
Abstract
Background:
Adolescents’ mental health is influenced by childhood trauma, emotional regulation, and psychological symptoms. This study aimed to explore these interconnections among adolescents attending a child and adolescent clinic.
Method:
Adolescents aged 13-19 from a city were recruited through purposive sampling. Data were collected using the Child Behavior Checklist (CBCL), Childhood Trauma Questionnaire-Short Form (CTQ), Difficulties in Emotion Regulation Scale (DERS), and Toronto Alexithymia Scale-20. Adolescents with severe mental or physical illnesses were excluded.
Results:
A total of 100 participants were recruited aged 13-19. The CTQ scores positively correlated with DERS Scores (r = 0.246, P < .05) and Internalizing scores (r = 0.325, P < .01). DERS Scores strongly correlated with alexithymia (r = 0.624, P < .001) and Internalizing scores(r = 0.556, P < .001). Regression analyses revealed CTQ, Alexithymia, and DERS scores significantly predicted Internalizing scores (R2 = 0.37). Mediation analysis showed that emotional regulation partially mediated the relationship between child trauma and Internalizing scores (B = 0.059, 95% confidence interval [CI] = 0.011 to 0.133, t = 1.92, P = .01), as well as the relationship between Alexithymia and Internalizing scores(B = 0.255, 95% CI = 0.129 to 0.465, t = 3.31, P < .001).
Conclusion:
Findings highlight the importance of emotional regulation as a mediator in the connections between childhood trauma, alexithymia, and psychological symptoms among adolescents. This complementary mediation underscores the dual impact of direct and indirect effects on psychological well-being. The findings reveal intricate links between childhood trauma, emotional regulation, and alexithymia in adolescents with psychological symptoms. Emotional regulation proved to have a pivotal role in influencing psychological well-being. These results emphasize the importance of considering emotional regulation when assessing and maintaining mental health in adolescents, further contributing to understanding treatment needs.
Keywords
There is a complex relationship among emotional control, early trauma, and alexithymia in teenagers exhibiting psychiatric symptoms. A transdiagnostic approach focusing on emotional regulation strategies can be utilized to mitigate the effect of trauma. There is a need to take emotional regulation into account when evaluating and maintaining teenage mental health.Key Messages:
Childhood trauma is a major public health problem with significant consequences for mental and physical health. It is estimated that 1 in 6 children worldwide experience some form of physical, sexual, or emotional abuse or neglect before the age of 18. 1 Adolescents who experience childhood trauma are at increased risk for developing a range of psychological symptoms, including depression, anxiety, post-traumatic stress disorder (PTSD), and substance use disorders. 2 One way that childhood trauma can impact psychological symptoms is through its impact on emotional regulation. Trauma can disrupt the development of the brain’s emotion regulation system, making it difficult for adolescents to identify, understand, and manage their emotions. It Is also evidenced that for adolescents who are at risk of developing mental disorders and emotional problems, factors like childhood trauma increase the susceptibility to psychiatric disorders.3-5 Estimates of around 30% of emotional issues have been attributed to childhood trauma. 6 This effect of childhood trauma on mental health can last till adulthood. 7
Alexithymia is another critical concept that falls under how individuals experience and express their emotions. Adolescents with alexithymia may have difficulty understanding their feelings, making it difficult to regulate them effectively. Alexithymia, a difficulty identifying and describing one’s own emotions, is another important factor that may mediate the relationship between childhood trauma and psychological symptoms in adolescents. Alexithymia is relatively common in adolescents, with prevalence rates ranging from 10% to 20%.8,9 Many factors such as childhood family environment, 10 early childhood experiences including norms in the family defining how emotions need to be expressed 11 ; emotional abuse and neglect, specifically emotional maltreatment in terms of belittling, blaming, or rejecting 12 ; emotional problems with caregivers during childhood 13 ; improper living conditions in childhood including a broken childhood home 14 or disrupted family structure 15 have been traced in the development of Alexithymia traits. Among adolescents, alexithymia has been linked with psychological symptoms, including depression, 16 heightened sensitivity to emotional difficulties and conflicts,17,18 and a reduced level of health-related quality of life 19 , anxiety, and internalizing problems. 20
Research has shown that alexithymia is a risk factor for developing psychological symptoms in adolescents, particularly in the context of childhood trauma. For example, one study found that adolescents with alexithymia who had experienced childhood trauma were more likely to develop PTSD and depression than adolescents without alexithymia. 21 Another study found that alexithymia mediated the relationship between childhood trauma and self-harm in adolescents. 22
Childhood trauma, on the other hand, can be viewed as a crucial risk factor in adolescents with emotional regulating difficulties. There is a growing body of research that shows a strong relationship between childhood trauma, emotional regulation, alexithymia, and psychological symptoms in adolescents. It is seen that adolescents who had experienced childhood trauma were more likely to have difficulty regulating their emotions and to experience psychological symptoms such as anxiety, depression, and PTSD. 23 It is also seen that adolescents who had experienced childhood trauma were more likely to have alexithymia.24-26
Despite the growing body of research on the relationship between childhood trauma, emotional regulation, alexithymia, and psychological symptoms in adolescents, there are still some gaps in the literature. One gap is that most research has been conducted on cross-sectional samples. This means that it is difficult to determine the direction of causality. For example, childhood trauma may lead to emotional regulation difficulties and alexithymia, which then leads to psychological symptoms. To the best of our knowledge, there is no Indian study in the published literature that explored the interaction of these variables and understands the predictors or contributors to psychological distress, especially in the context of Indian adolescents. This study was aimed at understanding the mediational pathway to examine the causal processes that led to psychological problems in adolescents with a history of trauma. This led to the development of a theoretical paradigm that states that emotional dysregulation brought on by childhood trauma is linked to alexithymia. 27 In turn, alexithymia may be connected to the intensity of psychological symptoms. To the best of our knowledge, teenagers in India have not had this model thoroughly studied. To our knowledge, this model has not been investigated systematically among adolescents in India.
