
Abstract
Background:
Executive function (EF) impairment has been demonstrated in patients with schizophrenia. This study attempted to examine the clinical and demographic correlates associated with the different components of EF in these patients using a comprehensive battery of neuropsychological tests.
Materials and Methods:
Consecutive inpatients with schizophrenia in remission were recruited. The following instruments were administered: (a) Positive and Negative Syndrome Scale (PANSS), (b)World Health Organization Disability Assessment Schedule 2.0, (c) Tower of London, (d) Stroop Test, (e) Controlled Oral Word Association Test, (f) Animal Names Test, and (g) Verbal N-Back Test. Sociodemographic and clinical details were also recorded. Data was analyzed using standard bivariate and multivariate statistics.
Results:
A total of 50 patients were recruited. The mean age of the population was 30 years (standard deviation [SD]: 7.74). The majority were male, literate, single, from a rural background, from a middle socioeconomic background, and unemployed. The mean dose of antipsychotic medication was 618.57 mg (SD: 282.08) of chlorpromazine equivalents per day. Impairment was found in the different sub-components of EF. On multivariate analysis, factors significantly associated with executive dysfunction were lower education, unemployment, lower income, positive PANSS score, higher antipsychotic dose, and history of treatment with electroconvulsive therapy.
Conclusion:
EFs encompass a wide range of cognitive processes that influence an individual’s ability to adapt and function in the society. These are often impaired in patients with schizophrenia. Clinicians need to be aware of these deficits and factors associated with them, to plan appropriate and effective remedial measures.
Executive function impairment in schizophrenia affects all domains of the individual’s functioning. Potentially modifiable factors such as the dose of antipsychotics and electroconvulsive therapy can significantly affect EF.Key Messages:
EFs consist of those capacities that enable a person to engage successfully in independent, purposive, and self-serving behavior. 3 It is an umbrella term that involves the regulation and control of processes such as working memory, reasoning, task flexibility, problem solving, planning, and execution. 4 These functions enable a person to develop and carry out plans, solve problems, adapt to unexpected circumstances, perform many tasks simultaneously, and adjust in the society. Deficits in EFs are not only present in patients with schizophrenia 5 but are also known to be present in adolescents who are at risk of developing schizophrenia and in the first degree relatives of patients with schizophrenia. 6 They can result in longer hospital stays, difficulties in everyday functioning, unemployment, poor treatment adherence, and increased medical comorbidities. 1
There are conflicting reports regarding the relationship between executive dysfunction and variables like gender, age, duration of illness, and severity of psychopathology. While some studies reported no significant associations, 7 other studies showed that demographic and illness-related factors do have an impact. 8
Studies from India have examined EF impairments in patients with schizophrenia in comparison to normal controls, those with bipolar disorder, and delusional disorder.9, 10 Associations between EF and sociodemographic, psychopathology, insight, suicide attempts, and functioning have been studied.11–16 A follow-up study reported deterioration in executive functioning in the ten years of treatment following diagnosis, 17 while improvement in EF has been reported following yoga therapy. 18
While many studies are limited by the lack of a range of tests done to assess EF, this study used a comprehensive battery of tests to evaluate different aspects of EF with a focus on clinical correlates that can potentially be altered to improve the patient functioning.
Materials and Methods
Participants
This was a cross-sectional exploratory study conducted between June 2013 and October 2014 in a tertiary care hospital. Consecutive inpatients who satisfied the International Classification of Diseases-10 (ICD-10) 19 diagnostic criteria for schizophrenia and were in remission 20 were contacted for possible recruitment to the study. Subjects between the ages of 18 and 65 years who were able to read English or Tamil were eligible to take part. Patients with severe language disorder; intellectual, visual, or hearing impairment; primary mood disorder; substance use disorder or organic disorder were excluded. The details of the study were explained and written informed consent was obtained from each participant and caregiver. Following recruitment, participants were assessed at a single point in time. All patients received treatment as usual. Sociodemographic details were collected by the principal investigator (JN), who also administered the tests of EF. Assessments of the severity of psychopathology and disability were carried out by the coinvestigator (SAV). The Institutional Review Board and Ethics Committee approved the study protocol.
Assessment
The following instruments were employed.
The Positive and Negative Syndrome Scale (PANSS): It was used to rate the symptom severity. 21 The PANSS is a clinician-rated scale considered as the gold standard to assess the clinical symptoms of schizophrenia. It consists of 30 items across three subscales: positive, negative, and general psychopathology. The positive and negative scales have seven items each, and the general psychopathology scale consists of 16 items. All items are scored from 1 to 7 based on severity.
World Health Organization Disability Assessment Schedule 2.0 (WHODAS) 22 : The WHODAS is a scale developed by the World Health Organization. It provides standardized disability levels and profiles across cultures in adult populations. It assesses disability across six domains: cognition, mobility, self-care, getting along, life activities, and participation. For this study, the 12-item version of the WHODAS 2.0 was used.
Tower of London (TOL): It measures the subjects’ ability to plan and to anticipate the results of their actions to achieve a predetermined goal. 23 It consists of two identical wooden boards, each consisting of three pegs of different height and three wooden balls. It requires the subject to rearrange the balls to match a model board in as few moves as possible. For this study, the NIMHANS version 24 was utilized.
Stroop Test: It measures response inhibition, which is the ease with which a person can maintain a goal in mind and suppress a habitual response in favor of a familiar one. 25 In this study, the Stroop Test from the NIMHANS Neuropsychological battery, standardized for the Indian population, was used. 24 The test consists of 176 words printed across 16 rows and 11 columns in four colors, with the color of the print occasionally corresponding with the color designated by the word. It involves two trials: first, reading the words as fast as possible column-wise, and second, naming the color the word is printed in, rather than the word. The score taken is the difference in time in seconds between the time taken to read the words from the time taken to name the colors.
