
Abstract
Background:
Delirium is a reversible state that, if ignored, can result in increased morbidity and mortality. Studies from across the world have shown that nurses’ knowledge regarding delirium is inadequate. This study is one of the very few Indian studies addressing this issue. The study aims to infer an intensive care unit (ICU) nurse’s knowledge regarding delirium.
Materials and Methods:
This is a descriptive study carried out in the ICUs of a multispecialty general hospital. A convenient sample of 220 nurses was recruited after obtaining written informed consent. Knowledge regarding delirium was ascertained using the Delirium Knowledge Questionnaire; this, along with the sociodemographic variables, was circulated as Google Forms through WhatsApp groups. Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 26, and results were presented as means and percentages.
Results:
The present study reveals that out of 211 nurses 130 (61.6%) had an average knowledge about delirium. Out of the 211 nurses 108 (51.2%) had average knowledge about clinical features of delirium and 105(49.8%) had average knowledge about etiology of delirium. More than half of the nurses (53.1%) had awareness regarding the medical management of delirium. In the domain of knowledge regarding non-medical management, 81 (38.4%) had excellent knowledge and 114 (54%) respondents had average knowledge regarding the prevention of delirium.
Conclusion:
The study calls for the need to provide educational interventions to the nursing staff for prevention, prompt recognition, and treatment of delirium.
Presented orally on 9/9/2023 at SIPSCON 2023—State conference of IPS Kerala Branch-Awarded the Young Psychiatrist Award.
This research elucidates knowledge of delirium among ICU nursing staff using the Delirium Knowledge Questionnaire. This research reveals that the nurses have only average knowledge regarding delirium.Key Messages:
Delirium is a reversible neurocognitive disorder, commonly diagnosed among hospitalized patients. This condition is common in intensive care unit (ICU) patients, with a prevalence ranging between 16.1% and 68.2% in various settings. 1 Though this is a crucial condition in the ICUs, studies suggest that this condition is inadequately diagnosed and treated in the ICUs. 2 Though recognizing delirium at the earliest is very critical, its treatment and prophylaxis are of low priority in ICUs with inadequate manpower.3,4 Delirium cannot be identified unless we monitor patients for the same. 4 Sadly, studies prove that delirium remains an enigma to the medical and nursing staff.5,6 Studies from across the globe have shown that nurses’ knowledge regarding delirium control in ICUs is inadequate. Unfortunately, there are huge gaps in Indian literature addressing this issue.
Delirium is characterized by (1) a disturbance in attention; (2) an acute onset representing an acute change from baseline attention and awareness, tending to fluctuate in severity during the day; (3) disturbance in cognition; (4) the mentioned disturbances are not explained by a pre-existing or evolving neurocognitive disorder; and (5) there is evidence that it is a direct physiological consequence of another medical condition, substance intoxication, or other multiple etiologies. 7 According to studies, the prevalence of delirium ranges from 32% to 80%. 8 It is a medical emergency that can increase morbidity and mortality. Furthermore, the economic burden of delirium is tremendous, as it increases the duration of hospital stay and the length of ICU stay.9,10 Delirium has a catastrophic effect on the prognosis and often results in neurocognitive sequelae after ICU hospitalization. 8 Many systematic reviews and meta-analyses substantiate that the most common risk factors for delirium are old age, medical and surgical comorbidities, impaired vision, dehydration, dementia, the retainment of a urinary catheter, and prolonged hospitalization. 11 However, early diagnosis of delirium guarantees favorable patient outcomes and is correctable with the treatment of the underlying etiology. 12
The major workforce in ICUs is the nursing staff and they are well equipped to carry on with treatment. 5 Their awareness, disposition, and implementation of treatment guidelines have a key role in diagnosing, managing, and preventing diseases. 13 Research reveals that a counteractive disposition by nurses affects the quality of services they provide. 14 Studies show that they are not knowledgeable enough to diagnose delirium, are not confident to care for delirious patients, and are confused regarding managing delirium. 15 Some of the studies also elucidate that managing delirium is not a top priority for the majority of the nurses. 16 Indian data regarding the knowledge of nurses about delirium is scarce. This study aims to ascertain the level of knowledge among ICU nursing staff about delirium at a multispecialty general hospital. This study may elucidate the need to provide educational programs for the nursing staff.
