
Abstract
Background:
Traumatic experiences in an early phase of an individual’s life stand out as a highly influential risk factor for poor developmental outcomes. Studies examining poor childhood experiences revealed childhood trauma linked to a negative impact on mental health. Therefore, the objective of this study is to comprehend and investigate the subjective childhood experiences of the affected children.
Methods:
A qualitative approach was adopted to explore the lived experiences with their consequences. The study employed a purposeful sampling technique to choose adolescents who had encountered abuse and were capable of articulating their experiences with clarity. In-depth interviews were carried out with 18 adolescents aged 13–18 years, all from childcare homes (mean = 16, SD = 1.46). The transcriptions of these interviews were analyzed using a thematic approach.
Results:
The analysis indicated that the children experienced physical abuse, sexual abuse, rape, abandonment, and neglected home environment. The children took responsibility for the abuse directed toward them and were also engaged in substance use. They further reported experiencing negative effects on their behavioral functions (anger, isolation), cognitive function (difficulty in concentration, low academic performances), emotional function (fear, helplessness), social function (withdrawal, mutism), and biological function (sleeplessness, lack of appetite) due to the adverse events in their life. Perceived needs, for instance, emotional, social, and educational support and positive relationship, as well as growth from traumatic experiences were stated by the children.
Conclusion:
The findings of the study could have practical implications for clinicians, aiding in the understanding of low emotional expression and unexplained behavior among individuals and assisting in addressing the underlying vulnerability to facilitate their overcoming of these challenges. Additionally, it is suggested that a comprehensive strategy be used that addresses stigma, cultural values, and social norms in addition to legal issues to address the problem.
Experiences of adversity during childhood result in trauma that impacts the holistic development of individuals. Such children encounter disruptions in various aspects of their well-being, including their behavioral, cognitive, emotional, social, and biological functions. Childhood trauma has been linked to feelings of self-blame and engagement in substance use. Children articulated perceived requirements, for instance, social support, emotional support, and positive relationship. They expressed personal growth stemming from traumatic experiences.Key Message:
Experiencing trauma during the early stages of an individual’s life stands out as a highly influential risk factor, contributing to adverse developmental outcomes and elevating the likelihood of psychological consequences throughout the lifespan.1,2 Research indicates that children who face adversities such as child maltreatment often lack access to proper nutrition, care, and educational opportunities compared to children in more prosperous regions or economies.3,4 However, it is important to note that these findings may not be generalizable to low- and middle-income countries (LMICs) like India. In India, millions of children may confront unique adversities such as conflict, community violence, and other traumatic life events. 5
Studies examining the effects of early childhood adversity in India have been relatively scarce, including a shortage of comprehensive research. 6 These adversities, which can encompass abuse and neglect, as well as associated behaviors like early smoking or drinking initiation, can have enduring repercussions on both physical and mental health throughout an individual’s life, potentially leading to mortality. 7 Furthermore, these adversities can be worsened by various factors, including socioeconomic status, poverty, urbanization (with disparities between rural or slum areas and urban zones), and even caste distinctions, 8 domestic violence, and assault by peers, which are associated with a series of psychological consequences, problematic behaviors, social problems, cognitive problems, and psychotic symptoms.9–15 Furthermore, while describing traumas, big trauma involves life-threatening events such as war and sexual abuse, which are more intense. Small trauma involves personal events such as bullying and punishments. Both these types can have adverse effects on the individual. 16
However, multiple and diverse types of traumatic incidents experienced by adolescents are referred to as cumulative trauma.17,18 Different types of childhood trauma might often co-occur within the same time frame such as witnessing domestic violence and physical abuse, 19 or child physical abuse and maltreatment. 20 It should be considered that 66% of children aged 2–17 years reported experiencing 2 or more types of trauma and 10% of them reported being exposed to more than 10 types of trauma associated with structural changes in the brain, which leads to stunted brain development.21,22
It has been estimated that one-third of the world’s population has experienced trauma during their lifetime, where one in five children in the world belong to India.23,24 According to the World Health Organization and a report of the National Crime Report Bureau, there was a 53.2% increase in crime against children from 2007 to 2017 in India due to their dependency, vulnerability, and relative social invisibility, with growing concern in specific areas such as abduction, abandonment, procuration of minor girls, and child marriage.25,26
Additionally, despite the government’s laws and policies, there has been a consistent increase in crimes against children in Assam over the past few years, as stated by the Assam Minister for Finance and Social Welfare. 27 Ensuring the safety of children from physical, emotional, and sexual abuse remains a significant concern in Assam, India. Harmful practices such as child marriage, child labor, and child trafficking persist, posing a serious threat, underscoring the urgent need to prioritize the protection of vulnerable children. 28
In her book Bitter Chocolate, 29 Virani explores the backdrop of these challenges within India. She delves into a society characterized by a strong patriarchal culture where practices like reprimanding, punishing, or physically disciplining children are considered cultural norms. 30 Moreover, India’s economic landscape is shaped by various external challenges stemming from its rapidly growing economy, pronounced urban–rural disparities, religious tensions, and geopolitical uncertainties.
