
Abstract
Background:
Adolescents are particularly vulnerable to emotion dysregulation (ED), a transdiagnostic marker of psychological disorders with implications for academic achievement, identity development, social bonding, mental health, and the overall well-being and development of adolescents. A well-validated tool for the assessment of ED is imperative for credible advances in research on ED among Indian adolescents. Difficulties in Emotion Regulation Scale-Short Form (DERS-SF) is a promising tool to assess ED but requires proper psychometric validation among Indian adolescents. The current study validated the factor structure and examined psychometric aspects including gender invariance testing of the DERS-SF in Indian adolescents aged between 14 and 20 years.
Methods:
In a cross-sectional study, a community sample of n = 2079 adolescents completed the English version of the DERS-SF, the Strengths, and Difficulties Questionnaire, the Barratt Impulsiveness Scale, and the Adolescent Problem Behaviour Index.
Results:
The six-factor model of the DERS-SF exhibited an acceptable model fit in the current study sample. Invariance testing revealed that the DERS-SF is conceptually interpreted in a similar manner by male and female adolescents. Two-way MANOVA indicated gender and age variations on a few DERS-SF subscales. Reliability for DERS-SF was good, α = 0.86. Adequate construct validity was demonstrated by moderate to strong associations of the DERS-SF subscales with measures of internalizing and externalizing symptoms, adolescent problem behaviors, and impulsivity.
Conclusions:
DERS-SF retained the popular six-factor structure with acceptable psychometric properties and hence can be reliably used with Indian adolescents.
Keywords
The six-factor model of the DERS-SF is valid in the Indian adolescent population and it represents the best interpretable factor solution of the DERS-SF. The DERS-SF and its factor structure holds good across genders and is interpreted in a similar manner by male and female adolescents that justify mean comparisons across genders. The awareness subscale though exhibits good reliability, yet it fared poorly on construct validity as compared to all other scales and hence should be interpreted with caution. Significant age and gender variations on the DERS-SF further lend credence to the construct validity of the DERS-SF which can be reliably used with Indian adolescents.Key Messages:
The concept of emotion dysregulation (ED) has evolved over time and crystallized into a comprehensive construct. Gratz and Roemer 1 defined ED as the “relative absence of any or all” the following abilities related to the emotions of an individual: (a) awareness about one’s emotions; (b) acceptance of one’s emotions; (c) inhibition of undesired behaviors and promotion of goal-directed behaviors in distressing situations; and (d) adaptive use of existing emotion regulation strategies to modulate one’s emotions to meet personal goals and situational demands.
Adolescents as compared to other age groups experience greater ED because they exhibit increased emotionality partly due to significant developmental transitions. 2 ED is believed to interfere negatively with adolescents’ adjustment,3, 4 academic achievement,5–8 career building, 9 development of clear identity,10, 11 social bonding, and overall psychosocial well-being.12, 13 ED in general has also been linked to many psychiatric disorders and is considered a transdiagnostic marker of psychopathology.14–17
ED in adolescents has received relatively little attention of researchers in India. Assessment of any construct or phenomenon is key to its scientific progress and the lack of well-validated assessment tools has been considered by many as one of the contributing factors to the relative dearth of literature on adolescent emotion regulation.18–20 Most of the studies undertaken to examine emotion regulation in adolescents either directly use or adapt tools originally developed and standardized for children or adults. One of the widely used tools to assess emotion regulation-related difficulties in adolescents is the Difficulties in Emotion Regulation Scale (DERS). 1 DERS has 36 items that assess difficulties in emotion regulation across six domains, namely: awareness of emotions, clarity about emotions, negative reactions toward one’s emotional responses, access to existing emotion regulation strategies, control of impulsive behaviors, and engagement in goal-directed behaviors. Kaufman et al. 21 transformed the original DERS into an abridged version, called the DERS-Short Form (SF). DERS-SF has 18 items that capture all the six dimensions of ED assessed by the original DERS. DERS-SF is suitable for use with both adolescents and adults and has demonstrated “equivalent to improved” psychometric properties as compared to the original DERS. 22 While shorter versions of assessment tools are desired in several contexts, especially clinical and longitudinal research, their use with adolescents is intuitively relevant. This is because adolescents as compared to adults may quickly experience boredom or fatigue when filling lengthy assessment tools, and therefore gives rise to the risk of random responding and lower response rates.23–27
In view of the background above highlighting the need and implications of a psychometrically tested ED tool, the present attempted to validate the factor structure and psychometric aspects of the DERS-SF among Indian adolescents. Since DERS-SF has largely a known six-factor structure, the present study directly examined the validity of the same six-factor model by employing confirmatory factor analysis (CFA) techniques. Next, the current study expanded the scope of CFA to include multi-group analysis for testing measurement invariance of the DERS-SF across genders of adolescents. Invariance testing is a rigorous psychometric exercise that determines if the DERS-SF is interpreted conceptually in a similar manner by adolescent males and females.28, 29 In colloquial terms, invariance testing will ensure that the DERS-SF does not mean apples to male adolescents and oranges to female adolescents or vice. Therefore, invariance testing examined if there is equivalence across genders in the factor structure, factor loadings, means and intercepts, and item residuals of the DERS-SF. Finally, the study examined internal consistency reliability, and construct validity by examining the association of the DERS-SF total score and its subscale scores with measures of internalizing and externalizing symptoms, and adolescent problem behaviors. The evaluation of construct validity was further supplemented by examining the association of the DERS-SF with other measures that have theoretical relevance to the construct of ED.
