
Abstract
Background:
Alcohol dependence syndrome (ADS) is a significant challenge for psychologists due to relapse and its impacts on well-being. Mindfulness-based relapse prevention (MBRP) has emerged as a potential solution, receiving increasing attention in the field of psychological interventions for ADS. This study aimed to evaluate the impact of MBRP, specifically on emotion regulation and alcohol craving as primary outcomes, alongside the secondary consideration of assessing changes in mindfulness levels.
Methods:
In this quasi-experimental study utilizing a pre-test/post-test design, 50 patients (aged 18–55) with ADS were enrolled in the intervention group (MBRP + usual care) and the usual care alone (UCA) group. The outcome assessment employed the Difficulties in Emotion Regulation Scale-18 (DERS-18) and Alcohol Craving Questionnaire-Short Form Revised (ACQ-SF-R) at three time points: pre-intervention (T1), mid-intervention (T2, four weeks after MBRP initiation), and post-intervention (T3, MBRP completion). Post-intervention comparisons between the intervention and UCA groups utilized repeated measures ANOVA (p < .05).
Result:
In the intervention group, significant within-group improvements were observed in mean scores of emotion regulation and craving at T1 (56.8 ± 7.6 and 41.6 ± 7.3), T2 (61.7 ± 10.5 and 41.5 ± 7.4), and T3 (61.5 ± 10.6 and 35.6 ± 5.4), with p values of .006 and .001, respectively. In comparison, the UCA group showed significant post-intervention differences in emotion regulation (46.9 ± 16.4) and craving (34 ± 11.82) scores, with a p value of .004. The effect sizes for emotion regulation (0.42) and craving (1.43) in the intervention group and for emotion regulation (0.50) and craving (0.47) in the UCA group further demonstrated more favorable outcomes in the intervention group, especially in reducing craving.
Conclusion:
Our research indicates that intervention and UCA yields moderate enhancements in emotion regulation; however, intervention demonstrates superior efficacy in diminishing craving, which is pivotal for relapse prevention. Incorporating MBRP with bespoke interventions might optimize the long-term treatment of ADS.
The World Health Organization 1 has recently emphasized that no level of alcohol intake can be considered safe without impacting health. Alcohol dependence syndrome (ADS) is a chronic disorder characterized by excessive alcohol consumption, contributing to over 3 million deaths annually and more than 5% of the global disease burden. 1 ADS is influenced by various factors, including genetic predisposition, neurobiological alterations, environment, and psychology.2-5 It is also recognized that ADS can vary in severity, comorbidity, and treatment response.6,7
Understanding ADS and effective interventions is vital for improving treatment outcomes and minimizing adverse effects. Despite available interventions, treatment-seeking disparities persist. 8 Severe ADS requires professional assistance, although some can reduce consumption without medical intervention. 9 Alcohol addiction has high relapse rates, with around 80% of relapse within a year of discharge, 10 with cravings playing a crucial role, making them a valuable target for influencing behaviors.11-13 Drinking excessively frequently impairs the ability to control one’s emotions,5,14,15 and continued alcohol use exacerbates emotional processing. 16 Emotion regulation, defined as the ability to modulate one’s emotional experience and expression, is acknowledged as a universal construct essential across a spectrum of psychiatric conditions, encompassing alcohol dependence, among others. Recent research in the field of addiction and relapse prevention has increasingly focused on the role of emotion regulation. One such study is by Zaorska et al., 17 which investigated the relationship between emotional dysregulation and distress tolerance in AUD patients. Utilizing the Difficulties in Emotion Regulation Scale (DERS), they identified a notable link between these factors, highlighting the significance of emotion regulation challenges in AUD. Emotion regulation plays a significant role in alcohol addiction, 17 and modifying one’s perspective can reduce consumption. 18
Cognitive-behavioral management emphasizes emotional awareness, coping strategies, and a higher tolerance for improved abstinence outcomes. 19 Limited research exists on systematically exploring emotion and alcohol outcomes. 20 Various therapies have demonstrated effectiveness in reducing alcohol dependence; however, the long-term impact of these interventions on relapse prevention and sustained abstinence remains a primary concern for therapists. Recognizing the current treatment constraints in addressing emotion dysregulation and craving, various mindfulness-based interventions have emerged, like mindfulness-based relapse prevention (MBRP), to target this objective. 21
MBRP intervention integrates cognitive-behavioral and mindfulness strategies to recognize triggers, modify responses tocravings and negative emotions, and strengthen overall well-being for improved long-term outcomes. 22 MBRP promotes non-judgmental awareness; improves self-awareness, emotion regulation, and attentional control; reduces impulsive alcohol responses; and promotes adaptive coping and positive emotions.23-25 MBRP combines relapse prevention training with mindfulness techniques, offering the potential for enduring effects in maintaining abstinence. 26 MBRP addresses negative mood without automatically reacting and reduces craving by recognizing these factors as critical factors in the relapse process. 9 An obstacle in MBRP is low adherence rates, with outpatient therapy having a compliance rate of 50%–60% compared to 70% for relapse prevention. 27 However, active participation in MBRP results in fewer and less severe relapses and improvements in overall quality of life. 9
The present study investigates the efficacy of mindfulness training in enhancing emotion regulation skills, which is a significant factor contributing to relapse. Moreover, reducing cravings has been recognized as a crucial target in treating ADS. 17 However, there is relatively limited research on emotion-related issues and their management in ADS. Hence, the present study addresses these issues within an inpatient setting, considering the lower adherence rates observed in outpatient therapy. The study aimed to examine differences and evaluate the effectiveness of MBRP in enhancing emotion regulation and reducing craving levels before and after the intervention compared to usual care alone (UCA) among the ADS in the Indian population. While the primary outcomes of this study center on assessing changes in emotion regulation and craving following MBRP, the secondary consideration encompasses exploring alterations in mindfulness levels among participants. This dual perspective seeks to comprehensively evaluate the interrelationships between mindfulness-based interventions, emotion regulation, and craving within the context of ADS treatment.