It is not surprising that physiological and neurobiological research has revealed that adversities such as child maltreatment can induce alterations in neural networks and hinder the development of the nervous, endocrine, and immune systems, resulting in physical, mental, and emotional dysfunctions, as well as chronic physiological harm. 31 Examining these less-explored facets of childhood trauma is crucial for cultivating a comprehensive understanding. The study, therefore, seeks to contribute to the currently limited knowledge on childhood trauma while simultaneously delving into and elucidating the subjective experiences of individuals who have been victims of such trauma during their formative years. Additionally, this research places emphasis on comprehending the psychosocial challenges and repercussions across diverse domains that children face, rather than exclusively focusing on predicting adverse outcomes in adulthood. The study aims to explore the experiences and perspectives of children undergoing different forms of abuse. The overarching objective is to ascertain the prevalence of childhood trauma and to elucidate the varied experiences and perspectives of children subjected to different forms of abuse
Methodology
Study Design
An exploratory qualitative research design with a thematic analysis was adopted for the study between 2022 and 2023 over a period of six months within childcare homes specialized for vulnerable children. Seven government organizations were selected for data collection by the State Child Protection Service, Assam, No. SCPS(G)217/2015/124. The organizations were: Butterfly Children’s Home, Nabajiban Children’s Home and Children Home for Girls (Nagaon), Children Home for Girls and Children Home for Boys (Kamrup), Gramya Unnayan Sangstha (Morigaon), and SOFTSEED Child Home (Sonitpur). Researchers who embarked on this inquiry possessed specific attributes such as empathy, active listening skills, and cultural sensitivity that enabled them to establish trustful relationships with traumatized child participants and navigate their narratives with care and respect. Furthermore, researchers remained acutely self-aware, recognizing their own biases, emotions, and assumptions that may influence the research process, ultimately shedding light on the intricate experiences of children affected by trauma.
Study Sample
Based on age, gender, and exposure to traumatic events, purposive sampling was performed to identify 18 youth, belonging to the age group 13–18 years from childcare homes (mean = 16, SD = 1.46). Additionally, all participants willingly continued their participation in the study; none declined to drop out. The purposive sampling method was employed to select children who had experienced at least two traumatic incidents and were residing in the institution for a minimum duration of three months, to ensure that they had not undergone any therapy as such. Children undergoing any therapeutic assistance were not included in the study. The children had no other mental health issues as assured by the caretakers. All the participants cooperated in the interview process. Qualitative studies can reach saturation at a relatively smaller sample size. Within a qualitative paradigm, qualitative research allows for in-depth exploration of the unique and complex experiences of traumatized children. It goes beyond quantitative data, giving the children a voice to express their thoughts, feelings, and perception.
Data Collection Method and Setting
After the study was approved by the Institutional Ethics Committee during the year 2022, in-depth semi-structured interviews were carried out in person to gather primary data to explore the lived experiences of abused children. Interview questions were prepared based on the literature review and the objective of the study. In order to build rapport with the children, a week was spent with them in each of the shelter homes before collecting the data, which assisted in building trust as well as collaboration. Additionally, they were made clear about the purpose of the study before the data collection procedure was initiated.
None of the respondents’ interviews followed a set format. Depending on the respondents and their perspectives on the subject, questions were asked in a different order and style. The semi-structured questions were provided with prompts to guide them with their answers. The interview lasted for around 45 min to 1 h. The study is a part of a PhD research work, and a pilot study had been conducted prior to the current study.
The goal of these free-floating interviews was to elicit the following data: depending on the interview’s flow, each participant was interviewed face-to-face and all participants were Assamese speaking. The interviews were audio-recorded for accurate interpretations and analysis. Saturation of data was discussed since we began to notice a repetition of concepts, or information, and new data no longer provided additional insights or perspectives. Data collection was done within the childcare institutes. Special rooms were provided in each of the institutes, and nobody except the interviewer and the participant was there, to maintain some privacy and confidentiality during the study. No repeat interviews were carried out.
