
Abstract
Background:
Cognitive dysfunctions play a critical role in the psychopathology of depression. They regulate various psychosocial and functional outcomes and affect workplace functionality, productivity, and relapses. An objective evaluation of affected cognitive domains is germane in understanding the relapses and functional recovery in depression. Thus, to know cognitive dysfunctions beyond affective biases, this study was conducted to compare the cognitive functions of drug-naïve patients with unipolar depression with healthy matched controls.
Methods:
Fifty patients diagnosed with unipolar depression as per the International Classification of Diseases, tenth revision: Diagnostic Criteria for Research (Depressive Episode and Recurrent Depressive Disorder) and 50 healthy controls were enrolled on an outpatient basis from January 2022 to June 2023. Cases were regrouped as mild, moderate, and severe based on Beck’s Depression Inventory (BDI-II). A battery of tests assessed the cognitive functions: Wisconsin Card Sorting Test, Trail Making Test, Visual Retention subtests of PGI Battery of Brain Dysfunction, Digit Span, and Verbal Memory. The Massachusetts General Hospital Cognitive and Physical Functioning Questionnaire was used for a subjective assessment of cognitive functioning.
Results:
The sociodemographic characteristics of cases and controls did not differ significantly. However, within-group and between-group analyses revealed significantly lower performance of cases compared to controls. Cognitive impairment was positively correlated with BDI-II scores.
Conclusion:
Depression is associated with dysfunction in the domains of planning, attention, sustained attention, and visual and verbal memory. This dysfunction is independent of cognitive and affective bias and may exist even after clinical remission.
Keywords
There is a high prevalence of cognitive dysfunction in depression which is independent of subjective cognitive and affective bias.Key Message:
Unipolar depression continues to be a part of the major classification systems to date. The tenth edition of the International Classification of Mental and Behavioral Disorders (ICD-10) is elaborated under the categories of depressive episodes, recurrent depressive disorder (RDD), and persistent mood (affective) disorders (dysthymia). 1 In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), they are congregated under the unified category of depressive disorders and include major depressive disorder (MDD) and persistent depressive disorder as specifiers. 2 The disorder continues to be diagnosed with the help of core criteria and additional criteria, which emphasize more on conation cum affect and less on cognition. 3 ICD-10 enlists complaints or evidence of diminished ability to think and concentrate/vacillation as a cognitive criterion for depressive episodes. 1 The cognitive criteria for MDD in DSM-5 are a diminution in the ability to think or concentrate or indecisiveness nearly every day (either by subjective account or as observed by others). 2
In 1967, Beck and colleagues postulated that biased acquisition and processing of information influence the etiology and course of depressive episodes. 4 They concluded that internal mental representations, or schemas, affect the perception of depressed individuals about themselves and the world around them and divided the depressive symptoms into emotional, cognitive, motivational, physical, and vegetative. 5 Evidence emphasizes emotional valence as a moderator of neural abnormalities in depression and resultant depression-associated deficits in the control of attention and biased processing of emotional information. 6 This cognitive affective bias theory has been able to reflect the distorted information processing and/or shift in focus from positive to negative stimuli and abnormal responses to negative feedback and decision-making, that is, preferential processing of negative materials. 7 Some studies found increased error rates and longer reaction times during executive function tasks, which are unexplainable with cognitive-affective bias alone, 8 whereas other studies pointed out that if the task demands sustain depressed participants’ attention and they have no opportunity to ruminate, cognitive deficits cease to appear. 9 This has led to a shift of focus from emotion processing dysfunctions in depression to cognitive dysfunctions in depression.
Cognitive functions (CF) are the processes that regulate cognition to flexibly guide behavior toward a goal, especially in novel situations. 10 Their deficits encompass problems in planning, completing goal-directed activities, organizing, initiating, sequencing, shifting, information processing speed, and working memory. The research has demonstrated impaired performance in various domains of CF in patients with depression, like inhibition or termination of a pre-potent response and shifting or alternating attention between tasks or mental sets.11, 12 Much of these cognitive deficits persist even after the complete remission of treatment, thereby providing strong evidence that cognitive deficits are more possibly integral components of depressive disorders than merely the byproducts of other symptoms.13, 14 They are integral to cognition as well as secondary to the other symptoms of depression, such as psychomotor retardation, motivation, fatigue, insomnia, and mood disturbances. They are associated with poorer treatment responses and suboptimal vocational rehabilitation. 15 Executive dysfunction has progressively been a target in ongoing clinical trials of novel antidepressant drugs.16, 17 Though there are many studies across the globe exploring CF in depression,18–24 there are only a few in the Indian subcontinent.25, 26 This study aims to compare the CF of drug-naïve patients with unipolar depression with healthy matched controls.