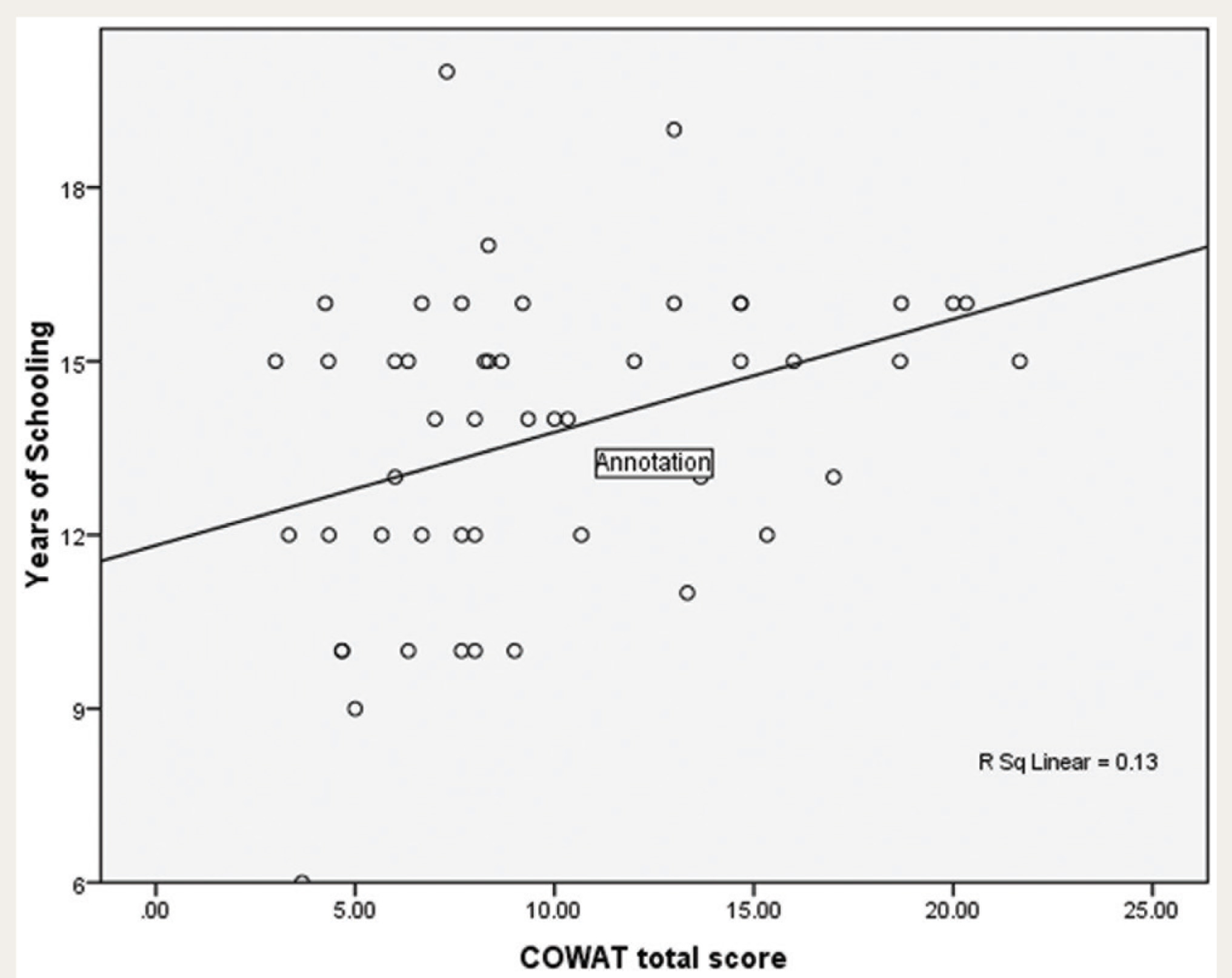
Relationship Between Controlled Oral Word Association Test Score and Education
Controlled Oral Word Association Test (COWAT): It measures phonemic or lexical fluency. It requires the examinee to generate a list of words beginning with a specific alphabet in a minute. The letters F, A, and S were used for English-speaking individuals, and the consonants “Ka,” “Pa,” and “Ma” were used for Tamil-speaking individuals. Proper nouns and names of numbers were excluded. The score taken was the average number of words across the three trials. 24
Animal Names Test: It measures categorical fluency and requires the subject to name as many different animals as possible, excluding the names of fish, birds, and snakes, in one minute. The total number of words generated is taken as the score. 24
Verbal N-Back Test: It measures verbal working memory. The 1 Back and 2 Back versions of the test were used. 24 It consists of 30 random consonants that are read out, of which nine are repeated randomly. In N-Back 1, the subject responds whenever a consonant is repeated consecutively, and in N-Back 2, whenever a consonant is repeated after an intervening consonant. The score is the number of hits and errors in each.
Pro forma for Sociodemographic and Clinical Variables: Information related to sociodemographic variables and clinical details (duration and severity of illness, treatment variables, etc.) were recorded in this.
Statistical Analysis
Mean and SD were employed to describe continuous variables, while frequency distributions were obtained for categorical data. Student’s t-test was used to assess the significance of associations between categorical and continuous variables, and Pearson’s correlation was used to assess the correlation between continuous variables. Multiple linear regression was done to adjust for age, education, and the number of sessions of electroconvulsive therapy (ECT). SPSS version 16 was used for analysis.