Method
Participants
The participants included school and college-attending adolescents (14–20 years; mean age 17 years) who could read, write, speak, and comprehend English. Though hard data regarding all the sociodemographic characteristics were not acquired, the targeted schools and colleges, however, varied in board affiliations (CBSE, ICSE, State board), fee structure, course specializations, socio-cultural milieu, and geographical locations. The approximate sample size of the study from which the current data was drawn was estimated according to the N:p ratio, where N was the required sample size and p was the number of observed variables. 30 The total number of participants recruited in the main study was n = 2079, but for the present study, the data was analyzed from n = 1993 adolescent participants who met the study criteria. Approximately 49% of the participants identified themselves as females and 51% as males.
Measures
Difficulties in Emotion Regulation Scale-Short Form (DERS-SF) 21
It is an 18-item shorter version of the original DERS. 1 DERS-SF measures ED-related difficulties among adolescents and adults across six domains: strategies, non-acceptance, impulse, goals, awareness, and clarity. DERS-SF employs a Likert response format: 1 = almost never to 5 = almost always. It gives a separate score on each subscale and an overall score where higher scores suggest a greater degree of ED. DERS-SF has exhibited excellent psychometric properties such as internal consistency reliability and concurrent validity among adolescents and adults. 21
Apart from the DERS-SF, the study also used other self-report measures including the Strengths and Difficulties Questionnaire, 31 the Barratt Impulsiveness Scale 32 (BIS-15), and the Adolescent Problem Behaviour Index for assessing the participant’s degree of impulsivity, psychological maladjustment, and extent of involvement in problematic or risky behaviors such as substance use and unsafe sexual practices.
Procedure
The study was approved by the ethics committee of the institute where the study was registered. Next, various schools and colleges in central Bengaluru were approached for sample selection which was based on convenience mode of sampling. The data collection was done in group settings and lasted from June 2017 to February 2018. The participants were sensitized regarding the nature and purpose of the study, freedom of participation, risks and benefits, confidentiality of identity (both individual and school/college), and the potential uses of the survey results. Any doubts, clarifications, or queries regarding the survey were addressed by the first author as and when the need arose. The study obtained written consent as well as assent from all the participants including the parents.
Data Analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) and Analysis of Moment Structures (AMOS) version 20. Eighty-six adolescents who had more than one item missing on the DERS-SF were removed from analysis leaving the total eligible sample for analysis at n = 1993. The series mean method was used to replace the single missing value of n = 135 cases on the DERS-SF. Normality was tested by estimating absolute measures of skewness and kurtosis, and Q–Q plots. Means, standard deviation, and percentages were used to summarize quantitative and categorical variables respectively. Cronbach’s alpha (α) was used to estimate the internal consistency reliability. CFA was employed to test the pre-existing six-factor model of the DERS-SF in the current study sample. Specifically, the maximum likelihood estimation procedure was used which is a preferred method of estimating model fit statistics for data sets with normal distribution and continuous variables. Gender invariance of the DERS-SF was examined by adopting multi-group CFA procedures. Age and gender variations across the DERS-SF subscales were examined with two-way MANOVA. To facilitate this comparison, adolescents falling in the age bracket of 14–17 years were labeled as middle adolescents and those in the 18–20 brackets were labeled as late-adolescents. Construct validity was examined by estimating Pearson’s correlation coefficients between the DERS-SF total and the subscale scores with other measures used in the study.
