
Abstract
Background:
Over the past 30 years, the clock drawing test (CDT) has generated considerable interest due to its usefulness in the early detection of cognitive impairments, particularly those seen in neurodegenerative dementias (including Alzheimer’s disease), vascular dementia, and mixed dementia. The present study aimed to determine whether the results of the “30-Point Clock Face Test” (CFT-30), a standardized version of the CDT that uses a 30-point scale, correlate with those of the Mini-Mental State Examination (MMSE).
Methods:
This is a retrospective, observational study. All patients hospitalized in a Hospital-University Clinic Geriatrics Unit (Grenoble Alpes University Hospital, Grenoble, France), from January 1, 2017, to December 31, 2018, were included. Patient data and scores were retrieved from hospital archives, and the results of the two tests of interest, MMSE and the CFT-30, were analyzed.
Results:
We included 214 patients aged ≥75 years. The mean ± SD age was 86.4 ± 5.6 years, and 68.7% were female. A strongly positive, significant correlation was seen between the CFT-30 and MMSE (r = 0.73, P < 0.001) scores. The total scores obtained by these two tests were identical (t = 1.22, P = 0.22).
Conclusion:
CFT-30 is a good complement to the tools usually used in the investigation of cognitive impairments in older people. In addition to its metrological qualities, the standardized and normalized CFT-30 is extremely simple and very fast to use.
CFT-30 appears to be a good complement to the tools usually used in the investigation of cognitive impairments in older people. The standardized and normalized CFT-30 is extremely simple and very fast to use. It has a strong correlation with the MMSE. Spatial markers (the base and the alarm bell) help to recognize it as a clock more easily and thus allow the objectification of difficulties in conceptualization (semantic disorder: difficulty in imagining the clock face and the hours) from other cognitive deficits (memory loss, visual-spatial disorder, executive function disorder, constructional apraxia).Key Messages:
Even though the multitude of different scaling methods and protocols of administration bring into question the validity of both the CDT and the MMSE, they are still used by many elderly-care facilities. A standardized protocol and method of scoring are essential to be able to share and compare the results of the CDT among different institutions, research groups, and countries. A meta-analysis 3 that examined a variety of scoring methods found the 20-item scoring method proposed by Mendez et al. 17 to be the most pertinent. Another study that compared different scoring methods on a group of patients diagnosed with mild to moderate stages of Alzheimer’s disease found that CDT had a high correlation with the level of cognitive impairment of the patients. 18 The Schulman scoring method 3 was found to be the best in terms of correlation with the level of impairment. Libon et al. 19 correlated the CDT with the MMSE and found that both tests were useful and complementary screening tools to detect cognitive impairment. 20
The “30-Point Clock Face Test” (CFT-30) 21 is a standardized version of the CDT, scored on a 30-point scale. The primary objective of this study was to assess the correlation between the MMSE and the CFT-30, two practical and commonly used tools.
Materials and Methods
30-Point Clock Face Test
The CFT-30 used is a validated and standardized version of the usual clock-drawing cognitive test proposed by the Center for Applied Psychology. 22 This test shows strong correlation (r = 0.77, P < 0.001) 22 with another test commonly used for the older people in France, the “Batterie d’Echelle Clinique—96” (BEC-96) 23 which is known for its sensitivity in detecting cognitive impairment in patients (the correlation between scores obtained by the BEC-96 and the MMSE is very high: r = 0.81, P < 0.001). 23
The CFT-30 is scored on a 30-point scale and can provide different qualitative profiles of cognitive impairment, given the pattern of the scores on the various items. The details of the scoring method are precise and easy to understand. A “threshold” score of 24 points on the CFT-30 gives optimal and highly satisfactory sensitivity (84.8%) and specificity (93.7%), accompanied by an efficiency of 88.2%. 22
Presentation and Instructions
The standardized test sheet proposes a predrawn blank circle (diameter 111 mm) and a central reference point (the axis of rotation of the hands), with a base and alarm bell serving as spatial landmarks (Figure S1). These fundamental reference points are intended to facilitate the recognition of the circle as a clock and also to assist the spatial execution of the test. The base and the alarm bell serve to facilitate the positioning of the cardinal points (12 h, 3 h, 6 h, and 9 h) and help in the division of the face of the clock and the good positioning of the other numbers. The simple and clear instruction is: “This drawing represents a clock face. The numbers indicating the hours are missing. Can you draw them on this clockface?.” The assessor should watch the subject as he/she performs the task so as to see how the subject proceeds. Self-corrections are accepted. The administration of this test takes no more than 2 min.
