
Abstract
Children constitute 40% of India’s population. Large number of children with psychiatric disorders and neurodevelopmental conditions are unable to access mental health services due to factors such as unavailability of these services in smaller urban and rural centres and lack of training for primary care providers. Given the relatively easy access to video conferencing technology, feasibility and acceptability of Telepsychiatry, there is an urgent need to invest resources and strengthen the use of Telepsychiatry for child and adolescent mental health training and serviced delivery . This viewpoint article discusses the need,scope,experiences and challenges related to use of Telepsychiatry in the area of child mental health.
Delivery of health care services, where distance is a critical factor, by all health care professionals using information and communications technologies for the exchange of valid information for the diagnosis, treatment, and prevention of disease and injuries, research and evaluation, and the continuing education of health care workers, with the aim of advancing the health of individuals and communities. 4
Terms “telepsychiatry” and “telemental health” refer to psychiatric and broader mental health services, respectively. 5 Telepsychiatry for adults was first used at the Nebraska Psychiatry Centre in 1957 and in 1974 for children by the Mount Sinai School of Medicine, United States of America (USA).6, 7 Telepsychiatry could have myriad objectives—direct teleconsultations versus training and capacity building; individual versus group service delivery; use by private practitioners for a small group of clients versus systematic use by primary, secondary, and tertiary health care systems; and emergency versus routine outpatient care—achieved utilizing either a synchronous (real-time) or an asynchronous (store and forward) format. Synchronous, two-way, interactive telecommunication format is commonly used, often in the form of video teleconferencing (VTC).
This article gives a perspective on the use of telepsychiatry in child and adolescent mental health care. We discuss the need, scope, operationalization issues, and challenges in telepsychiatry, as well as give an overview of national and international guidelines and current practice of child and adolescent telepsychiatry.
Need for Pediatric Telepsychiatry
Globally increased burden of child psychiatric disorders, shortage of child psychiatrists, inequitable distribution of existing resources, the “aging-out effect” of the workforce, and insufficient funding have led to increased use of telepsychiatry for children.8, 9 Gloff et al. 10 listed convenience, decreased cost, reduced stigma, and better coordination with multiple stakeholders as significant factors for the preference of telepsychiatry by children and their families. The prevalence of psychiatric disorders in children ranges from 6% to 15%. 11 The number of psychiatrists delivering child and adolescent mental health care in India is 1 per 4–5 million children, with most of them working in cities, making access to mental health care difficult to a large number of children. 12 Given the limited feasibility of reducing the resource gap and the increased access to technology across the country, telepsychiatry appears an ideal resource for the provision of mental health care for children. 13
Scope of Pediatric Telepsychiatry
International literature on telepsychiatry spans preclinical assessment, clinical evaluation, and follow-up care.14, 15 With adequate technological support in place, and consent and cooperation of the psychiatrist and patient, most aspects of psychiatric assessment and care are amenable for inclusion in a telepsychiatric framework, with adequate addressing of potential barriers and challenges.
Of substantial interest to practitioners and policymakers is the use of telecommunication technology in the training of care providers at the primary and secondary care levels, to upscale specialty services like child mental health. Training and mentoring programs exemplified by the Extension for Community Healthcare Outcomes (ECHO) model 16 have demonstrated efficient and practical skill development in the identification and management of complex disorders like autism at the primary care level. Skill enhancement of primary care providers is exemplified by actual practice change in terms of more appropriate prescribing of psychotropic medications by primary care providers. 17 Psychiatric conditions in children are challenging and confusing experiences for families. Inadequate first-level responses, mostly stemming from a lack of training, are common. The use of telepsychiatry to spread awareness in this manner can be a powerful tool in changing this scenario.
Telepsychiatry is widely used in the correctional settings in developed countries with several advantages, such as eliminating the need for travel, coordination with onsite staff, and timely evaluation and treatment.18–21 There are some challenges when working with this vulnerable population. There is a risk of a dual agency to both the juvenile justice facility and the patient. The telepsychiatrist must have adequate knowledge of the juvenile justice system, train correctional facility staff about mental health issues in juveniles, and ensure their privacy. 21
In the Indian context, telepsychiatry can play a vital role in fulfilling the obligations mandated by the Juvenile Justice Act,
22
2015, and the Protection of Children from Sexual Offences (POCSO) Act,
23
2012, through the following activities:
Teleconsultation for children and adolescents in child care institutions (CCIs). Teleconsultation for preliminary assessment as mandated by Section 15 of the JJ Act, 2015. Training staff of CCIs in the basic concepts of child development, child and adolescent mental health, and child protection. Training judiciary, members of the Child Welfare Committee, and Juvenile Justice Boards (JJBs) on child development and child and adolescent mental health issues. Online education of children in CCIs on child safety, child development, child mental health, and life skills. Telepsychotherapy support to children who need psychosocial support in the aftermath of sexual abuse.
