
Abstract
Purpose of the Review:
Substance abuse among young adults is a significant public health concern with detrimental consequences for individuals, families, and society. Family interventions have emerged as promising treatment approaches for addressing substance abuse in this population. This systematic review aims to synthesize the existing evidence on the efficacy of family interventions for young adults with substance abuse.
Collection and Analysis of Data:
A comprehensive search of electronic databases (PubMed, EBSCOhost, and Scopus) was conducted to identify relevant studies published between 2000 and 2023. Studies were included if they met the following criteria: (a) focused on family intervention for young adults (aged 10–25) with substance abuse; (b) employed a randomized controlled trial (RCT) or quasi-experimental design; and (c) reported on substance use outcomes. A total of 41 studies were included in the review. The findings suggest that family interventions are effective in reducing substance use among young adults. Specifically, family interventions were associated with significant reductions in behavioural problems and improvements in family functioning.
Keywords
This systematic review of studies focused on family intervention for young adults with SUDs. Family interventions were effective in reducing substance use and behavioral problems and improving family functioning. This review underscores the importance of involving family members as co-therapists in the treatment process.Key Messages:
Young adults aged between 10 and 24 years are highly vulnerable to substance use. 1 Substance use in young adults is higher than that in older adults for most of the substances.2, 3 Substance use among young adults gives rise to worries because it has the potential to negatively affect various aspects of their lives, including social interactions, emotional well-being, cognitive abilities, physical health, and academic performance. 4 Family factors such as impaired family functioning, limited warmth between mothers and children, elevated hostility in mother–child relationships, poor parental monitoring, and harsh maternal parenting practices are significant predictors of substance abuse in young adults. 5
In 1995, Liddle and Dakof initiated the first systematic review on the effectiveness of family therapy for substance use. 6 The review concluded that family-based addiction treatments hold promise and need to be proven. The findings were based on the limited number of published studies available then, and there were methodological limitations. Subsequent systematic reviews and meta-analyses7–17 suggest that involving family members in substance abuse treatment is beneficial in reducing substance use and improving family functioning among adolescents with substance use.
Research Gap