Moreover, studying mental health in Indian adolescents necessitates a culturally sensitive approach due to unique emotional expressions, the potential for specific traumas (if any), and the influence of cultural factors. The emotional expressions may differ in Indian adolescents, and there might be a social stigma or discouragement of openly expressing emotions, which could further complicate emotional regulation and contribute to alexithymia. While existing research supports this connection, more studies are needed to explore the specific nuances in the Indian context.
Methods
We theorize that emotional regulation may play a mediating role in the relationships between the independent variables (childhood trauma, emotional regulation, and alexithymia) and the dependent variable (psychological symptoms).
Participants
All adolescents aged between 13 and 19 years and attending the child and adolescent services were approached. Adolescents with neurodevelopmental disorders, mental retardation, or any chronic physical illness that may have affected the normal developmental course or inflated distress, any severe mental illness or physical illness interfering with the ability to give assent, or parent’s ability to provide consent were excluded from the current study. All adolescents visiting the clinical psychology services were screened irrespective of the diagnosis (except exclusion) or disorder severity since the main aim was to understand how the variables interact.
Purposive sampling was adopted to recruit patients based on the availability and accessibility of subjects over the continuous duration of 3 months. A previous study 28 from a tier 2 city in the northern part of India reported a large proportion of the sample with childhood abuse or neglect (83.36%) and experienced symptoms of one or more psychiatric disorders (83.33%). However, no such prevalence data are available from [Blinded for review].
Material
Socio-demographic proforma and Clinical data were collected for each participant. Child Behavior Checklist (CBCL- youth self-report measure) 29 included 113 items with a three-point Likert-scale response format that can be summarized into three scales: Internalizing, Externalizing, and Total Problems scales utilized for the study. Test-retest reliability ranges from 0.95 to 1.00, and Cronbach alpha (a) = 0.95. On CBCL, both borderline and clinical ranges were considered for analysis. Childhood Trauma Questionnaire – Short Form (CTQ) 30 was used to assess the extent to which adolescents experienced abuse (emotional, physical, and sexual) as well as neglect (emotional and physical) in the past using a Likert scale: 1 = never true to 5 = very often true. Cronbach alpha is 0.852. Reliability coefficients for subscales range from 0.61 to 0.95. The Difficulties in Emotion Regulation Scale (DERS) 31 is a commonly used self-report measure of subjective emotion ability. It has good internal consistency (Cronbach α = 0.93) and test re-test reliability. Toronto Alexithymia Scale-20 32 was used to measure adolescents’ difficulties in identifying (DIF) and describing feelings (DDF) as well as externally oriented thinking (EOT) using a Likert scale. It has a Cronbach alpha of 0.81 and a test-retest reliability of 0.77, which is at P ≤ .01. It is recommended to be a good measure to tap deficits in affect awareness and expression and operational thinking.
Procedure and Ethical Considerations
The study was approved by the institutional ethics committee where it was undertaken (Proposal No: XXXX). A team of mental health professionals, including a psychiatrist and clinical psychologist, diagnosed the adolescents and screened them for the study. The researchers explained the aims and procedure of the research to the selected participants and sought assent and consent from both participants and parents. They were informed about the anonymity and their right to withdraw from the study, which will not imply their treatment as usual. Adolescents presented with the risk of harming themselves or others during the interview were provided with immediate crisis support by the trained professional embedded within the facility through appropriate referral. The study followed all the principles laid down in the Helsinki Declaration.
