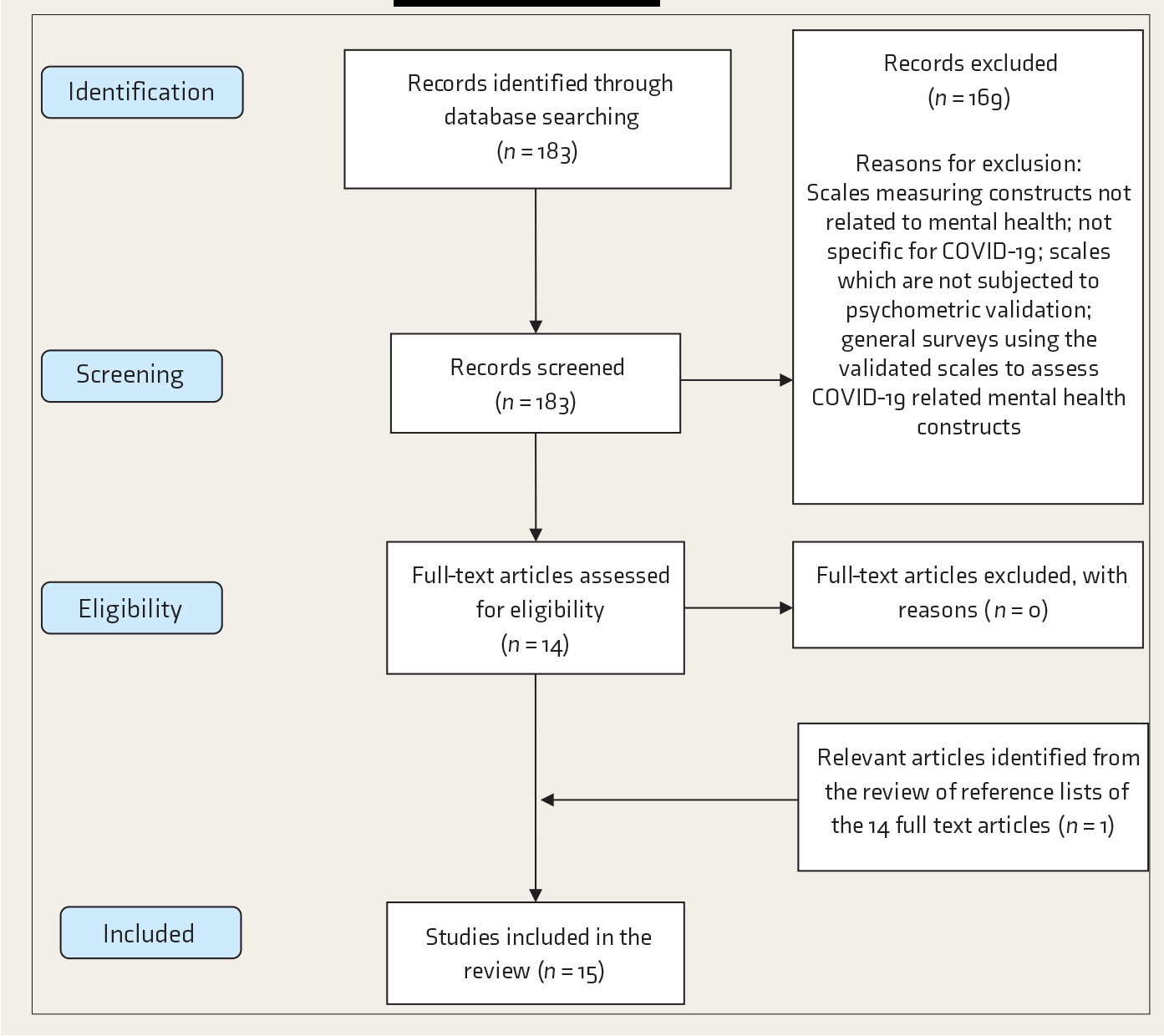
Selection of relevant studies: Figure 1 shows the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for the scoping review. The search strategy yielded 183 results. The EndNote bibliographic software package was used to import and manage all references. The title, abstracts, and key words of all the articles were independently reviewed by three investigators to check the relevance of these articles based on the selection criteria of the review. Scales measuring constructs not related to mental health and those that are not specific for COVID-19, scales which have not been subjected to psychometric validation, and general surveys using the validated scales to assess COVID-19-related mental health constructs were excluded from the review. The full texts of the 14 articles that were agreed upon by all the reviewers to be satisfying the study criteria after the initial review were reviewed. References from all these 14 articles were also reviewed to check if any relevant publications were missed in the electronic database search. The final review included 15 articles.20–34
Study charting and summarizing: All the 15 articles included in the final review were comprehensively charted and summarized. Summarization included details on the authors, journal, country, number of items, dimensionality, time of conduct of the study, and other psychometric properties of the scale. While summarizing the scales, the constructs and dimensions were identified based on the American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition, DSM-5). 35
PRISMA Flowchart of the Scoping Review
Results
An overview of the existing scales measuring COVID-19-related mental health problems have been provided in
Discussion
It is evident from the literature that along with the general stressors, a fear of prolonged outbreak, fear of infection vulnerability, and exposure or close contact with COVID-19-affected individuals negatively influence the mental health and well-being. 36 The psychiatric symptoms encompass depression, anxiety, somatic symptoms, panic attacks, psychosis, and suicidal tendencies.37, 38 CSS and C19 P-S consider the negative economic consequences of COVID-19 as contributing towards the COVID-19-associated mental health problems. Items relating to active search on the internet and social media for COVID-19 information are included in the CSS, along with practical concerns like worrying about cash transactions and future supplies of essentials, which makes CSS a comprehensive instrument among the available scales. However, CSS does not include behavioral responses to COVID-19, which found a place in C19 P-S, where items relating to avoidance of people who sneeze and spending extensive amounts of time on cleaning hands were included. Though it is not the aim of a scoping review to critically appraise/synthesize the findings, it is apparent that CSS, C19 P-S, and CPDI are more comprehensive measures compared to other scales included in this review. However, as the choice of an instrument depends on a lot of other factors such as feasibility and relevance and since all the validated scales demonstrated good psychometric properties, it is difficult to suggest the single best available instrument to measure COVID-19-related mental health problems.