Results
CFA of the DERS-SF
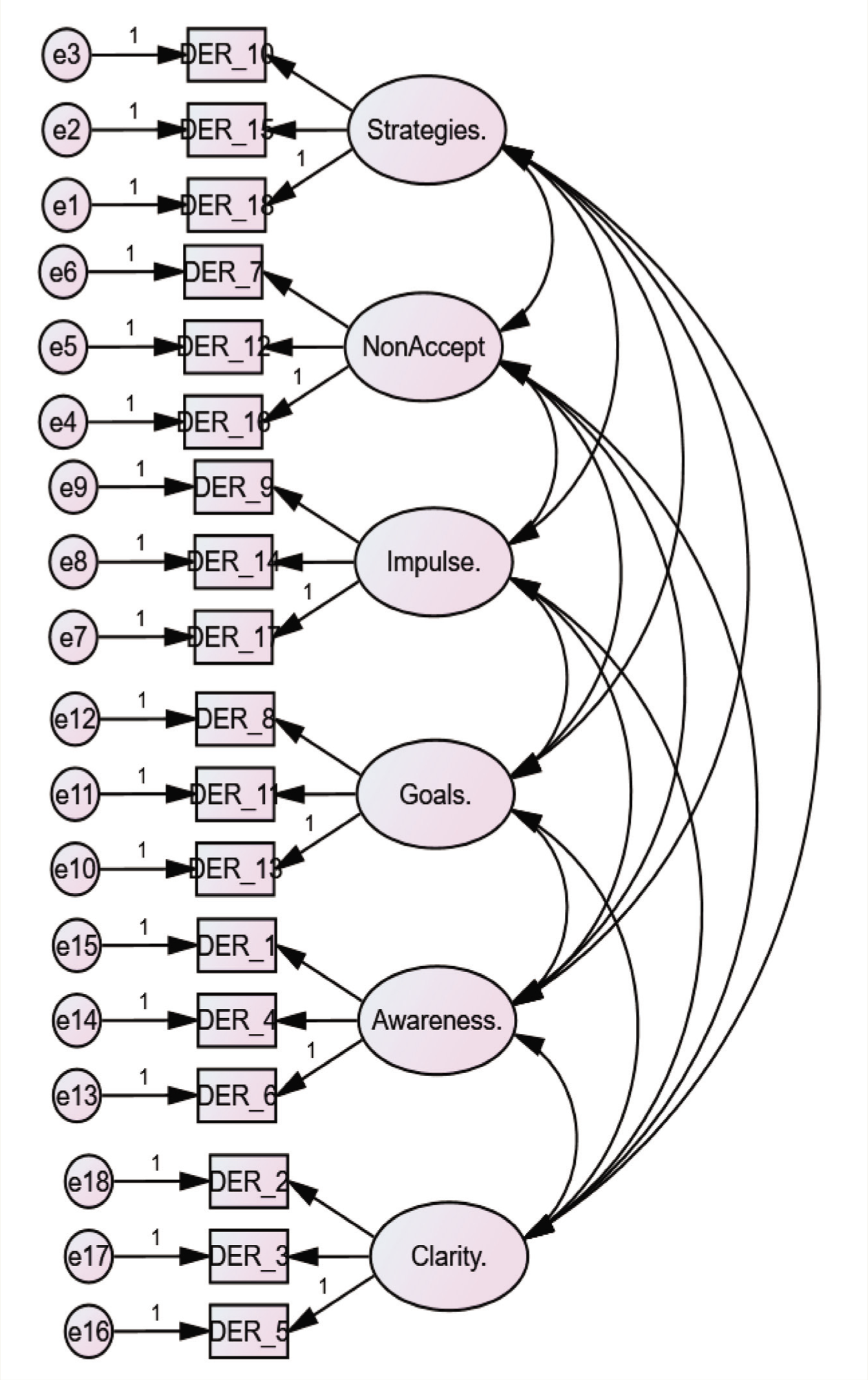
The data was normally distributed as revealed by a closer visual inspection of the Q–Q plots and absolute values of skewness and kurtosis which were within the acceptable range of ±1. The path diagram of the measurement model for CFA of the DERS-SF is depicted in Figure 1. We followed a conventional method of reporting the CFA results used in several validation studies involving the original DERS 1 as well as its short forms.19, 33–35 Specifically, we reported the following incremental and absolute measures of fit indices: Model chi-square (χ2), Bentler’s comparative fit index (CFI), the Tucker Lewis Index (TLI), the goodness of fit index (GFI), the root mean square error approximation (RMSEA) and the standardized root mean square residual (SRMR). We did not rely on the model chi-square (χ2) statistic and normed chi-square (χ2/df) for evaluating model fit to avoid the risk of committing type 1 error. 36 The CFA results suggested that the six-factor model of the DERS-SF exhibited an acceptable model fit with the data (χ2 = 845.98, df = 120, p < .001; χ2/df = 7.05; CFI = 0.95; TLI = 0.94; GFI = 0.95; SRMR =0.04, and RMSEA = 0.05). The factor loadings, which express a correlation between the item and the factor, were statistically significant and are depicted in Table 1.
The AMOS Path Diagram for the Six-factor Measurement Model of the DERS-SF.
Confirmatory Factor Analysis Loadings of the DERS-SF Items in the Study Sample.
