
Abstract
Background:
The transitional state between normal aging and dementia is known as Cognitive impairment (CI) where a person has memory complaints and objective evidence of CI but no evidence of dementia. With the globe undergoing a “demographic transition,” the magnitude of neurodegenerative disorders is rising. In India, 27.3% of older persons with comorbidities had CI. Early identification of CI will likely help initiate proper remedial intervention, leading to better overall outcomes. In order to determine the prevalence of CI in older persons and whether it is associated with co-morbid conditions, this study was designed.
Methods:
A descriptive cross-sectional study was conducted among 350 older adults aged ≥60 residing in rural areas of Lucknow, selected using multistage cluster sampling. The Hindi Mental State Examination (HMSE) scale was used to assess cognitive function. A pretested semi-structured questionnaire was used to collect information on sociodemographic characteristics and comorbidity status.
Results:
Among 350 participants, with mean ± SD age 70.66 ± 9.53 years, the prevalence of CI as per HMSE (<23) was 24.9%. Overall, the mean HMSE score was less in individuals with (25.2) than without (27.19) comorbidities. Those with comorbidities had significantly lower mean scores in all individual domains of HMSE.
Conclusion:
CI affects one-fourth of the older adult population. Risk increases with the presence of comorbidities. Hence, screening, and early treatment are recommended.
The prevalence of cognitive impairment is 24.9% among older adults residing in rural Lucknow. Factors significantly associated with it are low educational status, chronic illness, bone and joint disease, and poor vision.Key Message:
Cognitive disability is defined as a person’s inability to concentrate, recall new information, remember things they already know, or make decisions that have an impact on their daily lives. 1 It is sometimes seen as a sign of more serious illnesses like depression, dementia, or Alzheimer’s disease. As per Global Burden of Disease (2010), neuropsychiatric disorders among older adults are responsible for 6.6% of the total disability (DALYs), with 15% having mental disorders. 2
Worldwide, nearly 50 million people have cognitive impairment (CI), and by 2030, this number is expected to rise to 75 million owing to population aging. 3 Also, with the ever-expanding greying population, the number of people living with dementia is projected to double every 20 years. This growth rate will be highest in East and Southeast Asia (India, China). Globally, older adults are at significant risk of having multiple chronic illnesses with associated functional impairment, and for some, these issues are further exacerbated by memory issues. 4 Aging increases the risk of chronic diseases such as dementia and cardiovascular diseases, which are the leading causes of illness, disability, death, and healthcare cost, 5 and this burden is expected to jump drastically. 1 The age-associated rise in the share of chronic health conditions is steady and consistent in India. 6 India is a diverse country concerning geographical, cultural, and social factors; the observed prevalence of CI varies from 6.5% in Kashmir 7 and 3.5% in Himachal Pradesh 8 to 27.3% in Punjab 9 and 26% in Kerala. 10 A study in Uttar Pradesh reported a 5.5% prevalence of dementia in rural areas and 3.8% in urban areas. 11 Longitudinal Aging Study in India, a large-scale nationwide survey, also reported that 15% of older adults (≥60 years) had low cognition scores. 5
Factors like lack of education, genetic predisposition, midlife hypertension, midlife obesity, diabetes, unhealthy lifestyle behavior, metabolic factors, and other comorbidities have been attributed for the progression from physiological cognitive decline to CI. 12 Hence, without disease-modifying treatment modalities, modifiable factors provide a window of opportunity to mitigate the risk of developing dementia. Also, the WHO and G8 Dementia Summit (2013) prioritized prevention as a key element to curb the dementia epidemic. 13 With everchanging patterns of risk factors and scarcity of literature on the magnitude of comorbidities/multimorbidity and its association with cognitive function, the study was conducted to determine the prevalence of CI in older adults over 60 in the rural Lucknow population and its association with comorbidities.
Methodology
Study Design and Participants
A community-based descriptive cross-sectional study was conducted from January to August 2022 among older adults (≥60 years) residing in the rural areas (Dadupur, Natkur, Paharpur) of Lucknow.
Eligibility Criteria
Participants in the study were those over 60 who had lived in the designated areas for a minimum of a year after obtaining written consent. Individuals with any previously diagnosed psychiatric illness, Parkinson’s disease, stroke, epilepsy, severe head injury, or brain neoplasm (and other neurological disorders) or diagnosed with severe vision or hearing loss were excluded.