Statistical Analysis
The demographic characteristics of adolescents will be described using descriptive statistics. For data analysis, R 33 was used for correlation, regression, and mediational using the Hayes Macro Process plugin. 34
Results
To ensure that the assumptions of normality were not violated, preliminary analyses were conducted using the Kolmogorov–Smirnov statistic, which was non-significant for all variables except CTQ Scores. The multivariate normality assumption was addressed in the mediation analysis using bootstrapping, thus increasing the accuracy of the conclusions drawn from this research. Multicollinearity was acceptable after conducting collinearity diagnostics (tolerance values >.2, and variance inflation factors values <10). We recruited 100 adolescents aged 13 to 19 years, with 30% of the participants aged between 13 and 15 years and the remaining 70% aged between 16 and 19 (Table 1). Regarding gender, the sample was reasonably balanced, with 45% identifying as male and 55% as female. From our sample, 35% of the participants had a middle school education or below, while the remaining 65% had a senior school education or above. Half (51%) of the participants were from lower-income families, 30% from middle-income families, and only 19% from upper-income families. Most (82%) lived with both parents, while 18% of the sample lived with one parent. The participants’ residence was distributed across rural (30%), semi-urban (23%), and urban (47%) areas. Only 17% reported having no siblings, while the rest of the respondents had either one sibling or more, with 29% reported having three or more siblings. Half of the participants were the eldest in their family (57%), followed by those in the middle (29%) and the youngest (14%). Twelve (12%) of the participants reported a family history of psychiatric illness, and a quarter (26%) had a lifetime history of psychiatric illness. 26% of the participants were undergoing treatment for psychiatric illness. However, most participants had sub-syndromal or subclinical presentations for which they were referred for therapy. Finally, 11% of the participants were screened to have a risk for suicide.
Socio-demographic and Clinical Profile.
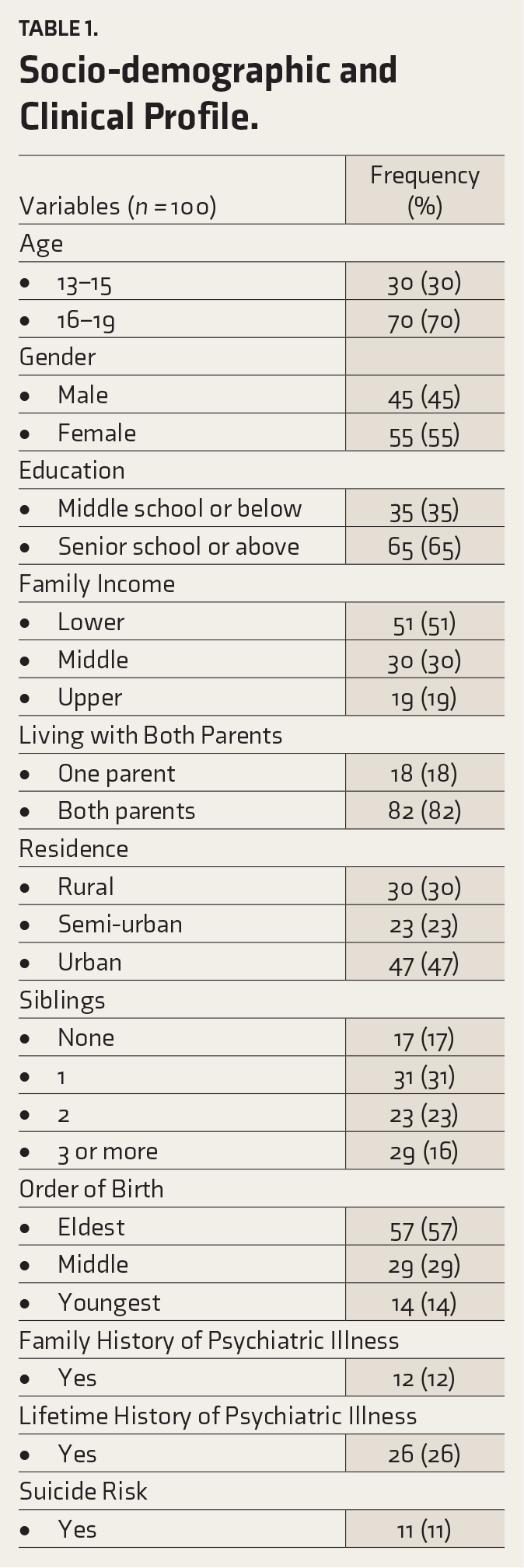
Table 2 presents the descriptive statistics and correlations among Internalizing score, Child Trauma Questionnaire (CTQ) total score, Difficulties in Emotion Regulation Scale (DERS) total score, and alexithymia total score for 100 participants. The mean Internalizing score was 74.1 ± 7.8. This variable showed significant positive correlations with CTQ total score (r = 0.325, P < .01), DERS total score (r = 0.556, P < .001), and alexithymia total score (r = 0.491, P < .001). The mean CTQ total score was 56.3 ± 16.4. Besides its correlation with the Internalizing score, the CTQ total score also showed a significant positive correlation with the DERS total score (r = 0.246, P < .05) but no significant correlation with the Alexithymia total score (r = 0.044, P > .05). The mean DERS total score was 104.3 ± 24.6. In addition to its correlations with the Internalizing score and the CTQ total score, the DERS total score showed a strong positive correlation with the Alexithymia total score (r = 0.624, P < .001). Finally, the mean Alexithymia total score was 18.5 ± 7.1. Besides its correlations with the other variables, no other significant correlations were reported for this variable. These results suggest that higher scores on child trauma (CTQ) measures, difficulties in emotion regulation (DERS), and alexithymia are associated with higher Internalizing scores. Furthermore, difficulties in emotion regulation (DERS) are associated with both child trauma (CTQ) and alexithymia, while child trauma and alexithymia are not associated.
