
Abstract
Background:
Despite significant prevalence of specific learning disorder (SLD) in India, insufficient efforts have been taken to deal with its burden. Currently, the workforce is limited and resources are expensive and difficult for families to access. Consequently, developing an alternative remedial program in the form of a home-based intervention (HBI) is imperative. This article describes the development phase of a manualized HBI program for 7 to 12-year-old children with SLD.
Methods:
Extensive literature search, 7 focus group discussions with parents of children with and without SLD and teachers/counselors (n = 44), and 22 in-depth interviews with SLD children (n = 9) and professionals (n = 13) were conducted. A thematic analysis was done. Intervention strategies were identified based on themes. Experts’ feedback about the content and structure of HBI was also taken.
Results:
The design and application of the HBI program integrate several intervention areas, including psychoeducation, learning strategies, cognitive, social, and behavioral techniques, and therapy for parents. HBI comprised 14 parent training sessions, the duration being 45 to 60 min per session, over six months. Parent training consisted of four steps. (a) The researcher/clinician describes the steps of reading, writing, or math strategies to the parents/caregivers; (b) the researcher/clinician implements the strategies with or without the presence of the child and observation by the parent; (c) the parent practices the strategies in front of the researcher/clinician; and (d) the researcher/clinician observes parents’ practice and corrects them if required.
Conclusion:
HBI manual for children with SLD-mixed type has been developed, keeping with all stakeholders’ perspectives. Further study is on the way to assess its acceptability, feasibility, and effectiveness.
Keywords
The first study to develop an HBI after exploring the needs of children with SLD and their parents through qualitative methods. HBI comprised 14 parent training sessions for 45 to 60 min per session over six months. HBI adopted a combined approach of remediation, cognitive retraining, behavioral management, and stress management.Key Messages:
Specific learning disorder (SLD) is common in the student population irrespective of their mother tongue and medium of instruction. Worldwide prevalence of SLD has been estimated to be 5% to 15%, 1 whereas in the Indian context, it affects 0.38% to 15.2% of the children. 2 Academic problems are the most frequently reported difficulties of children with SLD, whereas the other major difficulties encompass a broad range of cognitive deficits and social-emotional problems. 3 Because of their poor learning skills, many children with SLD experience low self-esteem, low confidence, low expectations from themselves, and poor peer relationships. 4 SLD may also negatively influence their parents’ lives. It predisposes the parents to higher stress levels, frustration, and dissatisfaction. 5 Therefore, researchers have advocated for management of SLD that also includes the familial needs 6 such as the need for home-based intervention (HBI), the parents can implement at home. 7
HBI has been found as an effective intervention approach to deal with a child’s learning problems.8, 9 It has several advantages: it promotes one-to-one attention and immediate modification offered by parents/caregivers,8–10 prevents missed classroom opportunities and/or stigmatization,11, 12 and helps overcome travel-time issues for a remedial session at clinics or hospitals.7, 13 It also supports parents in participating effectively in an academic intervention that positively affects the child’s literacy. 14 Additionally, the parents save their time, energy, and money, which may further motivate their full involvement in the intervention.
Recently in India, SLD has come to increased clinical attention because of an upsurge in consultations in the hospital settings. SLD has been recognized as a disability under the rights of persons with disabilities act (RPWD Act, 2016). However, intervention and remedial programs for these children are scanty and often beyond the affordability of parents. There are also limited provisions, resources, and workforce to deal with this problem. Because of this, national educational boards and state governments of India have formally granted certain concessions to these children, which include exemption from a third language, extra time in the exam, a scribe to write the exams, and reservation quota in certain fields of study. These concessions certainly reduce some of the problems these children face regarding their academic success. 15 But still there is a need for a more comprehensive and extensive program for their future success. Therefore, it becomes essential for the parents to equip themselves with the skills to empower their children.
Although the effectiveness of HBI has been researched in the Western literature, no Indian study has extensively looked for HBI development and its suitability in the Indian context. Only two case studies could be identified and they had found an overall improvement in a child’s academic performance and social and communication skills.16, 17 Hence, the development of HBI would be an essential step in meeting the parents’ and children’s needs and would also be an asset to teachers and mental health professionals (MHPs). Therefore, research was planned to develop an HBI for children with SLD and assess its utility in terms of accessibility, feasibility, and improvement in learning difficulties. This paper describes the development phase of a manualized HBI program for 7 to 12-year-old children with SLD.