Despite extensive literature highlighting the increased vulnerability of young adults to substance abuse and its widespread consequences across various life domains, there exists a significant research gap in examining family intervention models tailored to young adults. Earlier systematic reviews6, 17 laid the foundation for understanding the potential of family intervention for substance abuse. Subsequent systematic reviews suggested the positive impact of involving family members in substance abuse treatment. However, these reviews primarily focused on adolescents and adults. Therefore, there was a research gap concerning the effectiveness of family interventions for young adults. Moreover, the inclusion criteria for the studies were limited to the past 10 years. Hence, there is a necessity for a systematic review to bridge the gap by offering a comprehensive review of existing evidence on family intervention models specifically designed for young adults with substance abuse.
The systematic review aims to examine the family intervention models designed specifically for young adults with substance abuse. The objectives of the review were (a) to identify and analyse the existing family intervention models for young adults with substance abuse and (b) to evaluate the specific outcomes of the existing family intervention models. These outcomes include reducing substance use, enhancing family dynamics, and promoting sustained recovery among young adults.
Methods
Protocol Registration
A systematic review protocol was developed and registered within the International Prospective Register of Systematic Reviews (PROSPERO: CRD42023488865).
Search Strategy
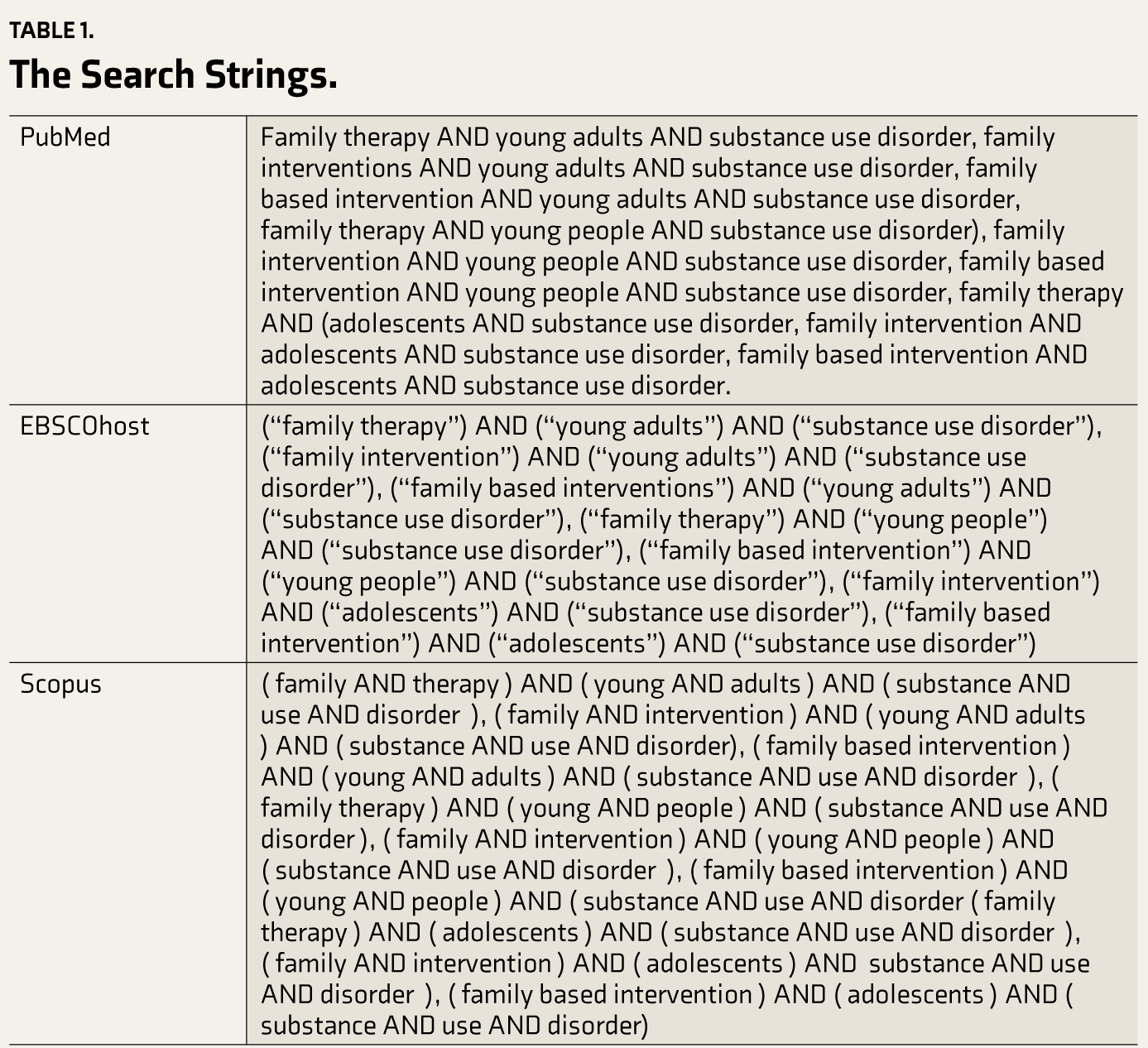
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines by Moher et al.18 to ensure transparency and validity in the study. A pilot literature search was carried out to identify the correct keywords and assess the feasibility of the literature search. Subsequently, search keywords were finalized. Search strings used for the literature search in PubMed, EBSCOhost, Scopus were given in Table 1. A comprehensive literature search was conducted in three electronic databases subscribed by the host institute, namely, PubMed, EBSCOhost, and Scopus, between May 1, 2023, and July 31, 2013 to identify studies on the effectiveness of family intervention in young adults with substance abuse between 2000 and 2023. Focusing on this time frame allows for a comprehensive examination of the evolution of family intervention models, treatment approach changes, and advancements in research methodologies over time. It ensures that it includes the most relevant and up-to-date literature.
The Search Strings.
Eligibility Criteria
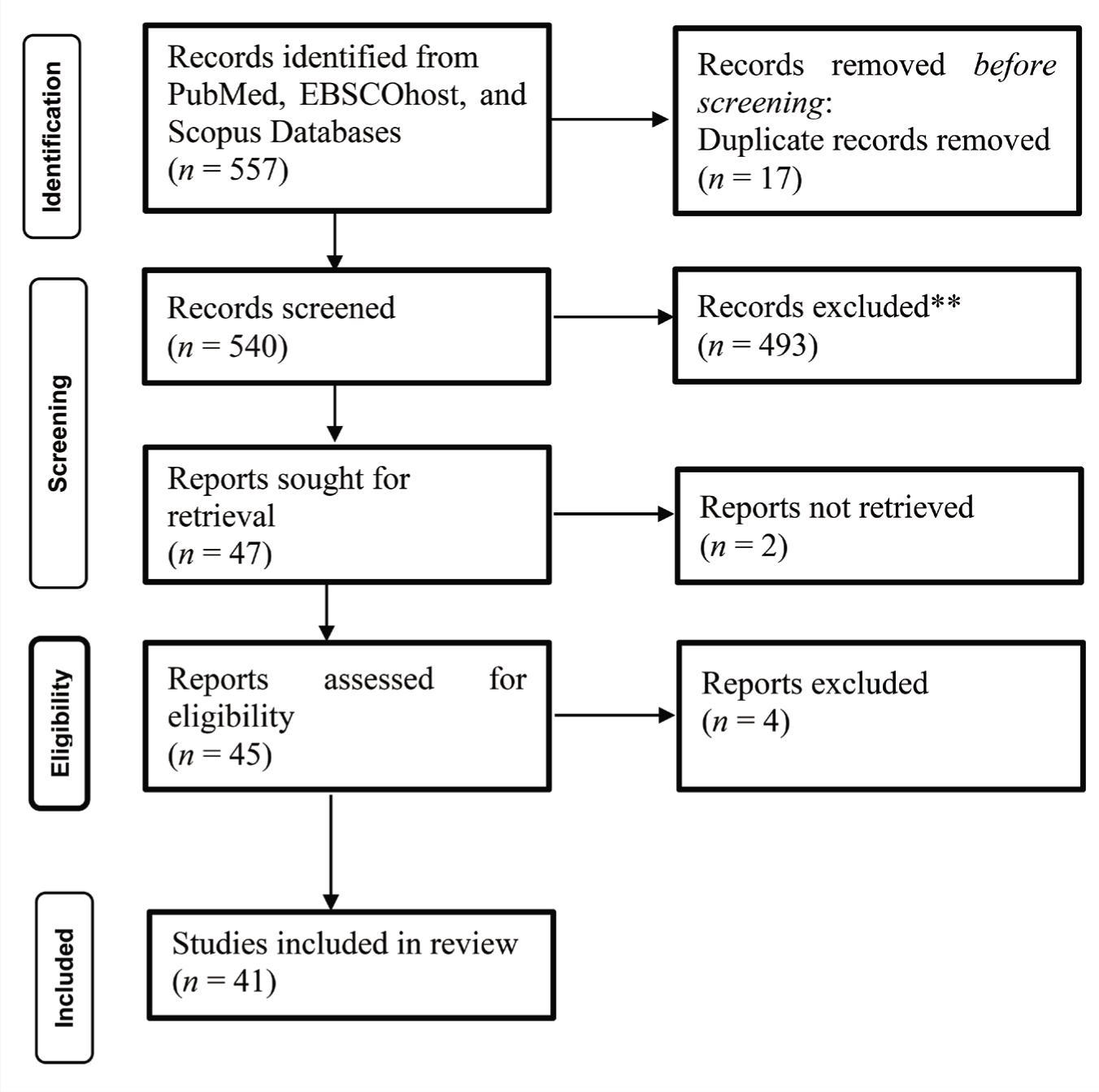
The systematic review included all randomized controlled trials (RCTs) and quasi-experimental studies reporting the efficacy of family intervention for substance abuse among young adults published in peer-reviewed journals in English from 2000 to 2023. This duration enables a thorough examination of the evolution of family intervention models, treatment approach changes, and advancements in research methodologies, ensuring the inclusion of the most relevant and up- to-date literature. Furthermore, studies meeting the following inclusion criteria were selected for the review. (Figure 1)
The PRISMA Flow Chart of the Literature Search and Selection Process.