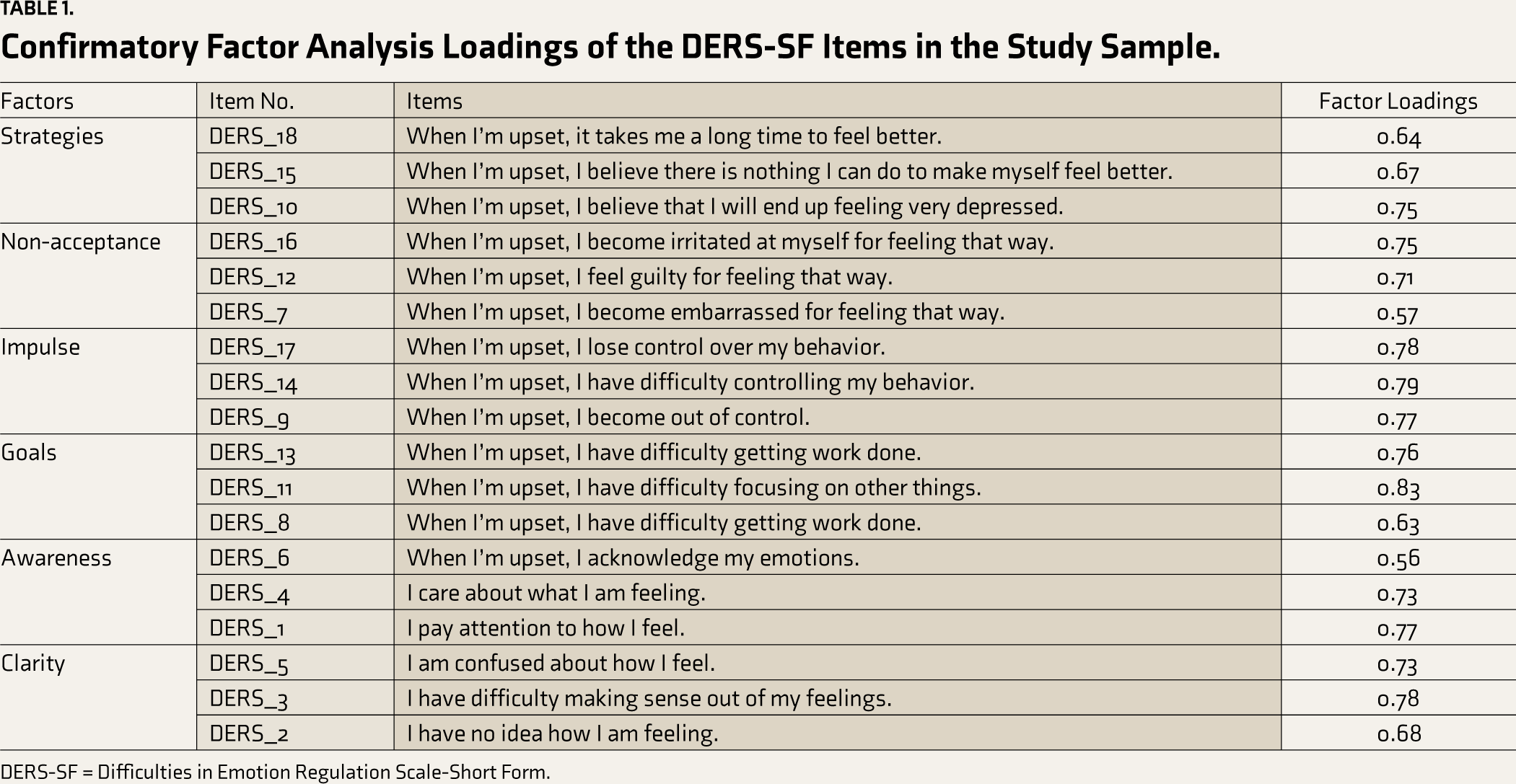
DERS-SF = Difficulties in Emotion Regulation Scale-Short Form.
Measurement Invariance of the DERS-SF Across Gender
We tested gender invariance of the DERS-SF at all four levels as recommended in the literature on invariance testing.29, 37 These include configural invariance (equivalent factor structure across gender), metric invariance (equivalent factor loadings across gender), scalar invariance (equivalent mean intercepts across gender), and residual invariance (equivalent item residuals across gender). We considered significant changes in the alternate fit indices such as ΔCFI and ΔRMSEA for establishing measurement invariance or non-invariance of the DERS-SF across male and female participants. Specifically, ΔCFI > 0.01 and ΔRMSEA > 0.015 indicated non-invariance of the DERS-SF at any of the four levels and vice-versa.28, 38 Although we have also reported Δ χ2 statistics, they were not considered for deciding measurement invariance because of the large sample size of the present study. 39 The results of the measurement invariance analysis were largely organized in accordance with the recommendations of Putnick and Bornstein 29 and are depicted in Table 2. It is evident from Table 2 that ΔCFI < 0.01 and ΔRMSEA < 0.015 for all four models. These results indicate a lack of credible change in the model fit statistics across genders after constraining of parameters at the metric, scalar, and residual levels.
Measurement Invariance Fit Statistics for the DERS-SF for the Female and Male Adolescents.
