
Abstract
Background:
The presence of a severe mental illness in the mother during the postpartum period may impact the whole family and specifically have an effect on the health of the spouse. The current study aimed to assess psychological distress, coping, and perceived social support of spouses of women with postpartum onset severe mental illness.
Methodology:
A cross-sectional descriptive research design was used, and 30 spouses of the women admitted to the mother–baby unit (MBU) for psychiatric inpatient care were included in the study. The assessments included sociodemographic details, Kessler psychological distress scale (K10), brief coping orientation to problems experienced scale (brief COPE), and Zimets’ multidimensional scale of perceived social support.
Results:
Around 50% of the spouses experienced severe psychological distress. Nearly 40% of spouses reported poor coping and 56.7% of spouses had moderate social support from family and friends.
Conclusion:
The findings indicate the need to address distress and coping in spouses of women with postpartum onset SMI.
Postpartum psychiatric illness in women can significantly impact mother–infant bonding and the mental health of the spouse. This study revealed that 50% of the new fathers had severe psychological distress, and 40% had poor coping to handle stress following the first episode postpartum psychiatric illness in their partner. It is essential to pay equal attention to new fathers’ mental health and extend support to cope with their partner’s postpartum psychiatric illness.Key Messages:
Postpartum psychosis is a severe mental health condition that often begins immediately after childbirth and is considered a psychiatric emergency. The global prevalence of postpartum psychosis is 0.89–2.6 per 1000 births.4, 5 During the postnatal period, a woman needs an adequate amount of care and support from her husband to overcome psychosocial stressors. 1 The transition to fatherhood appears to increase the risk of stress, anxiety, and depression among men. 6 Moreover, psychiatric illness in the wife affects the husband’s mental state, and paternal mental health is considered a significant public health issue. 7
Research on men’s mental health during the postpartum period is limited with more focus on postnatal depression. Significant psychological distress and severe stress have been reported among 13% and 2% of fathers following childbirth. 8 A population-based study from Brazil on paternal postpartum depression reported that 11.9% of the father’s clinical depression was associated with postpartum depression in their wives. 9 The antecedents for postnatal mental health problems among men are, being a single parent or high parental stress, traumatic childbirth, wife’s illness, lack of social support, and poor financial condition.10–13 The psychiatric condition of wife postchildbirth and cultural practices of families during the postpartum psychiatric illness extends the duration of treatment-seeking and it causes a greater amount of psychological problems among the spouse. The present study examined psychological distress, coping, and social support among the spouses of women with postpartum severe mental illness (SMI).
Materials and Methods
The study adopted an exploratory method under cross-sectional and descriptive research design. It was conducted at the Mother–Baby psychiatric Unit (MBU), where mothers with mental health problems are admitted with their infants till one year of age. Convenience sampling was used to interview the spouses of women admitted to the MBU. The Institute Ethics Committee approved the study (IEC), and subjects were recruited after obtaining written informed consent. Spouses of women with first-episode postpartum onset of SMI with a minimum of one-week duration of illness were invited to participate in the study. Spouses who were able to communicate in Kannada, English, and Telugu language were included. Spouses with a current or past major mental illness those who had applied for legal marital separation were excluded from the study. Psychosocial support was offered to the participants if needed.
Study Tools
The study used demographic data sheet, Kessler psychological distress scale K10, brief COPE (coping orientation to problem experienced) and perceived social support scale for collection of data. The scales were translated to vernacular language Kannada. Independent bilingual experts translated scales from original language (English) to vernacular language (Kannada) and vernacular language to original language, the concept equivalence and errors were checked in original and back translated versions before finalizing instruments.
Background Datasheet
Sociodemographic data sheet was used to collect demographic information of spouses.
The Kessler Psychological Distress Scale (K10) 14
K10 consists of 10 items, with each item having five responses (1–5) on a Likert scale. It measures psychological distress based on anxiety and depression that a person has experienced in the most recent four weeks period. A score of >30 indicates severe psychological distress, 25–29 implies moderate psychological distress, 20–24 indicates mild psychological distress, and a score of <20 indicates no psychological distress. The scale was administered at least after four weeks of onset illness.
Brief COPE (Coping Orientation to Problem Experienced) 15
This is a 4-point Likert scale with 28 items and mentions 2 types of coping. 16 (a) Maladaptive coping comprises of venting, denial, substance use, behavioral disengagement, self-distraction, and self-blame. (b) Adaptive coping includes positive reframing, planning, and seeking social support, active coping, and the use of emotional and instrumental support, acceptance, religion, and humor. In the current study, the majority of respondents had not selected-response three and four for items on the scale; hence, the three and four responses were recoded into response two and response one was considered the same. As the established cutoff range for a brief COPE scale was not available for Indian population, individual item analysis was performed.