Materials and Methods
This descriptive study was done in the medical and surgical ICUs of a multispecialty general hospital in southern Kerala. The study population was nursing staff working in the surgical and medical ICUs. The nursing staff who had given written informed consent and who had at least 1 year of working experience in the ICU were recruited for the study. Nursing trainees were excluded from the study. A convenient sample of 220 nurses was recruited for the study.
Two questionnaires were used for the purpose of this study. The first questionnaire had questions evaluating the demographic information, place of work, educational qualification, duration of experience in the ICU, and previous training experience regarding delirium. The second questionnaire was the delirium knowledge questionnaire formulated by Christensen. 17 Both questionnaires, along with the informed consent, were entered in a Google Form format. Delirium Knowledge Questionnaire was used in the study after getting permission from the author. 18 An answer sheet was also obtained from the authors. The questionnaire is self- reported and has 35 questions in true or false format. The first ten questions of the Delirium Knowledge Questionnaire pertained to symptoms and signs of delirium. The next 11 questions were related to the risk factors of delirium. The final set of questions covered the management of delirium.
The study was initiated after getting clearance from the institutional ethics committee. After obtaining approval from the nursing heads, the study was initiated. The questionnaires were circulated among the nurses through the respective WhatsApp groups.
Data collection took place between April and August 2023. This study does not make use of artificial intelligence.
Results
Due to reasons of repetition and incompleteness, nine questionnaires were rejected. Ultimately, 211 questionnaires were included in the study. Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 26. The data were entered into an Excel sheet. All descriptive statistics were expressed as mean ± standard deviation (SD) for continuous variables and number or percentage for categorical variables. A comparison of the means of the delirium score with education and previous training experience regarding delirium was done by the Student’s t-test after checking the normality assumptions. The comparison of the means of the delirium score with the workplace and years of experience was done by the analysis of variance. The delirium score and the association with education, workplace, years of experience, and previous training experience about delirium were determined by a chi-square test. To analyze the factors associated with excellent knowledge of delirium, logistic regression analysis was used. The level of significance was considered to be 0.05. For the purpose of this study, the overall scores yielded from the Delirium Knowledge Questionnaire were classified as poor (0–11), average (12–22), and excellent (23–35). The questionnaire was categorized into five subdomains: (1) knowledge about clinical features of delirium (n = 10 items), (2) etiology and causative factors (n = 11 items), (3) knowledge about medical management (n = 1), (4) knowledge about non-medical management (n = 2), and (5) knowledge about delirium prevention (n = 11). These scores were also categorized into three categories, that is, poor, average, and excellent, in a similar manner as above.
Profile of the Participants
The study evaluated the data from 211 female registered nurses (mean age: 32.2 years and SD of 6.5 years) working in the ICU. Among the 211 nurses, 96 (45.5%) subjects had 1–5 years of experience in the ICU, 72 (34.1%) had 5–10 years, and 43 (20.4%) had 10–15 years of experience. The majority of the participants had a bachelor degree in nursing (129 (61.1%) out of 211 nurses and the rest had a diploma in nursing (38.9%)). Notably, 60 (28.4%) nurses were associated with the cardiac ICU, 59 (28.0%) with the medical ICU, 62 (29.4%) with the neurology ICU, and 30 (14.2%) with the surgical ICU. Out of 211 nurses, 165 (78.3%) of the nursing staff have attended previous training sessions on delirium (Table 1).
Profile of Participants.