Some of the interview questions, for instance, were: Could you describe your family structure and upbringing? Have you experienced any traumatic events during your childhood? Can you share any specific incidents or situations that you consider traumatic from your childhood? How did these childhood traumatic experiences affect you emotionally, mentally, and physically? Have you found ways to heal and grow from your childhood trauma experiences?
Data Analysis
The researchers adopted a realist perspective, assuming that participants’ language accurately represented their experiences, meanings, and realities. The first author initiated the translation process. Subsequently, second and third authors verified the accuracy of these translations. NVivo was used, but no proper findings were identified; therefore, themes were extracted manually. Content analysis was performed using a thematic analysis framework; a qualitative analytical method was chosen for its ability to reveal both commonalities and differences among participant groups. After the interview, the primary authors reviewed the recorded data and transcribed it accurately in a Word document, then subsequently cleaned them to eliminate any unidentified information. Two faculties assisted in the process of data transcription. Each interview was treated as an independent unit of analysis, and significant segments within each text were identified and transformed into initial codes. These codes were developed through an inductive process involving multiple readings of the transcripts, during which patterns of reported motivations and participant reactions were noted. The codes underwent several revisions during the testing phase, which included coding randomly selected interviews, and they continued to evolve throughout the entire data coding process. Any discrepancies observed in interviews that were double-coded were reviewed, and consensus was reached to resolve any inconsistencies.
Themes were then identified to facilitate the organization and summarization of participants’ experiences and to connect these findings with prior research on substance use initiation, aiding our understanding of their relevance for substance abuse prevention efforts.
The two faculties were allowed to review the findings to ensure the perspectives were accurately represented; later on, the arguments were thoroughly reviewed. At the end of the interview session, the participants provided their positive feedbacks, venting their emotions and expressing the sense of presence of someone who was there to lend an ear to their hidden stories
Results
The thematic analysis of the interview allowed us to pinpoint distinct major themes, which are presented along with illustrative quotations.
Almost 12 youth participants experienced five or more traumatic events, four of them reported four traumatic events, and two reported three traumatic events in their lifetime. Youth participants reported being exposed to several types of violence, including seeing a friend or family member die, being in a combat situation, being forced to be apart from family, being raped, and parents’ lack of interest in providing access to basic necessities such as food, shelter, school activities, and medical treatment. According to the qualitative investigation, traumatic stressor exposures happen at the individual, family, and community levels. Participants were from both urban and rural population with lower socioeconomic status.