Descriptive Statistics and Correlation.
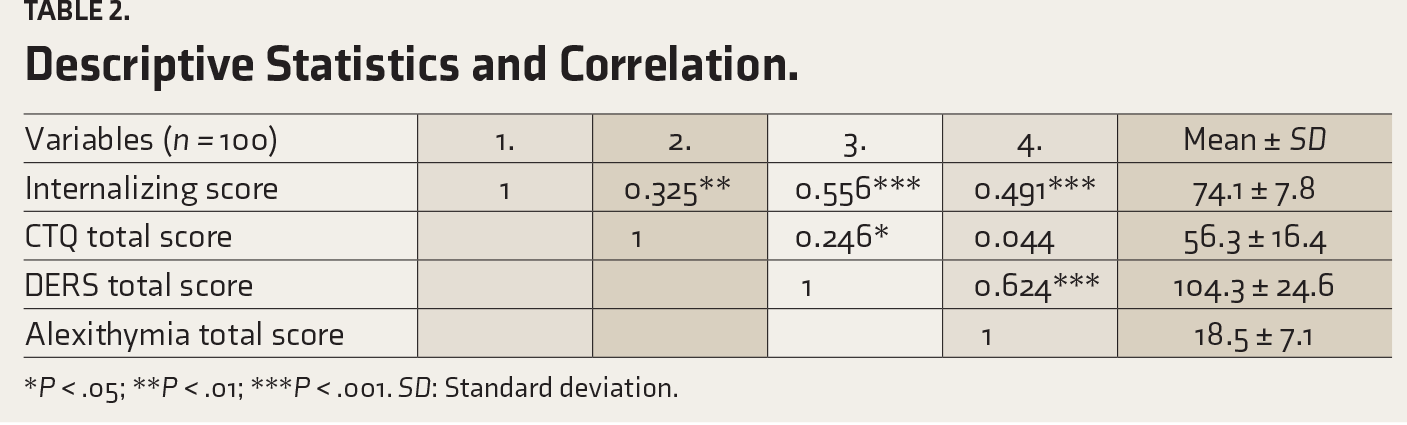
*P < .05; **P < .01; ***P < .001. SD: Standard deviation.
Table 3 displays the unstandardized regression coefficients (β), unstandardized standard error of the regression coefficients (SE B), and the standardized regression coefficients (β), R2, and F for change in R2 for the prediction of Internalizing scores based on three models with different variables. In Model 1, the CTQ total score was the only variable, accounting for a significant proportion (30%) of the variance in Internalizing scores (β = 0.56, B = 0.18, SE B = 0.04, P < .001). Model 2 included the Alexithymia total score and CTQ total score, explaining 33% of the variance, a significant increase compared to Model 1 (F Change = 5.6, P = .02). Here, CTQ total score remained a significant predictor of Internalizing scores (β = 0.51, B = 0.16, SE B = 0.03, P < .001), and the addition of the Alexithymia total score contributed significantly to the model (β = 0.20, B = 0.10, SE B = 0.04, P = .02). Model 3 incorporated the CTQ total score, Alexithymia total score, and Difficulties in Emotion Regulation Scale (DERS) total score. All three variables significantly predicted Internalizing scores: DERS total (β = 0.33, B = 0.10, SE B = 0.03, P = .003), Alexithymia total (β = 0.23, B = 0.11, SE B = 0.04, P = .006) and CTQ total (β = 0.28, B = 0.31, SE B = 0.11, P = .008). This model accounted for 37% of the variance in Internalizing scores, and the increase in explained variance (Model 2 to Model 3) was significant (F Change = 7.25, P = .008). These results indicate that as we added more relevant predictors, the model’s ability to explain the variance in Internalizing scores improved, with all three variables (CTQ total, Alexithymia total, and DERS total) demonstrating significant predictive value in the final model. In Model 3 specifically, DERS showed the strongest association with Internalizing scores (β = 0.33), followed by alexithymia (β = 0.28), and then CTQ (β = 0.23). These findings suggest that DERS might be a significant mediator in the relationships of Alexithymia and CTQ with Internalizing scores.