Sample Size
Sample size (N) = Zα/2 2 *p*(1 - p)/MOE²
As per an epidemiological study conducted in a North Indian older adult population, which used Hindi Mental State Examination (HMSE) score (≤25) to define CI, the prevalence was estimated to be 8.8% 14 ; based on this, 95% confidence interval, 4% type 1 error rate, and an assigned effect size of 1.6, 350 was determined to be the minimal sample size needed for a 10% non-response rate.
Sampling Technique
Multistage Cluster Sampling
In step 1, the Sarojini Nagar block was chosen by simple random sampling from a cluster of eight rural blocks in Lucknow. In stage 2, the Primary Health Centre (PHC) Sarojini-Nagar was selected randomly out of 7 PHCs in the Sarojini-Nagar block. In the last stage, three sub-centers were selected randomly to complete the desired sample size, considering the percentage of the older adult population (8.6%), current death rate, eligibility criteria, and provision of consent by participants.
Selection of Participants
Accredited Social Health Activist workers from the selected sub-centers were contacted, and the list of older adults in each sub-center was prepared separately. From the prepared list, individuals were contacted individually to achieve the targeted number of older adults from the respective subcenters using purposive sampling. Three hundred fifty older adults were selected, including 117 from each of the two subcenters (Dadupur and Natkur) and 116 from the Paharpur subcenter.
Data Collection
A pre-tested, pre-designed, semi-structured questionnaire was used to gather data. Every member of the home meeting the eligibility requirements was included in the study, which involved conducting house-to-house visits with the study population. Information was collected from consenting respondents on the socio-demographic profile (about their residence, gender, marital status, type of family, educational status, family income, respondent’s income, employment status, etc.) and clinical characteristics (self-reported history of hypertension, diabetes, COPD, bone and joint disease, vision or hearing impairment or any other chronic comorbidity). Cognition was assessed using the HMSE tool.
Assessment Tools
One of the most used screening instruments for assessing CI and Alzheimer’s disease dementia is the Mini-Mental State Examination. The Indo-US Cross-National Dementia Epidemiology Study created by Professor (Dr.) Mary Ganguli’s HMSE 15 as a screening instrument especially for the illiterate population. Items in the HMSE that required reading, writing, and arithmetic skills were modified. It comprises of 22 items, with a total score of 30, examining 10 major cognitive domains (orientation to time and place, registration, attention, concentration, recognition of objects, language function, comprehensive and expressive speech, motor functioning, and praxis). As most North Indian older adults are Hindi-speaking and have no formal education, the HMSE was suitable for our sample. The tool is 81.3% sensitive and 60.2% specific, and has an interrater reliability coefficient of 0.86 at the cut-off score of 23. 16 Tsolaki also reported maximum sensitivity (98%) and specificity (94%) at a cut-off score of 23. 17 It has been used in various studies among the senior population of India.
Operational Definition of CI
HMSE score ≤23 was considered “cognitively impaired.” These impairments were further classified as mild (HMSE score 16–23), moderate (HMSE score 11–15), and severe (HMSE score ≤10).
Data Analysis
Data analysis was done using IBM Statistical Package for Social Sciences, version 26. The chi-square test was utilized to evaluate related factors because the outcome variable, cognitive function, was categorical. If the anticipated frequency in a given cell was less than 5, the Fischer Exact test was employed, and a p value of less than .05 was deemed statistically significant. Utilizing binary logistic regression, the factors associated with CI were found. The degree of collinearity between the explanatory variables in the regression model was examined and the backward elimination (Wald) method was used for variable selection. p value <.05 was considered statistically significant. Mean scores of individual domains of HMSE were calculated and were compared among comorbidity and no comorbidity groups using the Mann–Whitney U test.
Ethical Aspects
Ethical approval was taken from King George’s Medical University Institute’s ethical committee; ethical reference number: V-PGTSC-11A/P8. The subjects who screened positive for CI were referred to a higher center for further assessment and management.