Participants’ experiences fell into four main categories: physical violence, sexual violence, neglect, and domestic violence.
Physical Abuse
Participants reported being physically injured from a very young age in different conditions. They felt fear in relation to being physically abused in different circumstances by father, relatives, and house owners.
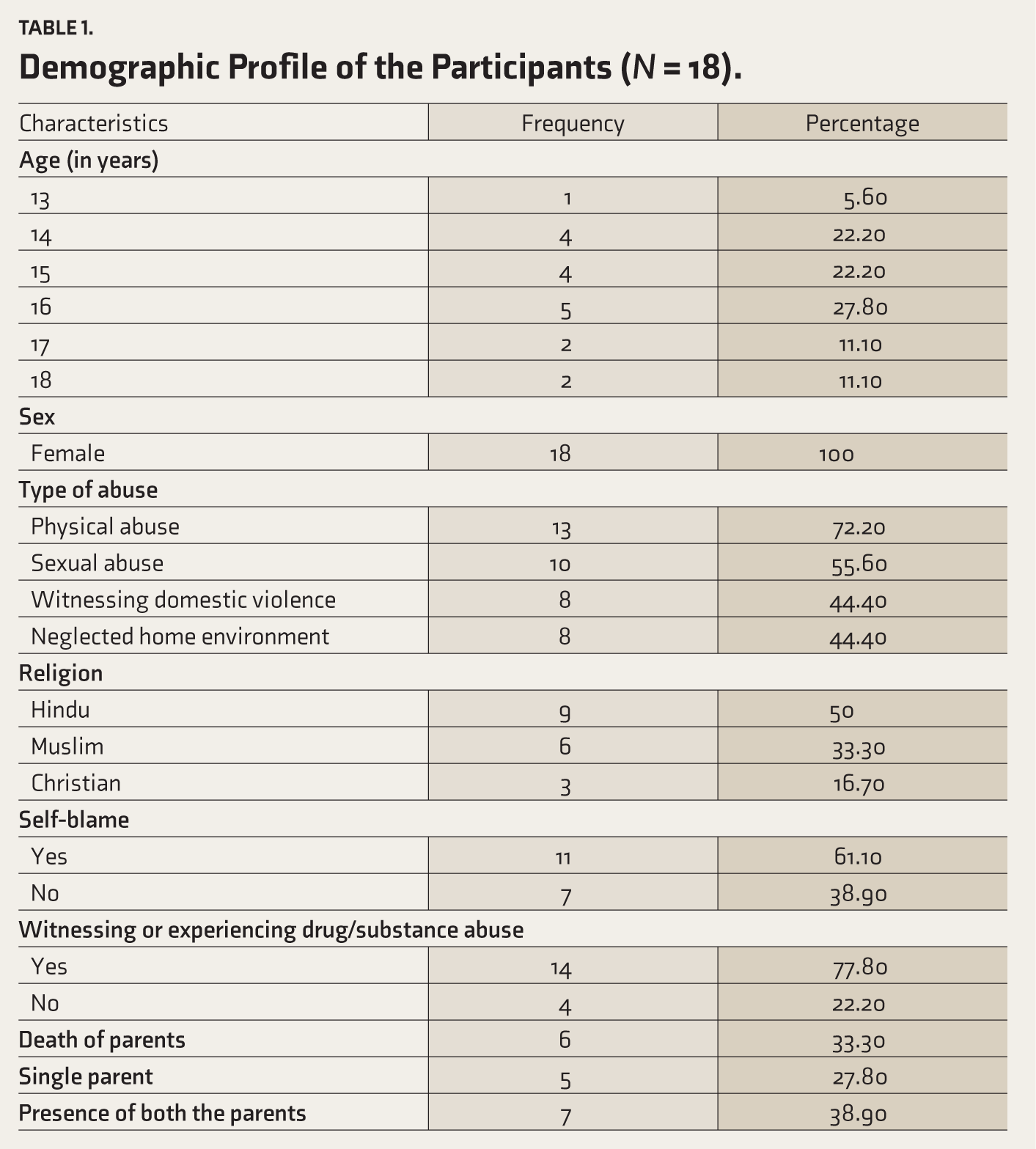
Table 1 delineates the demographic attributes of the research subjects, furnishing essential details regarding age, gender, types of abuse, religion, and other pertinent variables. Female participants aged 13 to 18 years were encompassed in the study. A majority of them encountered physical violence, succeeded by instances of sexual violence, witnessing domestic violence, and exposure to a neglected home environment. Additionally, 11 of the participants attributed blame to themselves for the abuse. Moreover, 14 individuals reported witnessing or experiencing drug/substance abuse.
Demographic Profile of the Participants (
A participant reported,
I was beaten up by my drunken father every day. Even my mother got slaps and punches along with me. There would be bruises everywhere on face, hand, leg. We both wanted to run away at times, but could not due to my grandparents, or else they would be left alone. I always have to live in fear of death.
However, physical abuse by house owners was harsher. The children who served as helpers were predominantly victims of physical abuse, experiencing daily anticipatory fear as a result. For instance, children were worried about being ambushed or, in a more general sense, fretful ruminations about potential yet unaddressed harmful effects.
I was scared that I would be beaten up by the aunty where I stayed. I always keep worrying that she would be waiting to hit me and kill me around the corner at a slightest mistake. So, I have to work with perfections every day. Even she once hit me so hard that my tooth fell off.
At the time, I did not quite have the guts to defend myself; I did not really dare, and I was a little afraid of the consequences that would come as a result.
Now and then, I would shiver, vomit, and was even hospitalized as I was unconscious.
At times, the children showed helplessness and hopelessness, as they had no one else as well as nowhere else to go, thereby ending up tolerating the abuse. The abuse paves the way for developing various psychological problems and poor mental health development such as anxiety and sadness.
Sexual Violence
Poverty within families is a significant factor in the development of sexual violence and abuse against women. For instance, a study of 2,410 women discovered that unemployment and the absence of women’s income increased their susceptibility to male sexual abuse and violence.
32
A participant reported,
We belong to a poor family. So, to meet our needs I have to work as a housemaid since a very young age. There I was frequently assaulted by the owner. I was uncomfortable with the inappropriate touch. I used to cry alone. Even thought of killing self and later had to run away, since things got worst.
One girl perceived herself as psychologically fragile and questioned the reasons behind this perceived vulnerability. Likewise, another girl expressed a desire to conform to the social identity assigned to her by her peers: “I would feel ashamed. Why me, it hurts me and not the others?”