Methods
A cross-sectional, observational, non-interventional, single-time assessment, hospital-based study was carried out on 50 drug-naïve patients with depression and RDD attending the outpatient service unit in the psychiatry department of a tertiary care hospital. A purposive sampling technique was used. The patients were diagnosed using the International Classification of Diseases tenth revision: Diagnostic Criteria for Research (ICD-10 DCR). 27 Patients with RDD were in relapse but off-medication for at least one month before presentation. Fifty age- and sex-matched healthy males were recruited as controls. The sample size was calculated using the mean and prevalence from an earlier study. 28 Patients with diabetes, hypertension, cardiovascular disease, dementia, and mental retardation were excluded, as these disorders impair cognition independently. A structured proforma was used to record the psychosocial profile and relevant medical history. Ethics clearance was taken from the Institutional Ethics Committee vide Reference IEC/Oct/2021 dated October 12, 2021, and data was collected from January 1, 2022, to June 30, 2023, by the Declaration of Helsinki 1975, revised in 2000.
Beck’s Depression Inventory (BDI-II) was administered to both patients and controls. BDI-II is a 21-item self-rated 4-point Likert scale, 0 to 3 (0 = least, 3 = most), with a score range of 0–63. Scores up to 13 are interpreted as minimal depression, from 14 to 19 as mild depression, from 20 to 28 as moderate depression, and from 29 to 63 as severe depression. There are two subscales of BDI-II, including a cognitive-affective subscale and a somatic-performance subscale, to measure the full spectrum of depressive symptomatology. BDI has good internal consistency with α ranging from 0.76 to 0.95 in psychiatric samples and 0.73 to 0.92 in non-psychiatric samples. It has a high test-retest reliability with a correlation of up to 0.86. It has been used in a range of cultural settings. The construct validity of BDI has high correlations with other standardized rating scales for depression. 29 Objective cognitive assessment was done using the Wisconsin card sorting test (WCST), computerized trail-making test (TMT), visual retention subtests of PGI Battery of Brain Dysfunction (PGI BBD), paper-and-pencil tests of digit span (DS), and verbal memory (immediate and delayed recall).30, 31 The Massachusetts General Hospital Cognitive and Physical Functioning Questionnaire (CPFQ) was employed for subjective assessments of cognitive functioning. 32
IBM Statistical Package for Social Sciences (SPSS) version 25 was used for statistical analysis. Chi-square was used to measure the difference between various socio-demographic, clinical, and neuropsychological variables, and t-tests were applied to discrete and continuous variables, respectively. Pearson’s correlation was used to determine the correlation, if any, between the variables. Descriptive statistics were applied to obtain the means and frequencies of socio-demographic and clinical data. It was found that most of the data was not normally distributed. Thus, the Kolmogorov–Smirnov test was used to check for the distribution of data on the ASEX, and Friedman’s analysis of variance (f ANOVA) test was used to compare the continuous variables. The mean scores on all the domains were compared across the study groups using the f ANOVA, and proportions and levels of significance were calculated from this.
Results
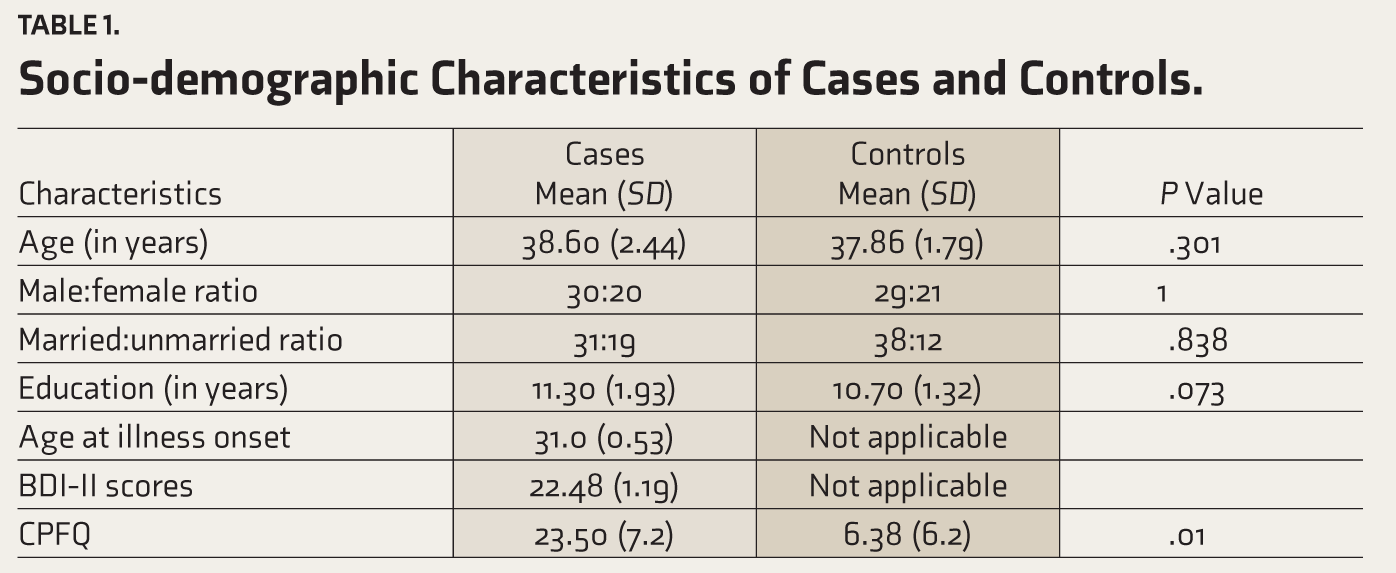
The mean age of cases and controls was 38.6 and 37.86, respectively. Sixty percent of patients and 58% of controls were male, and 62% of cases and 76% of controls were married. Most of the cases and controls were formally educated up to the 12th grade. In summary, the case and control groups did not differ significantly in baseline socio-demographic characteristics of age, marital status, and years of education (Table 1).