Results
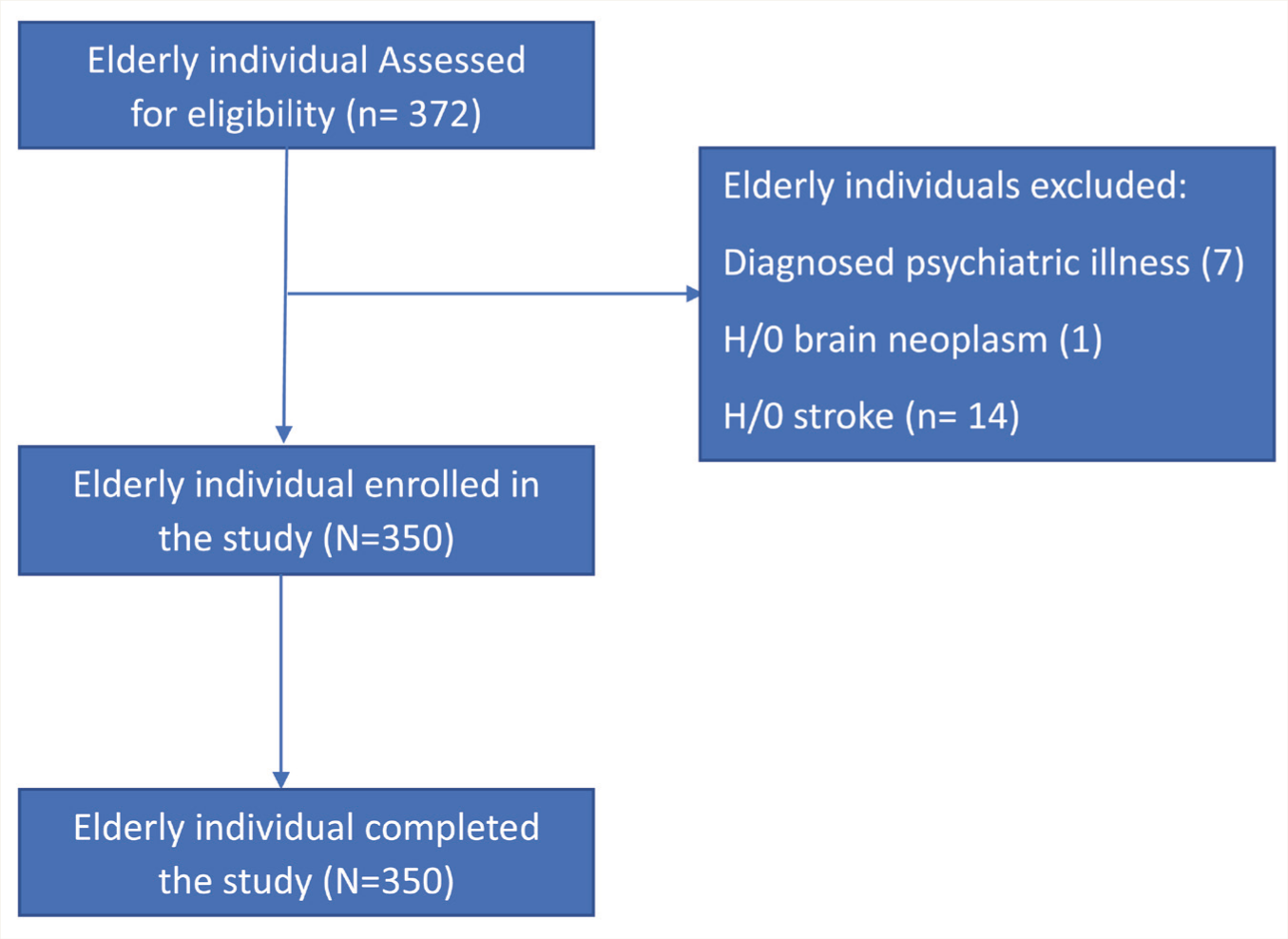
Three hundred fifty community-dwelling older adults participated and completed the face-to-face interview for cognitive assessment (Figure 1).
Study Flow Diagram.
Background Characteristics
The mean (SD) age of participants was 70.6 (60–101) years, with the majority being females (54.9%), married, and living in a joint family setting. Two-thirds of the participants reported the presence of one or more comorbidities. The most common self-reported chronic illness was bone and joint diseases (26.9%), followed by hypertension (22.6%) and diabetes (16%) (Table 1).
Association Between Co-morbidities and Cognitive Function Among Study Participants (N = 350).
