
Abstract
Background:
About 10% of first-time strokes and 30% of recurrent strokes develop into post-stroke cognitive impairment and are severe when associated with post-stroke depression. We aimed to examined the association of depression and cognitive impairment in patients after a stroke in acute, subacute, or chronic phases.
Methods:
Cross-sectional data of CT/MRI brain-confirmed stroke patients was obtained after protocol approval by the ethics committee. Socio-demographic data, the Patient Health Questionnaire (PHQ9), the Addenbrooke Cognitive Examination (ACE3), and the Barthel Index for Activities of Daily Living were administered. Normality assumptions and frequencies with percentages were assessed for continuous data. One-way ANOVA for group comparisons and Spearman’s nonparametric correlation with matrix plot display were done.
Results:
Stroke patients (13 with acute, 8 each with chronic and recurrent) aged 46–80 years were recruited. Higher Barthel Index scores across all groups were seen. Mean PHQ9 scores were in the moderate depression range with no differences among groups. The mean (SD) ACE3 attention score in acute cerebrovascular accident (CVA), 13.62 (2.76), was significantly higher than in chronic CVA, 9.63 (5.50). ACE3 language score was 20.15 (3.72) in acute CVA and 14.75 (6.84) in chronic CVA. Significant negative correlations were seen in ACE3 Memory in acute –.56 and in chronic cases- Attention –.76, Memory –.79, Fluency –.76. All CVA groups had moderate depression. Chronic CVA impacts cognition associated with depression more than other groups.
Conclusion:
The study shows a need for the assessment of cognitive impairments and depression for CVAs even where activities of daily living were better.
All CVA groups had moderate depression. Chronic CVA impacts cognition associated with depression more than other groups. There is a need to educate people about early treatment for CVAs even where activities of daily living are better.Key Messages
Stroke is clinically defined as a focal neurologic deficit caused by a local disturbance in cerebral circulation either by obstruction of cerebral blood (ischemic stroke) or by a rupture to a vessel wall supplying blood to either the brain or the spinal cord (intracerebral hemorrhage or subarachnoid hemorrhage, respectively). 1 The damage caused by a stroke to the brain can lead to long-lasting problems. The most common neuropsychiatric problems that can affect people after a stroke are cognitive impairment, depression, anxiety, apathy, emotional outbursts, pathological laughing and crying, and fatigue. About 10% of patients with a first stroke and 30% of those with recurrent strokes develop post-stroke cognitive impairment PSCI. 3 Patients with post-stroke depression (PSD) have a much greater degree of cognitive impairment than those without depression.
The time after a stroke is often divided into phases: the first 24 hours are the hyperacute phase, the first seven days are the acute phase, the first three months are the early subacute phase, the first 4–6 months are the late subacute phase, and from 6 months on, it is the chronic phase. 2 Recovery-related processes in post-stroke are time dependent in most cases.
Global studies have shown that cognitive impairments are common after a stroke. Common PSCI impairments are decreased processing speed, dysexecutive symptoms, and decreased memory. 4 Vascular dementia can also develop within one year of stroke onset. It is seen that patients with PSD have a much greater degree of cognitive impairment than stroke patients without depression. 5 A meta-analysis of prevalence studies showed that PSD will affect nearly a third of stroke patients throughout their course of recovery.6-8 Several studies have found that PSD is independently associated with greater disability, dependency, and poorer quality of life.9-12 Suicide ideation and potential contribute to the increased mortality risk in patients with PSD in approximately 12% of stroke survivors’ experience, according to a recent meta-analysis of 10,400 subjects. 13 Current or previous depression increases the odds of suicidal ideation by approximately 7- to 12-fold.
A systematic India review study has shown that crude stroke prevalence in different parts of India ranges from 44.29 to 559/100,000 people. 14 In a prospective study in India, the prevalence of cognitive impairment was nearly 20% among total stroke survivors. 15 Chaurasia et al. reported that 72% of 50 stroke patients had cognitive decline. 16 Jana et al. reported that the mean time to develop depression after stroke was 28.34 months. 17 Indian studies on the prevalence of depression show results like that in the West.18,19 With a relative dearth of Indian studies, it is important to examine the association of cognition and depression after a stroke, which forms the need for the study.
This cross-sectional study aimed to examine the association and comparison of depression and cognitive impairment in patients after a stroke in acute, subacute, and chronic groups.
Methods
Data was gathered from 30 male and female patients diagnosed with stroke from medical and psychiatry units at a tertiary hospital. Patients who fit the eligibility criteria and gave consent to participate were included in the study, which was approved by the Institutional Ethics Committee.