Methods
Study Design
This eight-week quasi-experimental pre-test/post-test study evaluated the effectiveness of MBRP as an adjunct to usual care in addressing alcohol dependence and preventing relapse. The study compared outcomes between the intervention group (MBRP + usual care) and the UCA group, examining differences in emotion regulation and craving levels within the intervention group and significant differences between the intervention group and the UCA group.
Participants
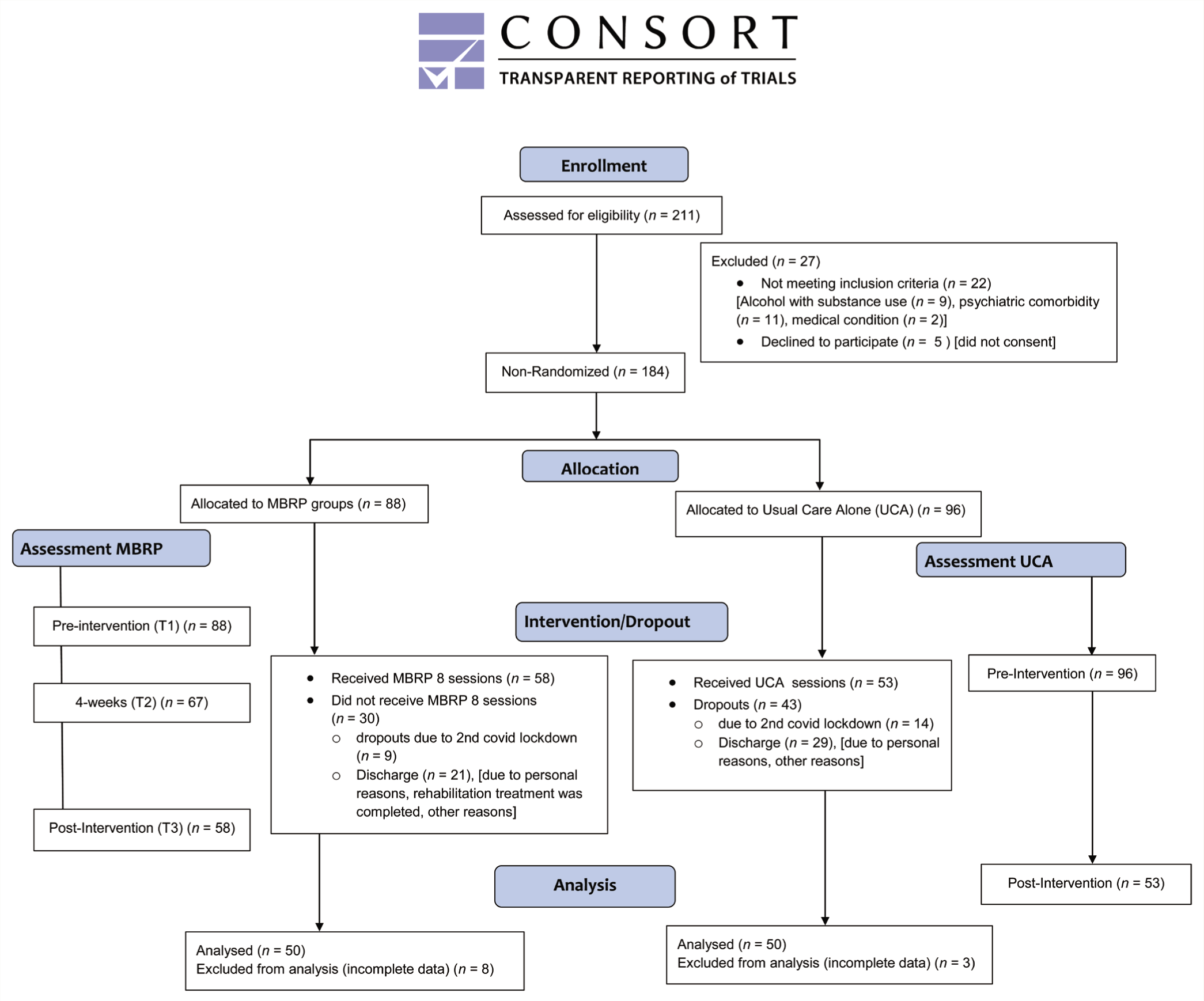
The study enrolled patients at a residential treatment center. Participants met specific criteria, including a diagnosis of F10.21 alcohol dependence syndrome according to ICD-10, abstinence from alcohol, informed consent, age between 18 and 55, completion of at least eighth grade, and medical detoxification treatment. Exclusion criteria included chronic physical illness, severe withdrawal symptoms, psychiatric comorbidities, substance abuse besides nicotine and caffeine, and an AUDIT score below 20. The residential facility provided data on alcohol-dependent patients aged 18–55 years. Initially, 211 patients were assessed; among these, 9 were excluded due to concurrent substance addiction, 11 were excluded due to psychiatric comorbidities, and 2 were excluded due to medical health issues associated with alcohol addiction. Additionally, five declined participation, citing resistance to any form of therapy. Ultimately, 184 patients met the criteria and were included in the study over one year.