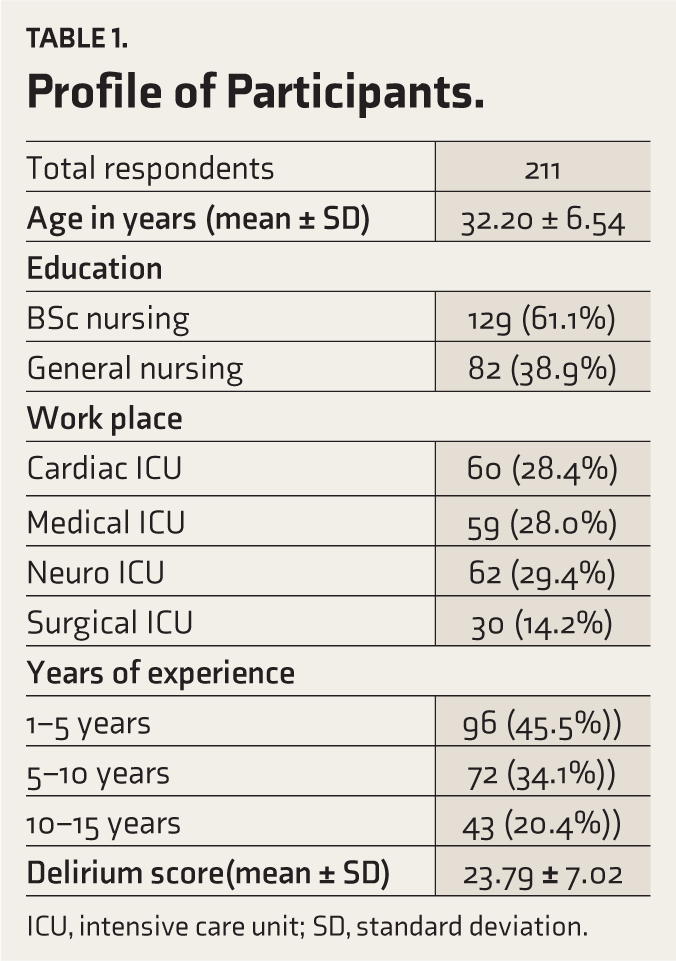
ICU, intensive care unit; SD, standard deviation.
Nurse’s Knowledge of Delirium
The tool had 35 questions. The overall scale and the five subdomains were analyzed to yield the results. The mean delirium score obtained was 23.79, with an SD of 7.02.
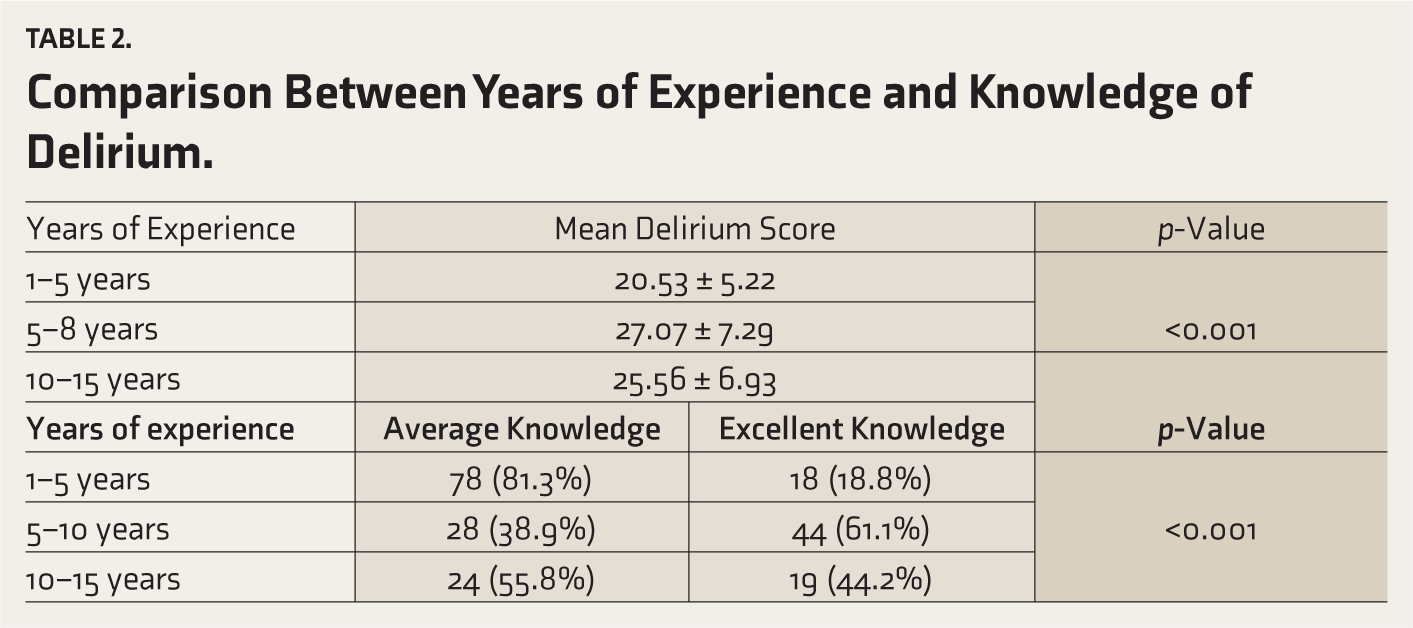
A significant association was obtained between knowledge and years of work (p < 0.001). The mean delirium score was higher among nurses with 5–10 years of experience, immediately followed by nurses with 10–15 years of experience. Comparison between years of experience and categories of delirium score (poor, average, and excellent) also yielded statistically significant results in the 5-year to 10-year experience group. Out of 72 nurses with 5–10 years of experience, 28 (38.9%) had average knowledge regarding delirium and 44 (61.1%) had excellent knowledge (p < 0.001) (Table 2).