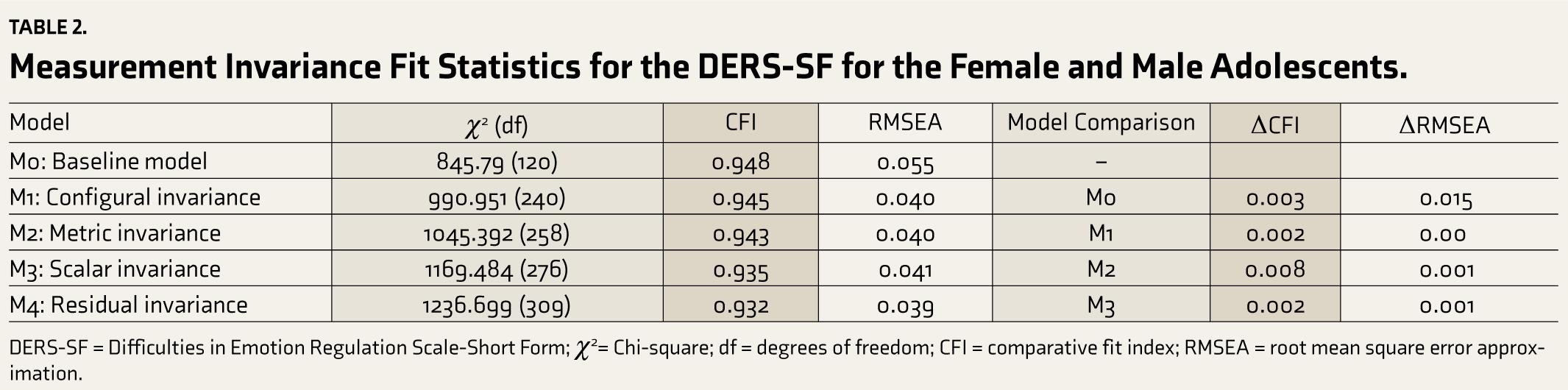
DERS-SF = Difficulties in Emotion Regulation Scale-Short Form; χ2= Chi-square; df = degrees of freedom; CFI = comparative fit index; RMSEA = root mean square error approximation.
Age and Gender Variations in the DERS-SF Subscales Among Indian Adolescents
Age and gender variations across the DERS-SF subscales were examined with the help of two-way MANOVA. We categorized adolescents between 14 and 17 years of age as belonging to “mid adolescence,” and those between 18 and 20 years of age as belonging to “late adolescence.” A statistically non-significant interaction between age and gender (F6, 1796 = 0.69, p = .66) was evident from the results of two-way MANOVA. There was, however, a significant main effect of the age (F (6, 1796) = 9.31, p < .001) and gender (F (6, 1796) = 7.96, p < .001) across certain DERS-subscales as is evident from Table 3. The main effect of gender was observed only for the clarity and the awareness subscales of the DERS-SF. In general, the male adolescents exhibited higher scores on the awareness subscale as compared to female adolescents ( 1 Mm = 8.5, 2 Mf = 7.76), whereas the reverse was true for the clarity subscale (Mm = 7.52, Mf = 7.98). Similarly, the main effect of age was reflected only across the awareness, impulse, and non-acceptance dimensions. In general, the middle adolescents exhibited greater mean scores on awareness (Mmid = 8.31, Mlate = 7.95), non-acceptance (Mmid = 5.15, Mlate = 4.89), and impulse ( 3 Mmid = 7.00, 4 Mlate = 6.40) subscales as compared to late adolescents.
Mean (SD) Values of the DERS-SF Subscales Across Subgroups of Gender and Age Along with p Values.
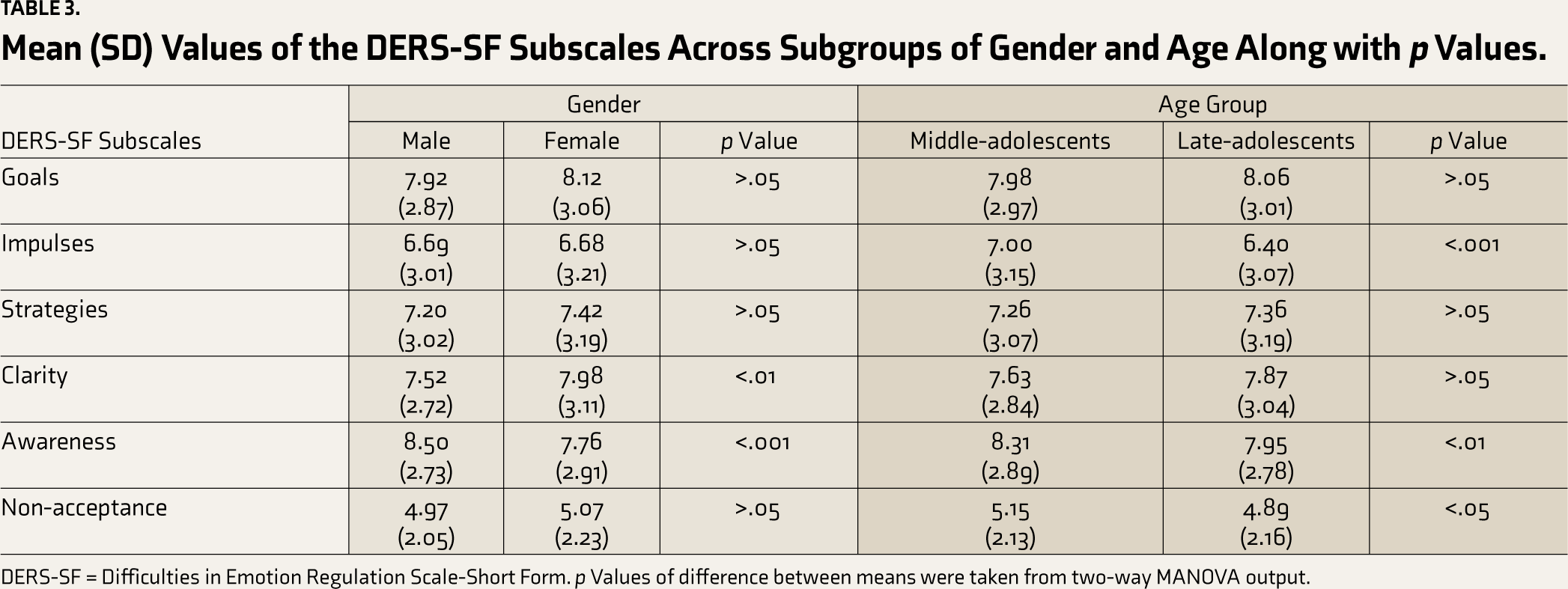
DERS-SF = Difficulties in Emotion Regulation Scale-Short Form. p Values of difference between means were taken from two-way MANOVA output.