Participant information, including demographics, alcohol-related history, and reactions to negative emotions, was collected using the Socio-demographic Proforma (SDP). Baseline assessments included the administration of the Alcohol Use Disorders Identification Test (AUDIT), 28 the Alcohol Craving Questionnaire-SF-R (ACQ-SF-R),29,30 and the Difficulty in Emotion Regulation Scale-18 (DERS-18).31,32 Due to COVID-19 and time constraints in this PhD study, simultaneous patient enrollment and randomization for the intervention and UCA groups were not feasible. Patients’ study inclusion relied on admission timings—interested admissions joined the intervention group, while others went to UCA. In each intervention group (6–12 participants), 58 completed the eight-week session, 9 dropped out (COVID-19-related), and 21 were discharged out of 88 participants. In the UCA group, 53 were completed, 14 dropped out (COVID-19), and 29 were discharged out of 96 participants. Participants who did not complete the full therapy sessions outlined in the study protocol were dropouts.
Conversely, completers were defined as individuals who adhered to the entire intervention schedule stipulated in our study design. The analysis included 100 participants: 50 in the intervention group and 50 in the comparison group. In the intervention group, four datasets were excluded due to incomplete responses during T3 assessments, three participants did not attend the T3 assessments as they were discharged just after completing the final session, and one participant could not complete all tests during T3 assessments. Similarly, initially, 52 participants completed the UCA treatment in the UCA group. We encountered difficulties completing assessments post-UCA treatment for three participants. To ensure a comparable number for analysis, we waited for one additional participant in the UCA group to complete the treatment and post-therapy assessments.
Data Collection
The study was conducted according to ethical protocols approved by the institutional review board. Participants were recruited from a residential treatment center where admission and discharge cycles were routine. Due to the facility’s practical constraints and the dynamic nature of participant admissions, a convenience sampling method was employed. Upon admission, this approach facilitated participant inclusion in the intervention group, accommodating their immediate engagement while considering operational limitations.
The allocation process was guided by participant readiness and availability within the MBRP therapy structure, which typically accommodates a participant size of 6– 12 individuals per group. Informational sessions conducted by the researcher with the help of facility management and staff outlined the study’s objectives, procedures, and potential benefits. Interested residents were provided with detailed information sheets and consent forms, engaging in discussions to address queries before consenting. Screening followed predefined eligibility criteria outlined in the study’s protocol.
To establish baseline measures, participants in the intervention group completed AUDIT, ACQ-SF-R, and DERS-18, as previously mentioned. After these assessments, motivational enhancement therapy (MET) was administered. Following MET, a pre-intervention assessment (T1) was conducted before MBRP was initiated for the intervention group, which included the DERS-18 and ACQ-SF-R. Follow-up assessments utilizing the same questionnaires were conducted at mid-intervention (T2), after four weeks, and after the therapy (T3), that is, post-intervention for the intervention group. Baseline measures for the UCA group encompassed the AUDIT, ACQ-SF-R, and DERS-18 assessments. After treatment completion, ACQ-SF-R and DERS-18 were administered for post-treatment evaluation. The final analysis included 50 participants from each group, totaling 100 participants. Figure 1 depicts the flow chart of the recruitment allocation and assessment process.
Flowchart of Recruitment Process.
Intervention
The MBRP program incorporated mindfulness practices within nine fixed groups, accommodating 6–10 participants each over eight weeks. This was conducted as outlined in Table 1 within a one-year timeline. MBRP is tailored to support individuals after they complete residential treatment. Given that our participants were already admitted to the facility, we implemented individual sessions of MET before the commencement of MBRP. The MET was administered after baseline assessments in the intervention group to enhance motivation and preparedness for subsequent therapy sessions. Following MET, the intervention group participants were allocated eight weekly sessions of MBRP therapy, lasting two hours each, involving meditation and daily home practice. This curriculum allowed participants to observe sensations, thoughts, emotions, and cravings without immediate reactions. The UCA intervention comprised standard inpatient modules focusing on relapse management, psychoeducation, group therapy sessions, and individual and family counseling. These components were designed to address the multifaceted nature of alcohol dependence and provide a holistic approach to care without the inclusion of specific mindfulness-based practices, without involvement in specific groups like the intervention group.
Sessions and Their Rationale for the MBRP Group.