According to American Psychiatric Association, concurrent validity is the extent to which one measurement is backed up by a related measurement obtained at about the same point in time, while criterion validity is reflective of the correlational nature of a measurement with an established standard of comparison. Convergent validity is defined as the extent to which responses on a test or instrument exhibit a strong relationship with responses on conceptually similar tests or instruments. 39 However, these expressions do not have consistent interpretations in the literature and may overlap. 30 For instance, it was reported that the concurrent validity of the Turkish version of FCV-19S was checked with Depression, Anxiety and Stress Scale-21 (DASS-21). DASS-21 is a short form of DASS-42 with three subscales: depression, anxiety, and stress. 41 Since DASS-21 measures constructs of depression, anxiety, and stress, which are different from the construct of interest of FCV-19S, which is fear, and as there is a fine distinction between these constructs as evident from DSM-5, the expression “convergent validity” could have been preferred while referring to the correlation between the Turkish version of FCV-19S and DASS-21. Similar observations relating to overlapping use of the expressions of validity were made by us with regard to measuring concurrent validity of FCV-19S by comparing with DASS-21 and PVDS, 42 which is a 15-item scale with two subscales of perceived infectability and germ aversion; assessment of concurrent validity of the Bangla version of FCV-19S with Bangla PHQ-9 depression measure 43 ; checking criterion validity of FCVS-T with BRS-T, 44 an instrument that assesses the ability to overcome difficult situations; assessment of concurrent validity of the Italian version of FCV-19S with HADS 45 and SMSP-A 46 ; assessing the concurrent validity of the Arabic version of FCV-19S with HADS-A, HADS-D, and HADS-T, which are the anxiety subscale, depression subscale, and combined scales, respectively.
Though it is an established notion that anxiety/fear may lead to suicidal tendencies and inclination towards substance use, there are no available scales that attempted to document these facets.47, 48 Also, none of the available scales included items on adopted coping strategies. It is noteworthy that the validatory sample for only a few scales was inclusive of the COVID-19-affected people. The mean age of the validatory samples across the scales ranged from 26.5 to 49.8 years; this finding is reflective of the necessity to consider population from different age groups in the validation process owing to the established contributory role of age in individuals’ progression towards severe disease. 49 The time of validation of the scales in correspondence to the emotional epidemic curve does play a significant role in influencing the responses of the participants. All the scales were validated during the first peak of the emotional epidemic curve; therefore, validation studies during the dipping phase and second peak phase of this curve are warranted. 50 A striking similarity between the majority of the scales in the present review was the predominant emphasis given to the somatic symptoms experienced by people on thinking about COVID-19. It is to be noted that the items on different scales included in the review concur to a considerable extent; this overlap must be understood in terms of the interchangeable use of the terms “anxiety,” “fear,” and “phobia” in common parlance despite the precise differences in meaning. 39 C19P-S and CPDI are the two distinct scales that differ from the other scales by integrating items representative of the behavioral dimension. Except for the COVID-19 Anxiety Scale, which consisted of items on a semantic differential scale, all the other instruments chose Likert response options, which is an interesting observation in light of the potential acquiescence bias with Likert rating scales. 51 COVID-19-imposed lockdown and quarantine measures may necessitate some individuals to stay away from their families. However, none of the available scales focused on separation anxiety. Failure to document the aspects of substance use and suicidal ideation is the other limitation observed in the existing scales, though these constructs were established to be possible consequences of fear and anxiety.47, 48 Another fundamental lapse identified was the inability of any of the existing scales to discern COVID-19-associated depression. Except for the OCS, 52 CAS, 20 and the Italian version of CPDI, 33 all the remaining scales included in the review inquire about the current status of the subject but do not necessitate the patient to respond by reflecting on their experiences from the past few weeks. Because it has been six months since the identification of the first COVID-19 case, there is a necessity to focus on acute stress disorder and post-traumatic stress disorder associated with COVID-19 among the affected and recovered. A health-systems-related concern that could have an impact on the mental health of people is the unavailability or inaccessibility of healthcare facilities, which was not included in any of the validated scales included in this review. The aforementioned lapses in the scales considered in this review were discussed by us after thoroughly reviewing the catalogue of WHO psychiatric instruments 53 and DSM-5. 