Scoring
To facilitate the scoring of items, the assessor must first draw two orthogonal lines to determine the correct positioning of the cardinal points (Figure S2).
There are two main dimensions to the scoring grid (Table S1): The first one concerns the “spatial organization” achieved by the patient; and the second dimension is the “ordering of numbers.” All scoring instructions are presented in Table S2.
Use of “Cognitive Profile” and “Clinical Profiles”
For a clinical reading of CFT-30 results, it is recommended to proceed in two stages (Figure S3): First, the assessor must enter the raw scores in the “Cognitive Profile” scoring sheet by ticking the appropriate boxes. Second, he/she should compare this cognitive profile with the clinical profiles. This is not a pathognomonic diagnostic reading, but simply indicative, to help the clinician formulate his/her diagnostic hypotheses.
Patients
This retrospective observational study analyzed the medical files of patients who had been hospitalized in a Hospital-University Clinic Geriatrics Unit (Grenoble Alpes University Hospital, Grenoble, France), from January 1, 2017, to December 31, 2018. While hospitalized in the geriatric unit, when possible, a cognitive assessment of the patient, consisting of the MMSE and the CFT-30, was systematically performed. Among the 252 patient medical files initially screened, 38 were excluded due to missing information or unclear data.
Procedure
We retrieved the medical files of the patients from the hospital archives and extracted the scores of the two tests of interest (the MMSE and the CFT-30) in detail. We also extracted the data on sociodemographic and clinical variables that could have a role in the effect we are looking at, such as age, sex, type of residence, level of formal education, and scores on the daily activity of living (ADL) 24 and the Instrumental Daily Activity of Living (IADL). 25
Ethics Committee
All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation, and ethics approval was obtained on February 20, 2020, from “CECIC Rhône-Alpes-Auvergne, Clermont-Ferrand, IRB 5891.” This study was preregistered at “Clinical Research and Innovation Department” of the Grenoble Alpes University Hospital (France), with Approved Baseline Methodology M004.
Statistical Methods
For statistical analysis, comparisons between data from basic demographic information, MMSE, and CFT-30 scores were performed using descriptive statistics, Pearson r correlation, t-tests for continuous variables; Kendall’s tau and χ 2 tests for categorical ones. The level of significance was 0.05. Analyses were performed using StatView, version 4.0 (Abacus Concepts, Inc., Berkeley, CA).
Results
Characteristics of the Population Studied
The historical cohort (Table 1) consisted of 214 patients (mean age = 86.4 years, SD = 5.6): 67 males (31.3%, mean age = 85.4 years, SD = 5.3) and 147 females (68.7%, mean age = 86.9 years, SD = 5.7).
Before their hospitalization, most of the patients mostly lived at home (home = 90.7%, nursing home = 5.6%, communal housing = 3.7%), and if not, men as well as women had been institutionalized (χ 2 = 2.77, P = 0.26).
The patients seemed to have a certain amount of autonomy in performing everyday activities (ADL, mean = 5.0/6, SD = 1.3), but performed less well in the IADL (mean = 3.2/8, SD = 2.8).