Hierarchical multiple Regression Predicting Internalizing Scores.
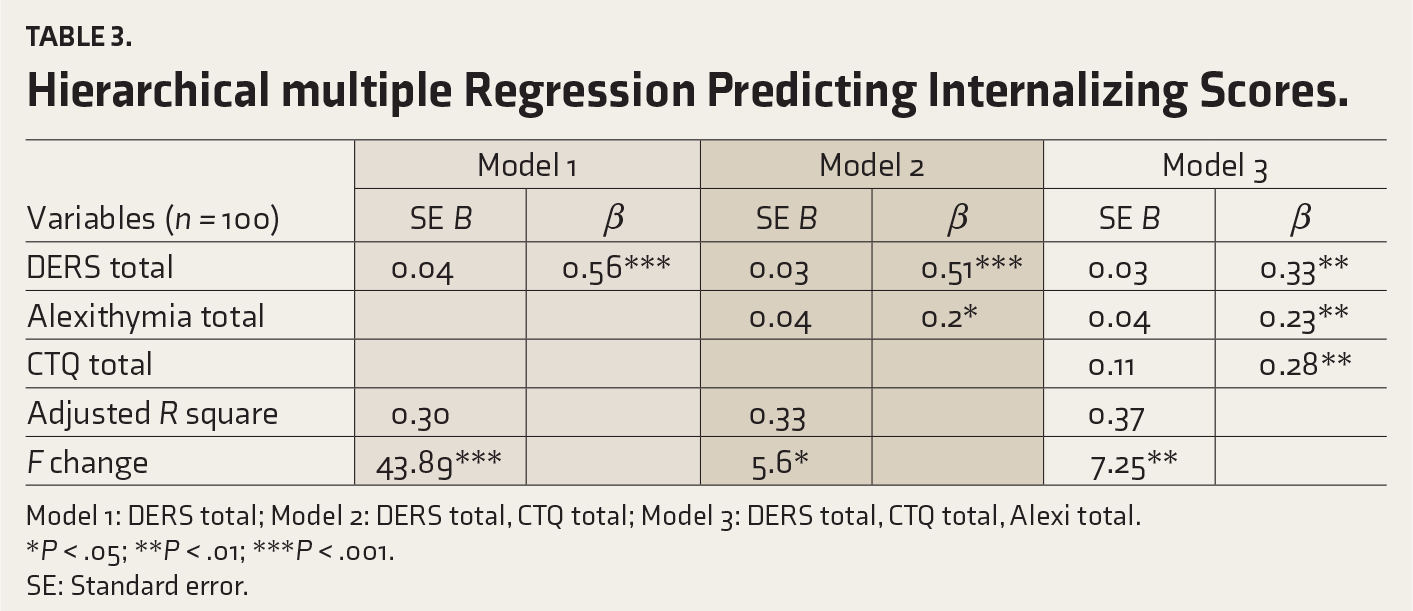
Model 1: DERS total; Model 2: DERS total, CTQ total; Model 3: DERS total, CTQ total, Alexi total.
*P < .05; **P < .01; ***P < .001.
SE: Standard error.
To check the mediating role of emotional regulation, we conducted mediation analysis using Hayes Process Macros 34 for R statistical package 33 with an indirect bootstrapping approach with 5000 sampling iterations and a 95% confidence interval (CI). We calculated the P value for indirect mediation using a separate calculator. 35 While performing multiple mediation analyses on the same sample, it is essential to consider whether the relationships between the variables in each model need to be theoretically justified and empirically supported. 36 Thus, separate mediation analyses with different mediators could be meaningful even when performed on the same sample, provided that the assumptions of mediation analysis are respected in each case and adequate theoretical justification for each model is given. The theoretical rationale has already been included in our literature review.