Comparison Between Years of Experience and Knowledge of Delirium.
A significant association was also obtained between knowledge and previous educational sessions on delirium (p < 0.001). Among the nurses who had attended classes on delirium previously, 78 (51%) had average knowledge regarding delirium, and 75 (49%) had excellent knowledge regarding delirium. Only 10.3% of nurses who had no prior exposure to delirium awareness classes had excellent knowledge regarding delirium. The results obtained were significant with a p-value less than 0.001. Out of 72 nurses, 59 with an experience of 5–10 years attended previous training on delirium (82%) as compared to 72% with 10–15 years experience (Table 3).
A significant association was also elicited between knowledge of delirium and the participant’s clinical setting. Those nurses working in the surgical ICUs produced a higher mean delirium score of 32.83 and an SD of 4.12. This group was followed by nurses working in the neurology ICUs who had a mean delirium score of 25.29 and an SD of 7.62. The nurses working in the medical ICUs had a mean delirium score of 20.17 ± 3.87. Those working in the cardiology ICUs had a mean delirium score of 21.27 ± 5.39. These results also were statistically significant (p < 0.001).
However, no significant association could be seen between educational qualification and level of knowledge regarding delirium (p = 0.060).
Out of 211 respondents, 130 (61.6%) had an average level of knowledge about delirium and 81 (38.4%) had excellent knowledge regarding delirium. Out of 211 respondents, 6 (2.8%) had poor knowledge about the clinical features of delirium (n = 10 items), 108 (51.2%) had average knowledge, and 97 (46.0%) had excellent knowledge. Regarding knowledge about the etiology and causative factors of delirium, 18 (8.5%) had poor knowledge, 105 (49.8%) had average knowledge, and 88 (41.7%) had excellent knowledge. More than half of the nurses (53.1%) had awareness regarding the medical management of delirium. In the domain of knowledge regarding non-medical management, 66 nurses (31.3%) had poor knowledge, 64 (30.3%) had average knowledge, and 81 (38.4%) had excellent knowledge. Of note, 114 (54%) respondents had average knowledge regarding the prevention of delirium, 8 (3.8%) had poor knowledge, and 89 (42.2%) had excellent knowledge (Table 4).