Operationalizing Pediatric Telepsychiatry
Operationalizing telepsychiatry for regular practice calls for attention to administrative, technological, and clinical issues. A needs assessment must precede operationalization. 24 Best practices in videoconferencing 25 recommend drafting a program overview, identifying services to be delivered via telepsychiatry, identifying the target patient population and clinicians to be involved in the program, requirements vis-à-vis space, training, technological support, staff, standard operating procedures (SOPs), regulatory and monitoring processes, and sustainability. The choice of the videoconferencing application must be made after appropriate verification of quality, reliability, security parameters, and backup processes. Technological equipment has to be well supported by trained staff with relevant clinical competencies in telepsychiatry. The Indian Telemedicine Guidelines recommend mandatory training for all practitioners intending to provide online consultation within three years of the notification. 26 Besides clinical competencies, adherence to standards of care, liaison with local clinics, and SOPs are vital. 27
Patient selection for telepsychiatry depends on the current abilities of the patient—Can he/she function well, even in unsupervised settings? Can he/she independently operate the videoconferencing tool? Can he/she independently ensure privacy and safety? Is there a history of aggression, self-harm, noncooperation with the service providers? These requirements are secured in the case of children by the caregiver who would assist in supervising and operating the VTC tool. Additional requirements for children and adolescents include developmental status and child-friendly spaces from where the child could join the call. There must be established liaison with the local health care system in case of any emergency. Although the Indian telemedicine guidelines, 26 2020, propose that there is no need for parental consent for the age group above 16 years, it is prudent to obtain permission from the parent for anyone below the age of 18 years, given the existing definition of “minor” in the Mental Health Care Act, 2017. 28
The multifaceted nature of child mental health problems optimally requires collaborative interventions (individual therapy/medication management for the child, family-based/parenting interventions, liaising with the school, and liaising with social services) by a multidisciplinary team. Typically a multidisciplinary team, simultaneously or sequentially, completes the evaluation and intervention processes. In a telepsychiatric setup, mode, and timeline of engagement with the child and family need to be devised in a manner that minimizes the repetition of information and confusion about multiple online appointments and maximizes care and comfort to the child.
Guidelines for Pediatric Telepsychiatry
Several professional organizations have formulated guidelines for pediatric telepsychiatry.
Key Elements of Children and Adolescents in Telepsychiatry Guidelines
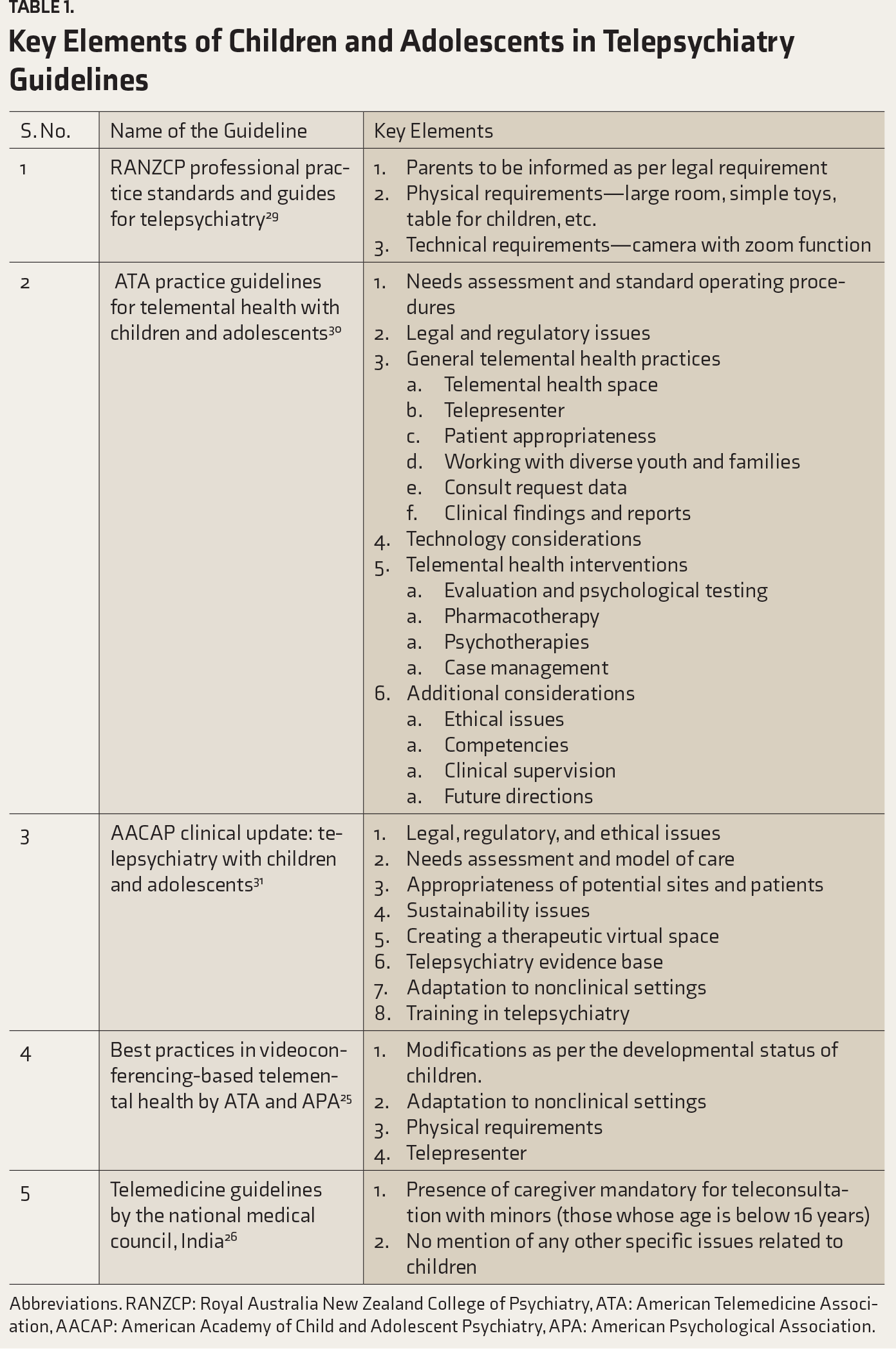
Abbreviations. RANZCP: Royal Australia New Zealand College of Psychiatry, ATA: American Telemedicine Association, AACAP: American Academy of Child and Adolescent Psychiatry, APA: American Psychological Association.
Experiences and Evidence-Base for Pediatric Telepsychiatry
Experiences and Evidence-Base in the International Context