34 Moreover, drawing on the insights provided in the WHO Assessment Instrument for Mental Health Systems (WHO-AIMS), the following were identified to be the domains of mental health systems that require attention and close monitoring, learning lessons from COVID-19: the articulation of agencies for public education and awareness campaigns on mental health, development of community mental health services, development of mental health component in primary healthcare, active functioning of mental health mobile clinic teams, the increased proportion of undergraduate training hours devoted to psychiatry and mental-health-related subjects, and refresher training for HCW in mental health facilities. 54 In line with these directives, Das discussed the need for telepsychiatry in active identification of individuals with psychological infirmity and provision of awareness education and psychological interventions in the Indian context. 55 There is substantial literature available on the feasibility and effectiveness of online mental health services during the COVID-19 pandemic across the globe.56–58
Spoorthy et al. 59 reported in their review that HCW across the globe had encountered a substantial degree of anxiety, stress, and insomnia in the course of the COVID-19 pandemic. Shanafelt et al. 60 summarized the possible sources of fear and anxiety among HCW during the COVID-19 pandemic; they also discussed the conventional self-reliant nature of health fraternity as an important contributor to anxiety while dealing with a previously un-encountered disease that is outside the professionals’ area of clinical expertise. Despite the increased vulnerability of HCW in developing mental health concerns in the process of battling a pandemic the health systems are not prepared for, none of the available scales were exclusively developed for HCW. The following are a few of the concerns that render HCW more vulnerable with regard to COVID-19 impact on mental health: limited availability of personal protective equipment, necessity to work for longer durations, fear among HCW about the possibility of transmitting the infection to family members, reports on COVID-19-associated deaths of HCW around the globe, possible discrimination out of fear of infectability from society owing to the involvement of these professionals in the care provision of COVID-19-affected, etc.60–62 Given these concerns, it is also imperative that psychometric tools meant to assess COVID-19-posed mental health concerns among HCW be developed and validated.
FCV-19S was observed to be the most commonly translated and cross-culturally adapted instrument, which is available in seven languages. The probable reason for this instrument to be preferred for cross-cultural adaptation in different countries was the fact that this is the earliest available COVID-19-related psychometric tool, published on March 27, 2020. The next psychometric tool 20 assessing coronavirus anxiety was published only three weeks later. Though CPDI was published on March 6, 2020, the full instrument was not made available in the publication. 33 The 7-item COVID-19 Anxiety Scale was observed to be the only COVID-19 psychometric tool validated in the Indian context. 31 While the adaption of validated measures developed in other countries is possible with a simple translation of the instruments to regional language, it is advisable to verify if the items in these tools meet the intended needs of Indian population, owing to the possible difference in psychological aspects between the populations. 63 Even within the country, rural and urban people can psychologically be different with regard to their COVID-19-related mental health problems; therefore, scale validatory samples must include participants from diverse geographical regions so that differences in item responses across different geographic categories may be determined. Also, checking the psychometric and dimensional stability of translated measures is warranted.
The limitations of this review include confinement to the English language and the PubMed database. Nevertheless, an overview of the existing scales and identification of the knowledge gap in the evaluation of the desired constructs provides a direction for future psychometric research with regard to COVID-19-related mental health problems.
The directives for future studies include the development of more comprehensive measures to document mental health problems posed by COVID-19 pandemic by incorporation of the aspects of suicidal ideation, post-traumatic distress, coping strategies, etc. These studies must also aim for representation from diverse age, geographic, and COVID-19 exposure groups.
Conclusion
This scoping review identifies that majority of the existing scales are heavily biased towards the somatic symptoms of COVID-19-imposed mental health problems. C19 P-S, CPDI, and CSS are among the scales which attempted to capture COVID-19-associated mental health problems comprehensively. FCV-19S, while being a unidimensional scale with only seven items, offers an opportunity for screening in busy healthcare settings and also allows cross-country comparisons, owing to its validation and availability in multiple languages worldwide. The seven-item COVID-19 Anxiety Scale was identified as the only psychometric measure validated in the Indian context and could be adapted in other Indian languages.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Measuring the Impact of COVID-19 on Mental Health: A Scoping Review of the Existing Scales by Viswa Chaitanya Chandu, Yamuna Marella, Gnana Sarita Panga, Srinivas Pachava, Viswanath Vadapalli in Indian Journal of Psychological Medicine
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.