CFT-30 and MMSE
The total scores obtained on the CFT-30 (mean = 20.18, SD = 6.25) and the MMSE (mean = 20.54, SD = 5.57) were identical (t = 1.22, P = 0.22). There was a strong positive and very significant correlation between the CFT-30 and MMSE test results (r = 0.73, P < 0.001).
Impact of the Level of Formal Education
The level of formal education (group 1 = primary education only, group 2 = completed junior high school, group 3 = attended high school) received by the patients (by sex) showed that groups 1 and 2 represent 82.7% of the patients, with men having received slightly more formal education than women (F = 5.44, P = 0.02).
Kendall’s tau showed a significant positive correlation between education level and the CFT-30 (τ = 0.17, P < 0.001) and between education level and the MMSE (τ = 0.20, P < 0.001) results. In addition, the CFT-30 was less influenced by education level than the MMSE. Table 2 shows that for MMSE the difference between the average score of patients in groups 1 and 2 was at the limit of significance (t = −1.7, P = 0.09), whereas this difference was significant between groups 3 and 1 and groups 3 and 2.
For the CFT-30, the mean scores of groups 1 and 2 were identical (t = −0.77, P = 0.44), whereas the subjects in group 3 had a mean score that was significantly higher than that of the other two groups. These results suggest that group 3 scored better than groups 1 and 2, which probably explains the significant, but weak, correlation between education level and MMSE, along with the correlation between education level and CFT.
Impact of Activities of Daily Living and Instrumental Activities of Daily Living
ADL and IADL responses appear to have a positive and significant correlation with both CFT-30 and MMSE results: ADL, MMSE (r = 0.40, P < 0.001); ADL, CFT-30 (r = 0.34, P < 0.001); IADL, MMSE (r = 0.54, P < 0.001); IADL, CFT-30 (r = 0.46, P < 0.001).
Discussion
The CFT-30 appears to be a good complement to the other tools commonly used in the investigation of cognitive impairments in older people.26–29 As the test results are shown graphically, the assessor can detect alterations (impairment or improvement) in the patient’s cognitive processes at a glance, even before calculating the score. The results can be confirmed by the “Cognitive profile” and the “Clinical profiles.”
In addition to its metrological qualities, the CFT-30 is extremely simple and quick to use. 30 These advantages explain its excellent acceptability. 31 Without any time constraint, it rarely makes the person ill at ease. Generally, the person considers this assessment as a simple exercise. He/she does not feel as if he/she is being judged because they do not perceive that the clockface drawing is aberrant, unlike some items in the MMSE (and other cognitive tests) where he/she may feel inadequate when confronted with the inability to verbally express the correct answer.
The CFT-30 provides a rapid and early assessment of visual-spatial deficits and constructional apraxia, 32 objectifies difficulties in spatial organization and logical thought, and can detect deficiencies in attention and executive functions.33, 34 Thus, the CFT-30 has become a psychometric assessment tool that is readily used to evaluate several cognitive functions. Over the past 30 years, the clock test has generated considerable interest due to its role in the early detection of cognitive impairments, 35 particularly those seen in neurodegenerative dementias (including Alzheimer’s disease), vascular dementia, or mixed dementia.
CFT-30 is not a memory test. However, memory deficits can affect the scores in the “numbering” and “sequence” items, without impacting the other items (“strategy”).
In the context of mild cognitive impairment (MCI), although some researchers have opined CDT as not useful 36 or as outrightly dubious, 37 many others agree on its utility in the assessment of these patients.38, 39 Furthermore, this test has proved its usefulness and sensitivity in the differential diagnosis of various types of dementias.40, 41
Contrary to many publications in this field,42–48 the CFT-30 benefits from standardized support (an examination sheet) and a standardized method of rating. It has many advantages:
A standardized predrawn blank clock face, which makes it easy to compare the results both at the intraindividual and interindividual level. A standardized, clear, easy to use, accurate, and easily understandable method of scoring for all assessors, which aims to homogenize the scoring among different assessors. The “cognitive” and “clinical” profiles make it easier to identify efficient or non-efficient cognitive processes, thus helping the assessor to refine his/her diagnostic hypothesis (see examples shown in Figures S4–S9).