Psychometric Properties of the DERS-SF Among Indian Adolescents
Tables 4 and 5 summarize different psychometric aspects of the DERS-SF among Indian adolescents. Internal consistency reliability as measured by Cronbach’s alpha (α) was 0.87 for the overall DERS-SF scale for the study sample. Cronbach’s alpha (α) for the six DERS-SF subscales ranged from 0.72 to 0.82.
Correlations Between the DERS-SF Subscales and Their Cronbach’s Alpha (a) in Indian Adolescents.
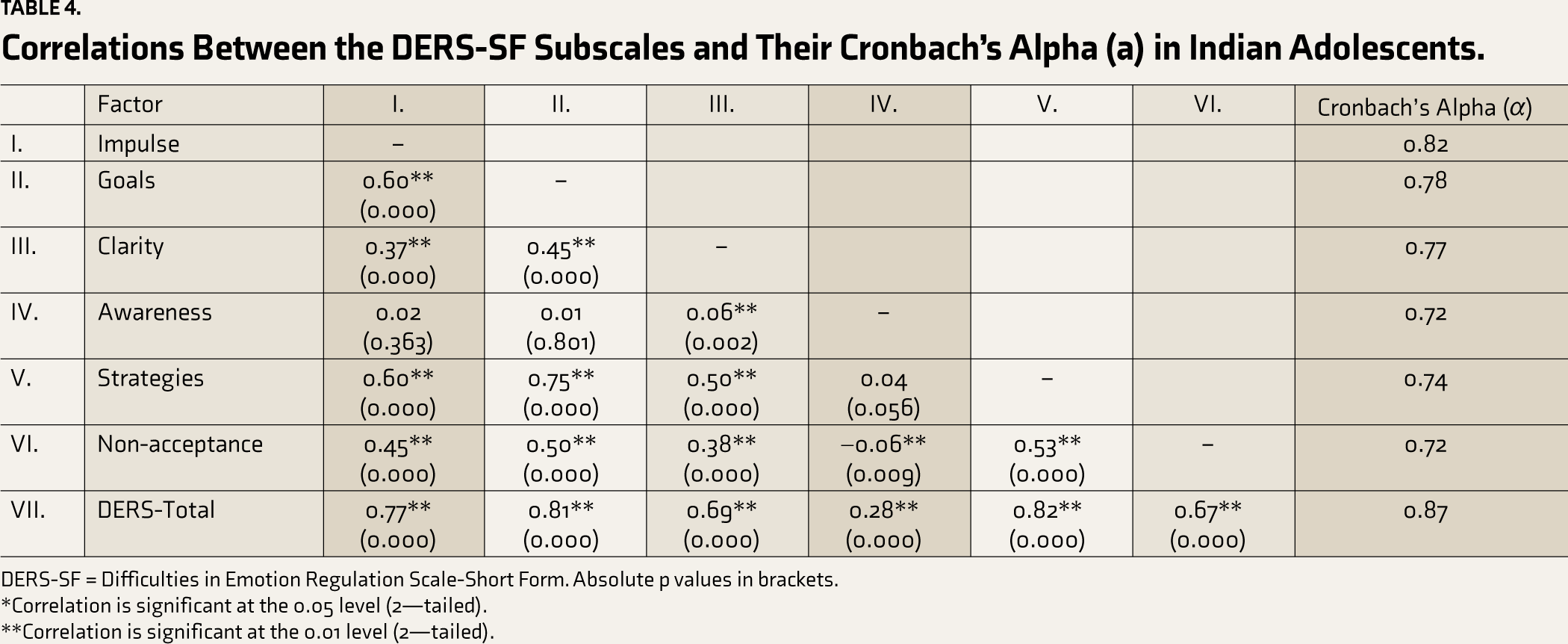
DERS-SF = Difficulties in Emotion Regulation Scale-Short Form. Absolute p values in brackets.
*Correlation is significant at the 0.05 level (2—tailed).