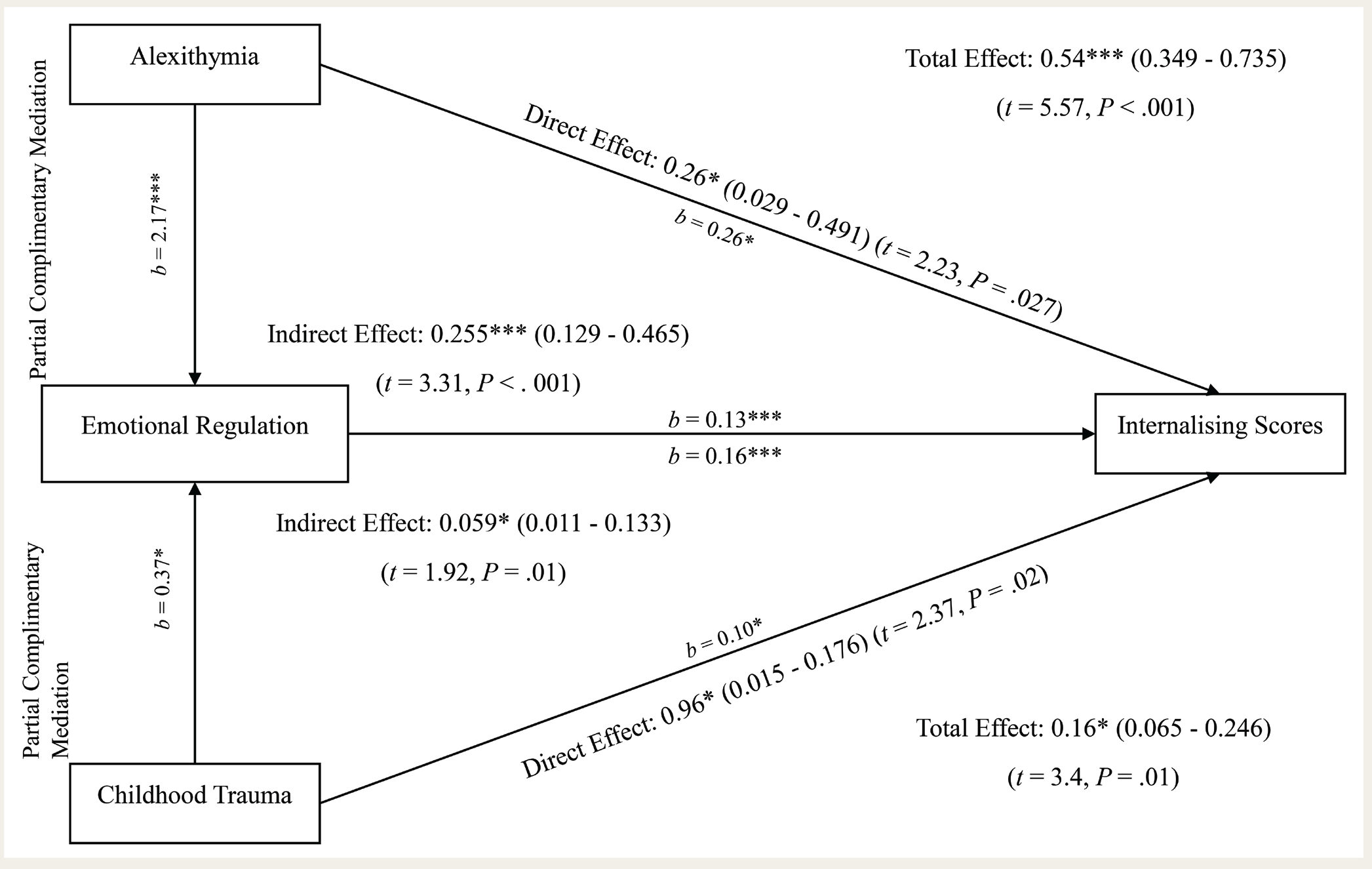
The results of the mediation analysis are summarized in Figure 1. In the first model, the total effect of Alexithymia scores on Internalizing scores was significant (B = 0.54, 95% confidence interval [CI] = 0.349 to 0.735, t = 5.57, P < .001). When DERS was included as a mediator, alexithymia maintained a significant direct effect on Internalizing scores (B = 0.26, 95% CI = 0.029 to 0.491, t = 2.23, P = .027). The indirect effect through DERS was also significant (B = 0.255, 95% CI = 0.129 to 0.465, t = 3.31, P < .001). This suggests that while alexithymia directly contributes to Internalizing scores, part of its impact is mediated by DERS. In the second model, the total effect of Childhood Trauma scores on Internalizing scores was significant (B = 0.16, 95% CI = 0.065 to 0.246, t = 3.4, P = .01). When DERS was included as a mediator, Childhood Trauma maintained a significant direct effect on Internalizing scores (B = 0.96, 95% CI = 0.015 to 0.176, t = 2.37, P = .02). The indirect effect through DERS was also significant (B = 0.059, 95% CI = 0.011 to 0.133, t = 1.92, P = .01). Like the first model, Childhood Trauma directly influences Internalizing scores, and DERS mediates part of this effect. These findings suggest that difficulties in emotion regulation play a significant role in partially mediating the relationship between Alexithymia and Childhood Trauma scores with Internalizing scores. This mediation is complementary 37 rather than competitive, that is, both the direct and indirect effects are significant, causing a change in the same direction.