Material and Methods
Study Design and Setting
A descriptive qualitative study approach was adopted (a) to understand the clinical, academic, and nonacademic construct of SLD and its impact on the child’s life from varied perspectives and significant challenges faced by parents and (b) to elucidate a potential intervention with target areas and mechanisms for the intervention plan. Postinstitutional Ethics Committee approval, the study was also registered with the Clinical Trials Registry of India (CTRI/2020/05/025057). Participants were selected through purposive sampling between July 2014 and April 2015. Written informed consent and assent were obtained from all before participation. Samples were taken from five centers in Delhi, India:
The Department of Psychiatry of a tertiary care center A hospital for mental diseases A school Two nongovernmental organizations (NGOs)
The index study followed consolidated criteria for reporting qualitative research (COREQ) guideline. 18
Participants
The study had the following five groups.
Group 1: Nine children with SLD-mixed type (as per ICD 10 criteria) aged 8 to 12 years. They did not have any comorbidity (assessed on MINI-KID). Psychiatry consultant confirmed the diagnosis of SLD, and clinical psychologists conducted SLD diagnostic assessments.
Group 2: Parents/caregivers of children with SLD mixed type aged between 8-12 years. The parents had to be aged 27 to 45 years, educated at least till 10th standard, staying with the learning-disabled child for a minimum of two years, and willing to give written informed consent. Families were excluded if another family member/sibling of the child also had a psychiatric, neurological, or chronic medical illness. Additionally, parents of those children with SLD who had comorbid psychiatric conditions except for attention deficit hyperactivity disorder (ADHD; assessed on MINI-KID) 19 or had a known history of organic conditions/medical disorders, or had impairment in hearing, vision, or speech because of which learning difficulties could occur were also excluded.
Group 3: Parents of normal healthy controls (NHCs) aged 8 to 12 years, intelligence quotient ≥85 (assessed on Malin’s Intelligence Scale for Indian Children) 20 and average or above academic performance according to parents and school reports.
Group 4: Primary school teachers and counselors with at least three years of experience working in primary classes.
Group 5: MHPs, including psychiatrists, clinical psychologists, and special educators specialized in managing SLD and having at least three years of working experience.
Measures
Sociodemographic Data Sheet
A semistructured interview schedule for all group participants was prepared for the study. It included sociodemographic details of participants, experience in teaching/counseling in the field of SLD/ mental health, etc.
Focus Group Discussion (FGD) and Interview Guide
FGD/interview guide was prepared to gather information on specific topics of concern and management of SLD. It had open-ended questions to discuss SLD children’s difficulties, parents’ experiences, and possible strategies to accommodate learning problems. We developed FGD/interviews moderator guides for each group of parents, teachers, counselors, special educators, and MHPs.
Procedure
The study was carried out in three steps.
Step-I: Literature Review for SLD Resources and Modules
This step involved an extensive review of existing literature to identify effective interventions in both Western and Indian scenarios. Published and unpublished material, peer reviewed and nonpeer reviewed materials, and case reports were part of this review. The search was conducted with various electronic databases: PubMed, PsycINFO, Educational Resources Information Center (ERIC), and Google Scholar. The search keywords were “learning disability,” “specific learning disorder,” “reading disability,” “dyslexia,” “reading fluency,” “writing disorder,” “dysgraphia,” “spelling disorder,” “mathematics,” “dyscalculia” and “intervention,” “treatment,” “remediation,” “parent-tutoring,” “parental involvement,” “parent training,” “parent participation,” “home-based instructions,” “parent–child paired reading,” and “parent-implemented intervention.” These keywords were used in various combinations. In addition, a further search was conducted by cross-referencing the articles and the books. The selection criteria for inclusion of different studies into the literature review were as follows: the study included an intervention for a learning disorder or academic skills, participants met diagnostic criteria for a learning disorder or reading disorder (dyslexia) or writing disorder (dysgraphia) and/or mathematics (dyscalculia), or mixed disorder, children were tutored either by the researchers or by their parents, the age of children was less than 13 years, and studies mentioned the number of students, intervention program, and the setting, length and duration of sessions.