Eligibility
Inclusion criteria were as follows: (a) Patients diagnosed with cortical or subcortical strokes by the physician, (b) ischemic or hemorrhagic strokes involving the internal carotid artery and its branches (anterior, middle, and posterior branches) or vertebra-cerebellar territory, (c) evidence of stroke on CT scan or MRI of the brain, (d) patients aged between 46 and 80 years, (e) both males and females, (f) patients who gave written informed consent to participate in the study, (g) no previous history of severe mental illness, and (h) ability to understand the question and be willing to answer all the questions.
Exclusion criteria were as follows: (a) Patients with significant head trauma, intracranial neoplasm, AVM, and aneurysms; (b) patients with rapidly evolving stroke symptoms; (c) previous history of severe mental illness; (d) patients who could not answer proforma due to their psychiatric or medical conditions, and (e) aphasia patients.
Instruments
Socio-demographic data capture was done using a self-designed proforma with stroke-related details, socio-demographic details as on the Kuppuswamy Scale updated for 2019, Barthel Index for Activities of Daily Living, and instrumental activities of daily living. 20 DSM-5 criteria were used for the diagnosis of depressive disorders due to another medical condition. 21 Patient’s Health Questionnaire (PHQ9) was used to assess depression. 22 Addenbrooke’s Cognitive Examination Scale (ACE III) was utilized to assess for cognitive impairment. 23
Sample Size Calculation
Calculation of sample size was done on the Statulator software. 24 From the literature survey, the following are the prevalence rates:6,7 Depression in post-stroke is around 33% of the studies cited in the literature review.
P1 (depression) = 0.33; precision or margin of error = 0.10, power = 0.95; using the sample size estimation formula for one proportion, the total calculated sample is 30.
Statistical Analysis
Normality assumptions for continuous data were tested by looking at the homogeneity of variances, skewness, Q–Q plots, and Shapiro–Wilk test (Supplementary File). Frequencies with percentages were assessed for categorical variables. One-way ANOVA for group comparisons with LSD for post hoc comparisons and Spearman’s nonparametric correlation was done. A matrix plot was used for display. A significant P value was .05 or below.
Results
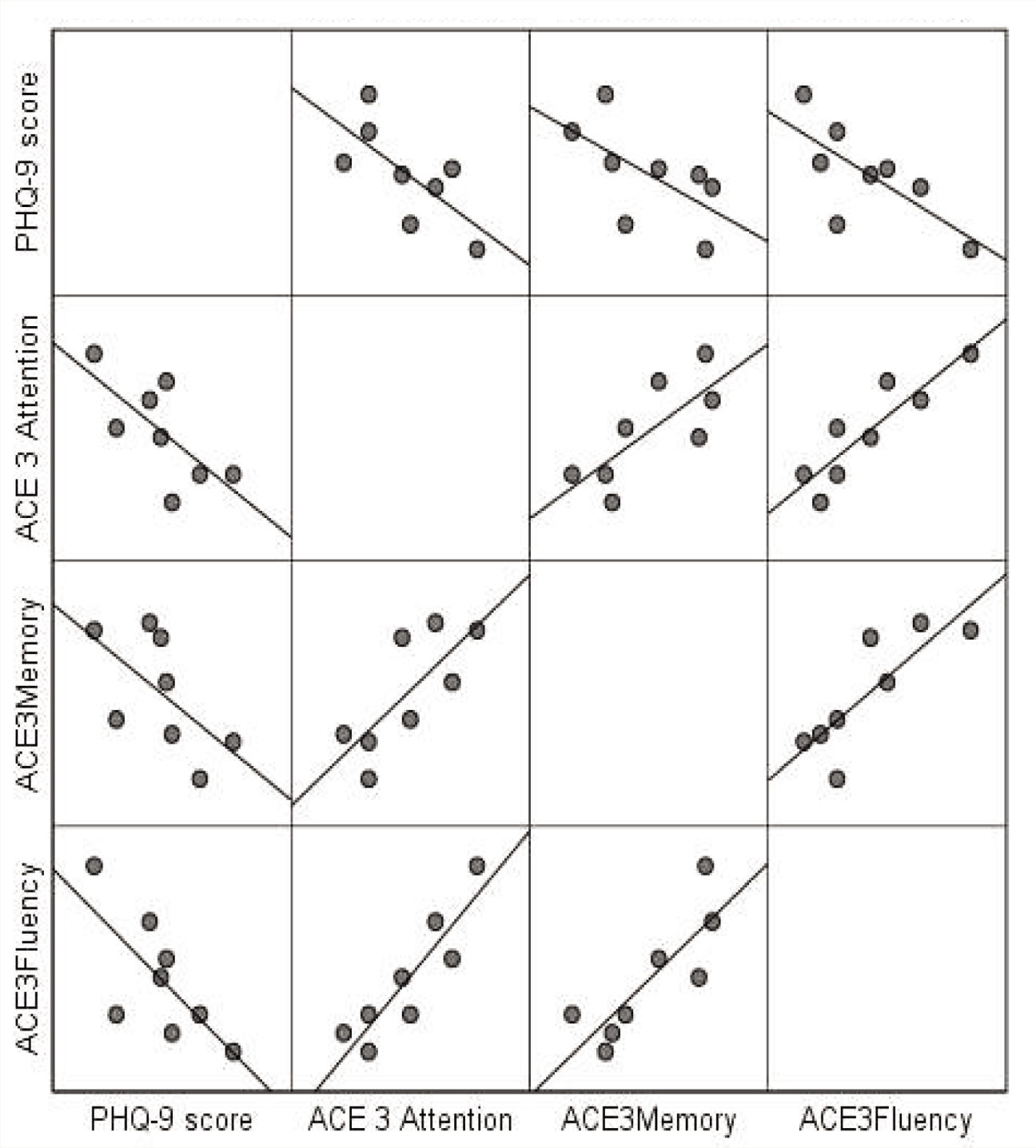
