
Abstract
The dissociative motor disorder is one of the most commonly diagnosed forms of dissociative disorder in the Indian population, especially among adolescents. However, there is a dearth of literature on effective psychotherapy practices in the Indian setting. This article details the unique process of employing an integrative psychotherapy approach with a 16-year-old adolescent girl diagnosed with dissociative motor disorder who presented with complaints of headache, deviation of mouth, multiple somatic complaints, inability to move her legs, episodes of loss of consciousness with jerking of upper limbs and a non-pervasive low mood. A detailed evaluation highlighted significant disruptions in attachment with caregivers, complicated grief, significant anger towards her family which did not find a space for expression, unhealthy coping mechanisms in the background of a slow-to-warm-up temperament and sociocultural stressors. The case formulation drew elements from the psychodynamic perspective, family systems approach, biosocial theory and the cognitive behavioural perspective. The intervention from the first session until termination is delineated in different phases which outline the significant themes that emerged along with the techniques used, challenges faced and therapist reflections. The role of the therapeutic alliance, working through transference, systemic work, primary and secondary gains and the importance of defences along with the aftermath of losing them becomes especially salient as the psychotherapy progresses in this case. The implications of the therapy process that can hold relevance to the management of dissociation disorder in the clinical setting are also discussed.
The dissociative motor disorder is a form of dissociation marked by a loss or alteration in physical functioning without any neurological or physical difficulty. 1 It can be a defence against a psychological conflict. 2 Early relational trauma and an insecure attachment are commonly associated with dissociation. 3 Primary and secondary gains that maintain the symptoms also accompany. 4 Further, theories like the window of tolerance model implicate the role of overwhelming emotional experiences and arousal in dissociation (a state of hypo arousal). 5 Hence, several factors underlie dissociation. This article highlights a unique case of dissociative motor disorder where an integrative approach was beneficial in addressing the multiple factors contributing to the symptoms. The process of therapy, therapist reflections and challenges are outlined.
Step 1—Clinical History and Assessment
A 16-year-old female studying in 10th grade from India, presented with complaints of headache, deviation of the mouth towards the left, multiple somatic complaints, inability to stand and move legs, episodes of loss of consciousness with jerking of upper limbs and a non-pervasive low mood.
History revealed the death of the patient’s father four years ago due to a stroke, and the mother’s remarriage after one year. Following this, she began experiencing fainting spells and shivering in upper and lower limbs without any neurological explanation. The EEG and MRI findings were within normal limits with no neurodevelopmental issues. The child lived at her maternal uncle’s house since the age of 13 when her mother moved away after remarriage, where she was allegedly criticised and neglected. During this time, she developed frequent headaches and pseudo-seizures exacerbated by interpersonal and academic stressors. They then consulted at the current study centre, a tertiary care hospital with mental health services for children and adolescents where inpatient admission was suggested. Along with psychotherapy, pharmacological interventions involved antidepressants followed by a mood-stabiliser, antipsychotic and benzodiazepine.
She is a single child. Perinatal history revealed a C-section delivery due to less amniotic fluid with no other complications. The mother reported physical weakness postnatally, as she was in her teens. Postnatal depression was not reported. The child stayed with her maternal grandmother for the first five years sharing a close bond with her with intermittent contact with her parents. Following her grandmother’s death, the child was brought back to her parents’ house. Here, she developed a closer attachment with her father as, according to the mother, the father was permissive while the mother was disciplinary suggesting inconsistent parenting styles. Temperamentally, she was slow to warm up, with an irritable mood, low adaptability, low responsiveness and high sensitivity to criticism. 6
Clinical Diagnosis
Rutter’s multiaxial diagnosis revealed the following:
7
Axis I—Dissociative motor disorder Axis II—Nil Axis III—Average intelligence Axis IV—Nil Axis V—Criticality, hostility from family members
Step 2—Initial Phase (Building Rapport and Further Exploration)
The therapeutic alliance has great significance in determining outcomes in dissociation. 8 Hence, the goals in this phase were to build rapport and create a secure and consistent therapeutic environment to facilitate expression, given her insecure attachment style.