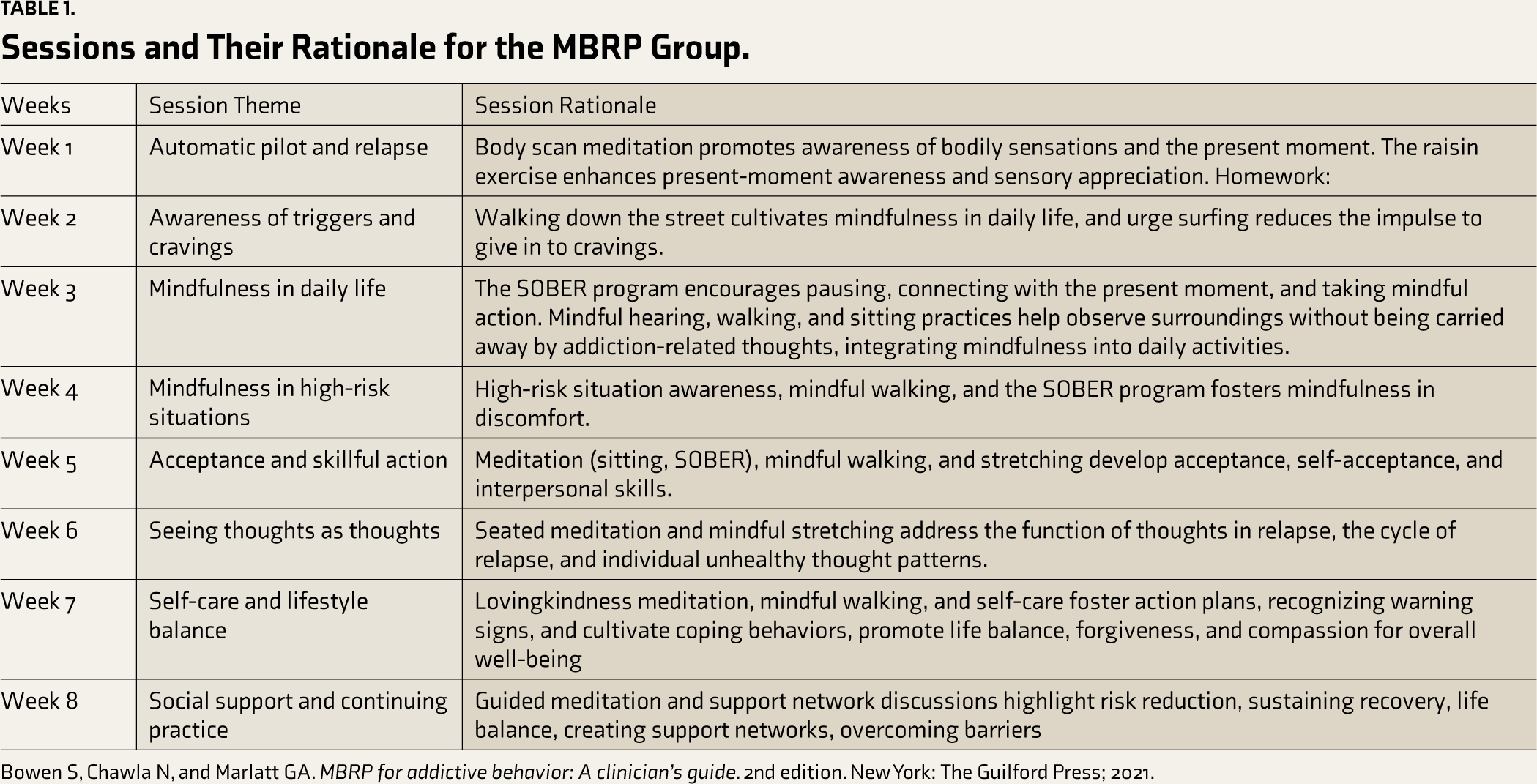
Bowen S, Chawla N, and Marlatt GA. MBRP for addictive behavior: A clinician’s guide. 2nd edition. New York: The Guilford Press; 2021.
Therapists
The MBRP therapy sessions were guided by a Rehabilitation Council of India–licensed therapist, who underwent specific training in MBRP during their doctoral studies, specializing in cognitive-behavioral and mindfulness interventions. This therapist rigorously practiced daily meditation and received weekly supervision. The UCA sessions were facilitated by counselors with an average of 15 years of experience delivering inpatient addiction services. These counselors hold expertise in group therapy, relapse prevention, and individual and family counseling, ensuring a comprehensive and informed approach to usual care.
Data Analysis
Data analysis was conducted using IBM SPSS Statistics 23. Normality was assessed using the Kolmogorov–Smirnov test. Fisher’s exact test provided descriptive statistics for socio-demographic data, reported as numbers (percentage). Repeated measures ANOVA examined differences within groups for pre-intervention (T1), mid-intervention (T2), and post-intervention (T3) measurements and between-group differences for pre- and post-intervention. Results were presented as mean ± SD. The significance was set at p < .05. Cohen’s d-effect size was reported to assess differences between groups.