Results
Sociodemographic and Clinical Characteristics of Study Sample
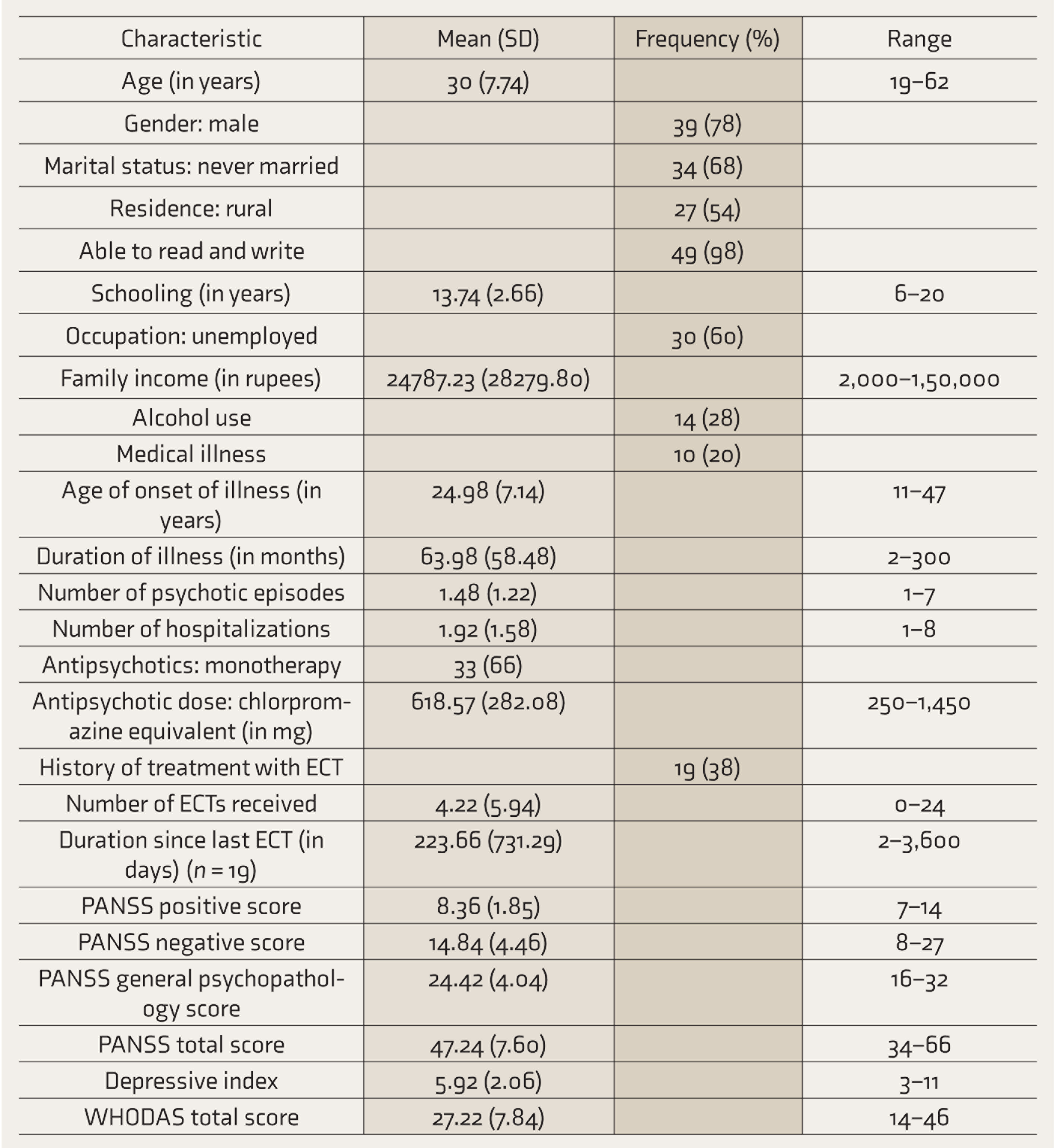
SD: standard deviation, ECT: electroconvulsive therapy, PANSS: Positive and Negative Syndrome Scale, WHODAS: World Health Organization Disability Assessment Schedule.