Despite well-established child psychiatry programs, the increasing demands of pediatric mental health needs have not been adequately met by the pediatric psychiatry workforce in the USA. The use of telepsychiatry has been crucial in mitigating access to mental health care, especially when geography and social determinants such as poverty, socioeconomic disparities, and lack of insurance coverage pose additional barriers. Over the last 50 years, the practice of pediatric telepsychiatry has evolved significantly. Besides synchronous and asynchronous delivery formats, in some cases, additional digital tools to collect structured data using mHealth (mobile health) have also been integrated into the overall virtual delivery of care. In order to provide a clinical and evidence-based framework, the American Academy of Child and Adolescent Psychiatry (AACAP) has created guidelines (refer to Table 1) and more recently video toolkits for the clinicians interested or actively engaged at different levels of Telepsychiatry. 32 The feasibility of pediatric telepsychiatry is well established across a variety of psychiatric disorders in the form of diagnostic reliability. 24 Besides, the clinical outcomes of treatment interventions provided using telepsychiatry in children are comparable to traditional, in-person care. 33 Teenagers spend much time in the online and digital world for their social connections, entertainment, self-expression, and in many places for education. Using the same framework for accessing health care has been advantageous for this population to engage reliably in their mental health services.
Although the evidence of clinical effectiveness is recognized, factors such as legal regulations, licensure, reimbursements, and insurance coverage influence the actual implementation and utilization of telepsychiatry in the USA. All 50 states in the USA have established regulatory telehealth guidelines and supporting infrastructure at varying levels. Just like the licensure requirements for the practice of medicine, a telepsychiatrist in the USA is required to have an active medical license in the state where they are located. Most of the states additionally make it a requirement to have an active license in the state where the patient is located, thus requiring multiple state-specific licenses in many cases. Permitting telepractice across states, even with a unitary license from the state of residence, is being actively explored recently. However, the variability in the regulations and malpractice coverage across the states act as barriers. At this time, there is no requirement for formal training in telepsychiatry for a psychiatrist to deliver care using this modality. Necessitating formal training before permitting online practice can be viewed as creating an additional barrier. Nevertheless, it is felt that proper training will help to address the novel components in telepsychiatry, like doing a physical or mental status examination via digital interaction. Financial considerations have also been important in the practice of telepsychiatry. Most health care expenditure is through commercial and government-funded health insurance programs that are administered through managed care entities. Similar to the regulations, the coverage of telehealth as part of the insurance benefit is a significant factor for providing and accessing telepsychiatry care.