The number of subjects who could be recruited was 13 in acute and 8 each in chronic and recurrent cerebrovascular accident (CVA) groups. Higher Barthel Index scores across all groups showed better activity in daily living. Mean PHQ9 scores were in the moderate depression range with no differences among groups. The mean age group was matched across the groups, as depicted in Table 1. Components of ACE3 scores across types of CVAs are depicted in Table 2. The mean (SD) ACE3 attention score in acute CVA, 13.62 (2.76), was significantly higher than in chronic CVA, 9.63 (5.50). Similarly, ACE3 language score was 20.15 (3.72) in acute CVA and 14.75 (6.84) in chronic CVA. ACE3 memory was 16.92 (6.11) in acute CVA and 12.50 (7.91) in chronic CVA. ACE3 visuospatial was 9.15 (5.16) in acute CVA and 5.50 (5.60) in chronic CVA. ACE3 fluency was 4.85 (1.62) in acute CVA and 3.88 (3.35) in chronic CVA. We performed Spearman’s nonparametric correlation among the PHQ9 and ACE3 components, including all 30 cases. It was seen that there was a significant negative correlation between PHQ9 and ACE3 memory (−0.45 and P value .015), ACE3 fluency (−0.40 and P value .18), and ACE3 language (−0.36 and P value .05). Correlations in each of the categories of CVAs are depicted in Tables 3, 4, and 5. Table 3 depicts cognitive associates in patients with acute CVA. A significant correlation exists between higher depressive rates and attention, memory, fluency, language, and visuospatial deficits. A significant correlation is found between fluency, language, visuospatial deficits, and cognitive deficits. Table 4 depicts a significant correlation in patients with chronic CVA between higher depressive rates and cognitive deficits in the areas of attention, memory, fluency, and visuospatial deficits. A significant correlation is found between language deficits and memory, fluency, and visuospatial deficits. Furthermore, a significant correlation is found between visuospatial deficits and attention, memory, fluency, and language deficits. Figure 1 depicts a matrix scatterplot of the variables in the chronic CVA group with their best-fit lines. There are few outliers, and the directions of correlations, as described in Tables 3, 4, and 5, can be visualized. Significant negative correlations were seen in ACE3 memory in acute (−0.56) and chronic cases: attention, −0.76; memory, −0.79, and fluency −0.76. Table 5 depicts a significant correlation in patients with recurrent CVA between memory deficits and language and visuospatial deficits.
Depiction of Age, Barthel Index Score, and PHQ9 Across Types of CVAs.