Another participant reported,
I was in a relationship for 3 months and my boyfriend raped me without my consent. Initially I did not know and was not informing my parents, but after 4 months doctor assured that I was pregnant. I felt ashamed and was keeping myself isolated for a long time. I tried to kill myself. But my family was supportive and has sent me to the shelter home. Even though I was surrounded by lots of people I often felt lonely. I felt like no one understood me. I was a confident girl, but now I feel everything is shattered. I feel myself to be worthless and I am scared of my future. I cannot even talk to my friends or family members. I think I would not be able to make any right decision anymore.
Participants acknowledged feeling resentment for the sexual abusers. According to how they put it, this hatred was a reaction to the aggression they experienced from their abusers, who they believed had engaged in willing cruelty or even sadistic behavior.
I admit hating him, he was aware of what he was doing, because he was not in a trance you know. He enjoyed injuring me, raping me and watching me suffer, therefore I do not feel any obligation to feel sorry for him. I was in pain but he did not stop. Now I am pregnant and never came back to accept me.
Though the participants’ feelings of hatred and aggression would be understood, however, most of the feelings are repressed because of the fear-induced restraints.
Similar results were concluded in a research that was conducted in the Indian state of Madhya Pradesh to document the experiences of sexually assaulted girls. 33 According to the study, girls’ delayed healing and re-traumatization are mostly caused by their families’ extremely strong emotional reactions to learning about the abuse. As a result, the topic of childhood sexual abuse is still taboo in India, where there is a great deal of silence out of fear of embarrassment and rejection from the community.
Neglected Home Environment
Parents are expected to raise their kids, provide them with opportunities to learn and interact with others, encourage their mental and physical development, and assist them in becoming masters of their environment. However, not many families are able to properly handle the taxing situation on an emotional and physical level. According to a study, 20–30% of parents have serious personal issues and/or exhibit bad parenting techniques to the point that their kids are at risk of abuse. 34 Moreover, neglect being the most common type of maltreatment, less is known about it than the other types.
My parents fail to provide basic necessities. They are unable to provide three-time meal. I often fail to wear clean school uniform, as I have only one shirt and pant and do not have any shoe for school. So, I often miss school. Moreover, many a times I have to sleep empty stomach at night. This happens because my father is an alcoholic and spends all his money in drinking, not thinking about his family. My mother ran away with another person, leaving us behind with our grandparents. I am really ashamed of my family and myself.
Children have also reported parental lack of supervision where there is failure in ensuring that the child is engaged in safe activities. Children have even reported parents exposing the child to an unsafe environment and leaving them unattended for a long time.
After my mother died, my father has stopped taking care of me. After some days he married another woman, and my stepmother is least concerned about me. She forces me to go to stay with my uncle, who often beats me after drinking, and they never come to see me for months. I feel very angry and often think of running away or sometimes killing myself.
Domestic Violence
The experience of domestic violence, both seeing violence between parents and personal accounts of being battered by family members, emerged as a recurring theme in about half of the interviews. This is a significant result since youths’ ability to cope with trauma and stress depends on their attachment with their parents and other caregivers. If parents are unable to cope with their trauma, they can limit their children’s ability to cope by acting as a protective factor. A 14-year-old girl describes how she witnessed her parents fighting.
My parents fight very often, and my dad kicks my mother out of the house. They occasionally get into fights when my father is drunk and does not come home on time. My mother shouts at everyone in the home when she is enraged. When they fight and injure one other, they are taken to the hospital for treatment. Later on, there would be no money for food.
Domestic violence definitely has a negative impact on the entire family’s mental health and financial stability. Money that is often used for food, clothing, and education is spent on alcohol and medical treatment.
When my dad is upset or angry, he hits kids, skips meals, and goes to the bar. He knocks food off the table when he returns intoxicated. Dad’s response is not ideal, since he might hurt one of us and then need money to take the injured person to the hospital.
These examples show that children witness and experience various forms of abuse, and they link alcohol use and resource depletion to the violence as well. However, experiencing violence can have a direct impact on mental health and well-being outcomes.
As seen in Table 2, some of the most significant effects of abuse are identified verbatim. The effects on behavioral functioning were manifested as pronounced anger, hypersexual conduct, suicidal attempts, mutilation, isolation, and harming others. Intriguingly, when discussing rage, most participants noted how they would get angry over little things and would use foul language and physically attack their siblings, peers, and occasionally their parents, intending to harm them. Additionally, hypersexuality included actions such as indulging in sexual activity with multiple partners at an early age, erotic talk, and being a people pleaser, in ways that please everyone. They were mostly engaged with adults in an effort to win their love and favor. Participants reported attempting suicide as well 35 using methods such as hanging, consuming petrol, and cutting veins, to escape from the pain and suffering. The participants stated being aloof and isolated. They appreciated alone time and being in their own space. The child’s academic functioning was the most impacted as a result of the considerable dysregulations such as behavioral, biological, social, and emotional functions. 36 This includes difficulty in concentrating, low academic performance, refusal to go to school, and difficulty in remembering things and understanding instructions. In turn, this leads to a general decline in academic performance at school, which is then linked to a loss of self-esteem.