A total of 117 abstracts were screened. Sixty-seven studies were reviewed after excluding duplicates (n = 81) and including cross-referencing reports (n = 31). Reviewed studies included reports/dissertation/book chapters (n = 13) and intervention studies for reading disorder (n = 27), spelling disorder (n = 3), mathematic disorder (n = 3), and at-risk learning disorder (n = 10), along with parent tutoring to normal children (n = 11).
Step-II: Need Assessments of Children with SLD and Their Parents and Identifying Intervention Strategies by Conducting FGD/Key Interviews
FGD and interviews were conducted primarily by the first two authors (PhD, female clinical psychologists, and having training in qualitative research) to identify problematic areas of children with SLD with respect to the Indian scenario, to understand the needs of the children with SLD and their parents, and to explore the learning strategies from the parents of normal healthy controls, teachers/counselors, MHPs, and special educators. A working relationship was established with all participants before study commencement, and they were asked for their willingness to participate in the study. Participants were explained about the nature and purpose of the research and assured of complete confidentiality. After obtaining the participants’ informed written consents and assents, face-to-face FGD and interviews were conducted. FGD was conducted with groups two, three, and four, composed of five to eight participants, and was continued till the theoretical saturation of themes. Key interviews were carried out with groups one and five as the group formation for FGD was challenging because of practical reasons. The authors also reviewed the clinical record files and findings of psychoeducational assessments of participating children to understand their problems to the depth, as the children with SLD had poor communication skills and limited cognitive abilities. They would take more time or need more opportunities to understand and recognize their emotions and thoughts. A moderator and a comoderator led the discussions using FGD and the interview guide format developed during the study. The FGDs and interviews began with open-ended questions and lasted 45 to 120 min. The detailed discussion explored the various aspects of SLD, its impact on children and parents, and the methods used in dealing with the child’s learning problems. The language of FGD was predominantly Hindi with parents of children with SLD and normal healthy controls, whereas both Hindi and English have opted for children with SLD, teachers, counselors, and MHPs. Each session was audio-recorded with the participants’ permission, and the second author maintained manual notes of all the discussions.
Thematic analysis was used to analyze this data qualitatively. Recordings obtained from FGDs and interviews were transcribed, and all personally identifiable information was removed. The manuscripts were analyzed through careful reading and rereading of the transcripts to identify the themes, 21 and then the themes were organized and coded using inductive analysis by AS and RB. The codes were then reanalyzed according to the categories for the frequency of repeated patterns across all the manuscripts. The themes and quotes were then translated from Hindi/bilingual to English by following the standard translation–back-translation method to ensure the actual meaning. Further, the investigator triangulation method was adopted to ensure the trustworthiness of data, enhance the objectivity of the coding, and reduce biased decisions in category development. Three other independent experts reviewed codes and categories. To reduce biased decisions and differences in the coding scheme (differences considered if disagreements >50%) and to generate alternate opinions, frequent debriefing sessions were held amongst researchers to reach a consensus.
Step III: Content and Face Validation of the HBI Module
Based upon the literature review and findings of the FGDs/interviews, the structure and content of HBI were finalized. Other relevant themes related to the children’s and parents’ perspectives were also identified. Apart from focusing on academic areas, HBI incorporated some other domains also like memory and attention training, social skills training, and behavior management. Additionally, for the management of parental stress, relaxation and problem-solving techniques were introduced in HBI. The first draft of the HBI module was then examined by the experts. The experts reviewed the module and reflected content-specific and overall module’s structure-related feedbacks. Content validity ratio (CVR) was then calculated by CVR = (Ne-N/2)/(N/2), in which Ne is the number of experts marking an item as essential, and N is the total number of participants. 22 The acceptable CVR values were determined as 0.78 to 1.