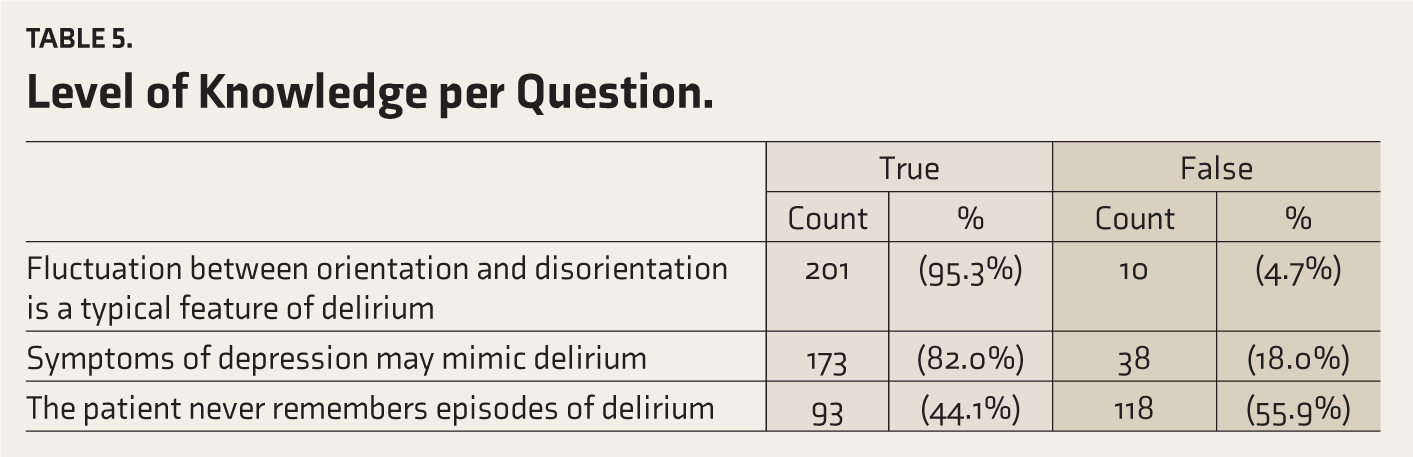
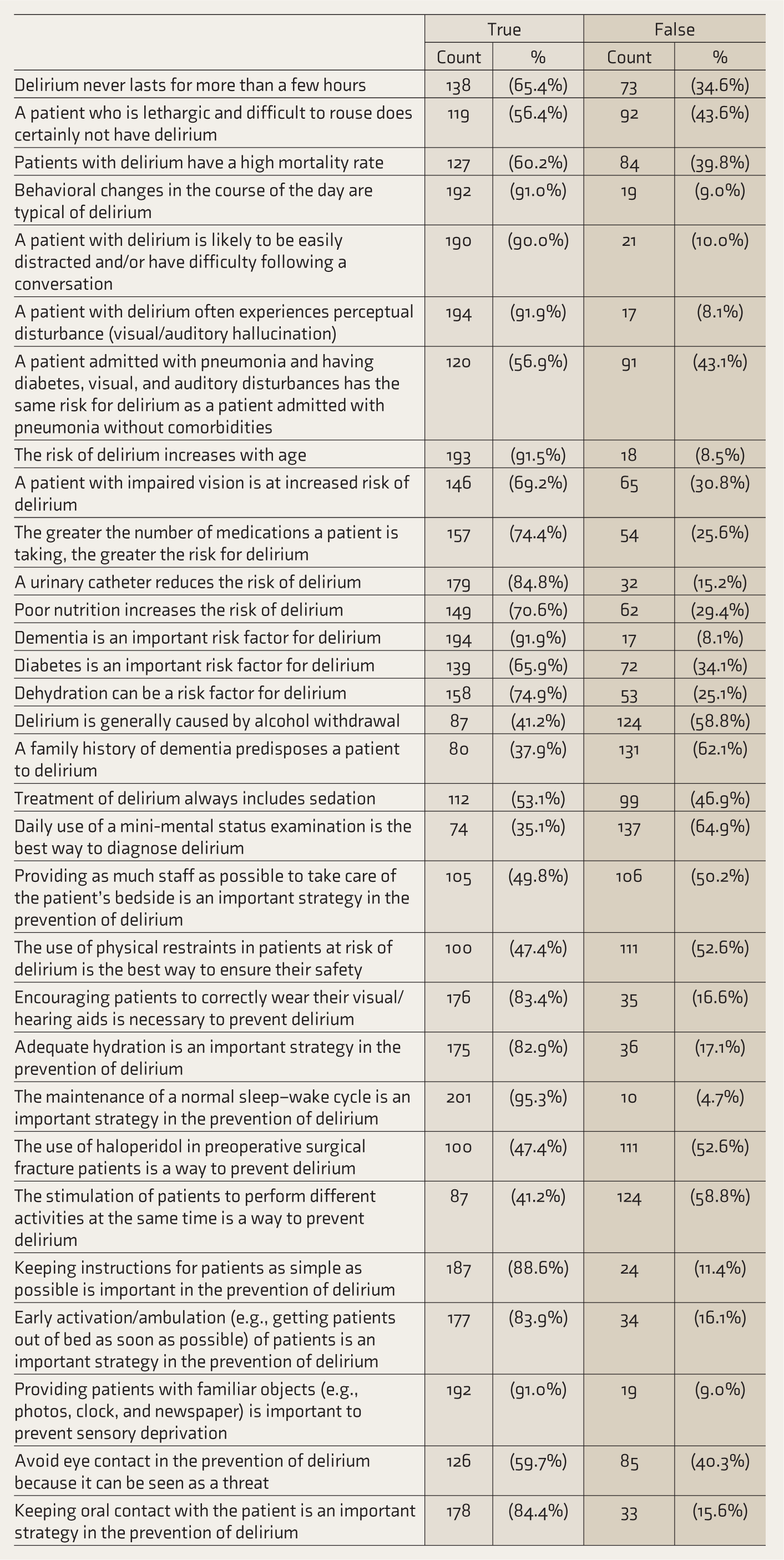
Level of Knowledge per Question
More than 50% of the nurses gave wrong replies to questions on causative factors of delirium, diagnosing delirium, and pharmacological and non-pharmacological management of delirium.
More than 90% of the nurses correctly answered questions about the definition of delirium, clinical features of delirium, causative factors, and non-pharmacological management of delirium (Table 5).
Factors Influencing Excellent Knowledge of Delirium
Univariate and multivariate analyses revealed that previous training experience about delirium and years of work experience significantly contributed to excellent knowledge regarding delirium. It was found that in the univariate analysis, by holding 1–5 years of work experience as constant, the odds of excellent knowledge of delirium were 6.81 for those nurses with 5–10 years of experience and 3.43 for those nurses with 10–15 years of experience (95% confidence interval). In the multivariate analysis, the odds ratio was 6.42 and 3.56, respectively (95% confidence interval).
It was also found that for those nurses who had previous training experience in delirium, the odds of excellent knowledge of delirium were 8.33 (95% confidence interval).
Discussion
This research elucidated the knowledge of 211 ICU nurses about delirium. Nurses in the ICU are proficient at detecting patient’s changes in cognition, and hence their role in diagnosing and managing delirium is paramount. 19
In this study, more than half (61.6%) had average knowledge, 38.4% had excellent knowledge, and none of the participants had poor knowledge. A similar study by Shreshtha et al. 20 revealed that about 65.9% of nurses had moderate knowledge of delirium. In a study by Xing et al. 21 , more than half of