Statistical analysis revealed the other qualities of CFT-30: the slight correlation, despite a very low P-value and therefore a statistically significant relationship, with the age of the subjects aged ≥75 (r = −0.18, P = 0.01), which makes it a test of choice for the elderly; the very low correlation with the patient’s level of formal education (CFT-30 appears less sensitive to the level of formal education than other neurocognitive tests);close correspondence with the BEC-96 (sensitivity at 84.8%, specificity at 93.7%, and efficiency at 88.2%), and a strong positive correlation with the MMSE (r = 0.73, P < 0.001).
This easy, fast, and standardized test deserves to be an international reference among the various CDT available in the field of cognitive assessments and early detection of dementia (Alzheimer’s and other dementias) in older people.
CFT and MMSE may be complementary, as the CFT assesses executive function, whereas MMSE does not assess executive function adequately. However, CFT may not replace the requirement for tools for brief cognitive assessment like MMSE.
Finally, CFT may be perceived as less complex than MMSE. However, it may not be useful in low- and middle-income settings with higher levels of illiteracy that will limit the use of pen or writing numbers.
Study Limitations
This retrospective study did not take into account the pathology that motivated the hospitalization of the subjects in a geriatric department. Nevertheless, this study has the merit of demonstrating the use, scoring, and interpretation of the CFT-30 (a standardized and normalized test) and its strong correlation with the MMSE. This promising result encourages us to conduct a multicenter prospective study of the relative diagnostic and differential capacities of the CFT-30 versus the MMSE in older people with neurocognitive impairments (particularly dementias).