Experiences and Perspectives of Children Undergoing Different Forms of Abuse.
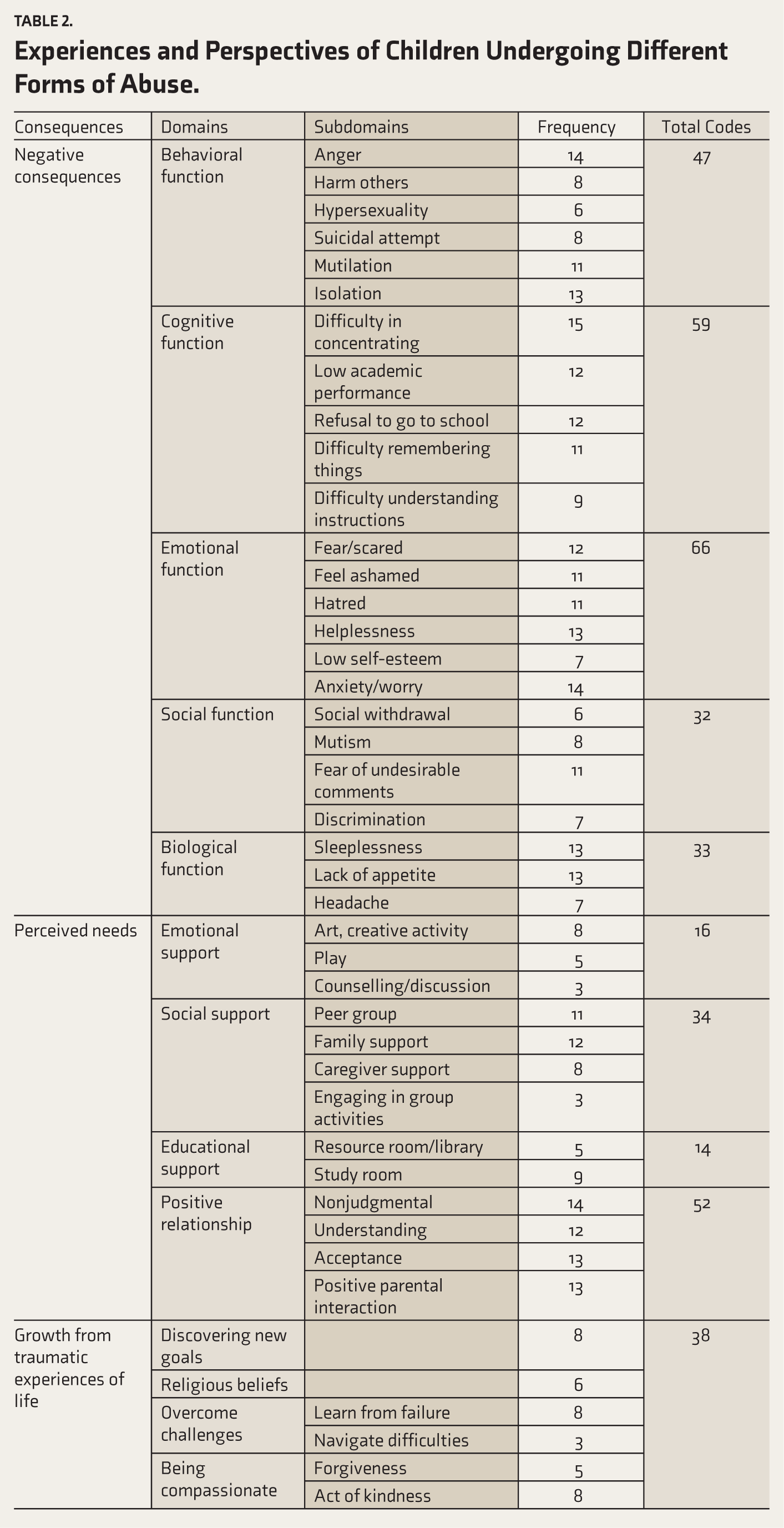
Fear became one of the most often expressed feelings by the children. Because abuse is linked to a lack of trust in other adults, this causes chaos in the lives of those affected and is frequently accompanied by a fear of recurrent abuse. As a result, the world seems to be a perilous place for them. In the children’s reports, there was a sense that everyone posed a threat. As a result, it was discovered that a common result was a generalized terror of adults. Shame is identified as a significant emotion and explanation for delaying disclosure. While shame has been characterized as a crippling sensation in which the self is considered flawed and unworthy, 37 the emotions and thoughts connected to shame revolve around how one is perceived by others, 38 thereby keeping selves isolated and secluded. Similar findings have been discussed about Asian women, where women’s concerns about cultural obligations stemming from “izzat” (family honor/respect and status in the community that will be disrupted upon nondisclosure of sexual abuse), “haya” (shyness of not discussing sexual matters in front of the elders), and “sharam” (means shame—in terms of sinful behavior or conduct that brings shame to the family) are three major factors. 39 The children usually had trouble falling asleep. According to reports, they had trouble starting and keeping up a good sleep for very long. Furthermore, children who faced abuse experienced a lack of appetite as well as headaches due to overthinking the situation.