Results
Baseline Characteristics
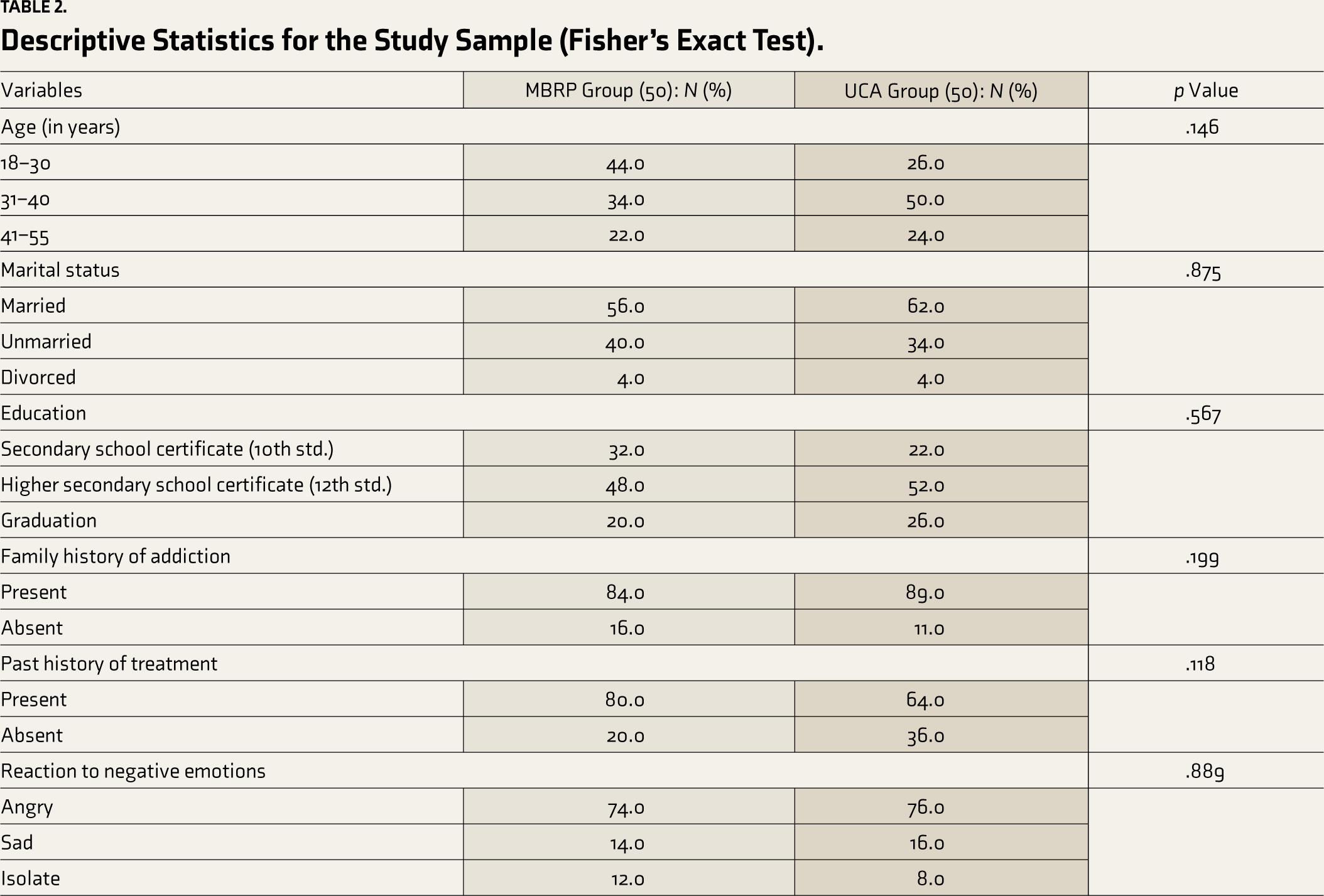
Fisher’s exact test was used for descriptive analysis (Table 2). Age and education levels did not significantly differ between the intervention and UCA groups. Most participants in both groups had a family history of alcohol abuse and a history of treatment. The reactions to negative emotions were similar in both groups, with most participants experiencing relapse due to these emotions.
Descriptive Statistics for the Study Sample (Fisher’s Exact Test).
Comparative Analysis of Intervention and UCA Group Outcomes
To evaluate the effectiveness of the interventions post-treatment, we employed repeated measures ANOVA to compare the outcomes between the Intervention and UCA groups, with a significance level set at p < 0.05. Detailed results, including specific p-values that highlight the differences between the groups at the conclusion of the interventions, are presented in Table 3.
Outcome Status of Both Groups During the Eight-week and Usual Care Follow-up Period (N = 100).