Population (P)
Young adults aged 10–25 years with substance abuse involving various substances such as tobacco/nicotine, alcohol, cannabis (marijuana), prescription medications, inhalants, and illicit drugs (cocaine, ecstasy, LSD, MDMA, hallucinogenic mushrooms, and other illegal drugs).
Intervention (I)
Various family intervention models are designed to address substance abuse in young adults, including psychoeducation, counselling, family therapy, and support programs involving family members.
Comparison (C)
The comparison group may involve young adults with substance abuse issues who did not receive family intervention or received standard care without a family-focused component.
Outcome (O)
Multiple outcomes were considered, including a reduction in substance abuse, an improvement in family functioning and dynamics, or a reduction in behavioural problems among young adults.
The review excluded meta-analyses, systematic reviews, literature reviews, protocol publications, guidelines, and treatment manuals. Additionally, studies assessing the effectiveness of interventions other than family intervention should have been considered. Furthermore, studies beyond social work and psychology’s purview were also excluded.
Literature Search, Screening, and Selection Process
The first author (KVB) conducted a literature search, and 557 articles were found in open access (PubMed: 244, EBSCOhost: 333, and Scopus: 0). These abstracts were uploaded to Rayyan Software for duplication removal.19 Rayyan Software eliminated 17 duplicate records. KVB, ES, NJ, and PKC independently reviewed the titles and abstracts of the remaining articles, applying the predefined inclusion criteria. Of the 540 articles, 493 were excluded after the screening as they did not meet the inclusion criteria. Forty-seven articles with full text were evaluated for eligibility, of which two full texts could not be retrieved. Hence, 45 articles were obtained and carefully reviewed to assess their eligibility with the inclusion criteria and the study objectives. Finally, 41 articles were found suitable for systematic review.
Data Extraction
Essential data were extracted systematically using predefined criteria from the selected studies, including authors, year, country, study aims, methods (study characteristics, participant demographics, specific interventions), and results (Table 2).
Family Intervention Models for Young Adults with Substance Use.
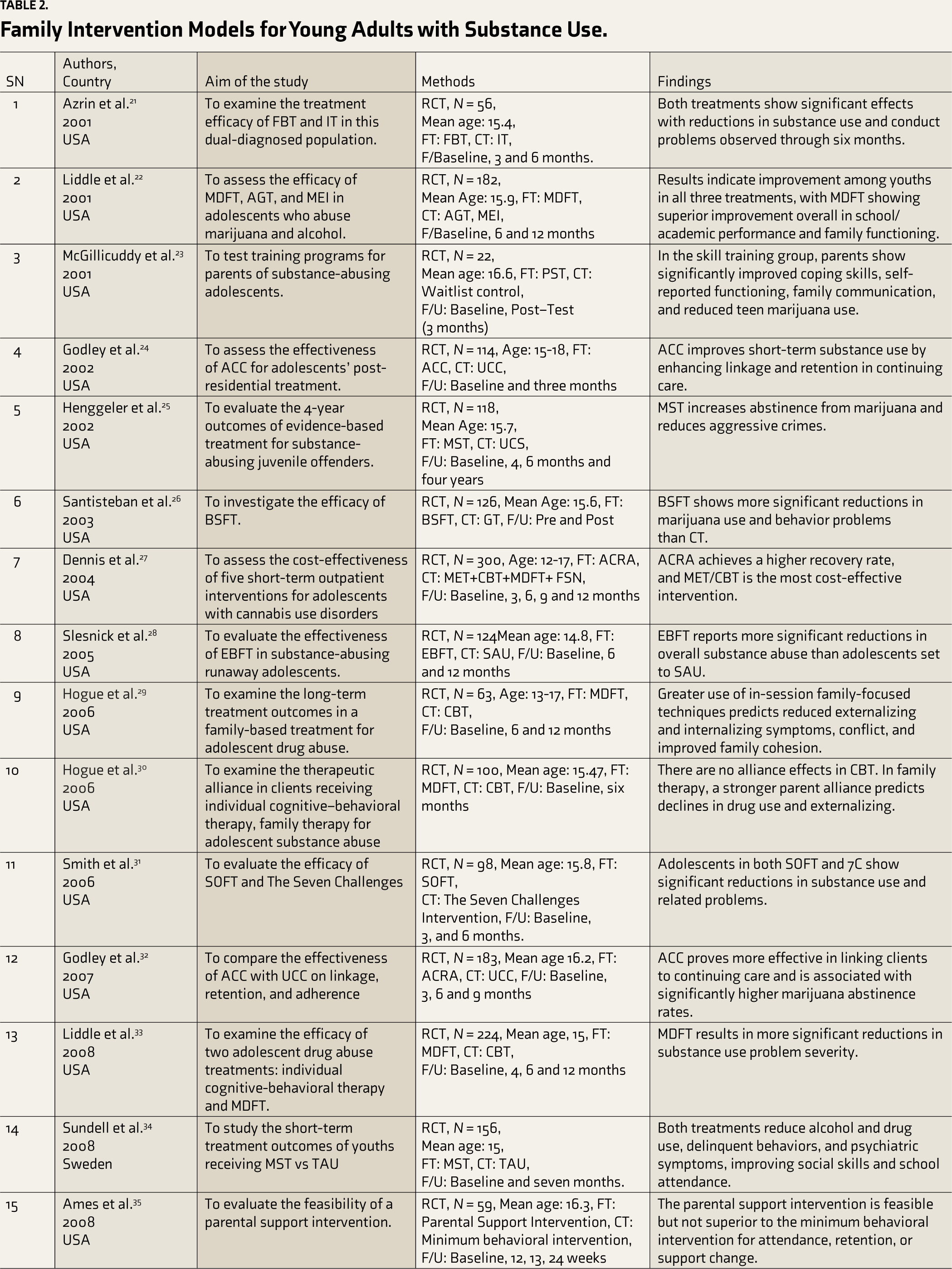
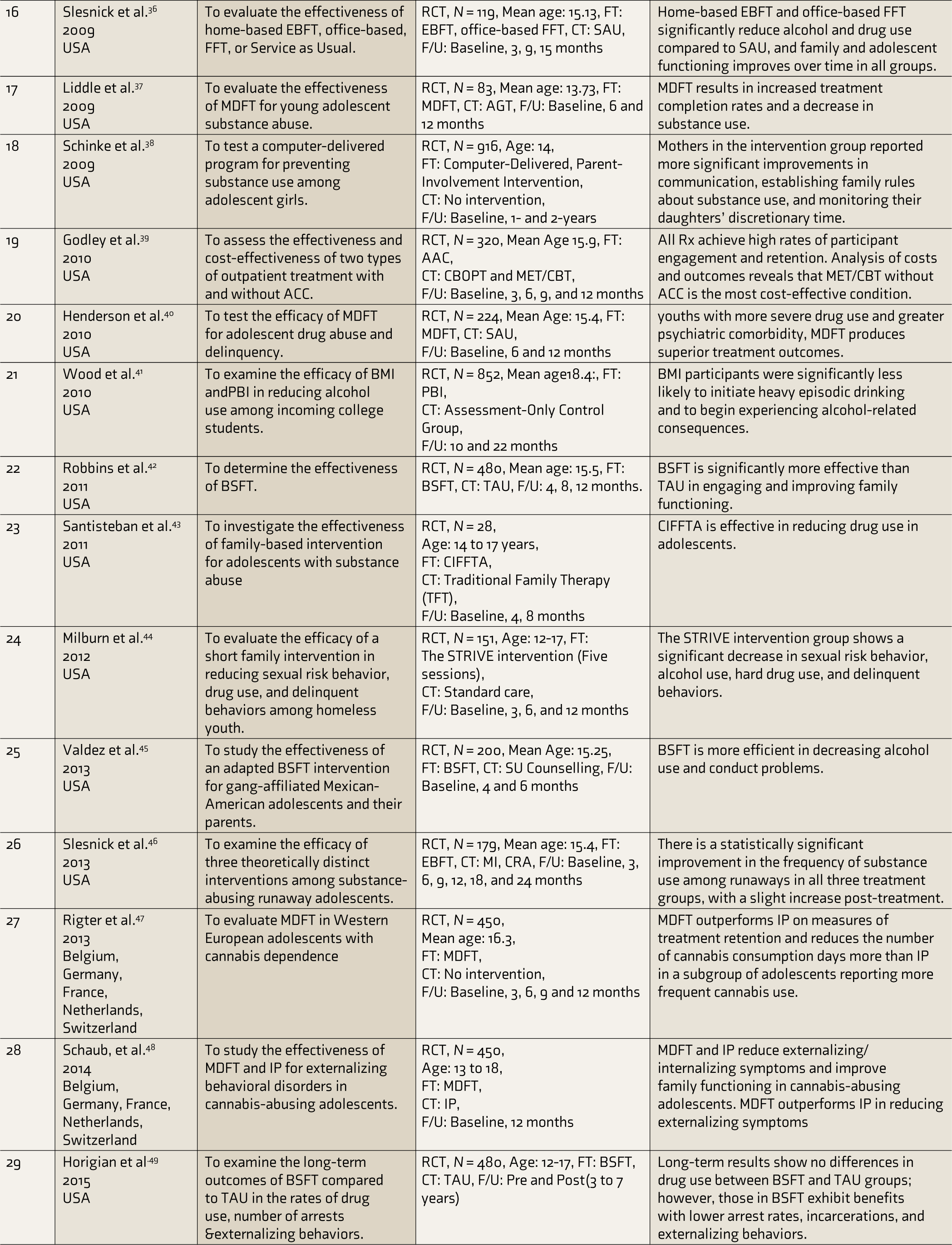
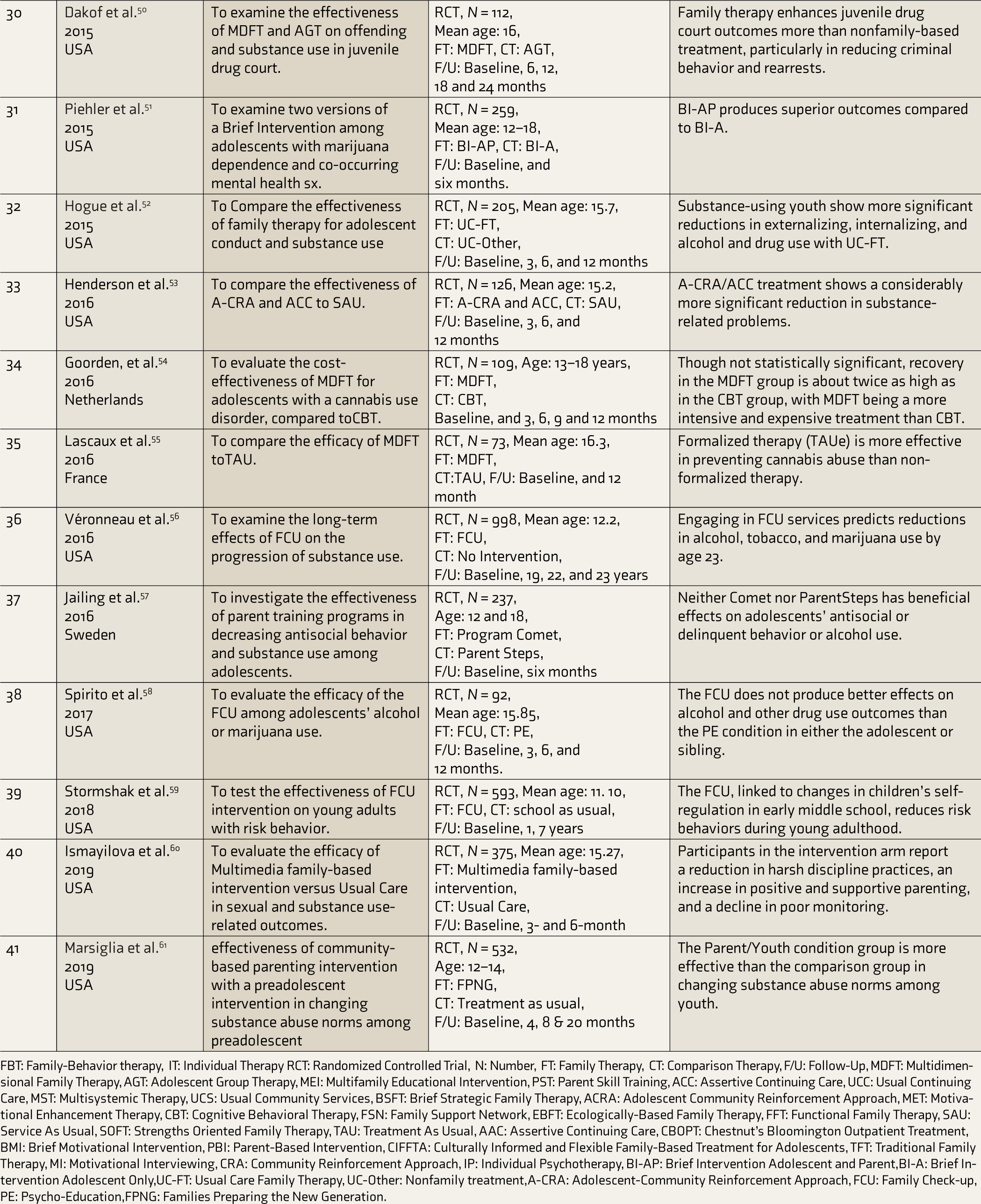
FBT: Family-Behavior therapy, IT: Individual Therapy RCT: Randomized Controlled Trial, N: Number, FT: Family Therapy, CT: Comparison Therapy, F/U: Follow-Up, MDFT: Multidimensional Family Therapy, AGT: Adolescent Group Therapy, MEI: Multifamily Educational Intervention, PST: Parent Skill Training, ACC: Assertive Continuing Care, UCC: Usual Continuing Care, MST: Multisystemic Therapy, UCS: Usual Community