Children who have experienced traumatic events may have varying requirements. Initial research indicates that emotional support is frequently identified as a primary need among traumatized children. These studies suggest that there is a desire to openly discuss feelings with a trusted individual.40,41 Families could play a critical role in delivering emotional assistance and offering physical comfort, particularly in the context of consoling and reassuring anxious children during medical procedures. Children who have experienced trauma frequently exhibit a yearning for play. Research demonstrated that engaging in play can significantly transform the lives of traumatized children both within their homes and in hospital settings. 42 Shortly after the trauma or even at a later time, children require emotional support, social bonds, and comprehensive information, all of which contribute to mitigating sentiments of abandonment, isolation, and anxiety. 43
Additionally, genuine social support encompasses understanding, empathy, and reciprocal assistance from peers, healthcare and educational professionals, as well as the broader community. In a study, it was revealed that children with brain injuries were inclined to engage with peers who were navigating similar circumstances, allowing them to exchange insights on addressing their challenges. 40 When support was perceived as positive and beneficial, it had a favorable impact on the children’s ability to navigate their traumatic experiences.
Traumatic experiences might in addition yield unexpected positive outcomes and advantages. Amidst trauma, children could attain a realization of the significance and purpose of life; some even exhibit the capacity to transform their experiences into positive tales.43–46 Moreover, trauma could act as a catalyst for establishing fresh life aspirations and proactive strategies to aid those in need, alongside adopting a modified lifestyle.45–47 Additionally, children may undergo a bolstered sense of self-assurance, bravery, and resilience, 46 equipping them with enhanced tools to surmount challenges. 47 Some children found solace in deepened spirituality and a closer connection with their faith through prayer and seeking divine blessings. 48
Discussion
The current study represents one of the first attempts to fully capture the viewpoint of children on the experiences of abuse, how childhood abuse has affected them, and the way they have managed to cope with the consequences. The current investigation revealed multidimensional themes that could serve as valuable insights for healthcare professionals and researchers, aiding them in integrating the most pertinent evidence and crucial concerns identified within these vulnerable groups of children who underwent traumatic experiences. The research encompassed an understanding of the perceived difficulties in everyday life associated with trauma, reactions to traumatic incidents, recognized needs, strategies for managing, and the possibility of individual development arising from these encounters. The review consistently revealed that children who had experienced trauma often found themselves in distressing and challenging circumstances, amplifying their adverse physical, psychological, and behavioral reactions to the trauma while hindering their mental well-being and day-to-day functioning, including self-care activities. These findings underscore the significance of prioritizing the well-being and needs of traumatized children.