The frontal assessment battery (FAB) 49 is not regularly used in our center. For future studies, a combination of the FAB and the MMSE would provide a more complete cognitive picture than the MMSE alone, as any functional impairment of the frontal lobe may be present with relatively normal scores in MMSE but give significant results in the CDT.
In addition, the correlations between education level and MMSE, and between education level and CFT-30, are weak because we used the level of formal education as “educational categories” (group 1, group 2, group 3) and not as “years of education” (continuous variable), which considerably reduces the number of values this variable can take. 15 The exclusive use of years of education, therefore, seems more appropriate during statistical analyses in the context of cognitive tests. This finding is crucial and should now be considered in all future studies on the impact of the level of formal education on cognitive assessments.
Characteristics of Study Participants (N = 214)
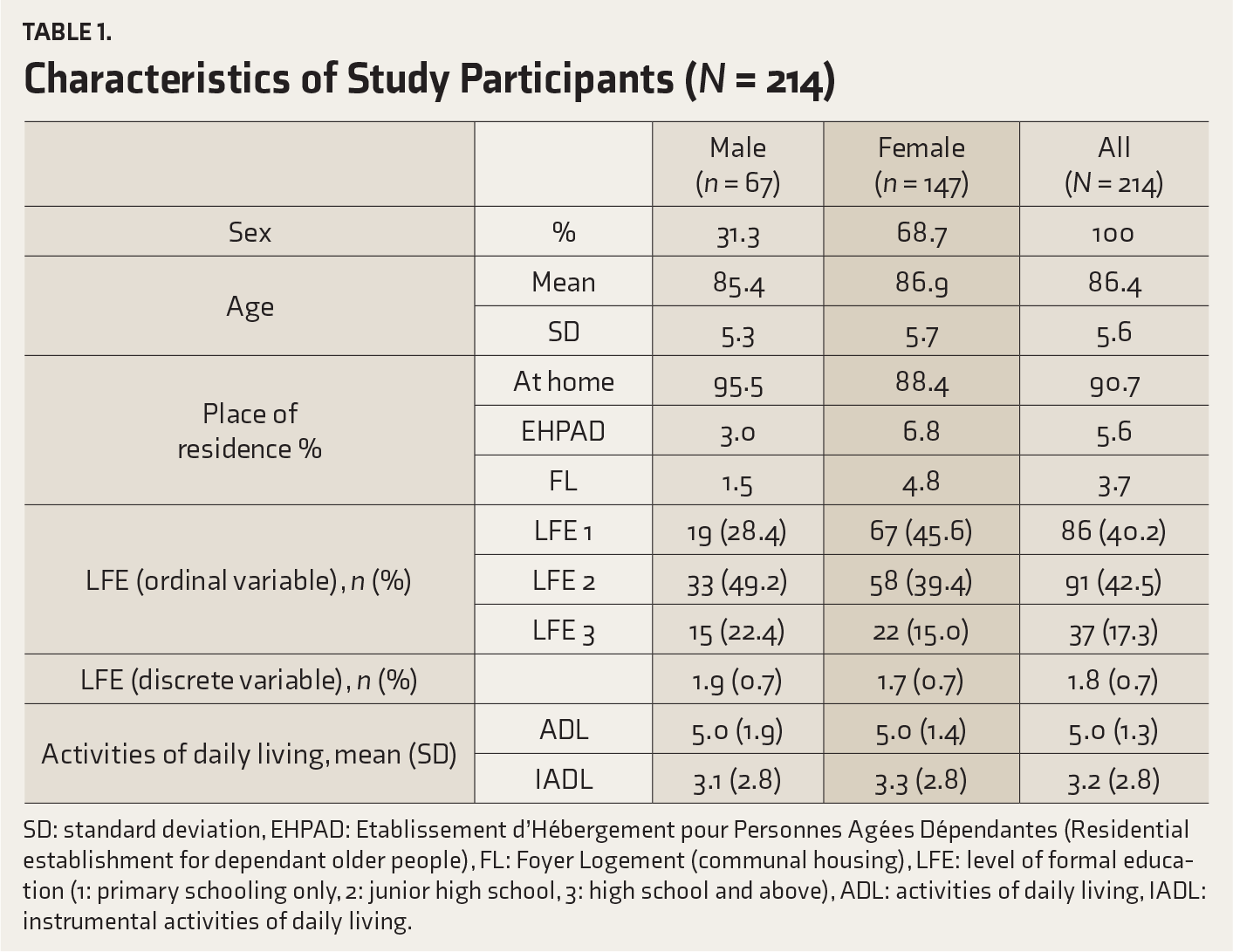
SD: standard deviation, EHPAD: Etablissement d’Hébergement pour Personnes Agées Dépendantes (Residential establishment for dependant older people), FL: Foyer Logement (communal housing), LFE: level of formal education (1: primary schooling only, 2: junior high school, 3: high school and above), ADL: activities of daily living, IADL: instrumental activities of daily living.