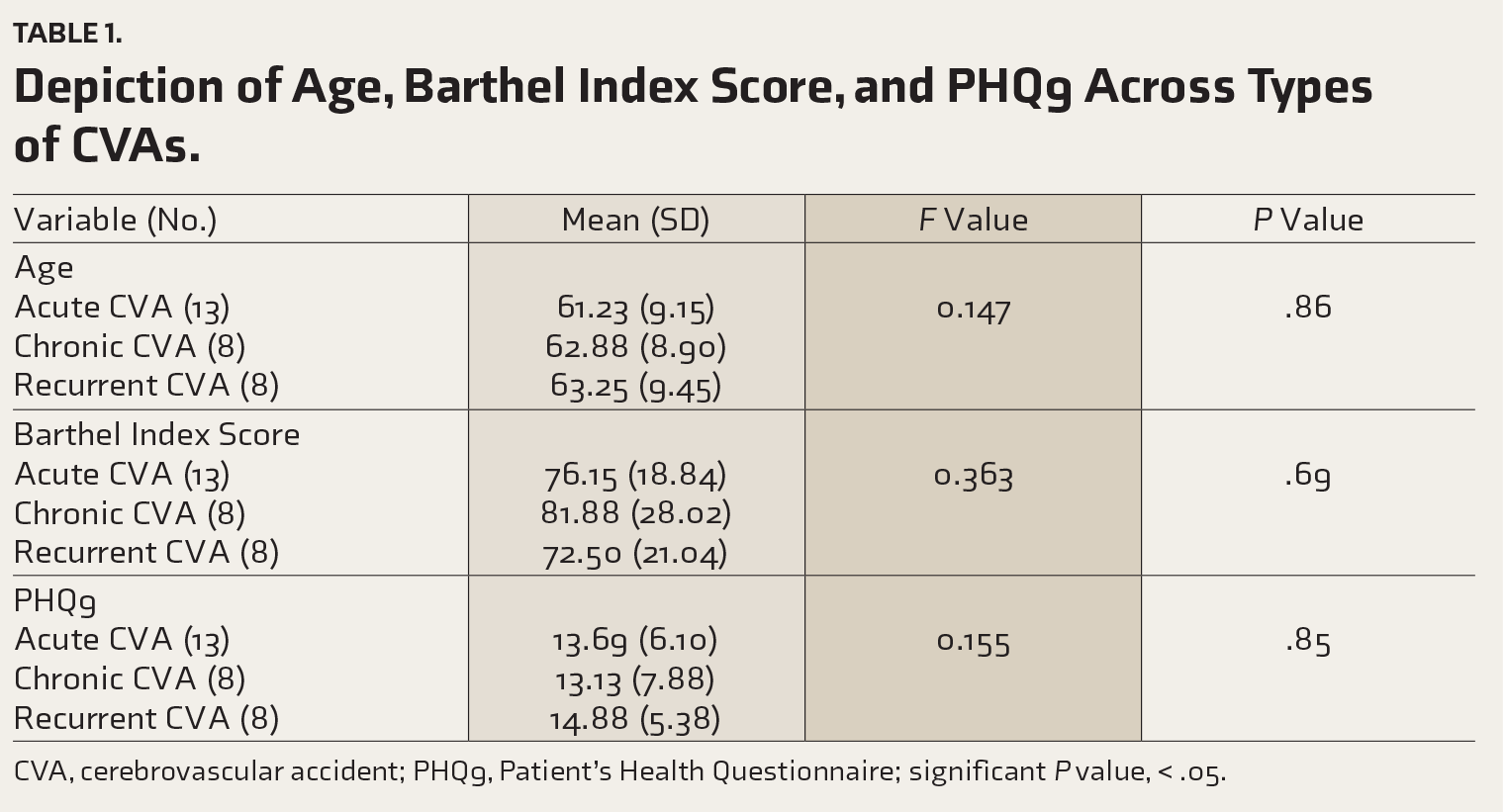
CVA, cerebrovascular accident; PHQ9, Patient’s Health Questionnaire; significant P value, < .05.
Depiction of Components of ACE3 Scores Across Types of CVAs.