Results
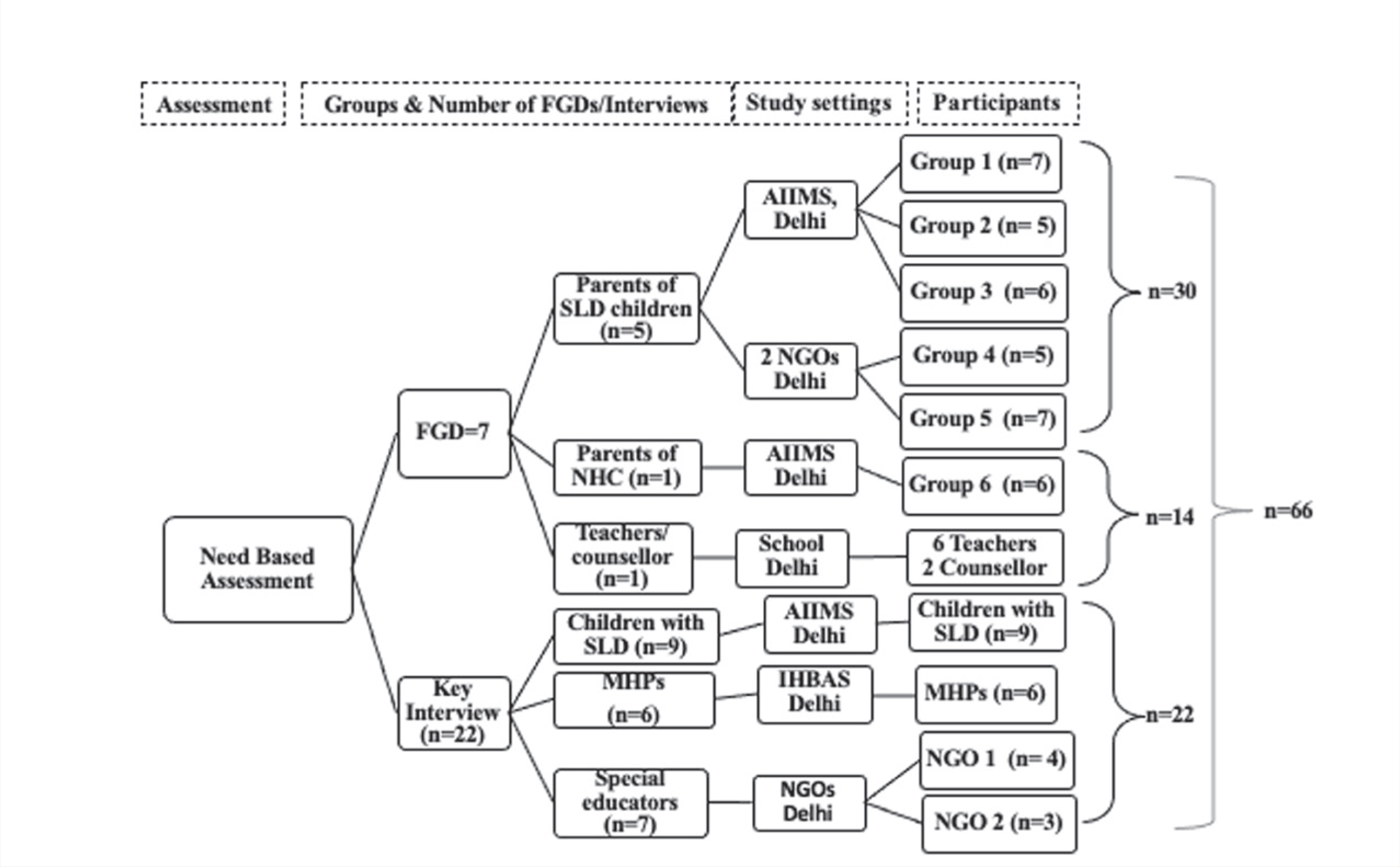
A total of 66 participants were recruited across 7 FGDs (n = 44) and 22 in- depth interviews (n = 22; Figure 1). The sociodemographic characteristics of participants from all groups are presented in Table 1. A majority of the participants were mothers (60%, n = 18) and housewife (66.7%, n = 20). All participants belonged to middle socioeconomic status and were from urban locality (100%). All children had average intelligence and SLD-mixed type while few children had the signs of ADHD (13.2%). All teachers/counselors and MHPs had five years and more than five years of working experience in the area of SLD, respectively.