Perceived Social Support Scale 17
It is a 7 (1–7) point Likert scale consisting of 12 items and 3 domains, namely, support from family, friends, and significant others. Scoring is done based on the number of items in a domain. A score of 5.1–7 indicates high support, 3–5 suggests moderate support, and 1–2.9 is considered as low support.
Participants
Spouses of postpartum mothers who were admitted to MBU, NIMHANS for treatment of postpartum onset SMI between the periods July 2017 to December 2017 and who fulfilled the study criteria were recruited for the study after obtaining written informed consent. The first author (PCP) administered the tools following training on administration of study tools.
Results
Sociodemographic Profile of Participants
A total of 30 spouses participated in the study. The age range of the spouses was 22–40 years, and the mean age was 31 years ± 4; 13 (43.3%) had higher primary education, whereas 7 (23.3%) spouses had education up to graduation. Around 14 (46.7%) spouses had been married for 1–3 years, and 13 (43.3%) of participants were married for a period 4–6 years. Twenty-two (73.3%) spouses were skilled employees, with 18 (60%) spouses hailing from lower socioeconomic strata, and 19 (66.3%) belonged to rural areas.
Clinical Profile of Mothers
Diagnosis of the women whose spouses were included in the study were 20 (73.3%) women diagnosed to have postpartum psychosis, five (16.7%) women diagnosed with the first episode of mania with psychotic symptoms, and three (10%) with severe depression. The duration of illness was less than 3 months in 21 (70%) mothers; 23 (76.76%) mother’s caregivers reported a history of inadequate bonding with baby during illness.
Psychological Distress and Social Support
On the K10, half of the spouses (50%) had severe psychological distress, and 7 (23.33%) and 4 (13.33%) spouses reported mild and moderate psychological distress respectively. Seventeen spouses (56.7%) had moderate social support from family and friends, and 13 (43.3%) reported high social support.
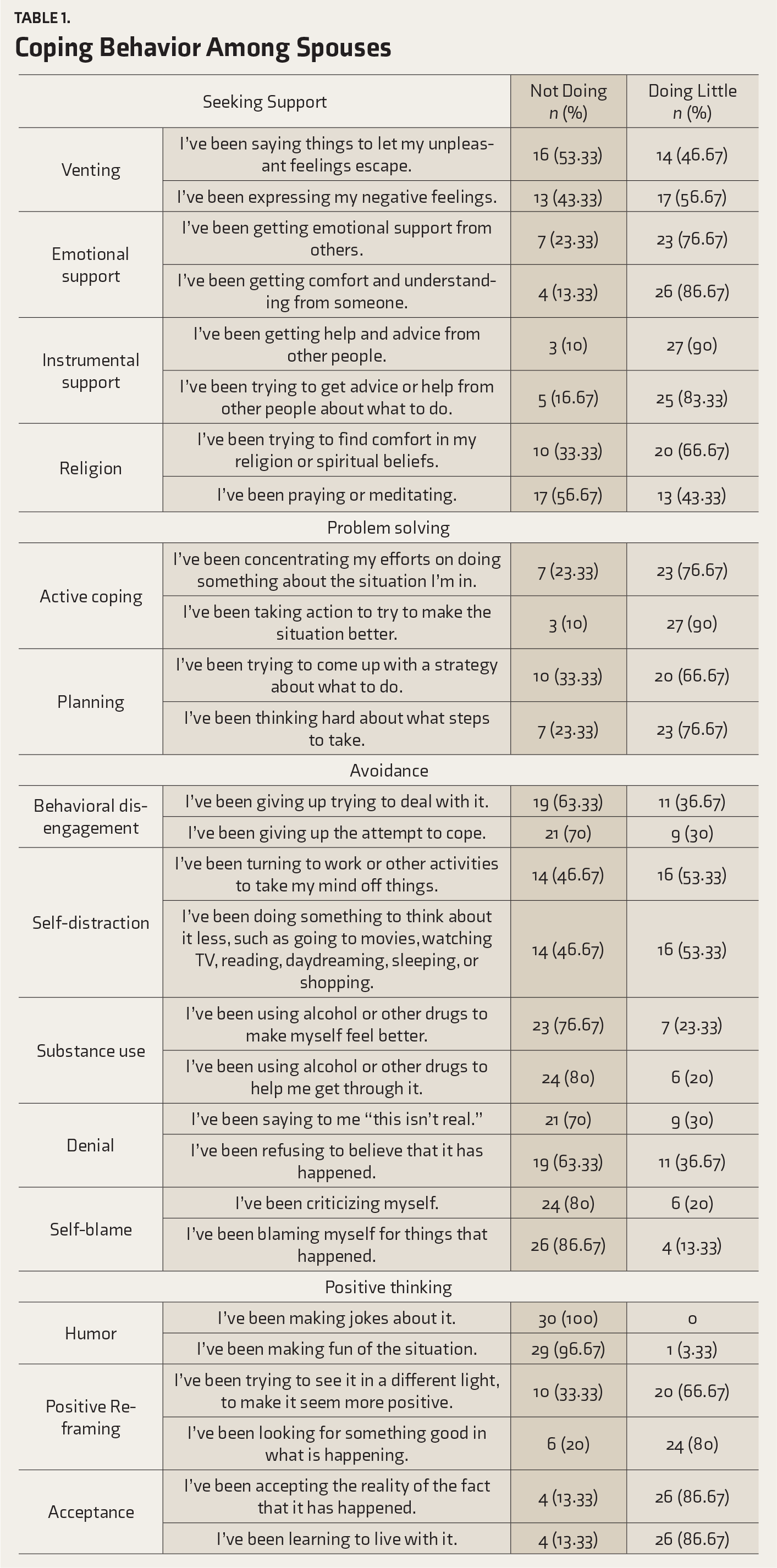
Coping Behavior Among Spouses
Discussion
The current study revealed that 50% of the spouses of women who had first episode of psychiatric illness with postpartum onset had severe psychological distress in the first month. Nearly half of them had moderate social support. A postpartum onset of SMI can have a significant impact on mothers, infants, and their partners as well as family members. The potential factors for increased psychological distress could be wife’s psychiatric illness, the added burden of household chores, work–life balance, changes in daily routine, and multiple roles in family, financial constraints, caring for the new-born, and absence of emotional attachment to wife during illness. 18 A study conducted in Sweden on father’s experiences following perinatal psychiatric illness in the wife found deterioration in relationship with the spouse, difficulties in managing and balancing the household chores, unable to complete the demands of the family, and inability to handle one’s own needs. 19 The incidence of paternal depression has ranged from 1·2% to 25·5% in community samples, with 24% to 50% of spouse’s depression being associated with the wife’s postpartum SMI. 20 A population-based longitudinal study showed a higher level of psychological distress in partners during pregnancy and postdelivery even when mothers did not have mental illness. 21 Current study findings were similar to previously published literature on rates of psychological distress among spouses of new mothers with mental illness. It is essential to address a spouse’s mental health when their wives are being treated for psychiatric disorders postdelivery.