Socio-demographic Characteristics of Cases and Controls.
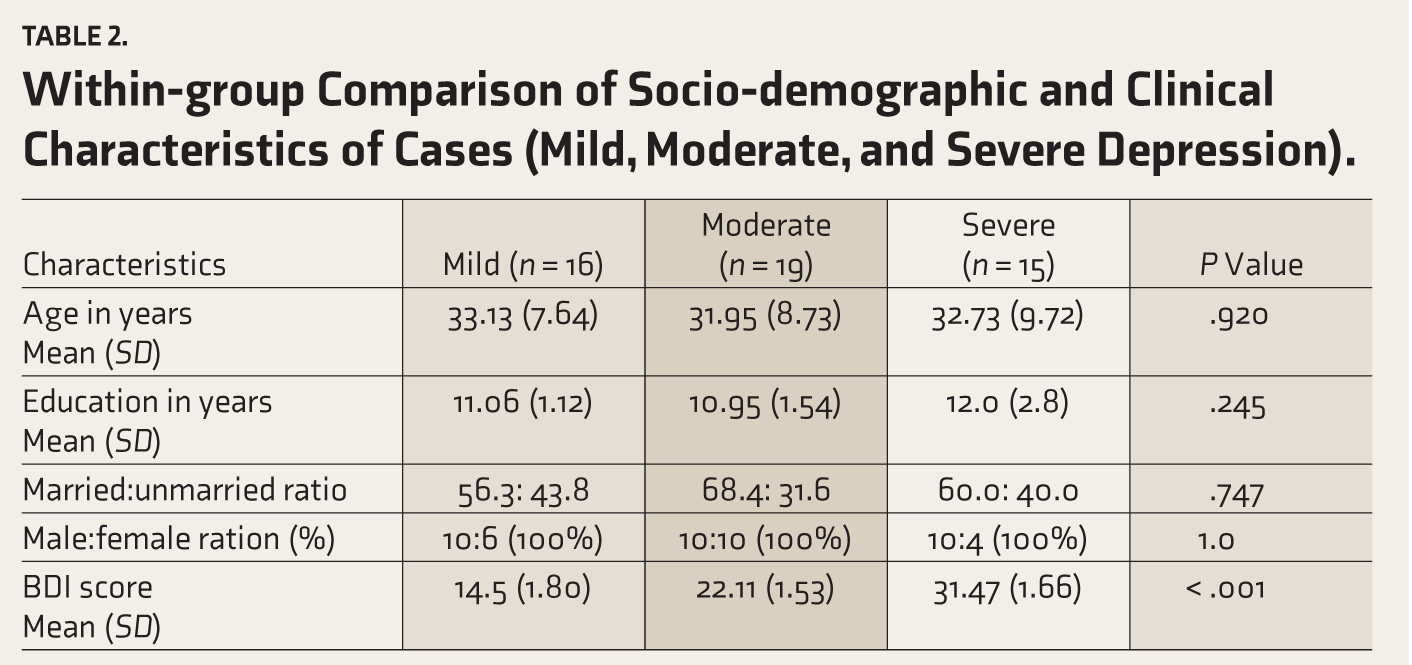
The cases were diagnosed as per ICD-10 DCR. The groups were divided into mild, moderate, and severe depression based on scores of BDI-II. In comparison between these groups, no statistical difference was found between age, education, and marital status. The mean BDI-II score in the mild depression group was 14.5, in the moderate depression group was 22.11, and in the severe depression group was 31.47 out of a maximum score of 63 (Table 2). However, the difference was significant regarding their BDI scores (p < .001).
Within-group Comparison of Socio-demographic and Clinical Characteristics of Cases (Mild, Moderate, and Severe Depression).