The adolescent entered the first session in a wheelchair. The therapist built rapport by striking conversation about her interests while also focusing on identifying significant themes and patterns in her thought process. She spoke of feeling lonely and isolated following her father’s demise. She felt betrayed by her mother as she had left after re-marrying and would only speak to her ‘when she was sick’. Further, when her uncle shouted at her, she used to cope by keeping quiet, going to her room, switching off the lights, closing her eyes and lying down in darkness. She said, ‘I like darkness’.
It was evident that the adolescent had difficulty expressing emotions, had an internalising temperament and tended to cope through isolation. She expressed feelings of abandonment and betrayal. The functions of her symptoms were keeping her mother close with gains of attention and concern. There was significant unresolved grief over her father’s death.
The difficulties in emotional expression, unprocessed grief and an insecure attachment style required more than one kind of approach to intervention as indicated in the literature.9–14
Step 3—Case Formulation
The case was formulated using an integrative psychotherapy approach drawing from the psychodynamic perspective (attachment theories), dialectical behavioural therapy (DBT) approach, cognitive approach and family systems approach and interpersonal therapy (Figure 1).
Representation of the Integrative Case Formulation.
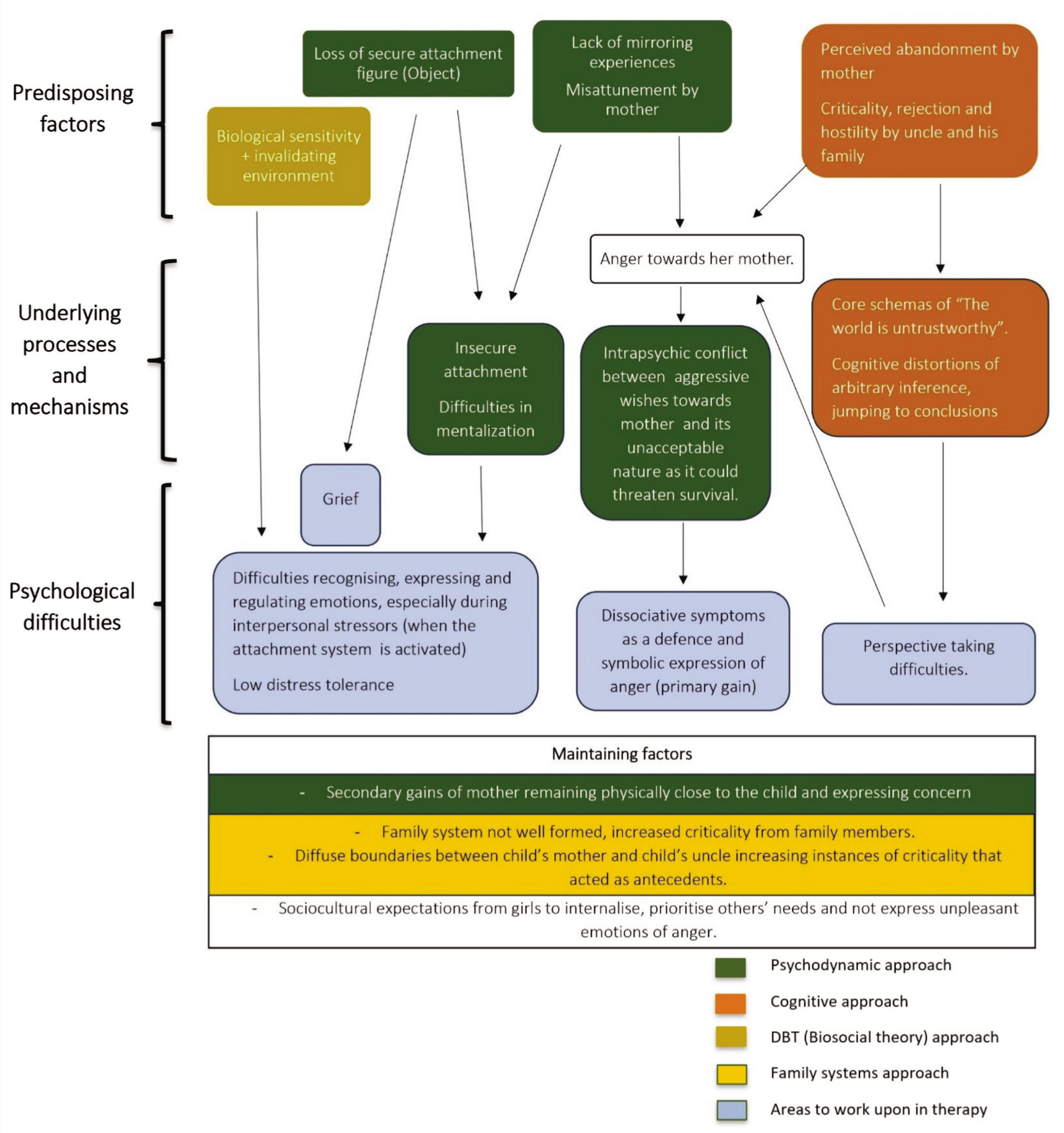
Her infancy was marked by a close attachment to her grandmother and reduced proximity to her parents. From a psychodynamic perspective, her grandmother’s death marked a disruption in attachment with the primary caregiver. She moved in with her parents at the age of five, where she reportedly experienced criticality, disciplinary measures and less warmth from her mother. This suggested misattunement, characterised by a lack of mirroring and maternal mind-mindedness which may explain the child’s difficulty in regulating emotions.
After this, there was the loss of another secure attachment figure (her father) followed by repeated experiences of invalidation, rejection and hostility in her uncle’s house. This possibly contributed to an insecure attachment with complicated grief. Attachment to her mother seemed insecure-ambivalent (she was an inconsistent figure and remained excessively concerned, yet critical). In other relationships, she had a preoccupied attachment with a negative internal working model of others, viewing them as untrustworthy. Furthermore, having her mother physically close was a gain while dissociative symptoms could be a defence against unresolved anger towards the mother (stemming from misattunement, criticality, rejection and abandonment).