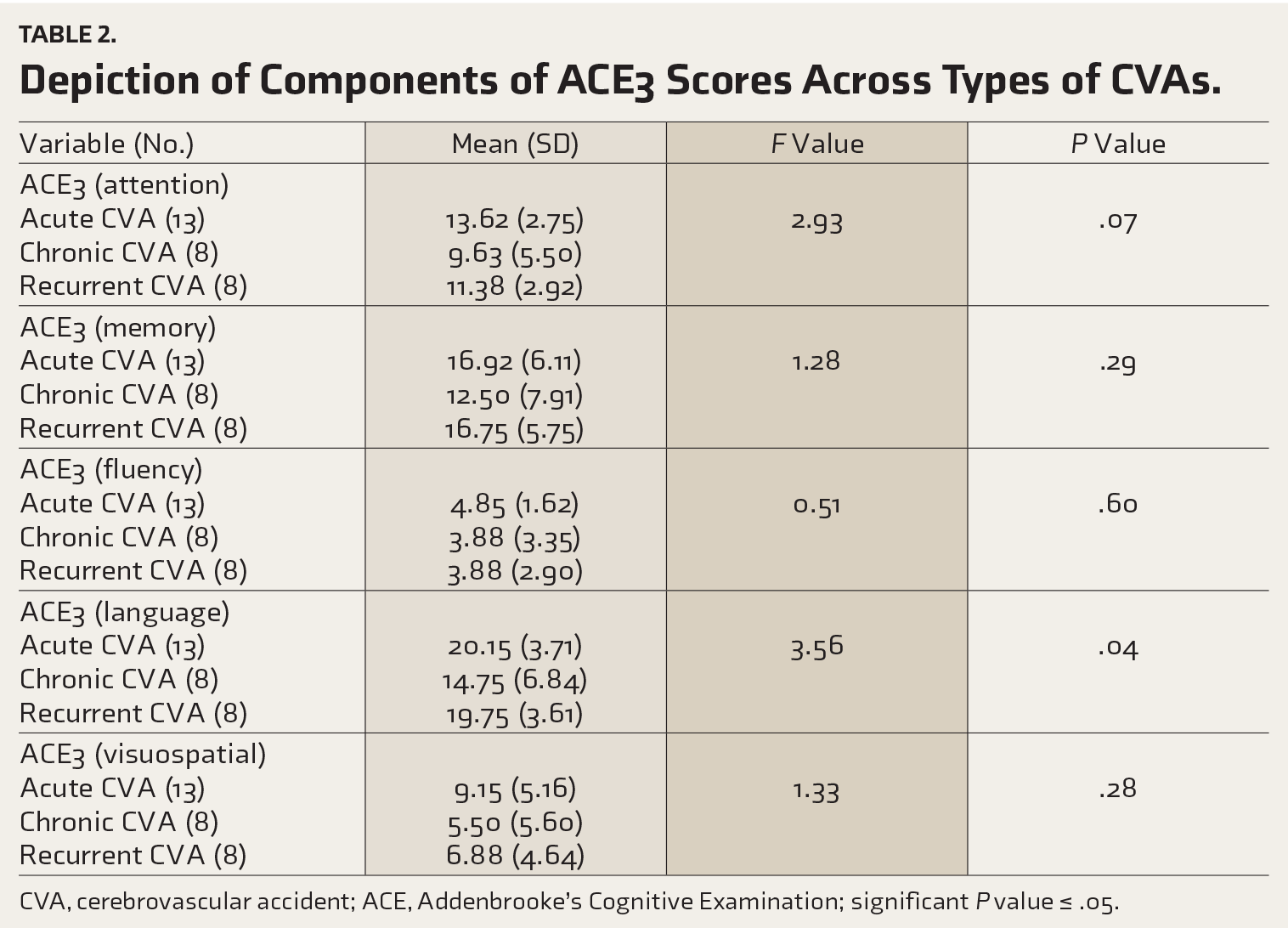
CVA, cerebrovascular accident; ACE, Addenbrooke’s Cognitive Examination; significant P value ≤ .05.
Nonparametric Correlations in Acute CVA (
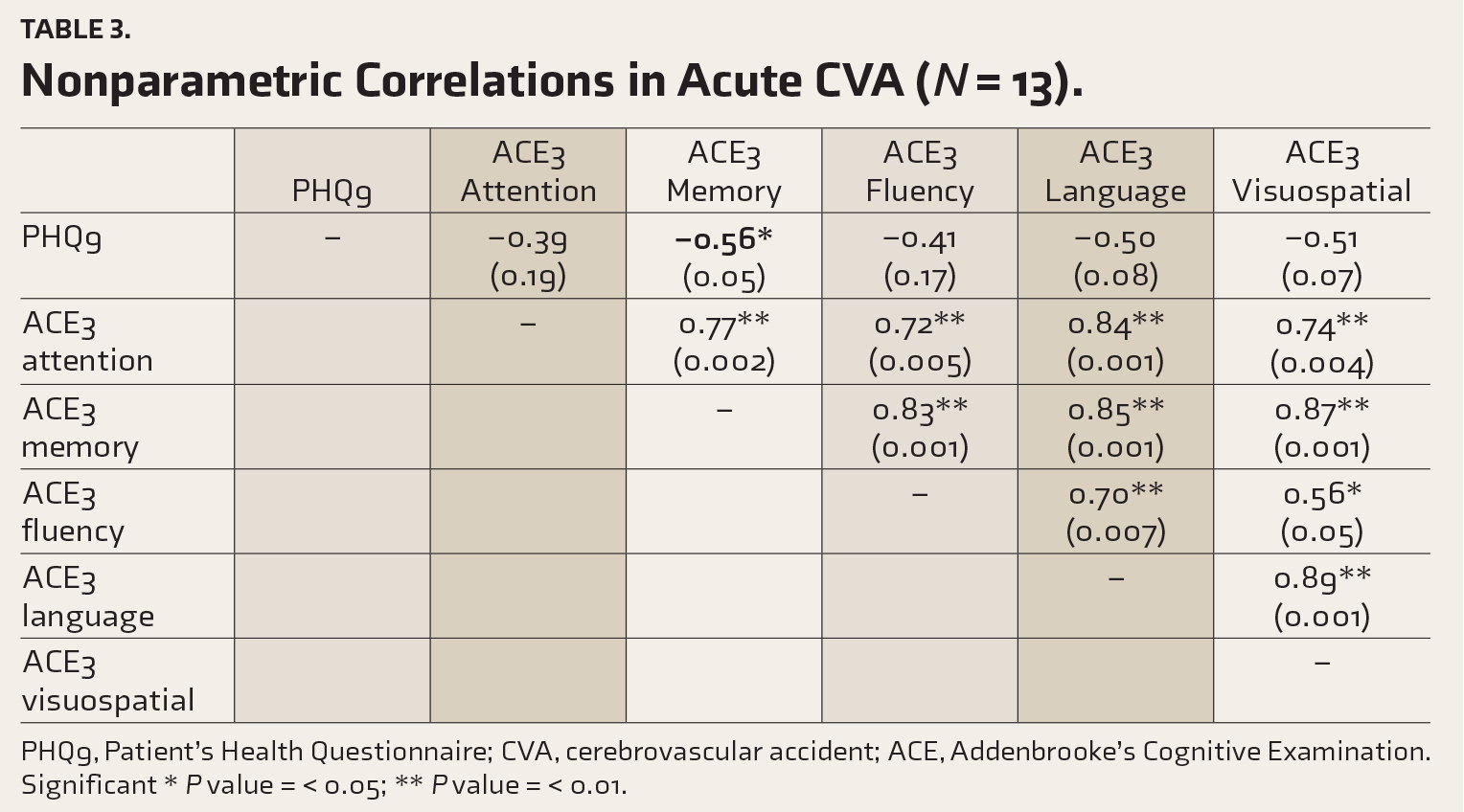
PHQ9, Patient’s Health Questionnaire; CVA, cerebrovascular accident; ACE, Addenbrooke’s Cognitive Examination.
Significant * P value = < 0.05; ** P value = < 0.01.
Nonparametric Correlations in Chronic CVA (
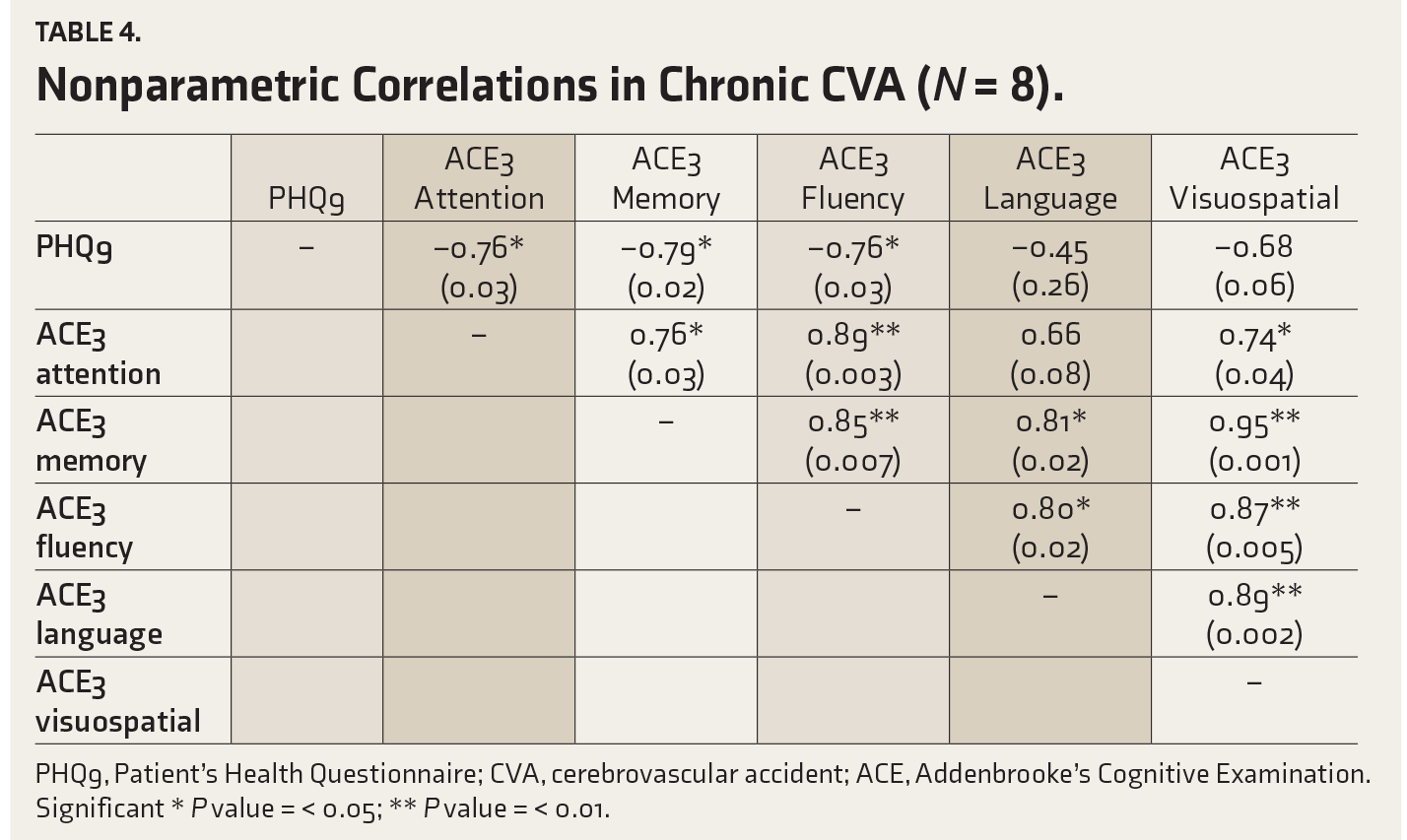
PHQ9, Patient’s Health Questionnaire; CVA, cerebrovascular accident; ACE, Addenbrooke’s Cognitive Examination.
Significant * P value = < 0.05; ** P value = < 0.01.
Nonparametric Correlations in Recurrent CVA (
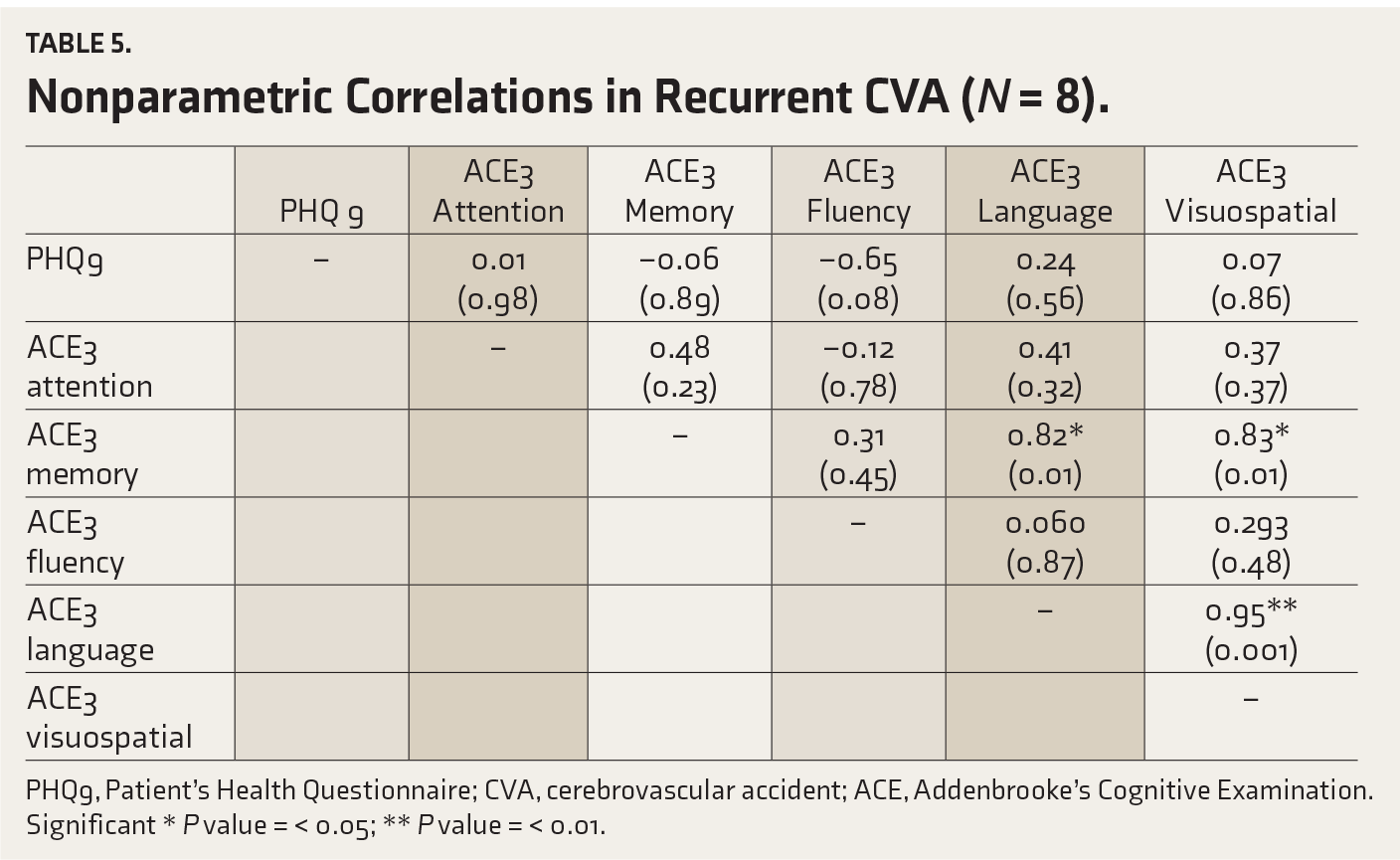
PHQ9, Patient’s Health Questionnaire; CVA, cerebrovascular accident; ACE, Addenbrooke’s Cognitive Examination.
Significant * P value = < 0.05; ** P value = < 0.01.
PHQ9, Patient Health Questionnaire; ACE3, Addenbrooke’s Cognitive Examination.
Discussion
Our study found no statistically significant differences among the three post-stroke groups in Barthel Index scores. All three groups had better daily activities. In a review of studies, Kutlubaev et al. found that depression was associated with poor functional outcomes in six of eight studies, while there was no such association in the other two. 9