Services, BSFT: Brief Strategic Family Therapy, ACRA: Adolescent Community Reinforcement Approach, MET: Motivational Enhancement Therapy, CBT: Cognitive Behavioral Therapy, FSN: Family Support Network, EBFT: Ecologically-Based Family Therapy, FFT: Functional Family Therapy, SAU: Service As Usual, SOFT: Strengths Oriented Family Therapy, TAU: Treatment As Usual, AAC: Assertive Continuing Care, CBOPT: Chestnut’s Bloomington Outpatient Treatment, BMI: Brief Motivational Intervention, PBI: Parent-Based Intervention, CIFFTA: Culturally Informed and Flexible Family-Based Treatment for Adolescents, TFT: Traditional Family Therapy, MI: Motivational Interviewing, CRA: Community Reinforcement Approach, IP: Individual Psychotherapy, BI-AP: Brief Intervention Adolescent and Parent,BI-A: Brief Intervention Adolescent Only,UC-FT: Usual Care Family Therapy, UC-Other: Nonfamily treatment,A-CRA: Adolescent-Community Reinforcement Approach, FCU: Family Check-up, PE: Psycho-Education,FPNG: Families Preparing the New Generation.
Quality Assessment (Risk of Bias Assessment)
The quality (risk of bias) assessment was conducted using the Quality Assessment of Controlled Intervention Studies tool.20 The tool consists of 14 criteria that systematically evaluate the robustness of methodological attributes. The total score, computed from the number of affirmative responses, categorizes study quality as poor, fair, and good (Table 3).
Quality Assessment (Risk of Bias Assessment) of the Studies.