**Correlation is significant at the 0.01 level (2—tailed).
Pearson’s correlation coefficient estimates of the DERS-SF with other variables as shown in Table 5 reflect its construct validity. The correlations of DERS-SF subscales with internalizing and externalizing symptoms were positive and largely moderate to high in magnitude. However, the awareness subscale showed a weak to very weak correlation with the externalizing and the internalizing symptoms respectively. The DERS-SF subscales, excluding the awareness and non-acceptance subscales exhibited modest positive correlations with the adolescent problem behaviors. The overall score of impulsivity exhibited a moderately positive correlation with the DERS-SF subscales, except for the awareness, and the non-acceptance subscales. The non-acceptance and the awareness subscales were modestly associated with the total impulsivity score.
Pearson’s Product Moment Correlation Coefficients Between the DERS-SF Subscales and Other Measures Used in the Study.
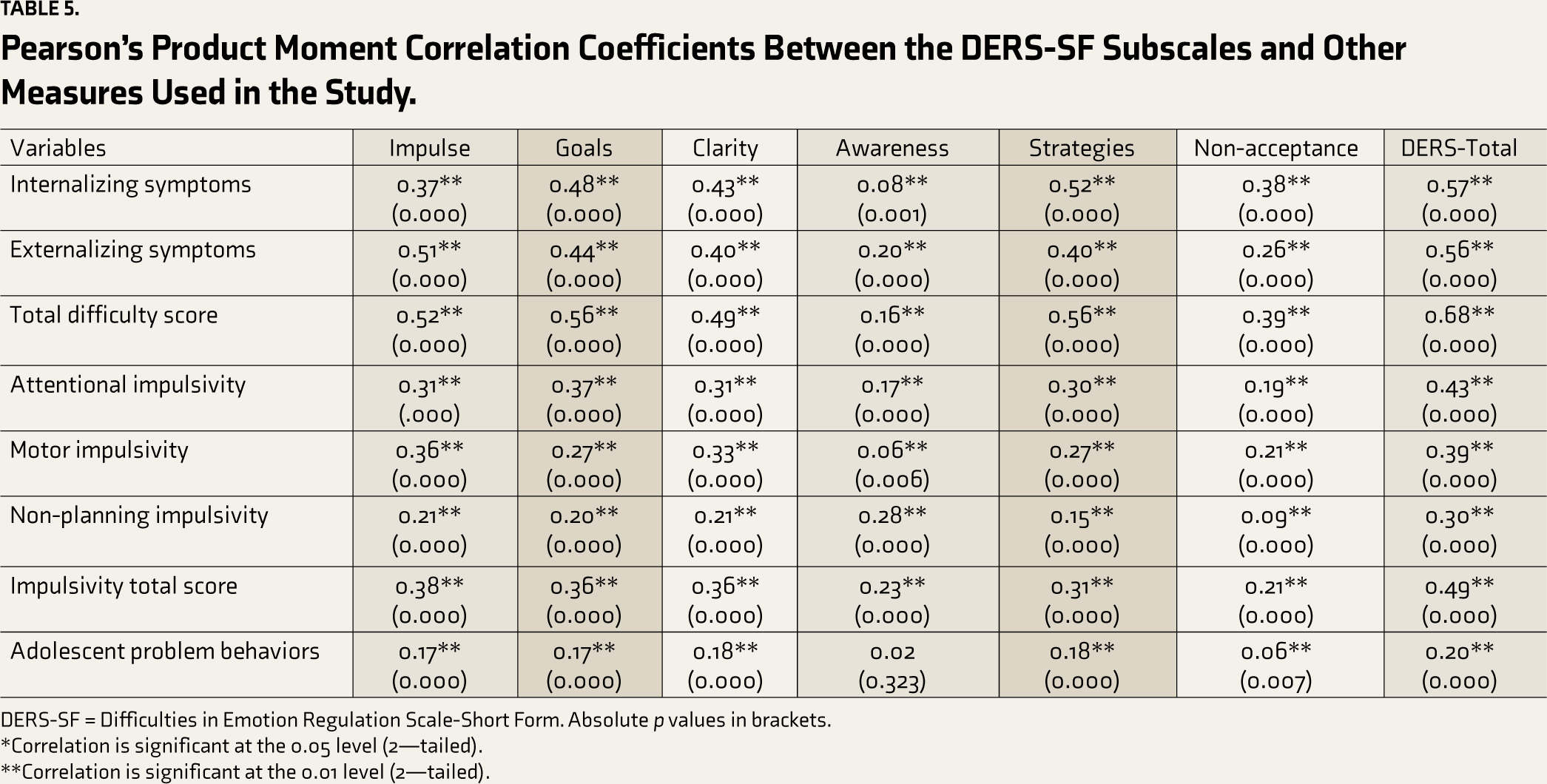
DERS-SF = Difficulties in Emotion Regulation Scale-Short Form. Absolute p values in brackets.
*Correlation is significant at the 0.05 level (2—tailed).