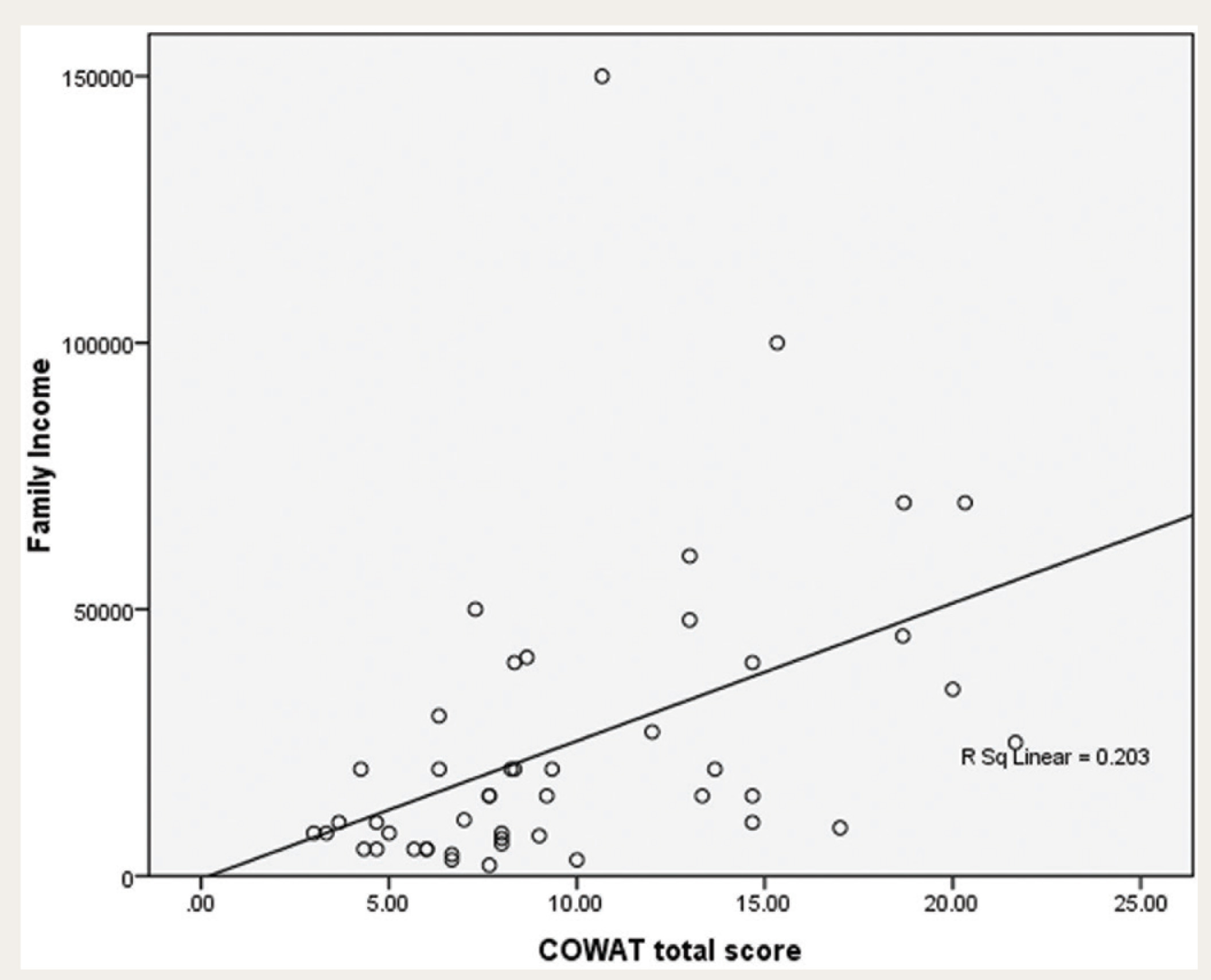
Relationship Between Controlled Oral Word Association Test Score and Income
Tests of Executive Functions
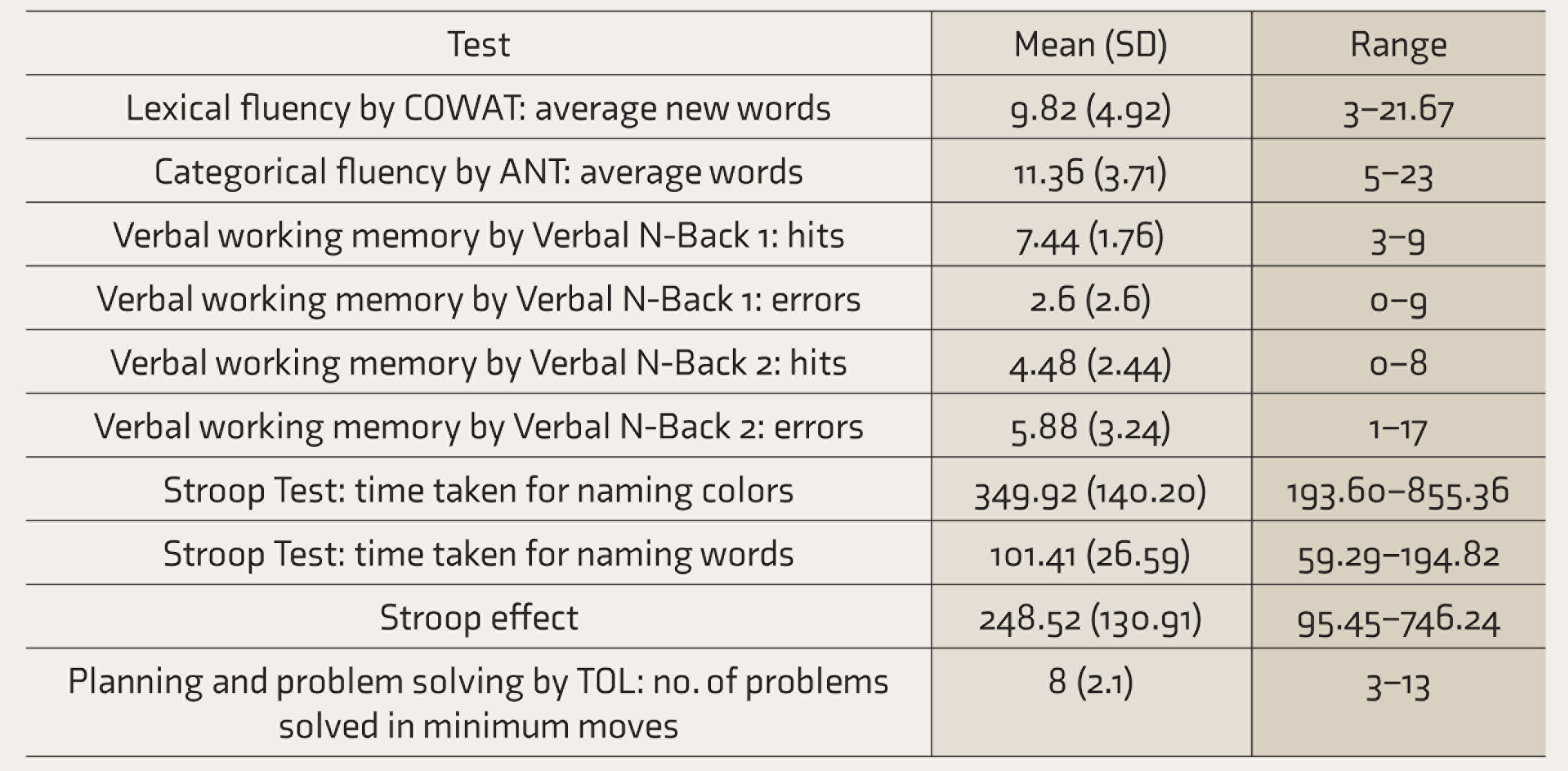
SD: standard deviation, COWAT: Controlled Oral Word Association Test, ANT: Animal Names Test, TOL: Tower of London.