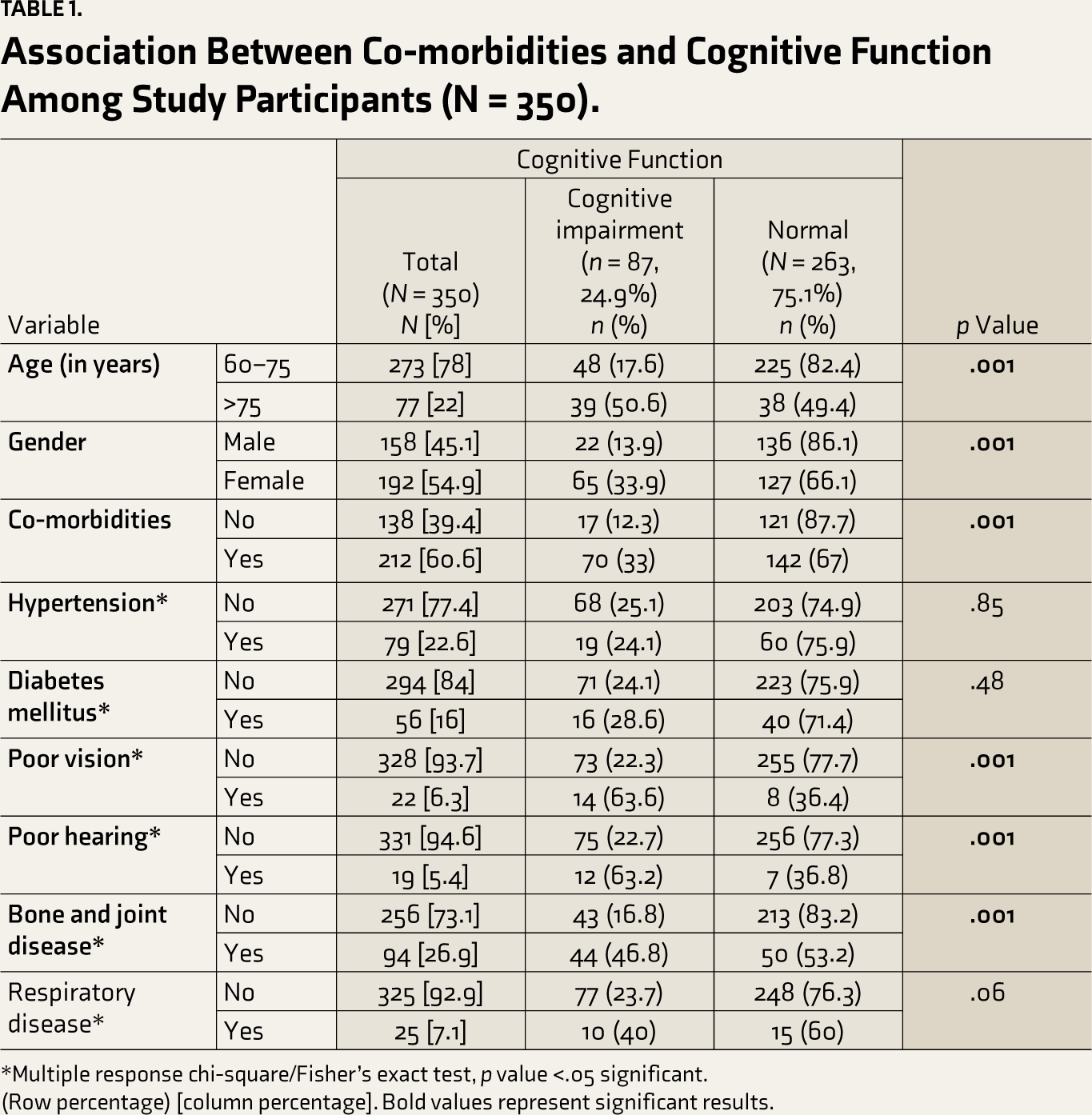
*Multiple response chi-square/Fisher’s exact test, p value <.05 significant.
(Row percentage) [column percentage]. Bold values represent significant results.
Clinical Parameters
On the day of the interview, the majority (70%) had their blood pressure (BP) in the elevated range. Also, 12.6% had random blood glucose levels in the elevated range. 26.5% of participants with elevated BP were screened to have CI (Table 2).
Association Between Clinical Parameters and Cognitive Function Among Study Participants (N = 350).