Mean PHQ9 scores were in the moderate depression range with no differences among groups. Hackett et al.’s study showed that following a stroke, depression between one and five years was seen in 25% cases. 6 Ayerbe et al. found that PSD was present in 29% cases and remained stable up to 10 years after stroke. 7 As per Jana et al., PSD was seen in 38.73% cases. 16
Pohjasvaara et al., in a large group of post-stroke cases, identified depression on Beck’s Depression Inventory in 43.9% and 44.6% cases, respectively, at 3- and 15-month follow-ups. Major depression more often had poor functional outcomes at 15 months. Poor functional outcome at three months also correlated with depression at 15 months. 11
In our study, in acute and chronic CVAs, a significant correlation was found between higher depressive rates and deficits in memory, attention, fluency, language, and visuospatial areas. In recurrent CVA, a significant correlation was found between memory, language, and visuospatial deficits. The level of significance in the correlation between cognitive deficits and higher depression in a descending order was chronic CVA, acute CVA, and recurrent CVA. Kang et al. reported a mutually negative relationship between cognition and depression. Also, they found statistically significant predictors of post-stroke cognition as chronic and emergent depression. 25
Kapoor et al. reported that depression and cognitive impairment were independent predictors of impaired higher-level functioning and community reintegration 2–3 years after stroke. 26 Blomgren reported cognitive dysfunction and depressive symptoms in stroke survivors even when neurological deficits were mild or absent. These deficits associated with fatigue negatively impact the performance of instrumental activities of daily living (IADL) even seven years after the stroke onset. 27 Arunima reported that nearly 50% of stroke patients, even with good functional recovery, continued to have cognitive impairment, and 33% had depression 2–3 years later. 28 Medeiros et al., in a metanalysis, found that large and multiple strokes with greater neurological tissue loss were predictive of higher frequencies of PSD. PSD rates were high in the first three months after the vascular event, with the odds ratio up to eight. 29
Limitations of the Study
A cohort study comparing the variables on repeated measures would give a better picture of the changes.
Conclusion
Our study showed that depression and cognitive impairments were prominent in the chronic CVA group even when the activities of daily living were better. Acute and recurrent CVA groups also had these impairments. There is a need to regularly assess for depression and cognition in CVA in all phases. Regular cognitive and mental status examinations of CVA patients in hospitals and follow-ups, especially in functional deterioration, could lead to better management of CVA patients.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We thank the nursing staff for their help while recruiting the participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Ethical approval was obtained by the Institutional Ethics Committee, Malla Reddy Institute of Medical Sciences, Suraram, Hyderabad (approval no: MRIMS/DHR-IEC-822022 dated November 3, 2022).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from participants of this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.