Factors Associated with Lexical Fluency: COWAT Score
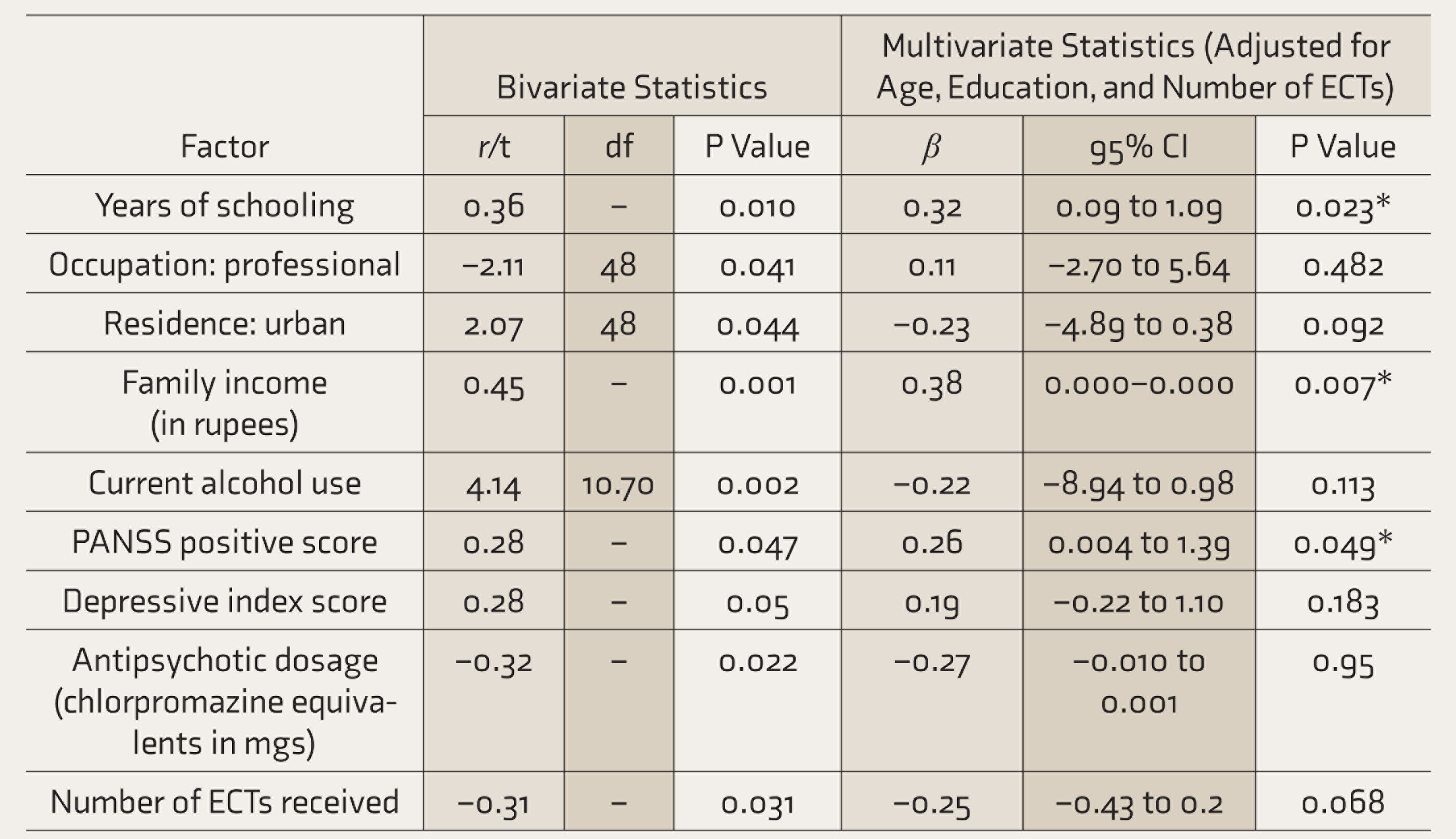
COWAT: Controlled Oral Word Association Test, r: Pearson’s correlation coefficient, t: t value on independent t-test, df: degrees of freedom, CI: confidence interval, ANT: Animal Names Test, TOL: Tower of London, ECT: electroconvulsive therapy.
Factors Associated with Categorical Fluency: Animal Names Test (ANT)
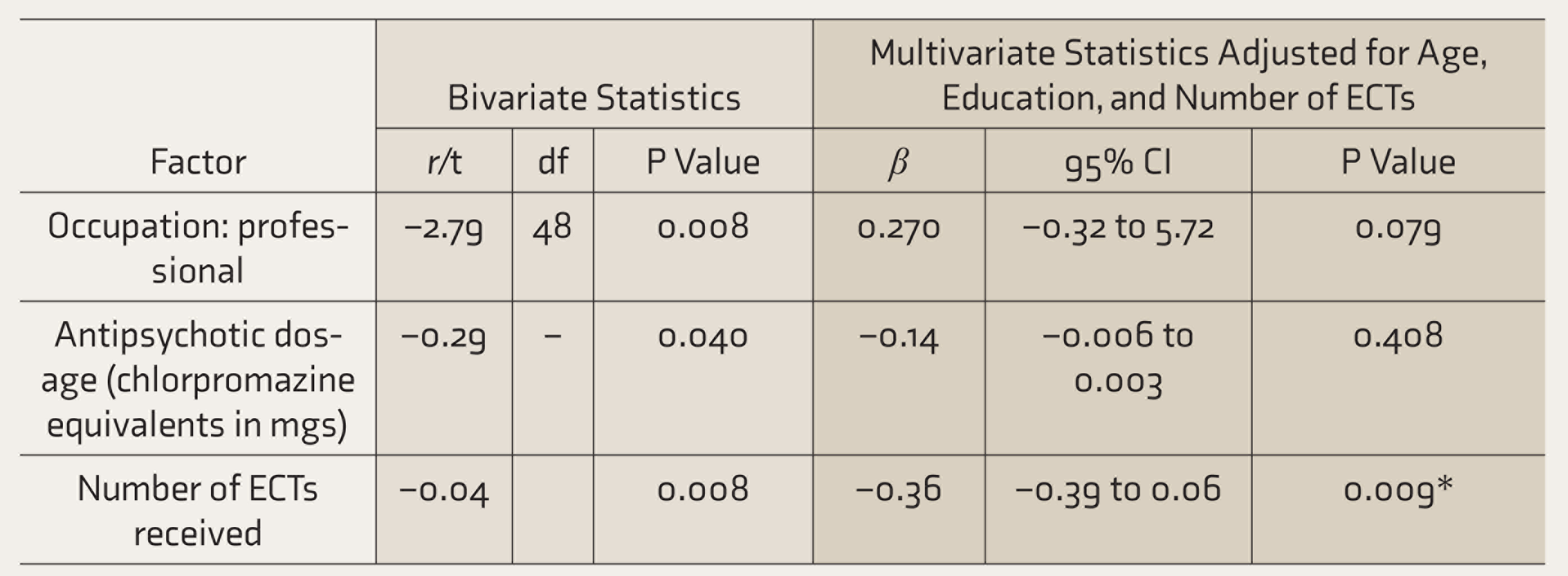
r: Pearson’s correlation coefficient, t: t value on independent t-test, df: degrees of freedom, CI: confidence interval, ECT: electroconvulsive therapy.