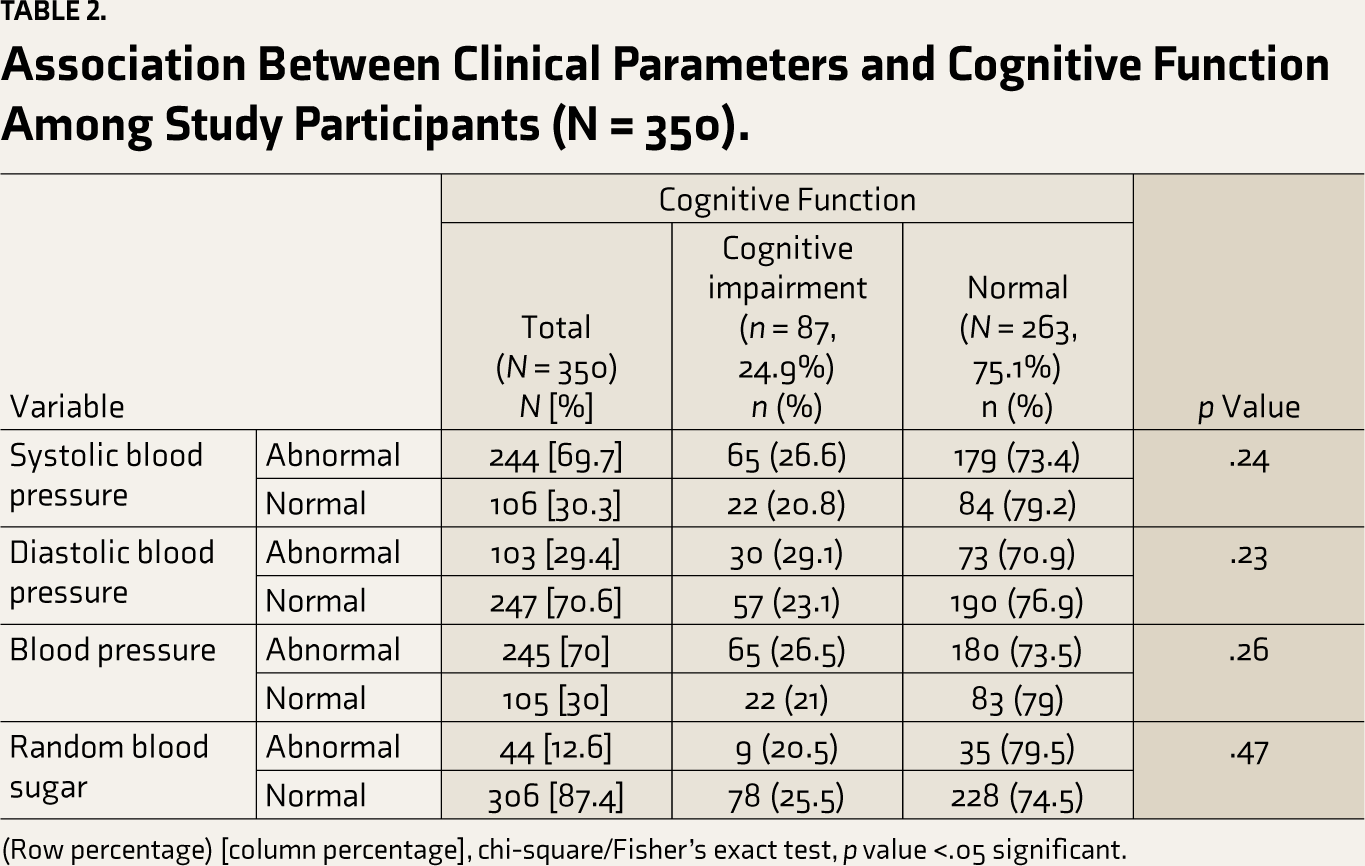
(Row percentage) [column percentage], chi-square/Fisher’s exact test, p value <.05 significant.
Prevalence of CI
Overall, 24.9% were found to have CI as per the HMSE. One participant scored 10 (severe CI). Of the 87 individuals with CI, 87.4% had mild impairment, and 11.5%, had moderate impairment.