From a cognitive perspective, the adolescent harboured core beliefs about the world and people being untrustworthy with cognitive distortions like arbitrary inference and jumping to conclusions (leading to a negative interpretation of her mother’s actions and difficulties in perspective-taking). This distressed her and served as an antecedent for dissociative episodes.
From a DBT (biosocial theory) perspective, the child’s temperamental vulnerabilities of emotional sensitivity coupled with an invalidating environment could explain emotional dysregulation, low distress tolerance and interpersonal challenges which also contributed to the symptoms.
A systems perspective indicated a poorly formed family system containing a disengaged and uninvolved mother who lived elsewhere. The parental sub-system showed inconsistent parenting along with diffuse boundaries between the mother and uncle as the former often let him make decisions about her child. The adolescent’s symptoms could be viewed as an attempt to gain power over her mother and keep the family together.
Step 4—Setting the Frame and Establishing Goals
A total of 35 sessions, around four per week, were held ranging from 30 to 60 minutes each and therapeutic techniques were integrated using psychodynamic models, cognitive behavioural therapy, dialectical behaviour therapy and interpersonal therapy.
The goals were:
Psychoeducation and reattribution Uncovering unprocessed emotions and conflicts Addressing grief Building a sense of agency Broadening social support
Step 5—Middle Phase of Therapeutic Intervention
This phase has been delineated in five sections based on significant themes.
Externalising the Internal
This phase focused on fostering healthy emotional expression and reducing dissociation in the face of overwhelming emotions. The therapist discussed the importance of expression using analogies (e.g., pressure cooker metaphor) and alternative ways of expressing through art, writing and talking to friends. Her initial resistance against self-expression was driven by guilt that she was defaming her family which was reframed into an act of genuine expression of her perspective.
It was crucial to empower her to build agency and reinforce her sense of self which could provide a buffer against dissociation. Her repressed emotional experiences, which only found an outlet through somatic symptoms, required mentation. This was facilitated by discussions about recognising her emotions and prioritising her needs.