Table 3 shows the factors associated with lexical fluency as measured by the COWAT score. On bivariate analysis, lexical fluency score was positively correlated with years of schooling (Pearson’s r = 0.36, P = 0.010), family income (r = 0.45, P = 0.001), PANSS positive symptom score (r = 0.28, P = 0.047), and depressive index score (r = 0.28, P = 0.05), and negatively correlated with the total antipsychotic dose (r = –0.32, P = 0.022) and number of ECTs received (r = –0.31, P = 0.031).
Figures 1 and 2 show the relationship that the COWAT score has with education and income. Those who were employed as professionals (t = –2.11, df = 48, P = 0.041), who were not using alcohol currently (t = 4.14, df = 10.70, P = 0.002) and from an urban habitat (t = 2.07, df = 48, P = 0.044) had higher scores on the COWAT.
The factors that remained significantly associated with lexical fluency after multivariate analysis using linear regression were years of schooling (β = 0.32, 95% CI = 0.09–1.09, P = 0.023), income (β = 0.38, 95% CI = 0.000 - 0.000, P = 0.007), and PANSS positive score (β = 0.26, 95% CI = 0.004–1.39, P = 0.049).
Categorical fluency score based on performance on the Animal Names Test was found to correlate negatively with antipsychotic dose (r = – 0.29, P = 0.040) and the number of ECTs received (r = –0.40, P = 0.004). Those who were professionals had higher scores (t = –2.79, df = 48, P = 0.008). Only the number of ECTs remained significant on multivariate analysis (β = –0.36, 95% CI = –0.39 to 0.06, P = 0.009) (Table 4).
Factors Associated with Verbal Working Memory: N-Back 1 and 2
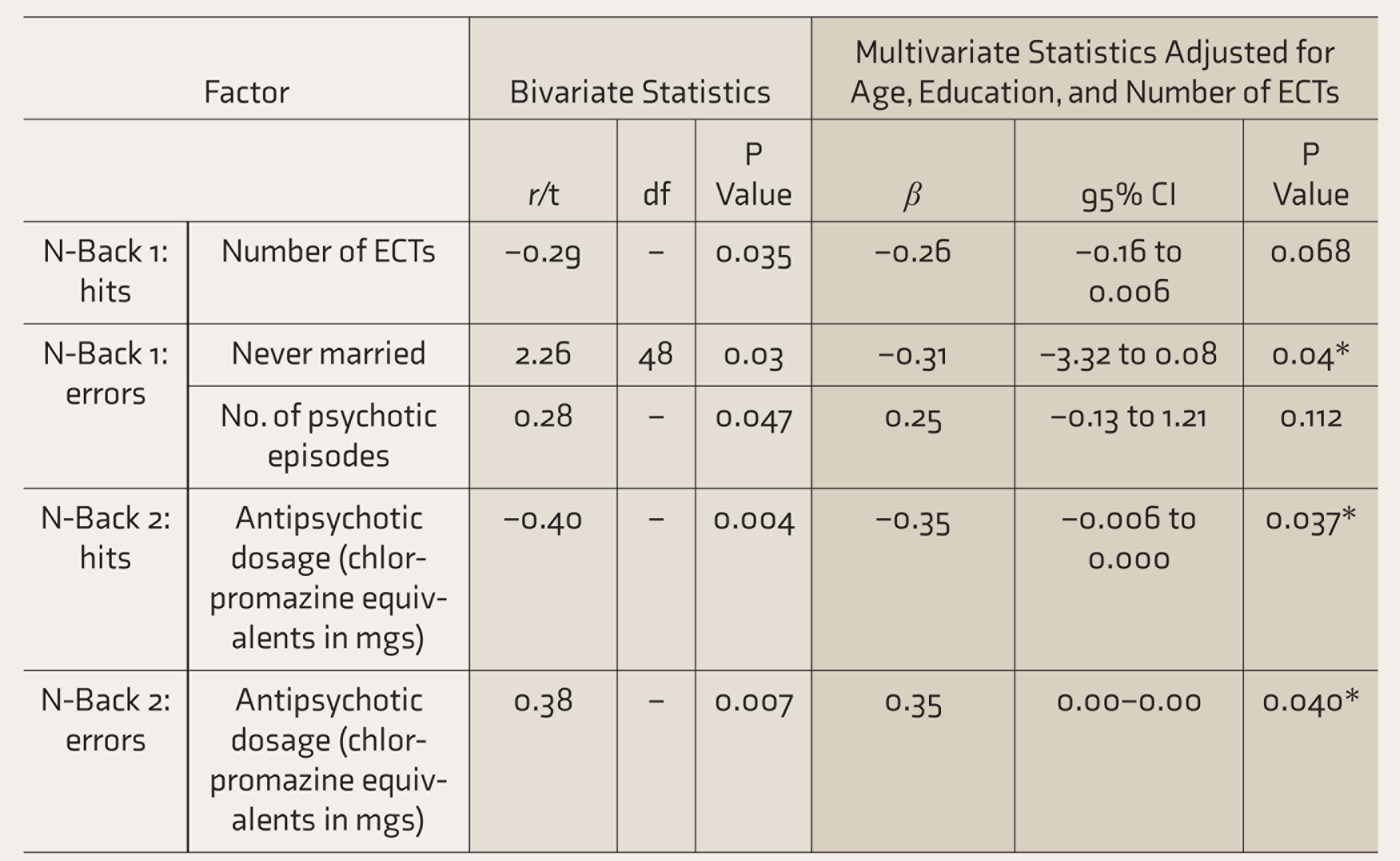
r: Pearson’s correlation coefficient, t: t value on independent t-test, df: degrees of freedom, CI: confidence interval, ECT: electroconvulsive therapy.