Reading, handwriting, spelling, writ- ten expression, mathematics, attention, memory, and social skill problems were the main themes that emerged on the basis of interviewing children with SLD, clinical files, and psychoeducational assessment reports.
Major themes and subthemes were identified after analyzing all five discussions with parents of children with SLD. Themes were kept into two broad categories: problems related to children with SLD and difficulties encountered by parents (Table 2). Two main themes and subthemes were found pertaining to problems faced by children with SLD, including academic and nonacademic problems. All parents talked about the child’s learning problems in academic areas, that is, reading, writing, and mathematics. Parents’ main concern was related to the child’s poor academic performance and some cognitive deficits (e.g., poor attention, concentration, and memory). Twenty-seven parents noticed that children got distracted very easily during study time and frequently forgot answers and spellings they learned a few minutes back. They also realized that their children were experiencing social and emotional problems (e.g., being submissive, sensitivity to criticism, poor self-esteem, and low frustration tolerance). Most parents reported that their children made excuses during study time (e.g., asking for water, frequently going to the washroom), felt lethargic, and sometimes showed temper tantrums. Further, some of the most significant challenges the parents faced were lack of awareness about SLD, attitude toward the child’s diagnosis, and parental burden.
Sociodemographic Profile of Participants Recruited for FGD/Interview (n = 66)