CI and Comorbidity
The association between CI and comorbidity status is in Table 3. A binomial logistic regression was performed to ascertain the effect of various independent variables on CI status. Linearity assumption was tested using model fit and pseudo R2 statistics. The logistic regression model was statistically significant (X2 (74.3), p value <.001). The model explained 28.4% of the variance. Older age, female gender, comorbidity, bone and joint disease, and poor vision were significantly associated with the risk of CI. Subjects over 75 were three times more likely to have CI than subjects between 60 and 75 years (AOR: 3.48, 95% CI = 1.81–6.69). The presence of any comorbidity was positively linked with CI, with more odds of having CI (AOR = 1.83, 95% CI = 1.40–4.21). Participants with bone and joint diseases were two times more likely to have CI (AOR = 2.17, 95% CI = 1.10–4.29) in contrast to subjects who did not report one. Similarly, those with poor vision were more likely to experience CI (AOR = 1.98, 95% CI = 1.66–5.91).
Logistic Regression Analysis for Identifying Independent Risk Factors for Cognitive Impairment (N = 350).
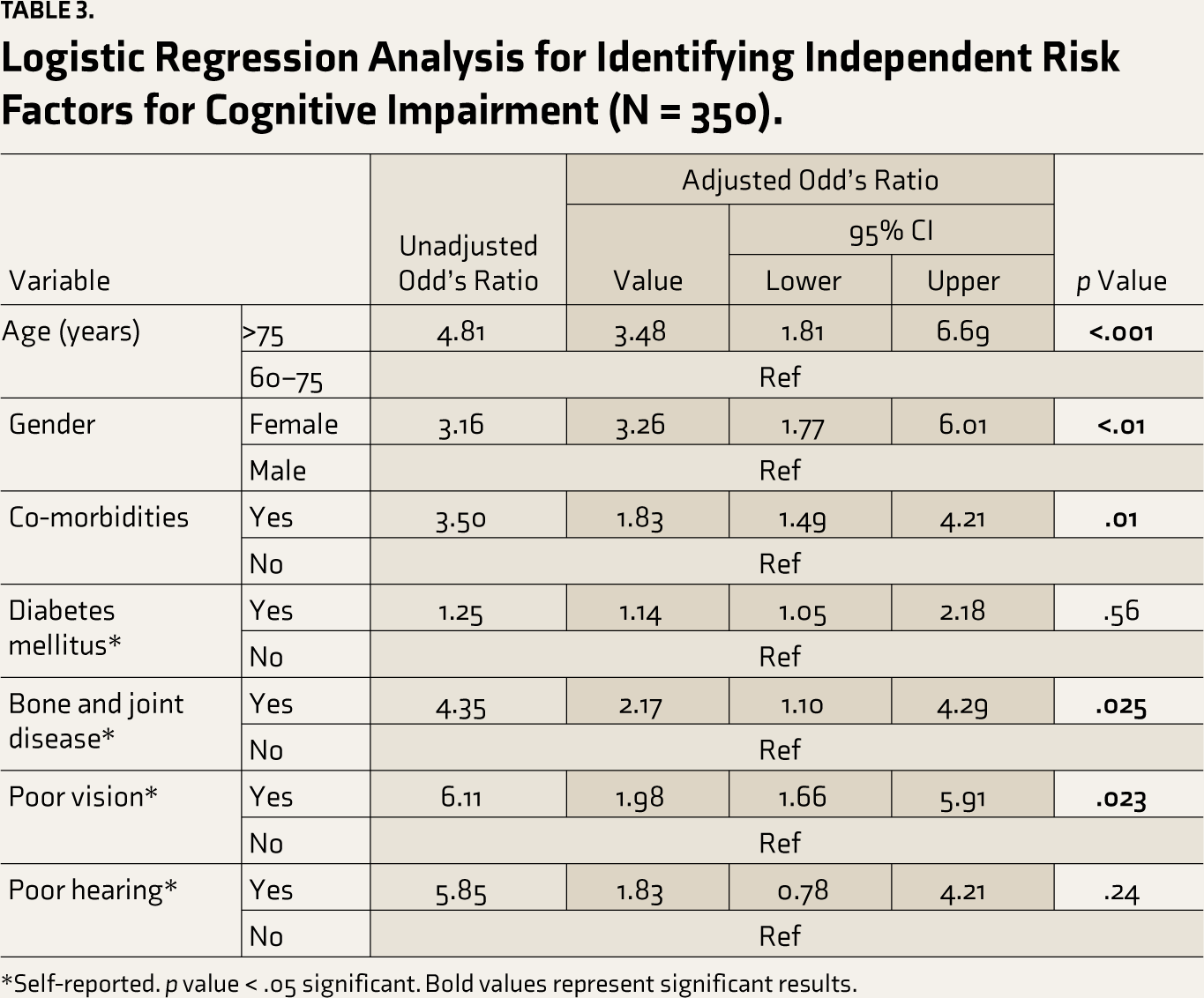
*Self-reported. p value < .05 significant. Bold values represent significant results.