Factors Associated with Response Inhibition and Problem Solving
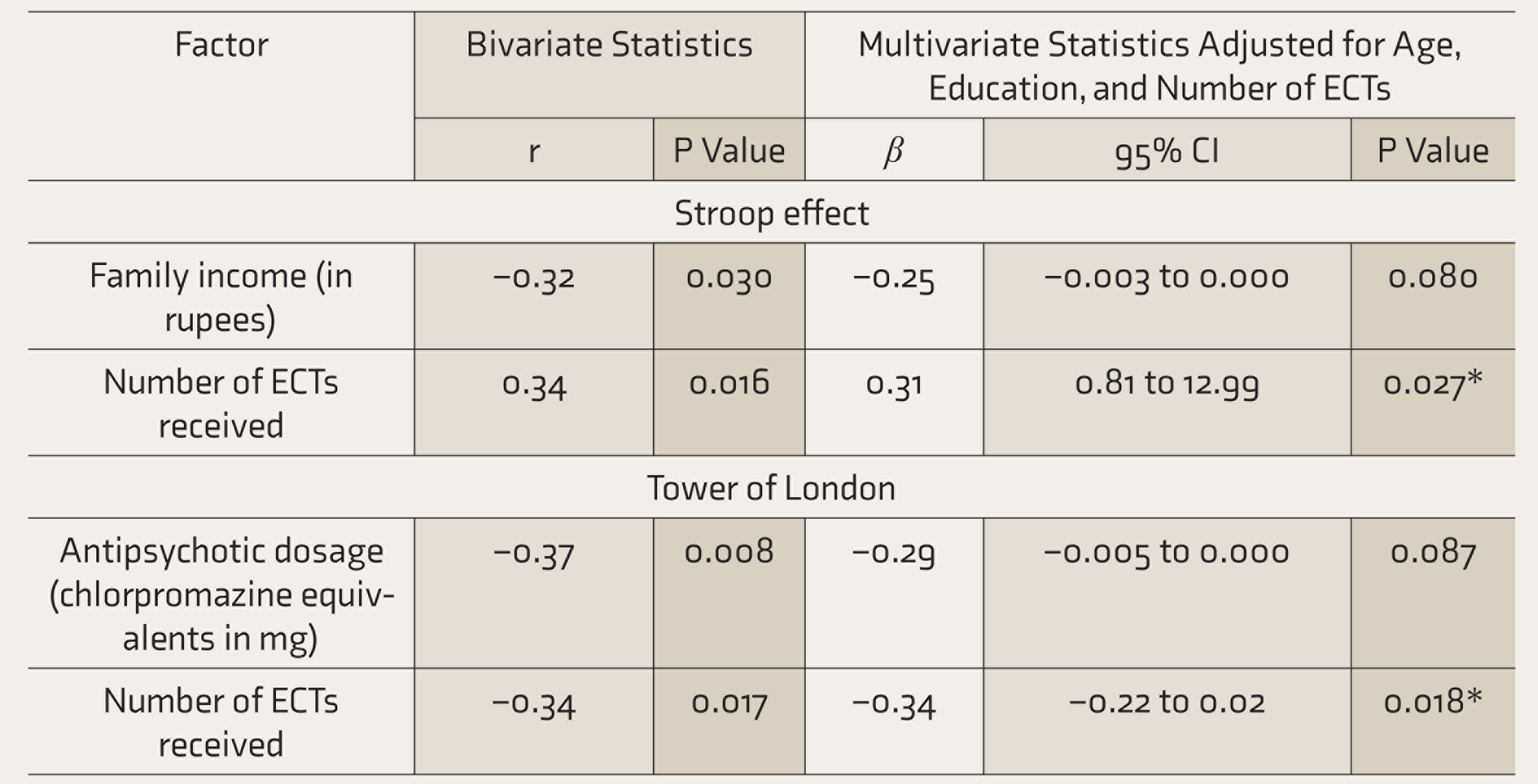
r: Pearson’s correlation coefficient, CI: confidence interval, ECT: electroconvulsive therapy.
On bivariate analysis, response inhibition score as measured by the Stroop Test was negatively correlated with family income (r = –0.32, P = 0.030) and positively correlated with the number of ECTs received (r=0.34, P=0.016); the latter remained significant on multivariate analysis (β = –0.31, 95% CI = 0.81–12.99, P = 0.027).
On bivariate analysis, problem solving score, as measured by the number of problems solved in minimum moves on the Tower of London test, was found to be negatively correlated with both antipsychotic dosage (r = –0.37, P = 0.008) and the number of ECTs received (r = –0.34, P = 0.017). Number of ECTs remained significantly associated on linear regression (β = –0.34, 95% CI = –0.22 to 0.02, P = 0.018) (Table 6).
The following factors were not significantly associated with EFs: age, gender, medical illness, age of onset and duration of illness, number of hospitalizations, and the disability score on WHODAS.
Discussion
This study adds to the existing literature regarding the correlates of EFs in patients with schizophrenia. Several cognitive functions have been included under the label of EFs. Many of them are independent of each other, are often multidimensional, and encompass several sub-component processes. This is evident in this study, as factors that influence the performance on one test of EF did not always have a similar effect on the other tests.
A few studies have reported greater deficits in some aspects of cognitive and EFs in males with schizophrenia.26, 27 However, this study did not find gender-specific differences, and one earlier study too had similar findings. 28
Most studies have demonstrated that in older patients with schizophrenia, cognitive impairment is more severe, with a significant decline in EFs.6, 29 However, no significant correlation was found between age and deficits in EFs in this study, similar to some earlier reports.7, 30
Higher levels of education are thought to reduce the risk of cognitive decline in people as they age, by increasing the cognitive reserve, maintaining the neuronal function, stimulating neural growth, and recruiting alternate neural pathways to maintain cognitive function. Therefore, regular involvement in intellectual activity during one’s lifetime has been considered a successful preventive intervention to reduce the risk of dementia.31, 32 This has also been shown to be applicable in schizophrenia, where lower education predicted more cognitive decline and years of education showed a positive correlation. 33 Murray et al. postulated that better premorbid educational attainment may compensate for deficits that occur as a result of the illness. 34 This matches with the findings of the present study, where years of education had a positive correlation with all tests of EF, and the relationship was significant in the case of lexical fluency. This specific association may reflect the larger mental lexicon or store of organized words that an individual acquires with a greater duration of formal education.