FGD, focus group discussion; SLD, specific learning disorder; NHC, normal healthy control; MHPs, mental health professionals; MSES, middle socioeconomic status; min-max, minimum-maximum.
Identified themes/suggestions from FGD with parents of NHCs and teachers and counselors, along with key interviews with professionals were taken. Almost all participants advocated similar strategies, approaches, and procedures for example, psychoeducation, multisensory approach, rewards, and reinforcement, explain concepts with examples, use of learning aids and over-learning and summarizing strategy. They suggested that strategies should be based on strengths and weaknesses of children with SLD in the management plan.
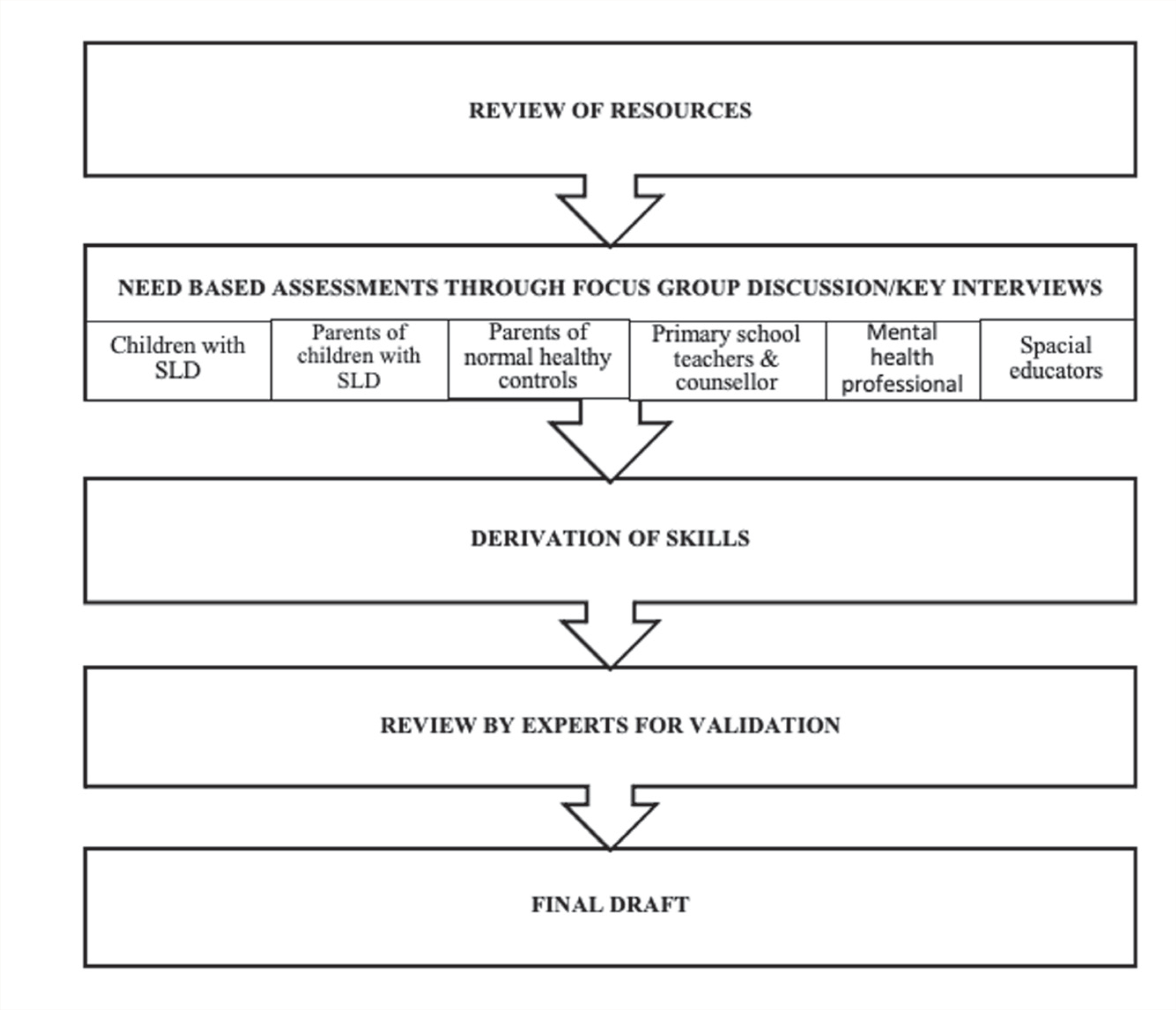
The HBI module was examined by the experts, including psychiatrists (n = 2), clinical psychologists (n = 5), and special educators (n = 2). There was a satisfactory level of agreement between the experts, suggesting good content validity (CVR = 0.91). All experts agreed with the content and structure of the module. Experts’ suggestions were incorporated. For example, using group psychoeducation sessions with parents of children with SLD instead of individual parent psychoeducation to normalize the parents’ attitudes toward the child’s diagnosis. Recording sheets for parents were modified to make it simpler and easy to practice. They were aimed toward regular monitoring of the child’s progress. Hence, the draft was modified as per experts’ feedback to take the final shape of the HBI module (Figure 2).
Steps involved in the development of Home-based intervention module
Summary of HBI Module
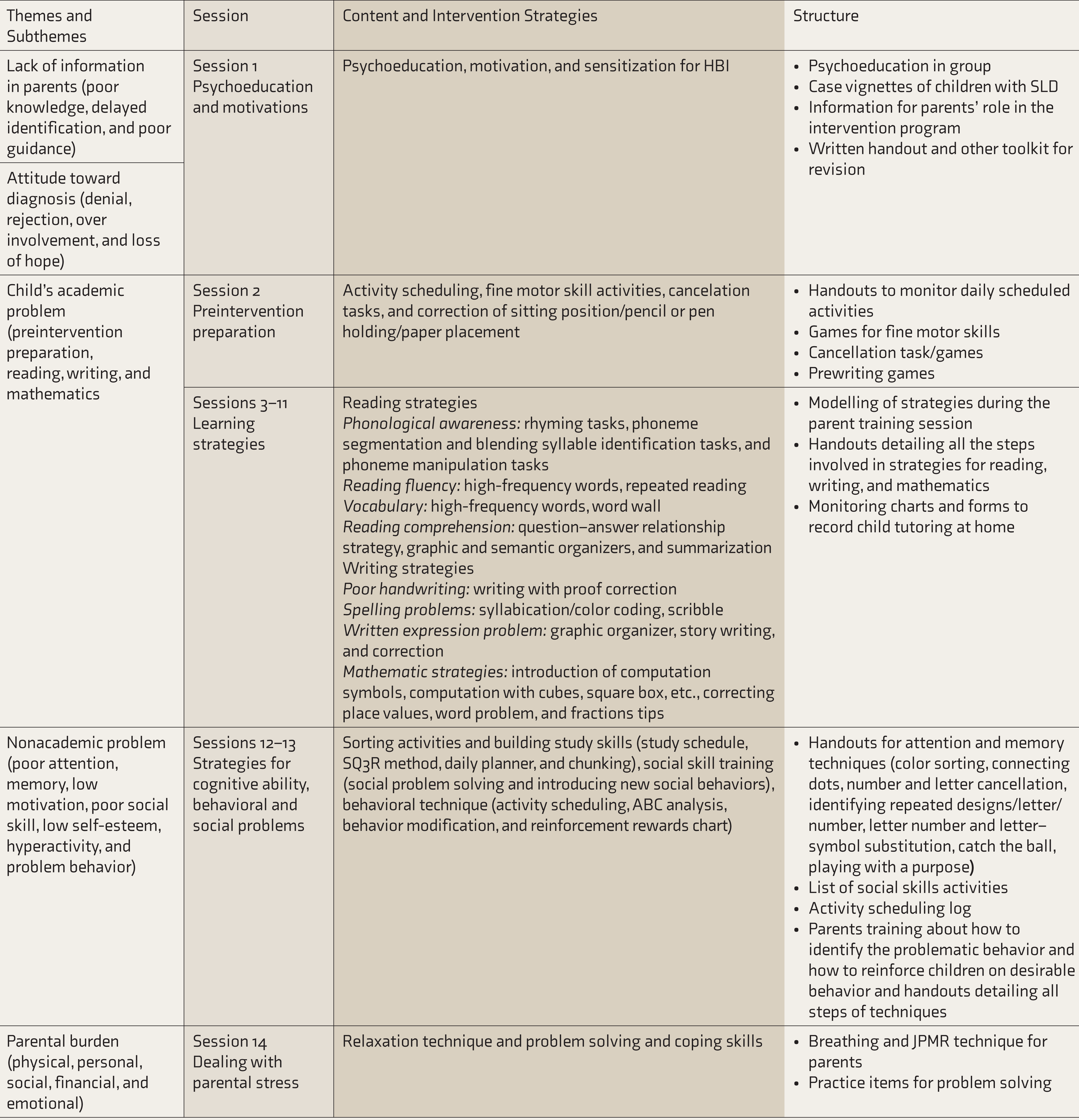