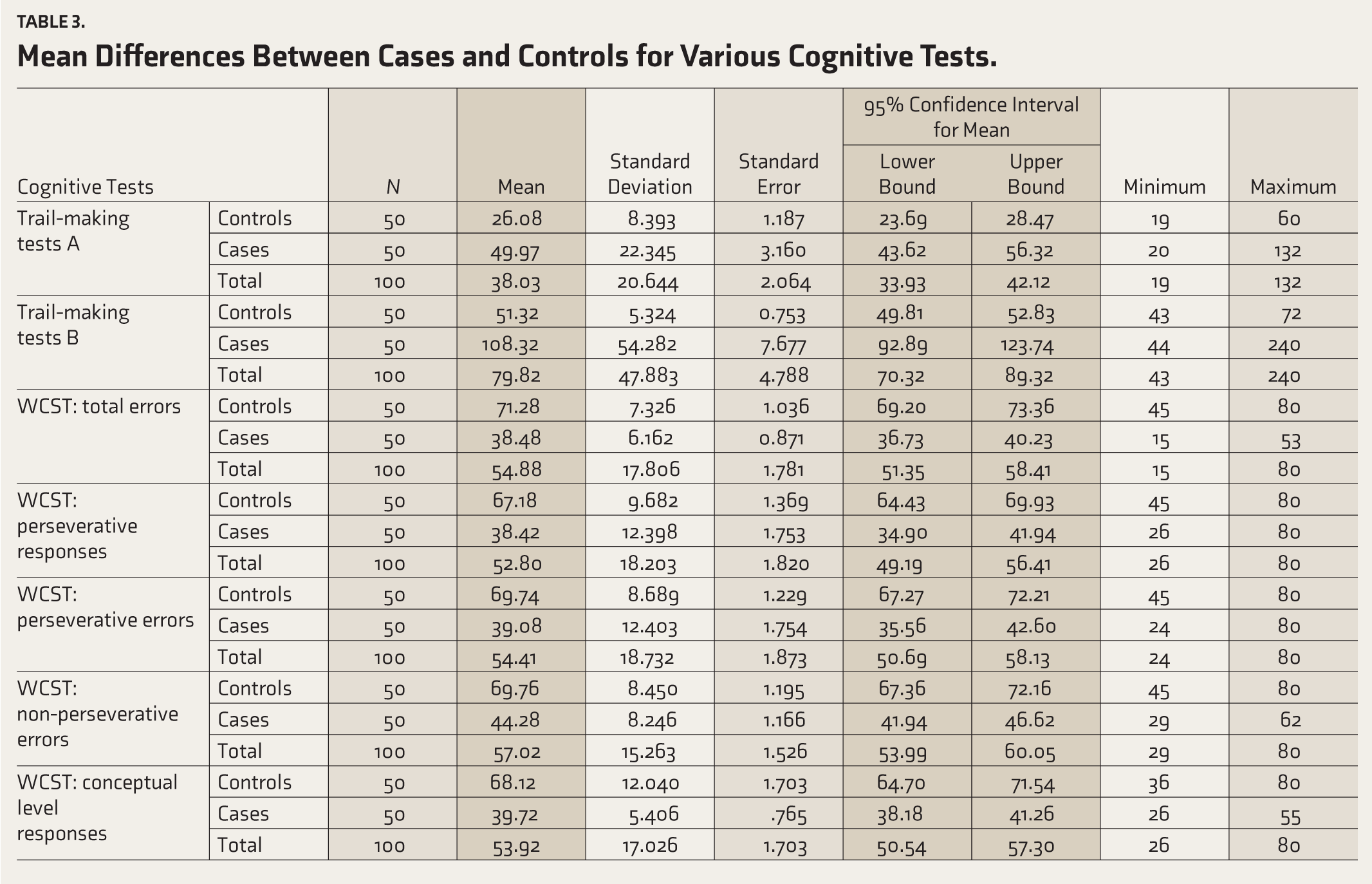
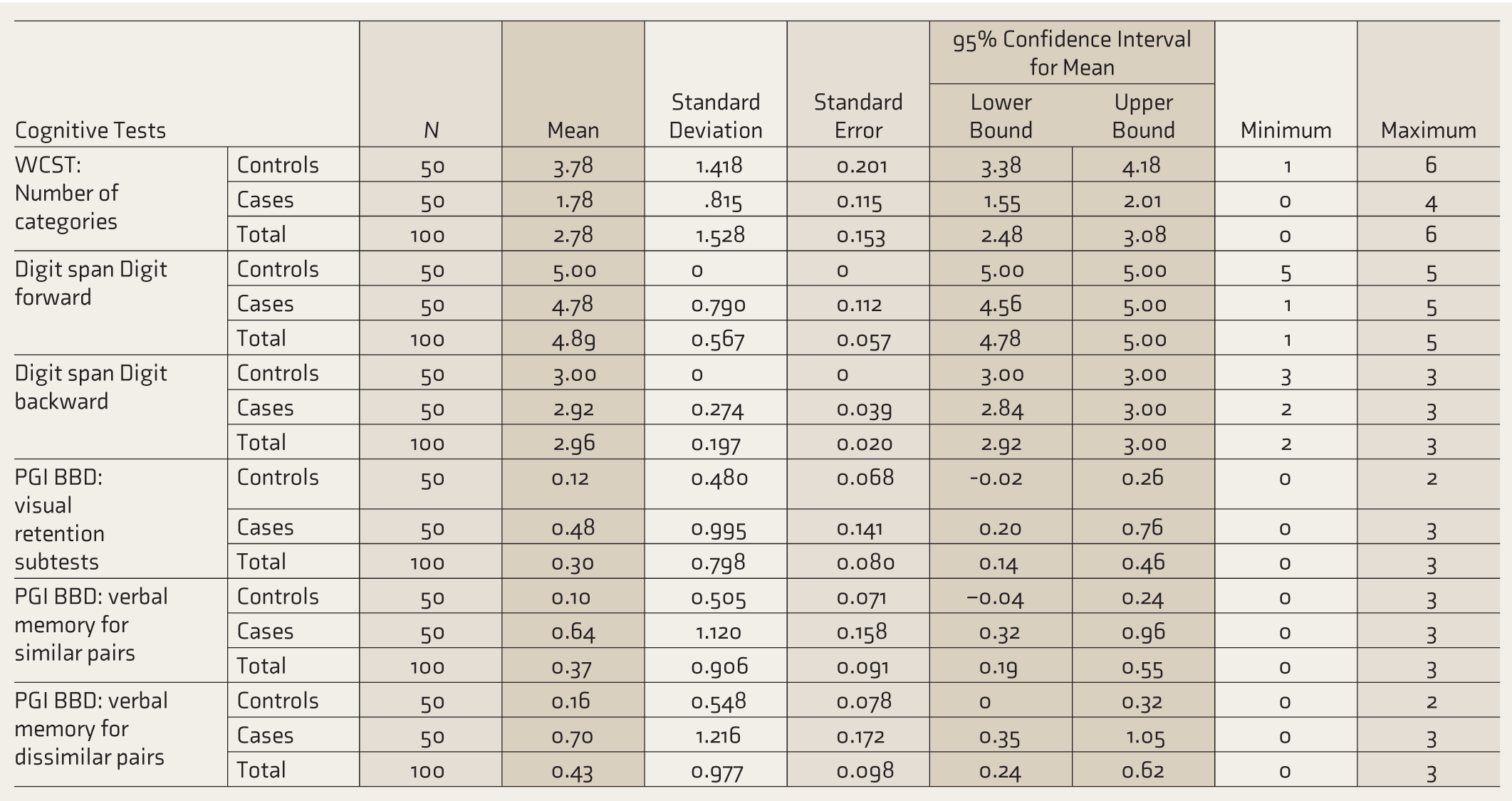
Freedman’s analysis of variance between cases and controls for TMT, WCST, DS, and PGI BBD visual memory and verbal memory tests revealed low performance in cases, which was statistically significant compared with controls. The controls performed better than patients in all these cognitive tests (Table 3).