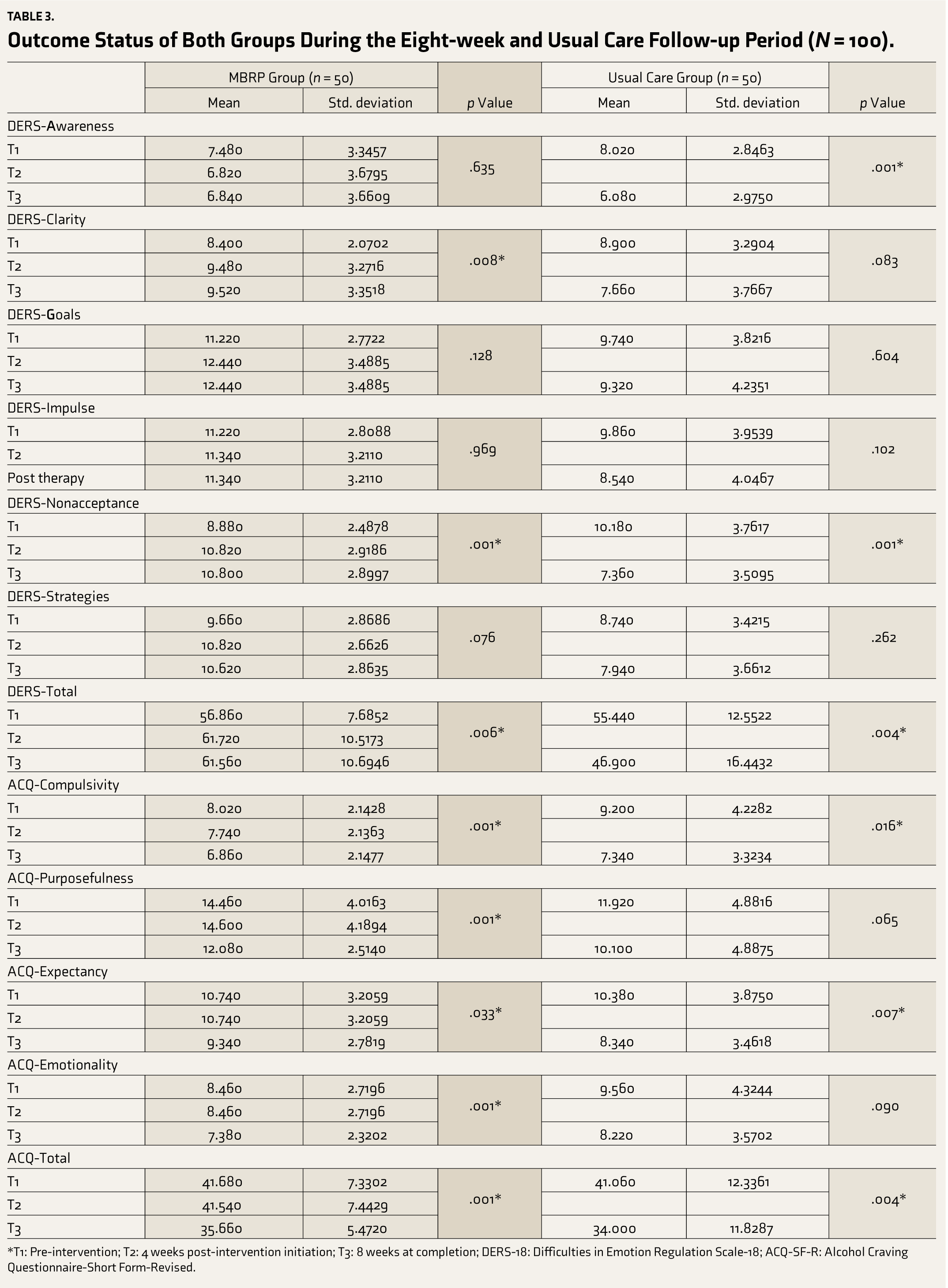
*T1: Pre-intervention; T2: 4 weeks post-intervention initiation; T3: 8 weeks at completion; DERS-18: Difficulties in Emotion Regulation Scale-18; ACQ-SF-R: Alcohol Craving Questionnaire-Short Form-Revised.
Within-group Analysis
Intervention Group
Notable improvements were observed in emotion regulation abilities (p = .006) and reduced alcohol cravings (p = .001). Significant differences were found in emotion regulation subdomains, including total mean score (p = .006), clarity (p = .008), and non-acceptance (p = .001). Various aspects of craving also showed significant differences, including the total mean score (p = .001), as well as compulsivity (p = .001), purposefulness (p = .001), expectancy (p = .033), and emotionality (p = .001).
UCA Group
Significant improvements in emotion regulation (p = .004) and craving reduction (p = .004) were noted. These findings indicate that participants in the UCA group demonstrated notable progress in these areas from the initial assessment to the study’s conclusion. Significant variations were observed within certain specific outcome areas as well. Notably, in emotion regulation, there were substantial changes, including a significant shift in the total mean score (p = 0.004) as well as in the areas of awareness (p = .001) and non-acceptance (p = .001). Similarly, in terms of craving, there were significant alterations, evident in the total mean score (p = .004) and specific elements such as compulsivity (p = .016) and expectancy (p = .007).
Between-group Analysis
The eight-week intervention period showed statistically significant differences between the intervention and UCA groups (p ≤ .05). The intervention group generally demonstrated more substantial improvements, especially in craving-related factors.
Effect Sizes
The effect sizes (Cohen’s d), calculated after the eight-week intervention period, provided valuable insights into the magnitude of differences between the intervention and UCA groups from pre-intervention to post-intervention. In both groups, the effect size of DERS-Total was medium (d = 0.42 for the intervention group and d = 0.50 for the UCA group). The effect size for DERS-Awareness was small in the intervention group (d = 0.15) and medium in the UCA group (d = 0.55), suggesting that the UCA intervention may be particularly effective in enhancing emotional awareness among participants. For DERS-Clarity, the intervention group showed a medium effect size (d = 0.48), compared to a smaller effect size (d = 0.29) in the UCA group. The effect size for DERS-Goals was small in both groups (d = 0.23 for the intervention group and d = 0.09 for the UCA group). The effect sizes for DERS-Impulse were also small in both groups (d = 0.05 for the intervention group and d = 0.27 for the UCA group). A medium effect size was observed for DERS-Nonacceptance in both groups (d = 0.59 for the intervention group and d = 0.63 for the UCA group). Lastly, the effect sizes for strategies were small in both the intervention group (d = 0.26) and the UCA group (d = 0.19).