Psychoeducation and Building Intra and Interpersonal Resources
This phase focussed on psychoeducation, reattribution of symptoms and enhancing the adolescent’s coping skills. Using Goldberg’s reattribution model, the therapist validated the distress associated with her symptoms without questioning their truthfulness. 15 The mind-body reciprocity was discussed using examples to signify the mutually impactful relationship between the mind and body. A timeline linking the exacerbation of her somatic complaints with psychological stressors helped facilitate a deeper understanding of her illness.
Grounding and distress tolerance skills were introduced with a rationale and situations where they can be useful. Subsequently, psychoeducation with her mother involved discussing psychological gains and enhancing communication with the adolescent.
The Unconscious Becomes Conscious
We never talk about my father. Everyone moved ahead and forgot him
(a quote from the adolescent).
During this phase, her grief became apparent. It was crucial to help her build a rich narrative of her father’s loss. She would break down during these sessions which was contained by the therapist. At times, silence and evocative language would encourage free expression and allow unconscious content to emerge which was met with a safe space and acceptance. She described the suddenness of her father’s death and the things that she could not convey to him. The therapist proposed that she write a letter to her father expressing all that she wanted to. The choice of reading it was up to her.
Her grief also encompassed a perceived loss of her mother associated with anger, resentment and hurt. Acknowledging these feelings brought in improvement in symptoms. However, losing the symptom also meant lowering defences which brought about low mood, suicidality and self-injurious behaviours, exacerbated by invalidating comments from her mother. Her self-harm tendencies resulted from her intense and unbearable anger towards her family, which she turned inwards resulting in depression. 16 Hence, validation and promoting safety without challenging her thoughts was important. An incident depicting this stance involved the adolescent snatching away the therapist’s pen to harm herself which was held firmly by the therapist expressing genuine concern for her safety without fighting her back. A course of electroconvulsive therapy also contributed to managing her suicidality at this point of treatment.
Further depressive symptoms were addressed through behavioural activation. To keep her engaged, the therapist partook in games with her as she was not willing to do activities on her own and encouraged her to do the same with other patients. Alternatives to self-harm were discussed. Cognitions associated with self-harm were reframed as ways to regulate herself in the face of hearing critical comments from her mother. A gradual reduction in self-harm was observed.
Re-experiencing the Mother and Motherhood
I have siblings whom I love very much. I feed them, take care of them when they are sick. They call me ‘Maa’…
(a quote by the adolescent expressing her idea of the desired mother)
As therapy progressed, she started expressing anger towards her mother with frequent outbursts and yet walked clinging onto her arm (exhibiting her ambivalent attachment style) indicating a strong need for maternal warmth and affection. This ambivalence extended to her other relationships where she desired closeness but had difficulty trusting them. The therapist reflected on this ambivalence and acknowledged its presence in close relationships. 17 Furthermore, elements of perspective-taking to help mentalise her mother’s actions were introduced. It was seen that dissociative symptoms along with keeping her mother close were also a way of expressing anger towards her, given the mother’s distress associated with the prolonged hospitalisation. Hence, expressing the primary emotion of hurt behind the anger was encouraged. Sessions with the mother were held by social workers who to discuss adaptive responsiveness towards the adolescent.
At this point, transference became significant. The adolescent would feel angry if a session was deferred, despite being informed in advance, and would often cling to the therapist’s arm while walking. Additionally, her dissociative symptoms disappeared in the presence of the therapist, possibly due to a validating environment as her distress could be expressed without physical symptoms. Experiencing the therapist as a mother figure extended her anger and need for affection in the therapeutic relationship. The therapist maintained a safe, validating, consistent environment with unconditional positive regard which could serve as a corrective emotional experience for the adolescent. 17
A challenge was to reduce the gains for her dissociative symptoms. It was a delicate balance to maintain between not providing gains without seeming unconcerned, especially when the adolescent dissociated in a session, to which the therapist responded by gently calling her name without reacting with excessive anxiety or concern.