Mediation Models with Emotional Regulation as Mediator for Alexithymia and Childhood Trauma (*P < .05; **P < .01; ***P < .001).
Discussion
Adolescence is a particularly vulnerable period for the development of mental health problems. Childhood trauma can further increase this vulnerability. One of the key ways in which childhood trauma can influence adolescent mental health is through its effect on emotional regulation. Children who experience trauma often have difficulty regulating their emotions, which can lead to a range of problems, including anxiety, depression, and anger outbursts. Another way in which childhood trauma can impact adolescent mental health is through its contribution to alexithymia. Adolescents with alexithymia may have difficulty understanding what they are feeling, which can make it difficult for them to cope with stress and adversity. 38
The present study examined the interrelationship between childhood trauma, emotional regulation, alexithymia, and psychological symptoms among adolescents attending special clinics. This study provides valuable insights into the complex relationships between various factors affecting adolescents’ psychological well-being. These findings open avenues for discussing the significance of emotional regulation as a mediator and the implications for understanding and addressing psychological symptoms in this population.
The demographic distribution is concurrent to the national demographics of adolescents with mental health problems with a similar distribution between males and females, higher in urban metro areas and risk for suicide.39,40 In the current study, it was seen that Internalizing scores positively correlated with childhood trauma, emotional dysregulation, and alexithymia scores. Numerous studies have demonstrated that children and adolescents with a history of trauma present with significantly higher(er) rates of Internalizing mental health issues, such as major depressive disorder, separation anxiety disorder, generalized anxiety disorder, panic disorder, and phobias.41-44 Similar to this, research has revealed links between alexithymia20,45,46 and a variety of mental health issues, such as generalized anxiety disorder and depression. In addition, it was observed in our sample that childhood trauma had a positive correlation with Emotional Dysregulation scores. This finding concurred with a meta-analysis of adolescents with a diagnosis of PTSD (post-traumatic stress disorder) who reported more emotion regulation difficulties than those who did not develop. 47 Similar measurements were used in another study that found that individuals with eating disorders have significantly greater rates of emotional dysregulation and childhood trauma than healthy controls. 48 We also observed that emotional dysregulation had a strong positive correlation with the Alexithymia scores. This is robustly supported by the literature, which shows a strong association between the two.49-51
In our study, childhood trauma had no significant correlation with the total score for alexithymia. Literature suggests different views, for example, in a study, it was seen that in the cases of PTSD and BPD (Borderline Personality Disorder), both independently contributed to higher alexithymia, and so did the severity of emotional and physical neglect. 24 On the contrary, our study is in line with the previous work, where alexithymia was weakly associated with emotional and physical neglect and did not have any relationship with emotional abuse. 52 Perhaps the types of abuse and its severity influence alexithymia, as already discussed by the authors earlier.
The results of Hierarchical multiple regression indicate that the model with all three variables, that is, childhood trauma, alexithymia, and emotional responsiveness, had the best predictive value of Internalizing behavior. In this model, emotional dysregulation had the strongest association with Internalizing scores, followed by alexithymia and then childhood trauma, which strongly suggested a pivotal role of emotional dysregulation with other variables. In the next phase, the mediation pathways were analyzed, and the two separate pathways hypothesized for the development of Internalizing problems were tested. One where alexithymia had a significant direct effect on Internalizing scores and another where childhood trauma directly influenced it. Both pathways had significant indirect effects mediated by emotional dysregulation. While alexithymia and childhood trauma directly contribute to Internalizing scores, part of their impact is also mediated by emotional dysregulation. These findings suggest that difficulties in emotion regulation play an important role in shaping an adolescent’s behavior. Various studies have proposed different models of associations between these variables. These findings align with our hypothesis and with numerous studies showing emotional dysregulation as a vulnerability underlying risk for Internalizing problems. According to a study, emotion dysregulation has a significant indirect relationship between psychopathology and childhood maltreatment, and the degree of the relationship increases with elevated alexithymia levels. 52 In an 800 school adolescents sample from China, structural equation modeling showed that alexithymia was connected with emotional processing issues, which were correlated with child maltreatment. 53 Alexithymia, in turn, was related to how severe the psychiatric symptoms were. The authors concluded that psychological health can be impacted by child maltreatment, but the link depends on how much processing difficult emotions and connecting with inner feelings is avoided. Previous research has shown that emotion dysregulation served as a mediator between child abuse and neglect and psychopathology.52,54,55 Previous work also suggested that alexithymia moderated the relationship between emotion dysregulation and psychopathology.56,57
In our study, since alexithymia had a direct effect on developing Internalizing problems, suggesting that the core features of difficulties in identifying, naming, and describing emotions were leading to withdrawal behavior and self-control inappropriately. Alexithymia and emotional dysregulation are conceptually overlapping, and alexithymia could lead to the use of poor emotional regulation strategies, thus leading to Internalizing problems. There is abundant research evidence that relates emotion regulation difficulties as well as alexithymia with a variety of health-related issues such depression, anxiety, and PTSD since people try to utilize counterproductive attempts to regulate effectively and even recognize emotions. 50 The authors attempted to comprehend the similarities between the two constructs. They suggested that emotional regulation issues, particularly a lack of emotional clarity and a refusal to accept emotional responses, mediate the effect of alexithymia on some aspects of mental health, including depression, anxiety, insomnia, somatic complaints, and social dysfunction. They concluded that their emotional regulation issues may largely cause the poor mental health seen in those with alexithymia.