This study also found a significant association between categorical fluency and occupation; those who were employed as professionals had higher scores on this test. While the cross-sectional nature of this study does not allow us to conclude the direction of this association or causality, this finding has been reported by other researchers also who found that the relationship persisted even when the effect of education was controlled for.35–37
In this study, lexical fluency scores were found to be positively correlated with income. A similar relationship between cognitive function and socioeconomic outcomes has been demonstrated in some 38 but not other studies. 30 Findings on the relationship between the different symptom groups of schizophrenia and EFs have been varied. Most studies have noted that the severity of negative symptoms correlates with poor performance on measures of EF, while almost no correlation has been found between positive symptoms and EFs. 7 We found an association between the positive symptom score and lexical fluency scores on bivariate and multivariate analyses. Bagney et al. noted a correlation between negative symptoms and EF deficits, which varied with the duration of schizophrenia. 39
We did not find any association between the duration of illness and EF deficits, similar to that reported by Sabeshan et al. 7 ; contrasting findings have been reported of greater EF impairment in patients with longer periods of untreated psychosis2, 40 and shorter illness duration being associated with stronger improvement during cognitive remediation. 41 In this study, patients with three or more psychotic episodes were found to show more severe deficits in lexical fluency and working memory in comparison to those with fewer episodes, but this did not remain significant on linear regression analysis.
While antipsychotic medications remain the mainstay of treatment in schizophrenia, there is emerging literature regarding the possibility that these drugs may contribute to the genesis of some of the abnormalities usually attributed to the disease. 42 In the present study, the dose of medication was significantly correlated with the different aspects of EFs, with higher doses associated with greater dysfunction in lexical and categorical fluency, verbal working memory, and problem solving. The negative influence of higher doses of antipsychotics and anticholinergics on executive and other cognitive functions have been previously reported.43, 44 The use of antipsychotic medications with more anticholinergic effects and higher lifetime antipsychotic dose-years have been found to be significantly associated with a poorer cognitive composite score, with no difference between the typical and atypical antipsychotics.45, 46 Cognitive remediation programs have found that such interventions are more effective in patients who are on a smaller amount of antipsychotics and less beneficial to those on high doses or polypharmacy. 47 The cognitive effects of the medication have been attributed to several mechanisms. Anticholinergic add-on drugs and antipsychotic medication with significant anticholinergic properties inhibit postsynaptic muscarinic receptors concentrated in the prefrontal cortex and hippocampus, areas thought to be concerned with EF and memory. A second mechanism postulated is the antipsychotic related dopamine receptor blockade, which, in addition to the beneficial effects on the positive symptoms of schizophrenia, may contribute to impaired cognition. 48 It has also been suggested that cognitive impairment in schizophrenia may be related to the metabolic comorbidity that is seen with the use of atypical antipsychotics. 44 The discontinuation of anticholinergic agents, as well as a reduction to the lowest effective dose of the antipsychotic drug, is recommended to reduce adverse effects, including the cognitive effects attributable to the medication.49, 50 The results of this study reiterate the findings of Rehse et al. that care should be taken in the prescription of antipsychotic agents. While small positive effects on cognitive functions are seen with normal or lower doses of antipsychotics, higher doses and polypharmacy may be deleterious and magnify disease-related deficits, further interfering with the patient’s functional recovery. 45 Our results highlight the fact that antipsychotics can affect EF in a dose-dependent fashion and emphasizes the need to prescribe the lowest possible dose of medication to prevent or minimize such cognitive side effects.51, 52
The literature on the effects of ECT on cognitive functions in general and EFs in particular is limited. Most have shown that ECT improves several neurocognitive domains, without evidence of worsening of any cognitive functions.53, 54 Many reviews suggest that any cognitive adverse effects that may occur are short-lasting and rarely persistent. 55 However, a few studies have reported persistent memory loss after treatment 56 and lower scores on tests of phonetic verbal fluency, which was significantly associated with the number of ECT sessions. 57 Tielkes et al. reported impairment in learning verbal information and executive functioning in older patients given maintenance ECT over a year, though the global cognition remained stable. 58 We found ECT to be significantly associated with executive dysfunction, with no correlation with the time elapsed since the last ECT session. Our findings draw attention to the importance of making attempts to minimize cognitive side-effects of this very effective and useful treatment modality by practicing unilateral stimulation techniques and ultra-brief pulse stimulations.
There was no statistically significant relationship between EF and scores on the disability scale in the present study, similar to some earlier studies59, 60 and in contrast with others.61, 62 The lack of a relationship has been attributed to sociocultural aspects such as family support available in countries like India that serve as protective factors despite the patient’s cognitive impairments. 59
While the cross-sectional nature of this study precludes conclusions on the direction of causation, the results indicate an association between EFs and some sociodemographic and clinical factors. As this was an exploratory study with a view to investigate and identify potential relationships with EF, multiple correlations were studied, increasing the possibility of a type I error (false positives). Further studies are needed to confirm our results.
Future research should also include longitudinal studies to examine the impact of variations in sociodemographic and clinical factors on EFs. These preliminary findings, however, emphasize the need to individualize and tailor pharmacological management, cognitive remediation, and other psychosocial interventions, such as social skills training and supported employment, to the specific EF deficits identified.
The study was limited by the small sample size. While no patient with a clinical diagnosis of intellectual deficiency was included, formal assessment of the premorbid intelligence was not carried out. The effect of benzodiazepines and anticholinergics, which some patients were prescribed, was not controlled for. The strengths include the use of consecutive sampling, standard assessments, two independent assessors, and multivariate analysis to adjust for confounders.
Conclusion
The dose of antipsychotic medication, ECT, education, employment, and income are associated with EFs. Knowledge of the nature of EF deficits and the associated factors can help clinicians address the individual patient’s problems and needs in order to improve his or her ability to adapt and function in the community.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by a Grant from the Christian Medical College, Vellore.