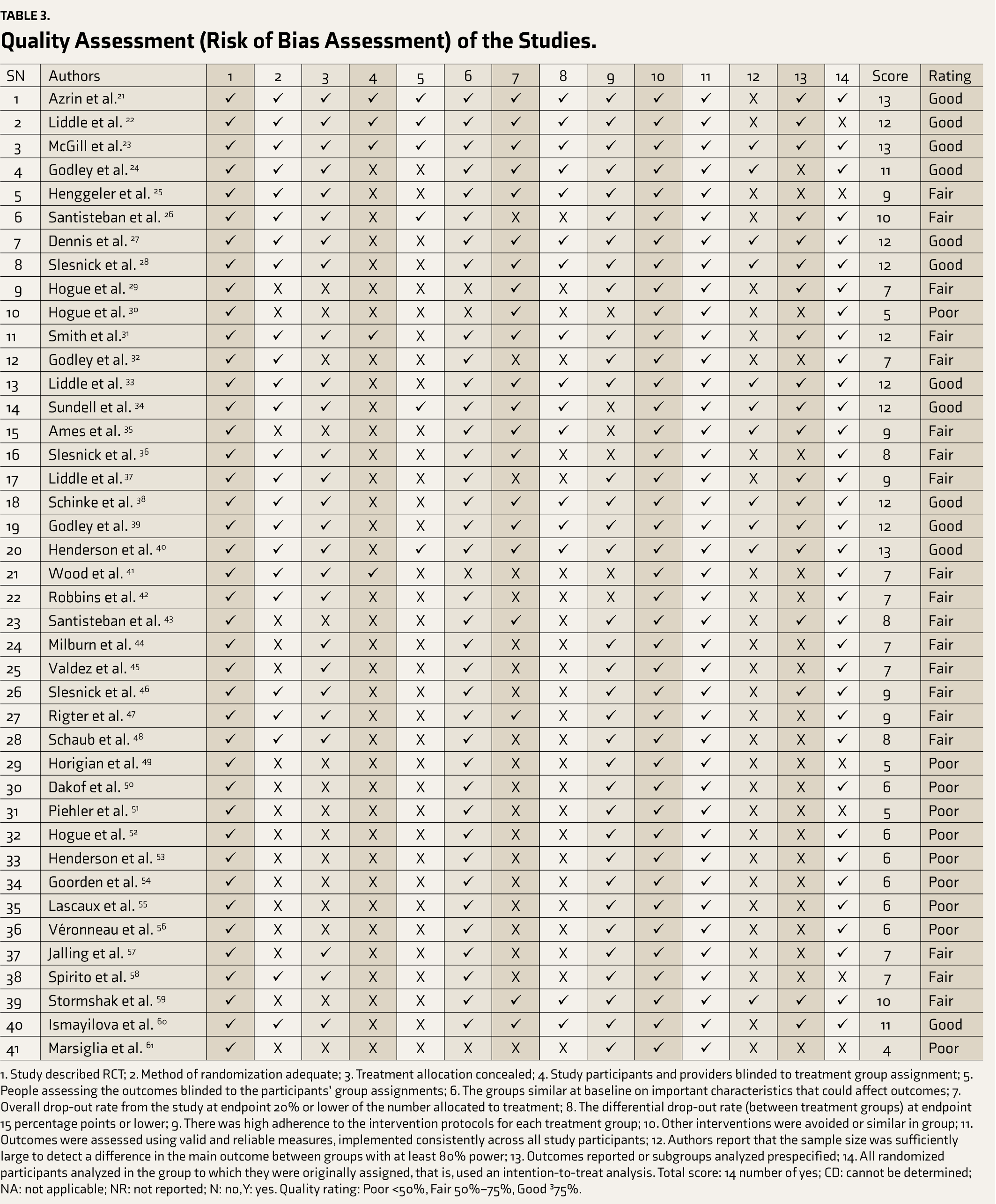
1. Study described RCT; 2. Method of randomization adequate; 3. Treatment allocation concealed; 4. Study participants and providers blinded to treatment group assignment; 5. People assessing the outcomes blinded to the participants’ group assignments; 6. The groups similar at baseline on important characteristics that could affect outcomes; 7. Overall drop-out rate from the study at endpoint 20% or lower of the number allocated to treatment; 8. The differential drop-out rate (between treatment groups) at endpoint 15 percentage points or lower; 9. There was high adherence to the intervention protocols for each treatment group; 10. Other interventions were avoided or similar in group; 11. Outcomes were assessed using valid and reliable measures, implemented consistently across all study participants; 12. Authors report that the sample size was sufficiently large to detect a difference in the main outcome between groups with at least 80% power; 13. Outcomes reported or subgroups analyzed prespecified; 14. All randomized participants analyzed in the group to which they were originally assigned, that is, used an intention-to-treat analysis. Total score: 14 number of yes; CD: cannot be determined; NA: not applicable; NR: not reported; N: no, Y: yes. Quality rating: Poor <50%, Fair 50%–75%, Good ³75%.
Two reviewers independently assessed each domain, and discrepancies were resolved through discussion/consultation with a third reviewer. The risk of bias assessment was considered in interpreting study results and determining the quality of evidence in the systematic review. The final review report included transparent reporting of the risk of bias assessment.
Results
Most of the studies were conducted in the USA. Participant ages ranged from 12 to 18 years, with differing mean ages across studies. Seventeen studies included both female and male young adults with substance use disorders, and one study was conducted among adolescent girls with substance use disorders. The commonly used tools include Problem Checklist, Child Behavior Checklist, Parental Bonding Instrument, Youth Self-report, Structured Clinical Interview for DSM-IV (SCID-IV), Global Appraisal of Individual Needs (GAIN), Timeline Follow Back Interview, Therapist Behaviour Rating Scale, Family Environment Scale, and Conflict Tactics Scale. The outcome measures covered a broad spectrum: improvements in conduct, symptom changes, school performance, family functioning, and reductions in substance use and criminal behaviour. Participants in the family intervention were mainly adolescents and their families, and the therapists provided the interventions with varied backgrounds, including psychiatrists, clinical psychologists, social workers, and counsellors. The review unveiled that alcohol and cannabis were major studied substance use disorders among young adults with a range of co-morbid mental health disorders, including conduct disorder, attention deficit hyperactive disorder, major depressive disorder, and anxiety disorders.