HBI adopted a combined approach of remediation, cognitive retraining, behavioral management, and stress management. It consists of four sections: (a) psychoeducation; (b) learning strategies; (c) cognitive, social, and behavioral techniques; and (d) therapy for parents. The first and last sections deal with the issues of parents’ understanding of SLD and parents’ stress management. In contrast, Sections 2 and 3 focus on the child’s learning, cognitive, social, and behavioral problems (Table 2). HBI comprises 14 parent training sessions to be conducted over six months. The first session is on parent psychoeducation, intervention plan, and role of parents in the intervention. It is followed by ten sessions to enhance, maintain, and promote the child’s overall literacy skills, including reading, writing, and mathematics. The next two sessions are devoted to the child’s difficulties in cognitive function and social skills and behavioral problems. The last session focuses on relaxation and problem- solving skills training for parents to combat their stress, frustration, and dissatisfaction. The parents’ training sessions include four sessions once a week for the first month and ten sessions once in two weeks (15 days) for the next five months. All parent training sessions are planned for 45 to 60 min. Parents’ training can be done at the clinic or school in the child’s presence or absence, along with a minimum of one home visit. Parent training instruction involves four steps: (a) The researcher/clinician describes the steps of reading, writing, or math strategies to the parents/caregivers; (b) the researcher/clinician implements or models the strategies in front of parents; (c) the parent practices the strategies in front of the researcher/clinician; and (d) the researcher/clinician observes parents’ practice and corrects them if required.
