
Abstract
Caregivers of patients with bipolar disorder (BD) undergo a considerable amount of burden. In India, family caregivers are the primary source of support and care for their ill relatives. The burden faced by family members of patients with BD often results in physical and mental health consequences. This may lead to negative interaction patterns such as hostility, criticality, and overinvolvement, termed as expressed emotions (EE). Here, we report how we addressed the EE in family members, using a single-subject design that involved the family caregivers (n = 2) of two adults who presented with a diagnosis of BD with a current episode of mania. An assessment of family caregivers, using the family questionnaire, revealed high EE. Family focused therapy (FFT) of 12 sessions was delivered over 3–4 weeks on an inpatient basis, with positive outcomes of reductions in EE and family stress and improved psychosocial functioning in patient that were sustained over 9–10 months. FFT can be an important add on psychosocial therapy to reduce EE and stress and to facilitate functioning and communication.
Case Report #1
A 27-year-old married lady from a rural background, with higher secondary education, belonging to the lower socioeconomic status, with 5 years’ history of BD, presented with 3 months’ history of irritability, decreased need for sleep, increased energy, increased psychomotor activity, and aggressive and assaultive behavior. The symptoms caused significant distress and burden to the family, especially the mother who accompanied her in this visit. She had a previous history of three episodes (in 5 years), each episode lasting 2–3 months.
She was admitted to the female inpatient psychiatric unit of National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru. On assessment, the therapist noticed that the current symptoms were triggered by drug default (the patient had stopped taking medicine for more than 10 months). In addition, there were family problems, as well. The mother was 56 years old, had primary school education, was widowed, and was working in a private factory. Due to the aggressive and disinhibited behavior, the patient was brought by the mother and admitted to female inpatient unit. She was diagnosed to have BD, current episode Mania with psychotic symptoms.
Details of Family Focused Therapy Session Conducted for the Caregivers of Two Cases
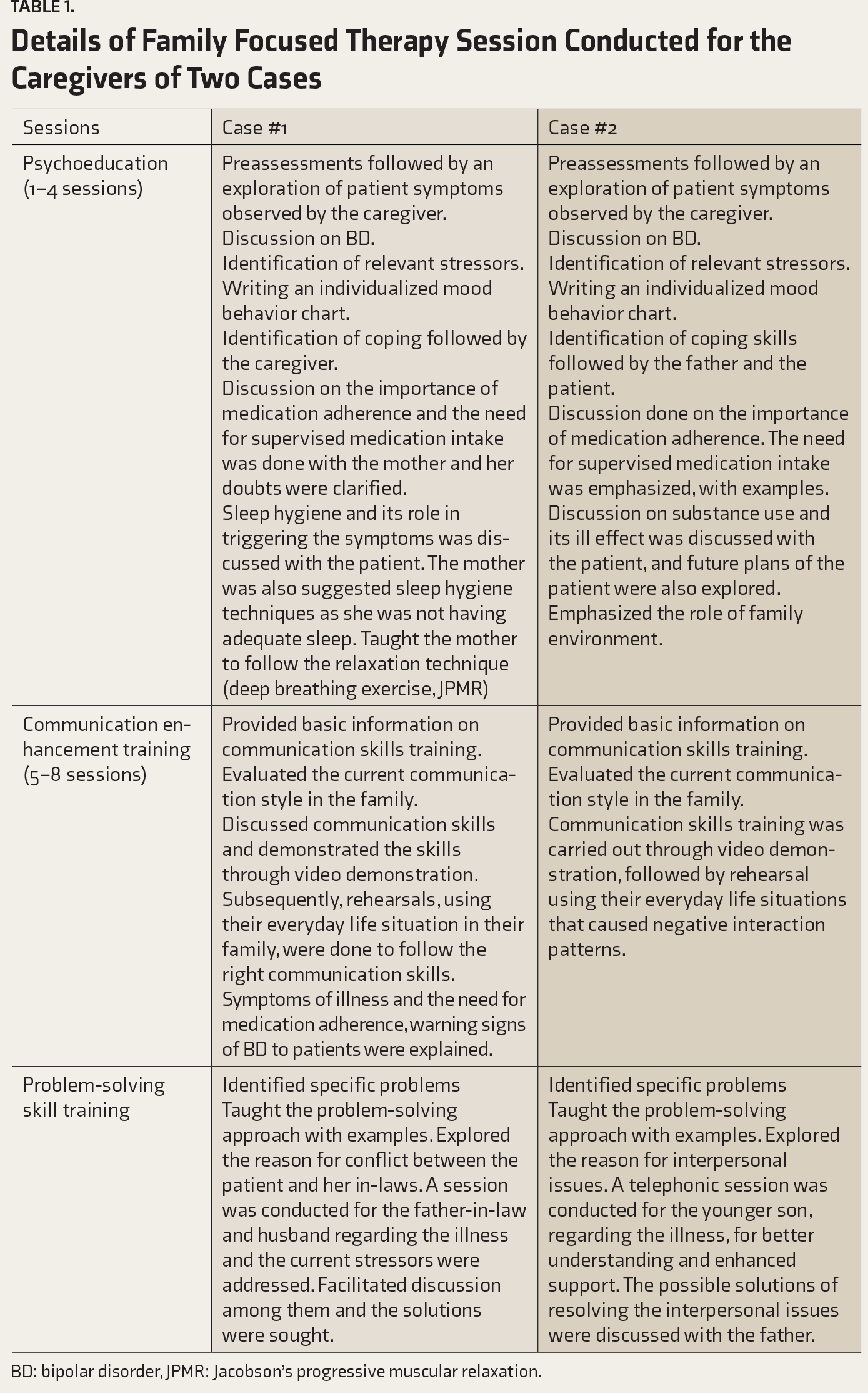
BD: bipolar disorder, JPMR: Jacobson’s progressive muscular relaxation.