The other pathway of childhood trauma having a direct effect on Internalizing problems and mediated by emotional dysregulation can be explained by various theories such as the “kindling” hypothesis and sensitizing effect, where researchers believe that childhood trauma might heighten sensitivity or enhance a person’s vulnerability to adverse events, that is, even seemingly insignificant occurrences could cause a person to have a strong emotional response later on. 58 Trauma can lead to increased unprocessed emotions, which can further lead to poor emotional regulation strategies. Adolescents who have experienced childhood abuse may feel shielded from addressing and processing upsetting emotional events, which may lead to a heightened degree of psychiatric symptoms.53,59 The use of avoidance tactics to protect against the distress brought on by abuse was driven by the adjustment of self-capacities in regulating effect. Thus, adolescents struggled with processing distressing emotions and connecting with their feelings, and many tried to repress distressing emotional reactions, a hallmark of poor emotional regulation. The current study highlights emotional regulation as a buffer against psychological distress in adolescents. Previous studies on Indian adolescents suggest that parenting practices potentially influence emotional regulation. Positive parenting techniques can equip adolescents to manage emotions effectively. (Singh P. Emotion regulation difficulties, perceived parenting, and personality as predictors of health-risk behaviors among adolescents. 57
Much of the existing research comes from Western populations. Investigating these factors in India considers the unique cultural influences on emotional expression and how emotions are perceived, regulated, and managed depending on the socialization aspect. This can reveal how these variables interact differently within an Indian context.
Alexithymia itself might manifest differently in Indian adolescents. The cultural emphasis on social harmony might lead to the externalization of difficulties, with adolescents expressing physical symptoms or behavioral problems instead of verbalizing emotional distress.
Adolescents who experienced abuse in early childhood may benefit from therapy that focuses on certain emotion regulation skills since this regulation of emotions is a transdiagnostic concept. The results also highlight the necessity of examining emotion dysregulation and alexithymia concurrently within the context of the link between childhood abuse and psychopathology in future studies and therapy planning. The findings of this study suggest that culturally sensitive transdiagnostic therapy that targets emotion dysregulation and alexithymia should be beneficial for those having a history of childhood maltreatment with comorbid psychopathology.
Strengths and Limitations
Despite the substantial strengths and implications, the present study has limitations. While a cross-sectional design limits our ability to establish causal relationships, mediation analysis can still be valuable in this study. It allows us to explore potential pathways through which childhood trauma might influence alexithymia via emotional regulation difficulties. This approach can serve as a springboard for future longitudinal studies that can definitively establish causality. Our research addresses the knowledge gap by investigating these pathways, which previous studies in the Indian context have only explored in terms of a simple association between childhood trauma and alexithymia. The sample was taken from a tertiary hospital clinical population with a purposive sampling, which is less superior to a multicentric communitywide study, which restricts generalizability, given the complexity of the relationships between the variables under investigation. We acknowledge the exploratory nature of our research and the need for further validation in future studies. As the self-report questionnaire approach was used in the current study, evaluating the subjective self-report and recall bias with care is important. In the future, surveys completed by individuals familiar with adolescents (such as parents and caregivers) may be used to review our findings. While the present study highlighted the significance of environment on the mental health of adolescents who experienced childhood trauma, the impact of individual characteristics, especially protective factors at play, was not examined. Future research can examine personal aspects such as personality, cognitive style, support, and familial environment.
Conclusion
It is imperative to provide support to adolescents having trauma in terms of helping them regulate their emotions and express them healthily. A transdiagnostic approach focusing on emotional regulation strategies can be utilized to mitigate the effect of trauma.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethics Approval
IEC-IHBAS 2022/5/14/V-1.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent/assent was obtained from participants of this study.