Fear of Losing a Safe and Secure Space
As she improved, a discharge plan was discussed which led to an exacerbation of suicidal ideation and low mood. Her symptoms would worsen when she anticipated a conversation about discharge underscoring the fear of returning to an unsupportive home environment. It was discussed that the hospital environment may have become a gain and a phased-out discharge would be beneficial. The adolescent seemed to view discharge as abandonment (linked to her earlier experiences) leading to an exacerbation in anger and suicidal ideation.
Discussing about discharge was a challenge. The therapist acknowledged her distress about going back home but also discussed the importance of her health to the treating team. It was discussed that discharge was also vital in evaluating how she copes in a natural environment and helping in planning further interventions. Through this, discharge was reframed as an act of care rather than an act of abandonment. With this, the adolescent agreed for discharged and stayed as an outpatient to ensure a smoother, phased-out termination.
Step 6—Termination Phase
Process
After discharge, she was seen on an outpatient basis for a week. The skills and prior discussions were reviewed. Post-discharge the adolescent was to stay with her mother and stepfather along with a hostel as an alternative option. Discussions were done with the mother on establishing boundaries with the adolescent’s uncle and reducing criticality to create a nurturing environment. The mother agreed to be more involved with the adolescent. Before the adolescent went back, she asked for a way to contact the therapist and an email ID was provided explaining when and how she could contact the therapist if required.
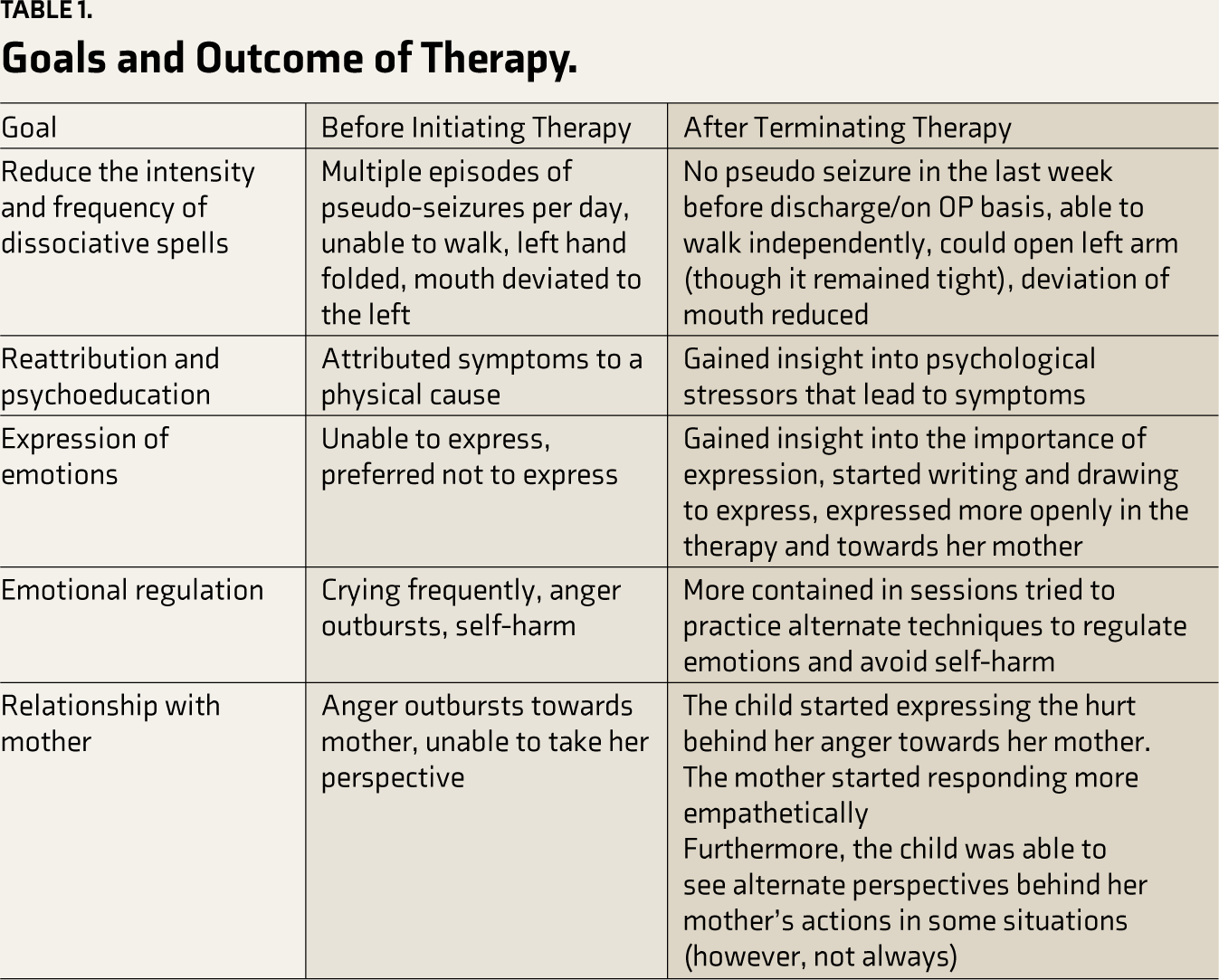
Outcome
The outcome of the therapy is summarised in Table 1.