Descriptive and Analytical Statistics for Level of Formal Education and CFT-30/MMSE Scores (N = 214)
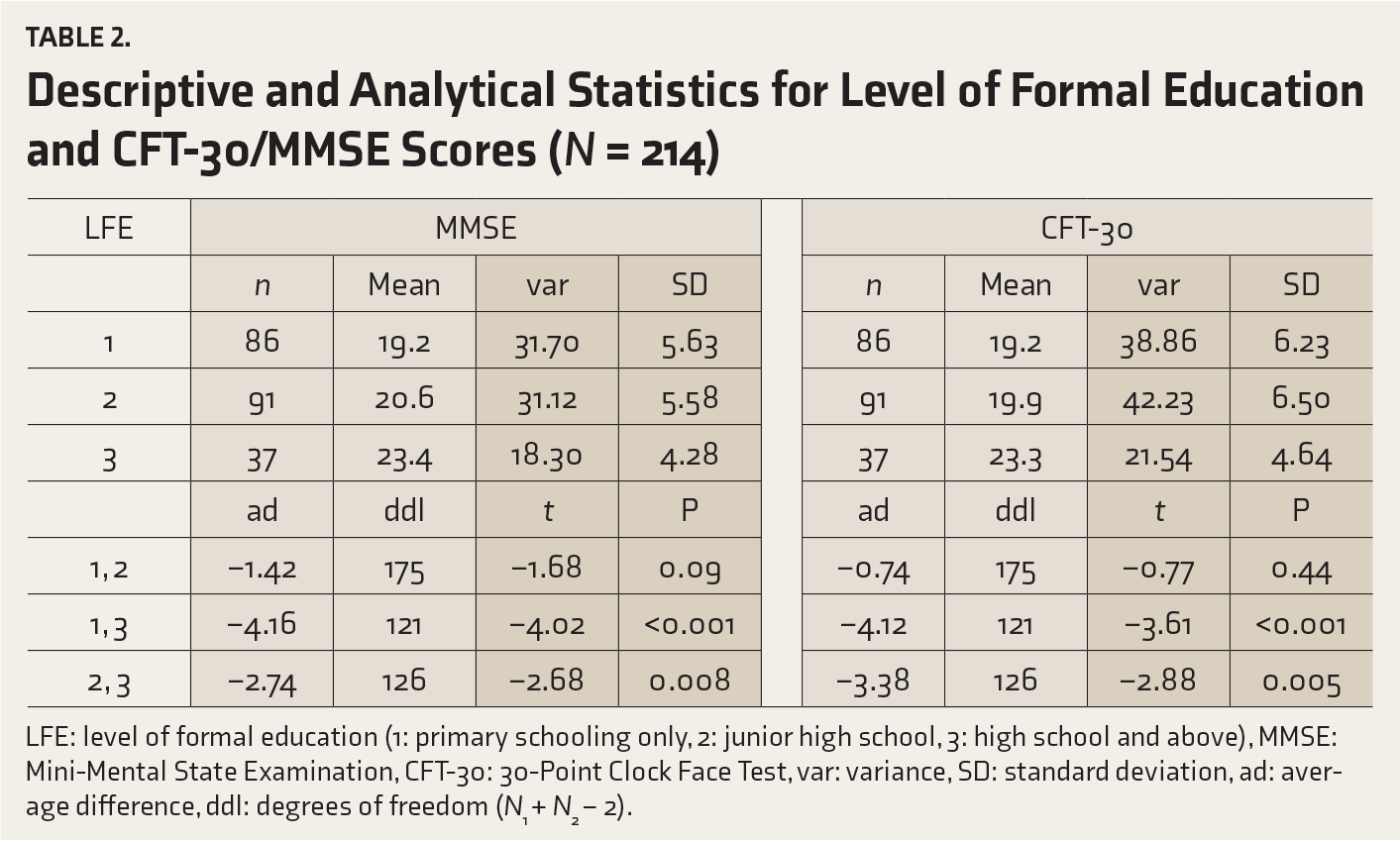
LFE: level of formal education (1: primary schooling only, 2: junior high school, 3: high school and above), MMSE: Mini-Mental State Examination, CFT-30: 30-Point Clock Face Test, var: variance, SD: standard deviation, ad: average difference, ddl: degrees of freedom (N1 + N2 − 2).
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Cognitive Screening Tool for Geriatrics: A Retrospective Observational Study on the Correlation of the Scores in 30-Point Clock Face Test and MMSE by Noureddine Bouati, Sabine Drevet, Nabil Zerhouni, Catherine Bioteau, Nathalie Mitha, Gaëtan Gavazzi, in Indian Journal of Psychological Medicine
Footnotes
Acknowledgements
The authors would like to thank Dr Alison Foote (Grenoble Alpes University Hospital) for critically reading and translating the manuscript. The authors would also like to thank Dr Sandra David-Tchouda (Grenoble Alpes University Hospital) for the valuable advice in statistical methodology.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.