Through physical contact and real compassion, parents, caregivers, and peers can help children recover from stressful situations. Children may underline the value of emotional and reciprocal support from family and peers. The distress levels of children can be alleviated through support from peers and other social connections, involving candid sharing, psychological solace, empathy, and reassurance. 49
According to studies on abused and neglected youngsters, they are more susceptible to stressful situations than their peers. For instance, they are aware that they are more likely to be excluded from school and to be the target of bullying. The mental health of a youngster may be impacted by these traumatic events. 50 The traumatic experiences have affected their life and mental health, as well as played a role in developing and maintaining the negative emotions. Children who experience severe stress symptoms typically struggle to control their actions and emotions. They could be clingy, terrified of unfamiliar settings, quickly alarmed, challenging to comfort, and/or aggressive and impulsive. Additionally, they may struggle to fall asleep and lose newly learned developmental skills. 51
The current study’s findings show that children in the age range from 13 to 18 years who were residents of the childcare institutes claimed to have experienced multiple abuses. No discernible difference was found between the age groups in the evaluation conducted to identify those who are at risk of abuse. An estimated 1.6 million children are abused or neglected annually. According to research, 30% of abused children are between the ages of 2 and 5, 40% are between the ages of 6 and 10, and 30% are between the ages of 11 and 17. In other words, children in younger age groups make up approximately 70% of the victims. These statistics were obtained from the judiciary. 52 According to a World Health Organization survey, 23% of children worldwide experienced physical abuse, 36% emotional abuse, 16% physical neglect, and 26% sexual abuse. 53
According to the recently released Global Status Report on Preventing Violence Against Children, 2020, children who experience violence throughout their lifetime have a higher chance of developing mental illnesses and anxiety problems. 54 A study revealed some substantial behavioral alterations in children who had experienced recurrent abuse. The first is the loss of self-esteem demonstrated by the fact that abused children have a bad self-perception, or “poor self-image,” referred by Hjorth and Ostrov, which makes them feel as though they have no choice but to put up with the abuser’s treatment. 55
Traumatized children frequently exhibited adverse reactions and aftermaths in response to trauma. However, conversely, a subset of these children could undergo constructive life transformations post-trauma, encompassing realizations about life’s meaning and viewing survival as an opportunity for improved living. Concurrent with recent research, it has been observed that traumatically affected children may also encounter post-traumatic growth, alongside the aforementioned negative consequences. For instance, a study delineated how traumatic experiences could prompt survivors to fortify their psychological well-being through introspection and surmounting challenges. 56 It is important to acknowledge, however, that post-traumatic growth, while resembling a coping mechanism and a defense against the detrimental effects of trauma, does not inherently mitigate distress, depression, or anxiety levels. 57 The degree of impairments endured by these individuals might hinge on factors such as access to mental health services and protection from cumulative traumatic events. 58 Given the observable stress reactions in traumatized children who experience growth, it is imperative to engage in early screening and recognition of both positive and negative repercussions of traumatic occurrences. Subsequently, appropriate and timely interventions can be devised to amplify or mitigate these impacts, respectively, aiming to bolster their constructive effects while attenuating the adversities.
In the context of interviewing children about their responses to traumatic experiences, it holds considerable significance for gaining insights into their cognitive processes and circumstances. This process often uncovers common subjective encounters and the repercussions of trauma. Nevertheless, eliciting reflections from children, particularly when their life situations entail negative and traumatic aspects, poses challenges due to their limited verbal and conceptual capabilities, recall proficiency, and developmental stage.59,60 When engaging in interviews involving young children, the inclusion of parents can enhance the richness of data, as parents serve as cues for the child and can elucidate interview queries and scenarios. 61 Interviews targeting young children should involve caregivers and prioritize the observation of behavioral manifestations over verbal expressions of their internal states. 62 Furthermore, the utilization of tailored assessment techniques encompassing the examination of both verbal and nonverbal cues, as well as their perceptions and comprehension levels, should be taken into consideration.59,60
In forthcoming assessments and qualitative research concerning children and trauma, it is recommended to employ methodologies that are more tailored and child-centric. Such approaches could encompass preliminary meetings with families to establish rapport and a confidential bond, as well as interviews conducted with individual children or in the presence of their parents based on the child’s inclination.
Limitations and Strengths
Any study that examines child abuse is going to have some methodological flaws. Survivors’ memories of how they dealt with the abuse in the past depend on comprehensive memory recall, and these memories may be skewed or false. Retrospective data may pose challenges because of changes in coping over time. As a result, survivors may not be able to access memories of previous phases of coping methods and may only remember more current ones. Moreover, there is a need to explore the role of institutions and systems in perpetuating or mitigating childhood trauma. Institutions such as schools, child welfare systems, and healthcare settings play crucial roles in identifying and responding to trauma. Research should investigate how these systems can be improved to better support traumatized children. During the interview, the children were able to talk openly about their experiences and provided information that could not have been obtained using quantitative methods. Furthermore, this methodology clarified the uses and characteristics of their experiences, consequences, and coping mechanisms.
Conclusion
In forthcoming assessments and qualitative research concerning children and trauma, it is recommended to employ methodologies that are more tailored and child-centric. Such approaches could encompass preliminary meetings with families to establish rapport and a confidential bond, as well as interviews conducted with individual children or in the presence of their parents based on the child's inclination.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Ethical approval was received from committee of Sikkim University under reference no: SU/REG/F-1/03/2019/Vol-II/890
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.