Mean Differences Between Cases and Controls for Various Cognitive Tests.
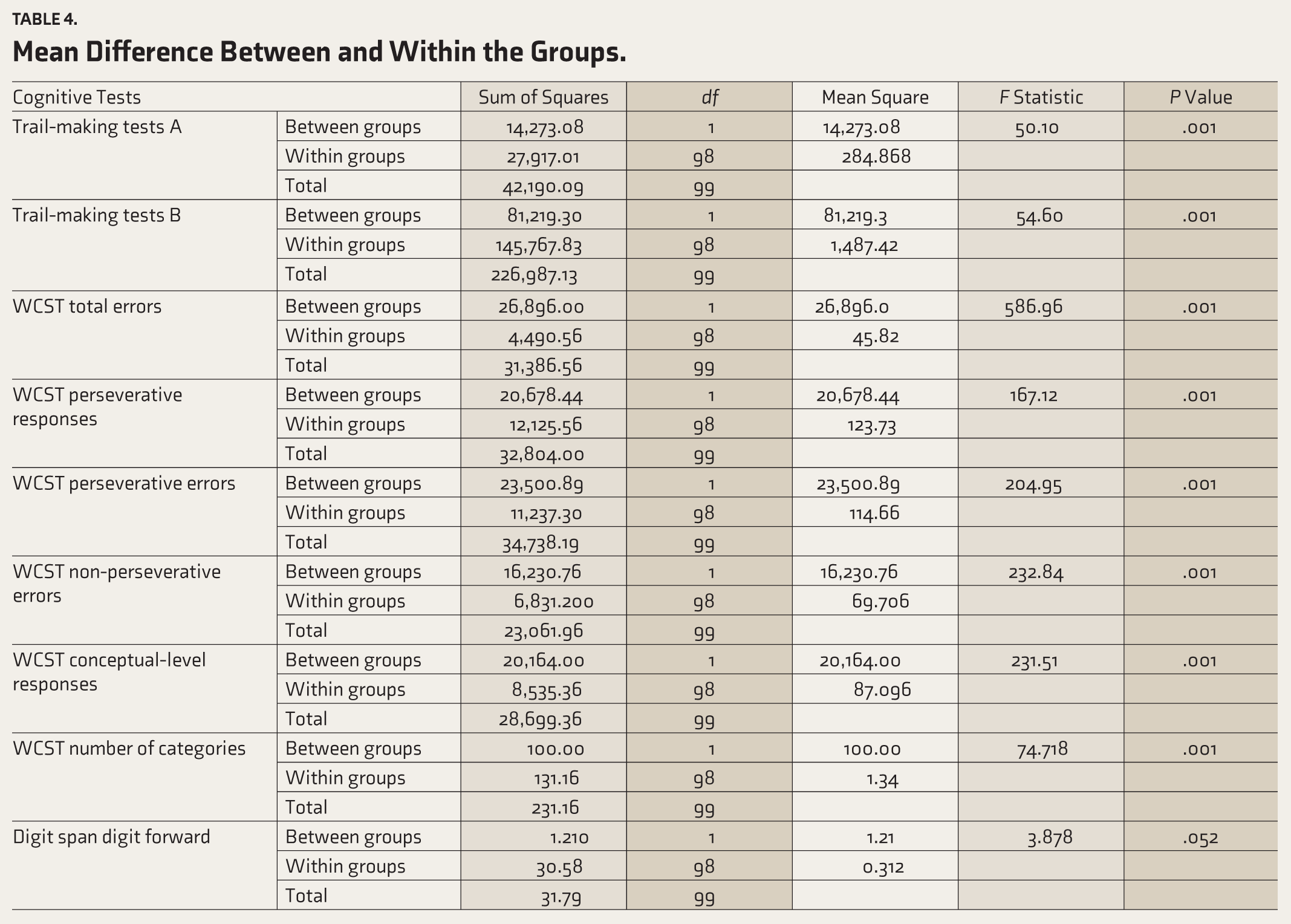
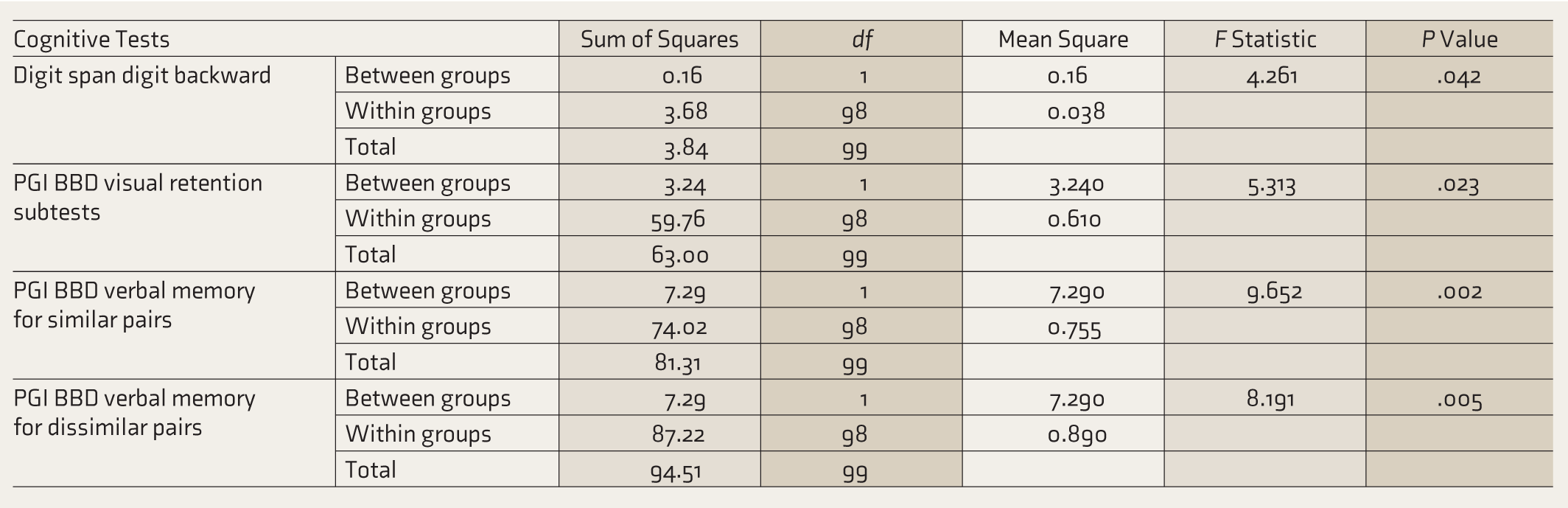
Freedman’s analysis of variance between case groups (mild, moderate, and severe) and within a case group for TMT, WCST, DS, and PGI BBD visual memory and verbal memory tests revealed low performance between case groups. On running the battery of tests on cases of the same group (within the group), the difference observed was not statistically significant (Table 4). This indirectly corroborated the fact that the participants in each case group did not differ in severity of illness, and thus, the study participants were correctly grouped as per the severity of illness other than the existing socio-demographic domains.