The last four sessions were about problem-solving techniques, as there were interpersonal issues between the patient and her in-laws, such as the illness of the patient and differences in opinion and arguments related to the asset. The mother was taught relaxation techniques of Jacobson’s progressive muscular relaxation and deep breathing exercises. She was instructed to practice them twice a day, to reduce the stress, and advised to continue that even after the discharge. The husband, the father-in-law, and the patient were asked to attend the session to resolve the conflicts among them. They were guided to sort out the family conflicts and find solutions themselves. The therapist functioned as a facilitator only. Once the acute symptoms subsided, the patient also attended the sessions and was provided psychoeducation on the illness.
Postassessment carried out by a blind rater (blind to the therapy/intervention as well as timing of assessment), after the completion of FFT, showed a reduction in the level of EE both subjectively as well as objectively (Figure 1). On telephonic follow-ups at the 6th and 9th months after the termination of the therapy, the mother reported that the patient has been asymptomatic and that she was taking care of the children and involved in household work. The patient was taking medicine herself with the supervision of the mother. The mother’s subjective report revealed a reduction in the amount of burden vested on her.
Case Report #2
A 28-year-old single man with a diploma in engineering, from a rural background and a nuclear middle socioeconomic status family, with a duration of illness of 10 years, presented with a one-month history of irritability, sleeplessness, increased talk, singing, ideas of grandiosity, increased psychomotor activity, and aggressiveness. The current episode was precipitated by drug default (the patient refused to take medicines and has not been on medication for 1 year). The episode significantly affected the psychosocial functioning of the patient and the family environment. He had a history of 5–6 past episodes, each lasting about 2 months. He was brought by the father to psychiatric emergency services and later was admitted for inpatient care.
Interview with the father (primary care provider) revealed that the patient had frequent changes of job due to his poor performance, such as not going regularly for the job, not completing work, frequent leaves, etc., in many companies. For the last 1 year, the patient was not working and wished to act in films and demanded money. He would also force the father to buy new clothes and a motorbike.
The assessment of the father revealed significant EE, increased stress, poor knowledge regarding the illness, and interpersonal conflicts with wife over the patient’s behavior. The age of the father was 58 years. He had studied up to 8th standard and had agriculture as the main occupation. He underwent 12 tailor-made sessions of face to face FFT (
A brief telephonic session was conducted for the younger siblings regarding the illness, with an emphasis on family support, since the father reported that the younger son had frequent fights with the patient due to poor knowledge of the illness, which made him think that the behavior of the patient as purposeful.
After discharge, they were followed up in the OPD every 2 months and a telephonic follow-up was done at the 10th month. According to the report of the father, the patient had maintained well, was compliant to medication, and was helping the father in agricultural work. Father’s subjective report indicated that he felt better with respect to caregiver burden. He was now able to concentrate on his work and also supervise the medication intake by the patient. These improvements were sustained up to 10 months after the discharge.