**Correlation is significant at the 0.01 level (2—tailed).
Discussion
This study attempted to validate the six-factor model of the DERS-SF in a large community sample of urban Indian adolescents. The results revealed an acceptable fit for the pre-existing six-factor model of the DERS-SF among the Indian adolescent sample. Hence our findings were consistent with Kaufman et al. 21 and other previous dealing with the psychometric aspects of the DERS among non-Indian adolescents.19, 20,34
The findings from invariance testing were also fully consistent with the findings of Kiekens et al. 40 Configural and metric invariance indicated that the DERS-SF has an identical factor structure, and the items contribute equivalently to their corresponding latent factors in male and female Indian adolescents. Scalar invariance justified the calculation and comparison of latent mean scores on the DERS-SF subscales between male and female adolescents. More importantly, these results also demonstrated that any gender differences on the DERS-SF subscales are reflective of actual differences in trait ED between male and female adolescents.
The results on gender differences indicated that male adolescents exhibited slightly greater deficits related to the awareness of emotions, whereas, female adolescents had greater deficits related to the clarity of emotions. Though the previous findings in the literature are slightly mixed, the results concurred with findings from the majority of the earlier studies.19, 20, 34 The middle-aged adolescents as compared to older adolescents exhibited greater deficits related to the awareness of emotions, non-acceptance of emotional responses, and difficulty inhibiting impulsive behaviors. Emotion regulation skills are shaped and influenced by the neuro-maturational process and the extent of socializing experiences, both of which are relatively underdeveloped and less extensive respectively among mid-adolescents as compared to older adolescents.41–44
The overall DERS-SF score including its subscale scores showed significant correlations with measures of internalizing and externalizing symptoms, impulsivity, and adolescent problem behaviors, thereby providing empirical support for its construct validity among Indian adolescents. These results largely concurred with the findings from previous studies.19, 20, 22, 34, 45–47 A notable exception to these results was the relatively poor validity of the awareness subscale as depicted by its modest correlations with the measures of psychopathology and adolescent problem behaviors. The poor validity of the awareness subscale has been consistently reported in the literature and has been explained from a methodological, conceptual, and operational point of view.1, 19, 20, 33 For example, some researchers attribute the poor validity of the awareness subscale to the reverse coding of the items in this subscale.48–50 Conceptual explanations emphasize the relevance of emotional awareness to the construct of ED. Awareness about one’s emotions is the first and most important component of the emotion regulation process that directly affects the perception of emotions. However, emotional awareness may not have a much active strategic role in the actual process of emotion regulation. For example, Bardeen et al. 48 maintain that the effective components of emotion regulation with potential implications for altering affective states and influencing psychopathology follow later in the series of steps of the emotion regulation process. Operational explanations attribute the poor validity of the awareness subscale mainly to the wording and framing of items of the awareness subscale. For example, Weinberg and Klonsky 20 argued that the wording used in the items of the awareness subscale may not be developmentally appropriate for adolescents. Based on this line of reasoning, it may be argued that the choice of words such as “care” and “acknowledge” in the awareness subscale (“I care about what I am feeling, When I’m upset, I acknowledge my emotions”) may not have clearly articulated or conveyed the intended aspects of emotions to adolescents in the present study.
Limitations, Future Directions, and Implications
Despite examining several psychometric aspects of the DERS-SF, the current study still has several deficiencies and limitations. The present study could not conduct comprehensive psychometric testing to include convergent validity, divergent validity, or test-retest reliability. Studies in the future involving Indian adolescents should include measures that assess constructs closely related to ED, and consider longitudinal assessments with the DERS-SF to address these deficiencies. Additionally, examining the specific relevance of the DERS-SF subscales to internalizing and externalizing symptoms would address the issue of the discriminant validity of the subscales. Another limitation is the generalization of findings to populations that were not part of the study sample notably early adolescents aged 11–13 years, rural adolescents, adolescents from other parts of India, adolescents with inadequate English comprehension skills, and adolescents with clinical conditions who are beset by significant emotion regulation difficulties. The self-report measures are prone to response bias and adolescents have been found to exaggerate their emotion regulation difficulties in comparison to their parental reports. 51 Task-based objective measures of emotion regulation could be employed in future studies to rigorously verify the validity of the DERS-SF among Indian adolescents. Future studies should also consider the adaptation and translation of the original DERS-SF into local languages and examine their psychometric aspects.
Emotion regulation difficulties are widely assessed in clinical and non-clinical settings. The DERS-SF would provide an efficient alternative to its lengthy parent version, the DERS, 1 to comprehensively assess adolescents for emotion regulation difficulties. Generating the percentile norms for the DERS-SF would be helpful in identifying adolescents whose emotional regulation skills deviate significantly from typically developing adolescents. For clinicians, the DERS-SF would be helpful for identifying specific emotion regulation deficits and can aid in individualizing the subsequent intervention programs for training such adolescents in emotion regulation skills. In clinical research settings, it can be used as an outcome measure to evaluate the efficacy of treatment modules such as emotion-focused therapy or dialectical behavior therapy which teach and train on emotion regulation skills.
Conclusions
The findings of the present study represent a valuable addition to the cross-cultural literature on the factor structure, psychometric aspects, and measurement invariance testing of the DERS-SF.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
This paper was the outcome of PhD study, for which ethical approval was granted by the Institute Ethics Committee (IEC) of the National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.