Regarding the Alcohol Craving Questionnaire (ACQ) subscales, the intervention group showed a significant effect size for ACQ-Compulsivity (d = 0.99) compared to a medium effect size in the UCA group (d = 0.38). The effect size for ACQ-Purposefulness was significant in the intervention group(d = 1.13) and small in the UCA group (d = 0.30). Both groups exhibited small effect sizes for ACQ-Expectancy (d = 0.46 for the intervention group and d = 0.45 for UCA). For ACQ-Emotionality, the intervention group had a medium effect size (d = 0.69), while the UCA group had a small effect size (d = 0.27). The total craving score also showed a significant effect size in the intervention group (d = 1.43) versus a small effect size in the UCA group (d = 0.47).
These results suggest that both groups experienced improvements in emotion regulation and alcohol cravings; the intervention group generally showed more substantial improvements in specific aspects, especially in craving-related factors.
Evaluation of Change
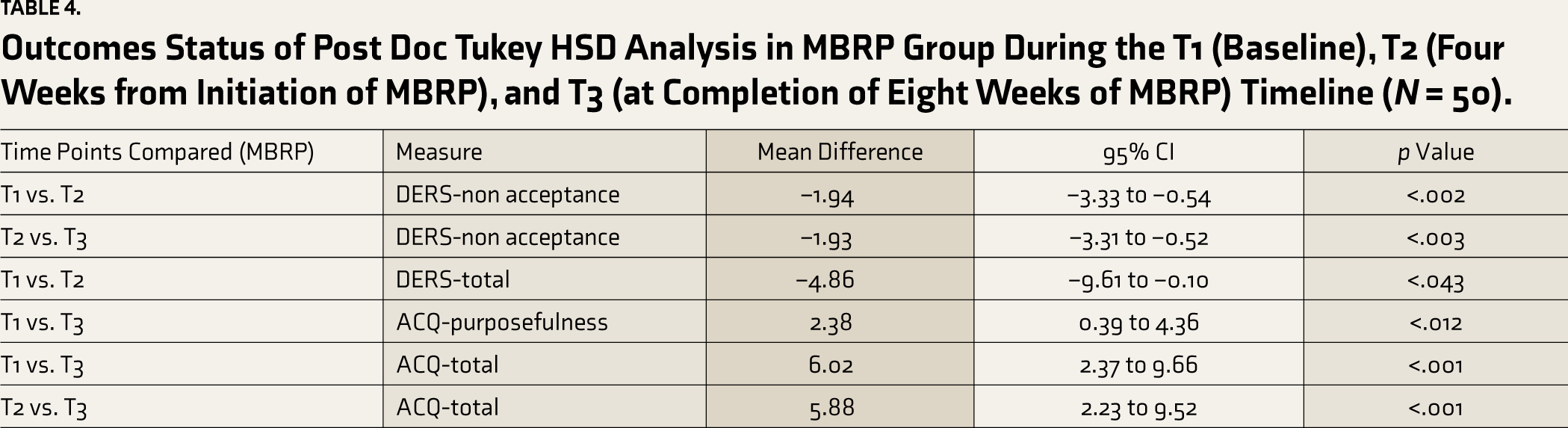
We conducted a post hoc Tukey HSD analysis to examine the differences between the timelines T1, T2, and T3 in the intervention group. For a detailed overview of the significant differences observed at these time points, including mean differences and confidence intervals, please refer to Table 4.
Outcomes Status of Post Doc Tukey HSD Analysis in MBRP Group During the T1 (Baseline), T2 (Four Weeks from Initiation of MBRP), and T3 (at Completion of Eight Weeks of MBRP) Timeline (N = 50).
Discussion
The study evaluated the impact of MBRP on emotion regulation and alcohol cravings in individuals with ADS. We observed that both the intervention group and the UCA group experienced improvements in emotion regulation and alcohol cravings. These results are significant as they indicate the potential benefits of both interventions in addressing critical aspects of ADS. The intervention group exhibited notable enhancements in craving-related factors, aligning with the intervention’s focus on mindfulness techniques for craving management. Additionally, both groups showed medium effect sizes for the DERS-Total score, suggesting that while the mechanisms of change may vary between the mindfulness-based approach of the intervention group and the standard care provided to the UCA group, both approaches can effectively address challenges in emotion regulation among individuals with ADS. This further underscores the effectiveness of standard care, including psychoeducation and individual counseling, in improving emotion regulation and reducing cravings. The improvements observed in both groups highlight the importance of comprehensive care in treating ADS and warrant further investigation into the distinct mechanisms driving these changes. In settings where specialists in MBRP are unavailable, the usual care may serve as an effective management. While usual care offers standard care, MBRP provides a specialized approach focusing on mindfulness and relapse prevention.
The present study’s findings align with those of Witkiewitz et al., indicating that targeted mindfulness practices can assist individuals in effectively monitoring and managing cravings. These results highlight the potential value of MBRP in addressing alcohol cravings and supporting individuals in reducing their desire for alcohol. 9 Consistent with current findings, a systematic review by Sancho et al., found that mindfulness-based interventions have demonstrated efficacy in reducing dependency, craving, and other symptoms associated with addiction while improving mood and regulating emotions. 21 Our findings support the potential efficacy of mindfulness practices in managing cravings over time. The observed improvements in craving-related factors among participants in the mindfulness-based intervention group suggest that mindfulness techniques can offer valuable tools for individuals struggling with cravings associated with ADS. By helping individuals develop awareness of their cravings and providing strategies for managing them, mindfulness practices can contribute to long-term craving management and relapse prevention. This underscores the importance of integrating mindfulness-based interventions into comprehensive treatment approaches for ADS. Combining mindfulness-based interventions with usual care or other active treatments has shown to be the most effective approach.