Assertive Continuing Care and Adolescent Community Reinforcement Approach
Assertive continuing care (ACC) has effectively improved short-term substance use outcomes by enhancing linkage and retention in continuing care. 21 Furthermore, it surpasses usual continuing care (UCC) in linking clients to continuing care, showing significantly higher rates of marijuana abstinence. 22 The adolescent community reinforcement approach (ACRA) emerges as a successful intervention for adolescents with cannabis use disorders, exhibiting a higher recovery rate compared to motivational enhancement therapy/cognitive behavioural therapy (MET/CBT). 23 Additionally, ACRA has proven to be more effective than MET/CBT in reducing cannabis use among adolescents with cannabis use disorders. 24
Brief Strategic Family Therapy
Brief strategic family therapy (BSFT) has shown superiority over school-based interventions in reducing marijuana use and behaviour problems. 25 Moreover, BSFT surpasses treatment as usual (TAU) in its efficacy, engaging adolescents and their families in treatment and enhancing family functioning. 26 The research extends further, revealing BSFT’s comparative advantage over substance use counselling in reducing alcohol use and conduct problems among gang-affiliated Mexican-American adolescents. 27 Despite long-term follow-up studies failing to show differences in drug use outcomes between BSFT and TAU, individuals who underwent BSFT display lower rates of arrest, incarceration, and externalizing behaviors. 28
Ecologically Based Family Therapy
Ecologically based family therapy (EBFT) surpasses service as usual (SAU) in reducing substance abuse. 29 Moreover, EBFT demonstrates superiority over SAU not only in reducing alcohol and drug use but also in fostering improvement in family and adolescent functioning over time. 30 Despite the absence of a statistically significant difference in the frequency of substance use among runaways in all three treatment groups, there is a slight increase post-treatment. 31
Family-Behavior Therapy
Both Family-behaviour therapy (FBT) and individual-cognitive problem solving (ICBT) are effective in reducing substance use and conduct problems in young adults with dual diagnoses. 32 Further research is needed to determine which treatment approach is more effective for this population.
Multidimensional Family Therapy
Multidimensional family therapy (MDFT) surpasses adolescent group therapy (AGT) and multifamily educational intervention (MEI) in enhancing school/academic performance and family functioning. 33 Furthermore, MDFT outperforms ICBT in reducing substance use problem severity. 34 Applying in-session family-focused techniques during MDFT correlates with reduced externalizing and internalizing symptoms, diminished family conflict, and enhanced family cohesion. 35 A robust parent alliance in MDFT predicts declines in drug use and externalizing behaviors. 36 Highlighting its efficacy, MDFT exceeds AGT in increasing treatment completion rates and reducing substance use. 37 Additionally, MDFT outshines ICBT in producing superior treatment outcomes, particularly for youths with more severe drug use and substantial psychiatric comorbidity. 38 MDFT proves superior to individual psychotherapy (IP) by enhancing treatment retention, reducing the number of cannabis consumption days, and minimizing externalizing symptoms in cannabis-abusing adolescents.39, 40 MDFT outperforms AGT in addressing criminal behaviour and rearrests. 41 Moreover, MDFT exhibits a higher likelihood of recovery compared to CBT for adolescents with cannabis use disorder. 42 Additionally, MDFT surpasses TAU in preventing cannabis abuse. 43
Multisystemic Therapy
Multisystemic therapy (MST) has demonstrated efficacy in enhancing abstinence from marijuana and decreasing aggressive crimes. 44 Furthermore, MST proves to be equally effective as TAU in the short term, showcasing its competence in reducing alcohol and drug use, curtailing delinquent behaviors, alleviating psychiatric symptoms, and enhancing social skills and school attendance. 45
Family Check-up
Engaging in family check-up (FCU) services has been shown to predict reductions in alcohol, tobacco, and marijuana use by age 23. 46 Additionally, FCU is as effective as preventive education (PE) in reducing alcohol and other drug use outcomes among adolescents and their siblings. 47 Furthermore, FCU has been shown to reduce risky behaviors during young adulthood by linking to changes in children’s self-regulation in early middle school. 48
Other Family-based Models
Parent-skills training (PST) has proven effective in enhancing parental coping skills, self-reported functioning, and family communication while reducing teen marijuana use. 49 Strength-oriented family therapy (SOFT) and the seven challenges (7C) demonstrate effectiveness in reducing substance use and related problems among adolescents. 50 However, a parental support intervention did not exhibit superiority over a minimum behavioural intervention regarding attendance, retention, or support change. 51 A computer-delivered, parent-involvement intervention has been shown to enhance parental communication, establish family rules about substance use, and monitor daughters’ discretionary time. 52 Brief motivational intervention (BMI) outperforms parent-based intervention (PBI) in reducing heavy episodic drinking and preventing alcohol-related consequences among incoming college students. 53 A brief intervention (BI) that includes both adolescent and parent sessions produces superior outcomes compared to a BI with only adolescent sessions among adolescents with marijuana dependence disorder and co-occurring mental health symptoms. 54 Culturally informed and flexible family-based treatment for adolescents (CIFFTA) is effective in achieving significant changes in drug use and parenting practices among Hispanic adolescents with substance abuse disorder. 55 The STRIVE intervention is effective in reducing sexual risk behaviour, alcohol use, hard drug use, and delinquent behaviors among homeless youth. 56 The study found that substance-using youth receiving usual care family therapy (UC-FT) showed more significant reductions in externalizing, internalizing, and alcohol and drug use compared to those receiving nonfamily treatment. 57 Preventive intervention programs for parents revealed that adolescents with adaptive coping skills exhibited a significantly lower prevalence of binge drinking. Neither Program Comet nor Parent Steps, two parent training programs, demonstrated significant effects on adolescents’ antisocial or delinquent behaviour or alcohol use. 58 A multimedia family-based intervention effectively reduced harsh discipline practices, enhanced positive and supportive parenting, and decreased poor monitoring among participants. 59 Families Preparing the New Generation (FPNG) can effectively change substance abuse norms among youth. 60
The quality assessment scores for the selected studies ranged between 7 and 14 across the 45 studies, suggesting variability in the methodological quality of these studies. The score range indicates that some studies received lower scores (closer to 4), suggesting potential methodological limitations, while others received higher scores (closer to 13), indicating better methodological rigor.