Despite technological advances, there is a significant digital divide between urban and rural areas across many regions in the USA. The broadband internet connection and high-speed phone data services are still not available in many areas resulting in the population being unable to access telehealth. Even if there is connectivity, the affordability to pay for the services and devices will limit the ability of many underserved and less privileged families. There are several programs through community and government partnerships for digital connectivity to bridge this gap. 34
In order to address the fundamental issue of workforce shortage and overall sustainability of mental health delivery, telepsychiatry is now being utilized for different models of workforce development such as collaborative and integrated care, peer-to-peer consultation, school-based telepsychiatry, and learning collaboratives using “hub and spoke” models.
Before Coronavirus disease-2019 (COVID-19) there was significant variability in the state-specific rules about the type of services provided (outpatient care), technology requirements (legacy systems), site or location of service (clinical setup), and the type of providers (only psychiatrists and psychologists) who could engage in the use of telepsychiatry for treating children. Depending on the state, it was also mandated to have an in-person visit before initiating medication management. There were also federal restrictions on prescribing controlled substances such as stimulants used for attention deficit hyperactivity disorder and benzodiazepines based only on telepsychiatry visits. The rules of confidentiality and patient privacy, as described in the Health Insurance Portability and Accountability Act (HIPAA) for health care, also applied to any care delivered using telehealth, thus limiting the use of commonly available technology. These different rules were often considered restrictive for the rapid adoption and scalability of telepsychiatry. The regulatory flexibility by temporarily waiving of these rules during the declared COVID-19-related emergency demonstrated that telepsychiatry is not only scalable quickly but also one of the most important modality for continuity of care for the most vulnerable patients during the pandemic. Whether the regulatory changes will continue is yet to be determined, but the continued expansion of telepsychiatry is certain. 35
Experiences and Evidence-Base in the Indian Context
Pediatric telepsychiatry has been more recent, with evidence-base being very limited in the Indian context. Following are the experiences in the Indian context:
Malhotra et al.
36
developed the Clinical Decision Support System for the diagnostic evaluation of children. This team proposed the term “tele-enabling model” for their novel model of service delivery.
37
Balasinorwala et al.
38
reported the feasibility of telepsychiatry service in the asynchronous mode. A total of 16 patients (17 % ) of those who availed the service were children. The Virtual Knowledge Network (VKN) at the National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, has been using a similar approach for training primary care providers.
39
The first certificate course in child and adolescent psychiatry focusing on neurodevelopmental disorders (NDDs) was launched in June 2019 and is now nearing completion. As part of this course, child mental health professionals at NIMHANS carried out an introductory training in various aspects of NDDs, for about 38 primary care physicians in the state of Chhattisgarh. Case presentations by the trainees replaced didactics to facilitate self-learning and real-time application of the knowledge gained. Such programs do not aim to develop expertise; instead, the goal is to develop skills for early identification of child psychiatric disorders, initiate a first-level response, and organize appropriate multidisciplinary referrals. Screening done by primary care physicians helps to provide timely intervention to the needy. Several children and adolescents require psychotropic medication alongside psychosocial interventions for adequate management of their behavioral/emotional concerns. As per the Indian telemedicine guidelines, 2020, except methylphenidate which comes under schedule X class of drugs, other psychotropic medications can be prescribed to children through a teleconsultation by a qualified psychiatrist.
26
At least in the initial few weeks of starting medication, children/adolescents need to be monitored, vis-à-vis specific side effects that may become particularly worrisome in some cases in this population such as behavioral activation with selective serotonin reuptake inhibitors, hepatic complications with atomoxetine, and blood pressure changes with clonidine, besides adequate parental supervision for the administration of medication. A liaison with an accessible medical setup must be ensured for timely monitoring.
Challenges in Pediatric Telepsychiatry
A detailed history and mental status examination are perhaps the best tools available for psychiatric diagnostics. 40 During the examination, a psychiatrist not only listens to the verbal responses from a patient but also observes general appearance and behavior, facial expressions, nonverbal gestures, and psychomotor activity. Mediation by a telecommunication channel (videoconferencing) restricts the psychiatrist’s observational field to verbal responses and, to some extent, facial expression. Clinical challenges in telepsychiatry perhaps emerge from this fundamental structural limitation, besides technological barriers that may exist for both the patients and the service providers. The provision of psychiatric care via telecommunication technology typically arises in atypical circumstances, such as the current COVID-19 pandemic that has unprecedentedly reduced outpatient attendance across medical services in the country. This often results in inadequate preparation for a reasonable delivery setup, vis-à-vis the large population to be catered. We discuss here technological and clinical barriers in the practice of telepsychiatry, with a specific focus on issues of children.