The study by Caselli et al. supports the current findings, demonstrating that mindfulness practice significantly reduces distress and alcohol urges. 33 It highlights the effectiveness of mindfulness interventions in reducing negative emotions and the desire for alcohol. Additionally, Tapper’s review analysis supports mindfulness’s positive impact on reducing alcohol-related distress and the urge to use alcohol, reinforcing the effectiveness of mindfulness-based interventions in addressing cravings and promoting healthier coping mechanisms. 12 Iranshahri and Jenaabadi’s study aligns with current findings, showing mindfulness therapy’s significant effectiveness in controlling cravings during addiction treatment and promoting healthier coping mechanisms for addiction. 34
Goldberg et al. identified craving as a significant factor in addiction relapse. 26 Ardame et al. reported a significant inverse correlation between mindfulness factors and craving, indicating that higher levels of mindfulness are associated with lower levels of craving. 35 These findings highlight the potential of mindfulness-based interventions that have demonstrated potential in addressing addiction and relapse factors, emphasizing the importance of integrating mindfulness skills into treatment programs. Historical Buddhist teachings align with contemporary research, such as Tapper et al., supporting mindfulness to overcome cravings and reduce addiction-related suffering. 12 The reduction in cravings observed in this study may be attributed to increased mindfulness and heightened awareness of sensations, thoughts, and emotions associated with craving. The development of acceptance and non-reactivity toward cravings likely contributes to these positive outcomes. 26 According to Marks, gradual exposure and non-reactivity cultivation can result in habituation and decreased intensity of craving responses. 36
Furthermore, this study aimed to examine the effects of MBRP on emotion regulation in individuals with AUD. Results showed a moderate improvement in clarity, indicating enhanced understanding and acceptance of emotions. Mindfulness impacts emotion regulation through another mechanism: mindfully noticing one’s emotions and articulating the internal experience using language. 37 This practice facilitates the augmentation of emotional clarity and fosters the development of the realization that emotions are temporary and distinct amalgamations of sensations and thoughts. 15 Consequently, individuals may accept their emotions without automatically reacting to or evading them. 38 Mindfulness-based interventions and similar therapies emphasize the importance of understanding and labeling emotions to develop practical emotion regulation skills. 39 The verbal expression of emotions plays a crucial role in emotion regulation. 38 Skillfully describing one’s inner experience allows effective down-regulation of negative emotions, influencing one’s experience and expression, while difficulties in describing inner experiences may lead to suppression or avoidance.24,40
Moderate improvements in emotion regulation in both the intervention and UCA groups may be attributed to the therapeutic techniques employed in both interventions. The ability to skillfully describe one’s inner experience, a skill of mindfulness practices, psychoeducation, group therapy, and individual counseling, emphasized in both groups, can serve as a means to effectively down-regulate negative emotions, allowing individuals to exert influence over their emotional experiences and expressions. Long-term mindfulness therapy, as well as the techniques used in UCA, may be necessary to restore and normalize emotional regulation in individuals with ADS.
This study acknowledges several limitations that may impact the interpretation and generalizability of its findings. One potential limitation of this study is the relatively small sample size, which may limit the generalizability of the findings to a larger population. Additionally, the study relied on self-reported measures subject to recall and response biases. Furthermore, the absence of a follow-up assessment restricts the ability to assess long-term effects or changes over time. Moreover, the non-randomized design and convenience sampling method limit the ability to draw causal inferences and may introduce selection bias. The overlap in treatment components between the intervention group and UCA groups may also confound the interpretation of the specific effects of MBRP. Lastly, the inclusion of only male adults in the sample may limit the generalizability of the findings to other genders and age groups. These limitations emphasize the crucial role of future research in addressing and overcoming these constraints, ultimately enhancing our comprehension in this field. The findings of this study imply that MBRP might contribute to enhancing emotion regulation and reducing alcohol craving in individuals diagnosed with ADS; it is essential to acknowledge that this study is exploratory. The quasi-experimental design and the context of the Indian population limit the generalizability of the results. Therefore, caution should be exercised in interpreting the findings, and they should be viewed as preliminary evidence supporting the potential benefits of MBRP in this population.
While our study has demonstrated significant changes in most outcome measures in both groups, it is important to interpret these findings cautiously. Our study’s limitations, including the quasi-experimental design, convenience sampling method, reliance on self-reported measures, and potential overlaps in treatment components between both groups, may impact the generalizability and interpretation of our results.
Conclusion
The above findings suggest that MBRP shows promise in addressing emotional regulation difficulties and managing cravings in alcohol addiction. One of the most important aspects of handling cravings while abstaining from alcohol appears to be the individual’s ability to recognize and label different feelings and use appropriate coping mechanisms in times of stress. However, it is essential to note that these results are preliminary and should be interpreted cautiously. Further studies with more rigorous designs and controls are needed to confirm and extend the effectiveness of MBRP in this context.
Footnotes
Acknowledgements
We appreciate Dr. Gopinath M., Opto Research Consultancy Services, for their expert research support that significantly enriched this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Ethical approval was provided by the Ethical Committee, Faculty of Behavioral Sciences, SGT University, Gurgaon, Haryana.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from all participants before the commencement of the study.