Discussion
The systematic review consists of various family intervention models for young adults with substance abuse that are effective in reducing substance abuse, improving family functioning, and reducing behavioural problems. Among the specific family interventions reviewed, ACC and ACRA are particularly effective in achieving higher rates of abstinence from marijuana and improving treatment retention. BSFT is also a promising intervention for reducing marijuana use and behaviour problems. EBFT, FBT, MDFT, MST, and FCU are all effective in reducing substance use and improving family functioning.
The studies reviewed provide strong evidence for the efficacy of family interventions in treating substance use among young adults. It was found that incorporating family interventions into treatment led to reductions in substance consumption and improvements in family functioning. Similar findings were reported from previous studies.14–16
The quality assessment of studies in this view reveals a diverse methodological rigor across the selected literature. Notably, several studies32, 49, 38 demonstrate the robust methodology, scoring consistently high across the assessed criteria and receiving a “good” quality rating (≥75%). Few studies had poor methodological rigor. 36 Most studies fall within the “fair” quality rating (50%–75%), indicating moderate methodological rigor. These findings highlight the heterogeneity in the methodological quality of the studies reviewed, emphasizing the importance of critically assessing the risk bias in individual studies and indicating where future research could be taken up to address the lacunae in methodological limitations.
The effectiveness of family interventions can be attributed to several factors. First, family interventions provide families with the information, skills, and support they need to help their young adults recover from substance abuse.23, 55 Family interventions can improve family functioning through communication and conflict-resolution strategies. 33 Third, family interventions can help families develop healthy coping mechanisms for reducing behavioural problems among young adults.49, 55
Family interventions and other evidence-based treatments such as individual therapy and pharmacotherapy are the most effective. 35 Additionally, family interventions were ineffective in individuals with violent behaviour and co-morbid severe mental illness.55, 61 Despite these limitations, family interventions offer a promising approach to treating substance abuse among young adults. As research continues to emerge, we expect to see even more effective family interventions developed.
Our review has many strengths. The review provides an extensive overview of several family-based interventions encompassing a diverse range of approaches for young adults with substance abuse, ensuring a comprehensive review. The review’s focus on long-term outcomes, particularly for interventions including BSFT, MDFT, MST, and FCU, enhances its relevance in assessing sustained impact beyond the treatment period, providing valuable insights into the enduring effects of family interventions. The systematic review contains outcomes such as family dynamics, school/academic performance, reduction in criminal behaviour, and other problem behaviors. The review provides clear recommendations for specific interventions, emphasizing those with demonstrated effectiveness in improving substance use outcomes, family functioning, and long-term behavioural outcomes. The review may serve as valuable guidance for clinicians, researchers, and policymakers.
Limitations
Significant limitations should be considered. The review included studies that varied in participants’ demographic and clinical characteristics, design, duration, and outcome measures, contributing to heterogeneity in the evidence that challenges and necessitates a cautious interpretation of the results. The review may be susceptible to publication bias, as studies with favourable outcomes were more likely to get published. The publication bias could overstate the overall effectiveness of family-based interventions. Participants’ demographic and clinical characteristics across studies vary, impacting the generalizability of the review findings. Variations in substance use severity, co-occurring disorders, and cultural backgrounds could influence intervention outcomes. While showing positive immediate outcomes, some interventions may lack long-term follow-up data. This limitation restricts the enduring effects of specific family interventions beyond the observed study period. The review has limitations in identifying the potential adverse effects of family-based interventions. Future research may systematically investigate and report any adverse outcomes or unintended consequences.
Future Directions
Future research can strive for greater standardization in outcome measures, facilitating more robust comparisons across studies. Consistent measurement of substance use outcomes, family dynamics, and behavioural changes would enhance the reliability of the findings. Efforts may include more diverse study populations, various cultural backgrounds, socioeconomic status, and substance use profiles. This would enhance the generalizability of the findings to different demographic groups. Conducting more long-term follow-up studies for interventions, especially those lacking extended outcome data, would contribute to a deeper understanding of sustained effects. This is crucial for assessing the lasting impact of family-based interventions on young adults. Rigorous comparative effectiveness research may be prioritized to compare different family-based interventions directly. Future studies can explore the potential adverse effects of family interventions and investigate implementation challenges. Understanding potential drawbacks and barriers to implementation will inform more balanced decision-making in clinical practice. Investigating the potentials of integrating technology into family-based interventions, considering the effectiveness of artificial intelligence (AI)–assisted interventions in line with evolving healthcare delivery and technology’s increasing role in treatment.
Conclusion
The systematic review provides robust evidence supporting the efficacy of various family-based interventions in addressing substance abuse among young adults. The positive outcomes observed across different interventions underscore the importance of involving families in the treatment process. The multifaceted benefits of these interventions include improvements in substance use outcomes, family functioning, and long-term behavioural outcomes. Family-focused approaches are integral components of comprehensive treatment strategies. The systematic review findings suggest that family-based interventions hold significant promise in the prevention of and recovery from substance abuse among young adults by promoting positive family dynamics and individual well-being.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
Ethical committee approval is not required as this study is a systematic review and did not involve human subjects as participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.