Technological Barriers
Unlike an informal video call, videoconferencing for clinical purposes requires attention to the knowhow of various app functions (e.g., operating audio-video settings, and lighting, room arrangement).41, 25, 35 Issues with gaze angle, distortion in the on-screen display, and transmission delay can impede free communication flow between the psychiatrist and the patient. 41 The psychiatrist also needs to adjust to appropriate “webside manners,” by voice and expression modulation. 35 Inadequate technical support and a lack/limited availability of telepsychiatry competencies are frequently perceived barriers by clinicians.41, 42, 43 The Indian telemedicine guidelines allow practice using modalities like telephone, video-calling, and even via texting. 26 Children and adolescents may show more interest in these varied modalities.44, 45 However, like that in in-person consultations, constant adult support and supervision will be required right from scheduling an appointment, to the call setup, to ensuring regularly scheduled contact with the service provider.
Clinical Challenges
During telepsychiatric consultations, clinicians tend to perceive a lower quality of rapport, satisfaction, alliance, and comfort than patients. 46 Perhaps for patients and families, the benefits of telepsychiatry—lower travel expense, getting help from the comfort of their homes, reduced waiting time since online appointments can be scheduled with better time regulations, not having to miss school in order to travel for the consultation outweigh any possible reduction in clinical care quality. Children with conditions like autism spectrum disorder, posttraumatic stress disorder, or social anxiety disorder, may show better comfort during teleconsultation than when in in-person consultation. 47 Besides psychiatry has long moved from “praecox” diagnoses to using structured assessment instruments that can very well be administered over telecommunication. However, clinicians sense the lack of gestalt from an in-person consultation, especially in therapeutic settings. Patients need to be periodically assessed for the suitability for continuing telepsychiatric care. 48 The evidence base to inform telepsychiatric practice is still evolving, and clinicians must rely mostly on their best judgment to dictate the appropriateness and sufficiency in a particular case. 26 A significant impetus for a governmental interest in nurturing telemedicine is to expand health care accessibility in remote and rural areas. In psychiatric practice, perhaps more than in other medical fields, because of the heavy reliance on verbal information, clinical challenges amplify when psychiatrists are called upon to see children and adolescents, elderly patients, and patients in geographically and culturally distant areas that may have varied colloquial expressions and idioms of distress. 49 Issues of privacy, safety, confidentiality, and boundaries, for both the clinician and the patient, require specific attention in telepsychiatry. These are pertinent issues for adolescents, especially, who may be wary of their family members’ involvement with or access to a telecommunication exchange with the psychiatrist. These issues also gain prominence in the disclosure of abuse and therapeutic work thereof. Telepsychiatry is not just about using any internet-enabled device. It is crucial to ensure that the device is being used from a secure physical and web location, unlikely to be disturbed or accessed by others. Definite plans for session structure, consent/assent procedures that cover disclosure of abuse, SOPs for reporting and continuity of care (especially choosing between continued telepsychiatry or a shift to in-person care), could be essential aids for the child and adolescent psychiatrist when it comes to dealing with sensitive issues like child sexual abuse. In such scenarios, it would also be important to adhere to a multidisciplinary approach in order to have ready access to collaboration with clinical psychological, social work, legal, and other services.
The ease and pace offered by technology come with the flipside issues of social isolation and technology burnout, especially for clinicians who may have to spend substantial working hours over the internet depending upon their telepsychiatric engagements. This may add to reluctance in the psychiatrist to engage in this new modality of care. Clinical scenarios, such as aggression, self-harm, intense affective, or psychotic states, are not amenable for telepsychiatric care. Health-facility based care for these has to be stated a priori to every patient seeking telepsychiatric care. Assessments in child and adolescent psychiatry are typically multisession, multi-informant, and multiformat. 50 The diagnosis of behavioral and emotional issues in children and adolescents typically crystallize out of a series of meetings with the young person and significant others where a psychiatrist spends time trying to understand and decode the multiple influences in a child’s life and the likely clinical consequences. Can a telecommunication platform duplicate this process? Depending upon the age of a child, a psychiatrist uses multiple techniques—play-based, projective, joint activities—to develop rapport and facilitate an expression of emotional distress. With the limitations in the field of view and modalities of engagement, creative solutions need to be devised to replicate these processes via telecommunication.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.