Goals and Outcome of Therapy.
Step 7—Follow Up
For six months, the adolescent maintained well following which there was increased criticality from the extended family. She presented with depressive symptoms a year after terminating therapy and was provided with appropriate interventions and referrals. A stable gain from previous treatment was the significant improvement of dissociative symptoms which was reflected by her expressions of emotions such as guilt and anger. Her depressive symptoms reduced gradually with no return of dissociative symptoms leading to healthy socio-adaptive functioning.
Reflections and Discussion
This case highlighted the importance of understanding the meaning and functions of symptoms. Symptoms communicate what cannot be conveyed healthily (anger towards family in this case) due to certain constraints. Hence, listening to the need behind the symptoms, what they are defending against, and their purpose is essential in planning interventions with individuals with dissociation. Addressing these can have a trickle-down effect, leading to reduced symptoms and enhanced well-being.
Second, therapists often shy away from using the word integrative or eclectic. However, this case demonstrates how addressing the major problem areas through different suitable approaches can be beneficial.14,18 Most pathology involves complex contributing factors and integrating approaches to holistically address them is indicated especially in dissociative disorders. 14 However, one needs to be careful about the timing and rationale behind incorporating these techniques. For this case, techniques of reattribution provided insight into her symptoms and aetiology. 15 Techniques to address grief (evocative language, letter writing, narrating the incident) and emotional regulation (labelling, discussing primary and secondary emotions, alternate methods of expression) helped verbalise and process conflicts and non-mentalised emotions.13,19 Grounding and distress tolerance skills helped broaden the window of tolerance whereas behavioural activation, reframing and perspective-taking helped address core beliefs to reduce unpleasant affects, thereby, ameliorating distress and antecedents for dissociation.5,13,18 A strong therapeutic alliance, working through transference, containment and consistency along with empathetic and active listening brought about corrective emotional experiences to manage attachment injuries.8–11 Hence, all these techniques were integrated and utilised at appropriate times to help the adolescent.
Third, the importance of working through transference was apparent in this case. Working through may not necessarily include confrontation or interpretation but an acknowledgement of the need behind it to, provide an environment that fulfils it, which can be extremely beneficial and serve as corrective emotional experiences for the patient.
Lastly, this case highlights the socio-cultural factors that contribute to pathology. The adolescent came from a rural village in India where cultural stressors prevented her from staying with her mother. Patriarchal notions prohibited girls from expressing difficult emotions, further strengthening her internalising coping style. Building a stronger sense of identity and normalising feelings and expressing emotions, along with systemic work form an important part of the intervention, especially for women in the Indian subcontinent.1,20
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from The Institutional Ethical Committee—Behavioural Sciences Division at the National Institute of Mental Health and Neurosciences, Bengaluru, India [Reference No: NIMHANS/EC (BEH.SC.DIV.)MEETING/2023].
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
The adolescent and her mother both consented to psychotherapy treatment. The adolescent and her mother both provided written informed consent for the publication of anonymised data.