Participants were divided into two groups to assess the impact of comorbidities on individual domains of HMSE. Table 4 shows the overall and sub-domain-wise HMSE scores among participants having and not having any medical comorbidity. Overall median HMSE score was less (26) among participants who reported any medical comorbidity (28), and this difference was statistically significant. Also, the median scores in almost all the subdomains were less in participants with medical comorbidities, except in “naming,” “repetition,” “sentence,” and “copying.”
Discussion
The prevalence of CI in this study was 24.9%. Pais et al. conducted a systematic review and showed the global prevalence of CI to be 5.1%–41%. 18 Different studies have reported varying prevalence of CI (Jadenur et al. 19 : 14.0% and Khanna et al. 20 : 8.4%), owing to the different cut-off values.
Overall, 60.6% of our participants had one or more chronic illnesses; among them, 33% had CI. Tables 3 and 4 show that chronic illnesses are positively associated with CI. Gondim et al. 21 showed a positive association between CI and self-reported diseases, including hypertension (OR = 2.06), stroke (OR = 2.88), and acute MI (OR = 2.94). Similarly, Mehra et al. 22 reported that the prevalence of CI was higher among older adults with Non-Communicable Diseases (NCDs), and this significant difference persisted even after controlling for confounding factors like age and gender. The cause of cognitive decline due to hypertension or DM can be chronic hypercerebral perfusion and secondary brain damage. 23 Chronic conditions, particularly after midlife, are causes of advanced cardiovascular and cerebral diseases and are linked with extensive cognitive decline. 24 Bone and joint disease were the most reported chronic illnesses (26.9%) and were significantly associated with CI. It is difficult to interpret this association as bone and joint disease can be a manifestation of chronic malnutrition or physical inactivity, among other factors, and hence can be linked with cognitive functioning rather than having direct causation. As this is a cross-sectional study, ascertaining temporal causation is beyond its scope, and further, in-depth cohort studies are required. The prevalence of CI is higher among subjects with comorbidities. Mean scores in the individual domains of the HMSE scale and the overall score were significantly lower among subjects who reported comorbidity compared to subjects with no comorbidity, which further supports the available data.9,25
Domain Wise Score as Per Co-morbidity Status (N = 350).