We did not find many spouses who had adopted maladaptive coping. Probably, it was due to the adequate support from family and friends. In this study, 43.3% of spouses reported high levels social support during the wife’s illness, which included instrumental, emotional support, seeking help, and taking advice from friends and family. In contrast, a study from China reported that there was a significant difference in perceived stress and depression among the first time Chinese mother and father. Perceived stress and depression in fathers was significantly associated with the partner’s depression. The authors reported that this might be due to changing roles like baby care, being parent, and one-child policy in China, which has added to the stress in fathers. 22 Taiwanese husbands perceived lower social support, higher stress, and lower self-esteem during the postnatal period compared to their wives. 23 However, in India, the reason for higher social support during the wife’s illness could be due to cultural factors such as family ties, family systems, and family environment. This support to the unaffected individuals reduces the burden, so that they can cope better in a problematic situation.24, 25
A couple’s mental health during the perinatal time is interdependent, and fathers’ positive involvement decreases the adverse outcome of a mother’s mental illness. 26 Despite the finding that a good proportion of spouses reported adequate social support, nearly half of them needed additional help. Regarding coping, majority of spouses had practiced adaptive coping. However, they still had challenges possibly due to inadequate knowledge about the illness, lower self-confidence, poor problem-solving skills, and difficulty in identifying the local resources to use to improve the situation. However, there are no studies conducted in Indian settings on coping among partners during postpartum psychiatric illness in their wives to substantiate the findings.
The major limitation of the study is that it is derived from a psychiatric hospital setting. As sample size is small and limited to postpartum SMI, generalizability of the findings is limited. The small sample size also did not permit us to assess the relationships between psychological distress and other variables such as coping and social support or with illness variables. The study excluded spouses with pre-existing mental illness; however, other confounders such as marital discord, life stressors, and health of infant, which could lead to increased psychological distress, were not studied in sample. It is plausible that subjects regarded participation in this study as an opportunity to express their concerns and to get some kind of support. This study was conducted after the first week or a month of onset of illness, and hence, the levels of distress might still be high. This study also did not assess the severity of the mother’s illness and the health of the infant, which might be factors that contribute to the high levels of psychological distress experienced by the spouse.
Healthy coping and psychological well-being in the spouses are important to enable them to cope with SMI in their wives during the postpartum period. Routine screening for mental well-being of the spouse, psychoeducation, group interventions, and creating spouse support groups need consideration for helping them cope when a wife is hospitalized due to SMI at an important time of a family’s life cycle.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.