Mean Difference Between and Within the Groups.
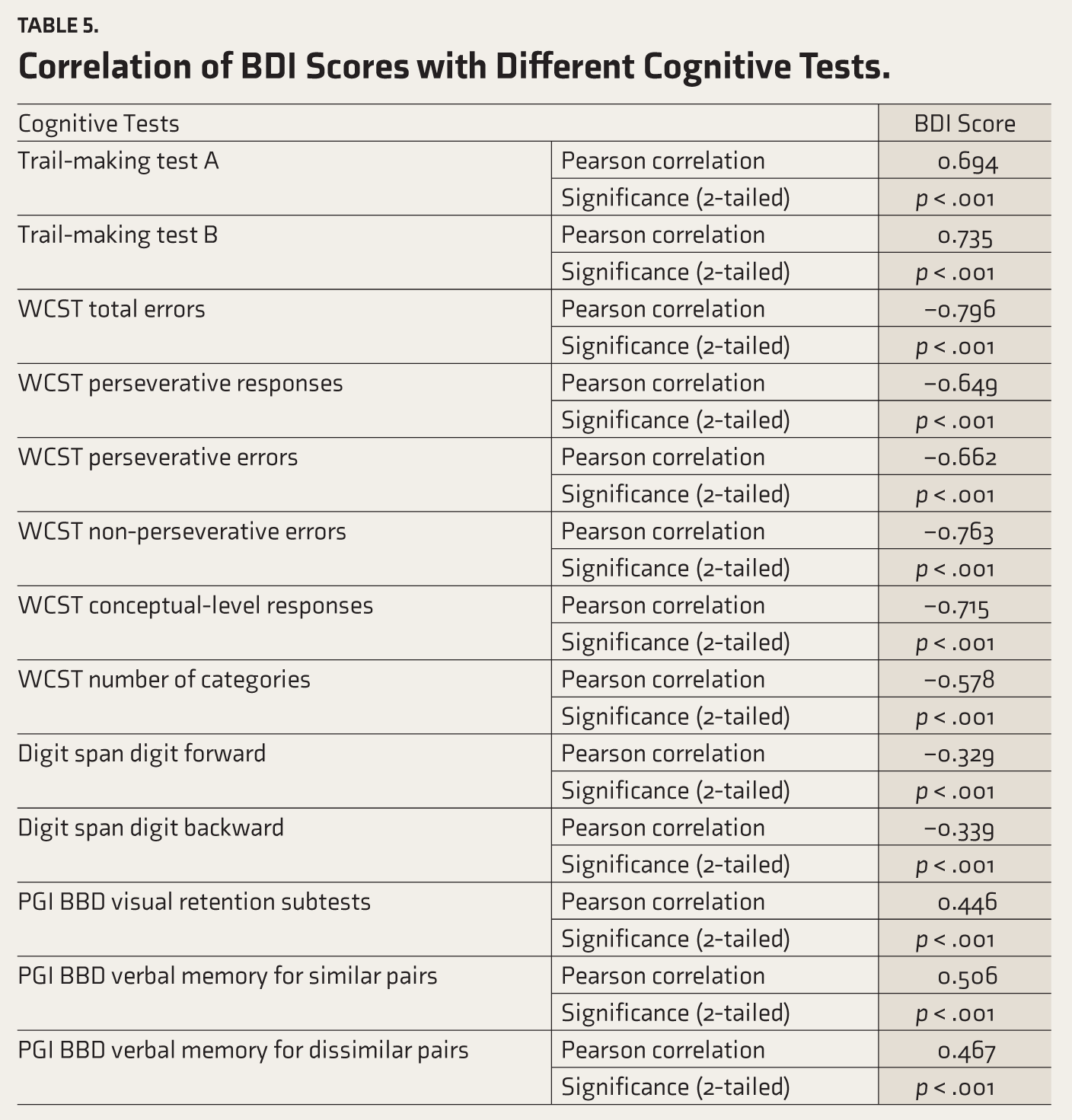
Another important finding of this study was the relationship between increasing BDI-II scores and cognitive performance. The BDI scores were positively correlated with PGI BBD and the trail-making test, while they were negatively correlated with WCST and DS. It was found that cognitive impairment in some cases was directly related to BDI score severity. In other words, the more severe the depression, the worse the performance on cognitive tests (Table 5).