Overview of Home-Based Intervention Module
Discussion
To the best of the authors’ knowledge, this is one of the first studies from the Asian subcontinent aimed to develop an HBI based on the needs of children with SLD and their parents. FGDs and interviews were chosen for need-based assessment because of a long history of using FGD as a research method to elicit experience with illness and grasp the contextual basis for making culturally sensitive interpretations.23–25 The need-based process helped develop the module’s content which is need-based, valid, and culturally appropriate. Literature has also documented that while planning the treatment for SLD, clinicians or researchers should first assess the needs and preferences of the children and their caregivers. 26
It was also noticed that most parents are not fully aware of their children’s learning and behavioral problems at home and school. This finding is in consonance with the previous studies, reporting insufficient knowledge about the core basic issues of SLD among parents.27, 28 Hence, HBI entailed psychoeducation, motivation, and intervention plan. It is believed that once the parents are empowered with the core knowledge about SLD, right from their child’s diagnosis, they would realistically accept the diagnosis and readily participate in remedial education or intervention. 29
HBI encompasses strategies for reading and writing (Hindi and English) and strategies for mathematics. Previous qualitative research from India also revealed that children with SLD took more time to complete assigned writing tasks, made more mistakes in spelling, and had difficulties in reading and comprehension.28, 30 Through FGDs, interviews, and review of resources,31–36 strategies for the above skills were identified.
It is noted in the literature that one method cannot improve all academic areas. For example, phonologically-based methods do not address all aspects of reading disorder, such as reading fluency and comprehension.37, 38 Considering this fact, the current module encompasses many evidence-based strategies to encourage a child’s overall academic performance. These children may also have deficits in information processing and social skills, affecting their academic performance.39, 40 Hence, it is believed that cognitive retraining targeting the areas of attention, memory, and visuospatial abilities may significantly enhance cognitive function and simultaneously improve performance in mathematics and other skills.38, 41, 42 Additionally, to deal with a child’s social and behavioral difficulties, it is necessary to encourage children to cooperate and build positive relationships with peers and behave appropriately. 43 Because of this, along with learning strategies, cognitive training, social skills training, and behavior management were incorporated in the HBI.
When parents repeatedly fail to manage their child’s concentration on homework, along with the fact that they frequently receive complaints from school teachers regarding academics and problem behaviors, they feel disappointed and at times give up. 26 Moreover, they start experiencing stress,26, 27, 44 disturbing their parent–child relationship. 45 Thus, the quality of caregiving and caregivers’ psychosocial well-being should be promoted and supported.46, 47 In-depth family education about SLD, remedial programs, and parenting techniques to manage behavioral problems need to be provided by MHPs to enhance the caregivers’ psychosocial well-being.26, 29 Hence, relaxation and problem-solving skill training were included in the module.
In India, the mothers primarily take the responsibility of dealing with children’s academic and behavioral problems at home. Mothers or caregivers should not face difficulties maintaining a good balance between their family life and the child’s skills training. Thus, every task in HBI has been kept for 10 to 15 min of practice. Additionally, the child’s homework can be used as the reading and writing materials so that practice does not demand extra time. Parent training for 45 to 60 min per session for six months was based on previous literature that had reported effectiveness of parent-implemented intervention in rehabilitating the child’s reading, writing, and mathematical problems.16, 17, 48–50
Moreover, this study was an effort to develop an HBI adapted for Indian children with SLD, making the intervention relevant for Indian school-going children. It will also impact the child’s compliance with intervention as the parents will carry it out at home.
Despite the strengths of the index study, one must consider a few limitations too. Our study is exploratory research that used a qualitative method where the given sample was small and restricted to the diagnosis of SLD-mixed type. A limited workforce or experts is an issue in India. Therefore, only a few professionals working with children with SLD have participated in the study. Finally, the results of this study must be considered exploratory; further evaluations for feasibility, acceptability, and effectiveness of HBI are required.
Conclusion
Index study described the development of the HBI program and attempted to provide an orientation and update for MHPs, educators, teachers, and parents who want to support their children with SLD. Its design was based on a theoretically robust empirical base, previous intervention studies, and a combination of perspectives and strategies provided by different stakeholders in the field of SLD. HBI offers a comprehensive and promising new form of intervention for SLD that may widen its boundaries from an excessive focus on fixing scholastic skill difficulties to incorporating behavioral and emotional well-being of the children with SLD and from center-based tutoring by researchers/educators to home-based tutoring by parents. The results definitely add crucial points to the existing literature for adopting interventions for the holistic development of children with SLD. However, much work needs to be done with more sophisticated study designs to establish the evidence base for the efficacy of HBI for children with SLD and the generalizability of its effects.
Footnotes
Declaration of Conflicting Interests
The authors have no potential conflicts of interest to declare with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.