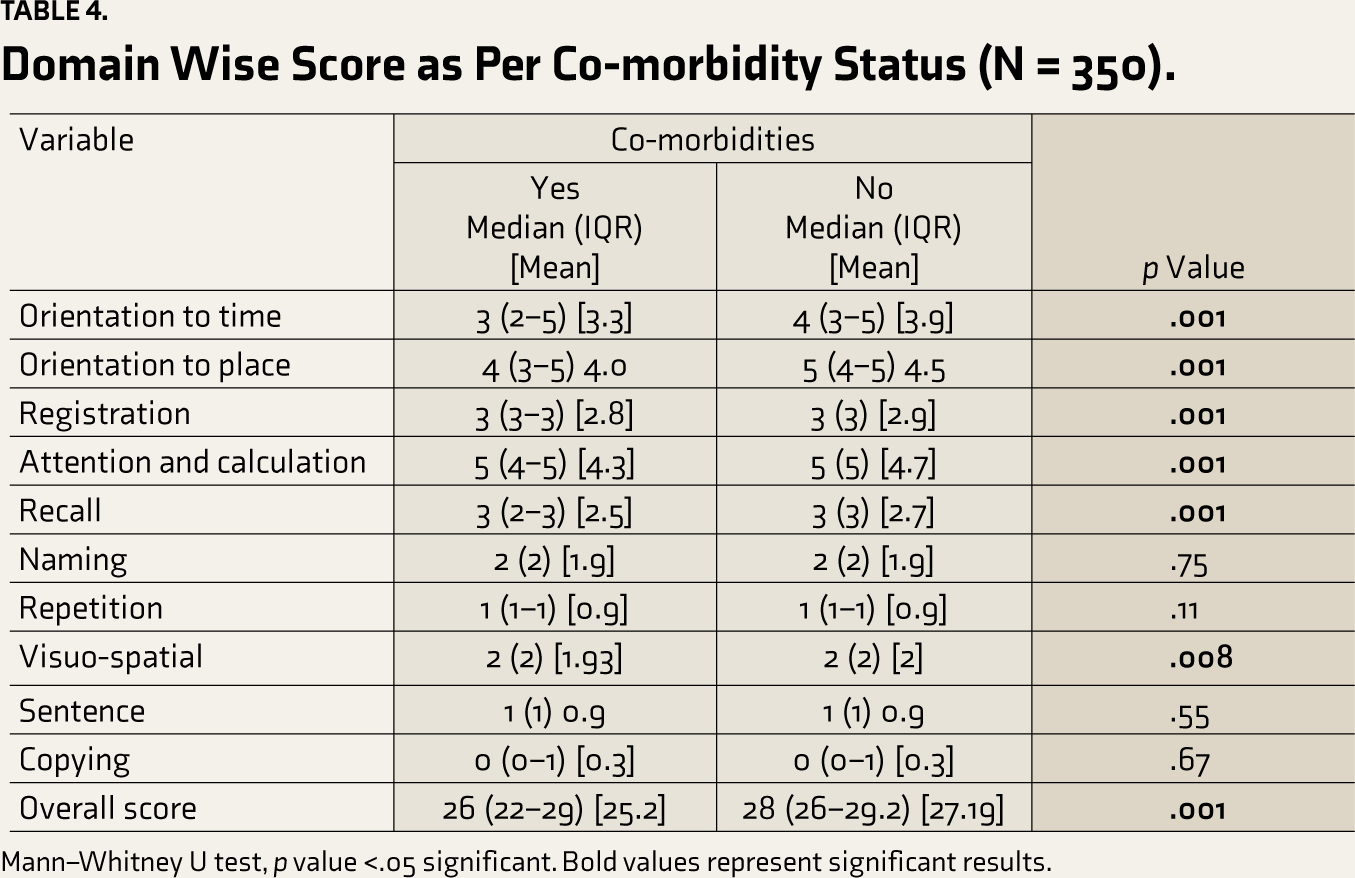
Mann–Whitney U test, p value <.05 significant. Bold values represent significant results.
It is now well-known that CI is associated with genetic and environmental risk factors. Occupation, diabetes, vascular condition, leisure activity, physical activity, and nutritional status significantly impact the individual’s cognitive function. Hence, screening for such conditions provides a good opportunity owing to their modifiable nature. Basic preventive measures like proper and adequate diet, a physically active lifestyle, correcting malnutrition, and early treatment of cardiovascular risk factors can prevent or even reverse cognitive decline.
Limitations
Cognitive function was assessed by the HMSE scale, which has its limitations. By cross-sectional study design, cognitive function was not assessed before the illness. Hence, temporal causation between comorbidity and CI cannot be ascertained. Being a community-based study and time-constrained, detailed psychiatric assessment and further diagnosis of cognitive functions could not be done. Also, undiagnosed cases of depression were missed, which is one of the major causes of cognitive decline and could have created a bias in the cognitive score.
Conclusion
There was a 24.9% prevalence of CI. Cognition was impaired in 33% of the comorbid subjects, and the average score in each domain of the HMSE was less in subjects with comorbidity. Hence, old-age comorbidities are positively linked with cognitive decline. Owing to the epidemiological transition most developing nations, including ours, face, a dire need to focus on modifiable risk factors, especially NCDs and other comorbidities, to lower the risk of CI and dementia. Health and wellness centers, which are approachable to the community, are an excellent opportunity through which comprehensive geriatric assessment and monitoring for treatment adherence and compliance can be done. In contrast to the previous literature from the country, which has mainly focused on the correlation of hypertension and diabetes with cognitive decline in a hospital setting, this study focused on general comorbidities commonly prevalent among the senior population in the community and their association with cognitive function. Further diverse community-based follow-up and interventional studies with larger sample sizes are needed to determine our findings’ validity. It is high time to focus on geriatric care, including screening for CI and comprehensive geriatric assessment as part of routine care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.