Discussion
It is a single subject design that involves caregivers of two adult patients. Both the patients were diagnosed to have BD with a current episode of mania. The nature of the illness and the severity of the symptoms affected the social and occupational functioning of the patients as well as the family, which led to high EE and increased stress due to a poor understanding of the illness and an inability to manage the patients who were not adherent to medications. The same was reflected in objective measures of EE by family questionnaire, which was administered by a blind rater (a trained nursing professional) at both pre- and post-assessment (
Pre and Post-assessment Score on Expressed Emotions and Family Stress Among Primary Caregivers
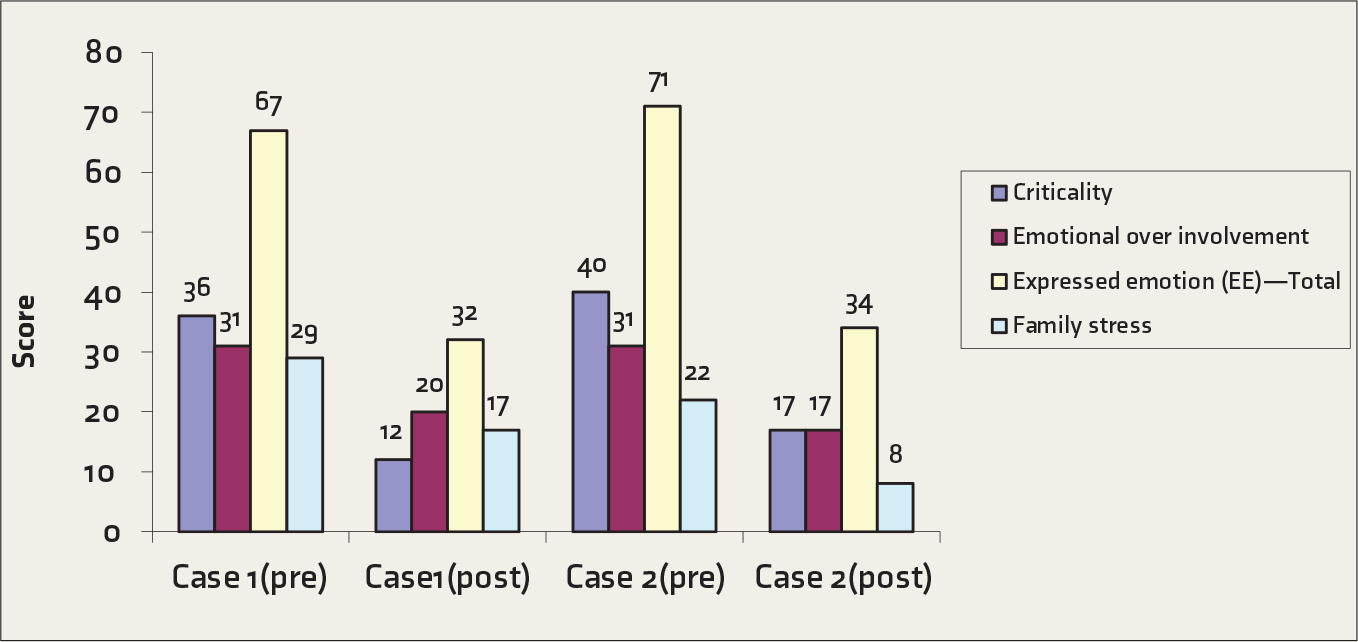
Education about illness would have majorly contributed to reduced EE and psychoeducation along the rest of the therapy components would have contributed to reduction in stress. This was maintained for 9 and 10 months, respectively, in the two patients after discharge, as reported by the caregivers. Both the caregivers did not receive any additional intervention during the follow-up period, and according to the caregivers, the patients adhered to the medications advised by the doctor. Similar results were found from the previous study where a reduction in symptoms and rapid recovery and low EE after FFT were noticed. 16 FFT plays an important adjunctive role in treating persons with BD. Implementation of psychoeducational treatments such as FFT for families of persons with BD appears to hold promise and are reported to lead to a greater reduction in relapse rates than other psychosocial treatments. 17 However, the effect of FFT on EE in family members has not been adequately examined. Thus, these case reports provide preliminary evidence for the effectiveness of FFT on EE as well as stress experienced by the caregivers. To suit the Indian setup, the frequency of the sessions was increased, and the video on communications skills was taken to suit the cultural and the patients’ family context. Since the literature on the role of FFT in the Indian subcontinent is sparse, these early findings suggest that it may be a useful adjunct to the treatment of patients with BD. Reduction in EE may indirectly have a favorable impact on the course of BD, as seen in the two patients described here. Some of the limitations of the study are using a single tool for assessing EE, not focusing on the other family dynamics, and not assessing the functioning using objective measures.
Conclusion
FFT may be a good initiative, especially in the Indian context, to improve the caregivers’ understanding of BD, which in turn reduces EE and stress and improves the communication pattern in the family, thereby leading to better interpersonal relationships, drug compliance, and relapse prevention.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr K. Muralidharan, Professor, Department of Psychiatry, NIMHANS for his support and comments on the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.