Correlation of BDI Scores with Different Cognitive Tests.
Discussion
Our study found that almost all the patients had deficits in one or the other domains of the cognitive test battery used in the study. Our results are consistent with a study that concluded that cognitive deficits are likely to be a persistent feature in some forms of adult-onset MDD. 33 Also, another recent meta-analysis has buttressed our results by showing a modest but significant relationship between clinical depression and subthreshold depression with cognitive control measures, namely, inhibitory control, planning, cognitive flexibility, and set-shifting. 22 This prevalence is higher than the prevalence found in studies done in Europe (83%) and the Mediterranean (76.6%).34, 35 Also, our results are far higher than results in Asia and the Indian subcontinent, which showed a varied range of cognitive dysfunction in acutely depressed and remitted patients from 12.6% to 58%.25, 36 This variation might have resulted from different study designs, sample size differences, socio-cultural differences between those countries and India, and varied psychometry tools. In addition to the above variation, the geographic location of these countries and seasonal variations contributed to this variation. 37
WCST requires a complex set of cognitive functions, including the ability to think abstractly, selectively attend to a particular perceptual dimension, and shift cognitive set. The results of the present study show that patients with major depression exhibited significant deficits when performing the WCST. The finding of a significant difference between depressed and non-depressed healthy controls on WCST performance implies that there may be a relationship between state-related cognitive impairments during a depressive episode. The day-to-day performance of the individual may be affected not only by the depressed mood and motor retardation but also by the impairment in executive functions, and previous studies support this. These cognitive deficits should be acknowledged during clinical evaluation and treatment, and the patients need to be followed up and evaluated subsequently for the persistence of cognitive deficits and their effect on the rehabilitation aspects. Our study further unearthed that the relapse of depression progressively adds to existing cognitive impairment. The significant increase in perseverative responses and errors, trials for the successful completion of the first category, and lesser number of complete categories achieved by the patients as compared to the healthy controls highlighted the cognitive impairments in domains of ability to keep information of the ongoing sorting strategy (working memory), the ability to recognize a change in set, shift in sorting strategy accordingly, and the demand on cognitive reserve to conceptualize the change. This agrees with existing literature, which supports that a longer duration of illness worsens cognitive dysfunction, which is a risk factor for treatment resistance. In this context, some studies have revealed the possible role of the hippocampus in context-dependent memory and working memory.38, 39 However, most of the research focusing on executive dysfunction, as measured by the WCST, has drawn similar correlations of involvement of the frontal lobe in schizophrenia.40–42 Of late, the hippocampus seems to be influencing the domains assessed by the WCST, which were otherwise thought to be subserved by a fronto-subcortical circuit originating in the dorsolateral prefrontal cortex and orbitofrontal cortex and then projecting through the striatum and thalamus to return to the prefrontal cortex. 43
This study has some limitations as well. First, the precedence and outcomes of cases have not been addressed. This statistical analysis did not include the total duration of illness, and the study included drug-naive cases of both depressive episodes and relapsed recurrent depressive disorder. Thus, the impact of the duration of untreated depression on cognitive functions could not be assessed. Second, patient cooperativeness during the administration of cognitive battery might have affected the results due to long sittings and motivation for completion of the test inherently due to the core depressive symptoms themselves. Third, patients with more severe depression could have resulted in scores shaded by subjective affective bias and might have reflected far worse performance versus actual underlying cognitive dysfunction.
Further prospective observational studies comparing depressive and cognitive symptoms before and after treatment would provide more insights into the evolution of cognitive dysfunction in depression. Future research may also be performed to understand and evaluate the extent of cognitive dysfunction in the normative population. Cohort studies on unaffected sample populations may be conducted to study if mild cognitive impairment detected in such normal individuals predisposes them to the development of depression later in life. This may help in understanding the possible bidirectional relationship between depression and cognitive impairment.
Conclusion
Cognitive dysfunction is a core pathological feature of depression that is often under-valued in the management of the disorder. It serves as a principal mediator of functional and psychosocial outcomes, with implications for workplace productivity and an imminent return to work. This study supports the existing evidence of a high prevalence of cognitive dysfunction among patients with depression and found cognitive dysfunction in planning, attention, sustained attention, and memory. The result of this study further adds to current knowledge of the relationship between cognitive dysfunction, the severity of depression, and patient functioning. Also, it highlighted that the recognition and evaluation of objective measures of cognition are independent of subjective cognitive and affective bias. This objectified understanding of cognitive dysfunction may be considered an integral part of MDD management and is likely to be germane to improved functional outcomes in depression, particularly considering functional recovery beyond remission as well as in relapse of the disorder.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.