the nurses had an intermediate level of knowledge about delirium. Similar results have been obtained in other studies investigating nurses’ knowledge about delirium.5,22 However, another study conducted in North India found that ICU nurses had poor knowledge and were not confident in diagnosing and managing delirium. 16 This finding is in line with many other studies that have revealed the inadequacy of knowledge of delirium.5,23 Furthermore, a systematic review also reported that nurses had poor knowledge regarding delirium and were unable to detect it. 9
There was a significant association between work experience (p < 0.0010) and knowledge. An equivalent study by Shreshtha et al. 19 also supports this finding that there is a significant association between work experience and level of knowledge. However, the study by Elfeky and Ali 24 revealed that there is no association between knowledge and work experience.
This study also reveals a statistically significant association between previous training and knowledge of delirium. This is similar to the results made by Hamdan-Mansour et al. 25 and Yue et al. 26 A previous study from South India connoted that providing educational sessions to nurses about delirium can improve their knowledge. 27 Many studies have found that educational programs improve nurses’s knowledge about delirium.28,29
This study reveals that nurses with 5–10 years of experience in the ICU had more knowledge regarding delirium. This could be due to the fact that the majority of the participants (82%) in this group have attended training sessions on delirium previously, thus substantiating the above finding. Notably, 72% of those nurses with 10–15 years of ICU experience had previous training experience in delirium (Table 3).
Level of Knowledge and Previous Training Experience on Delirium.
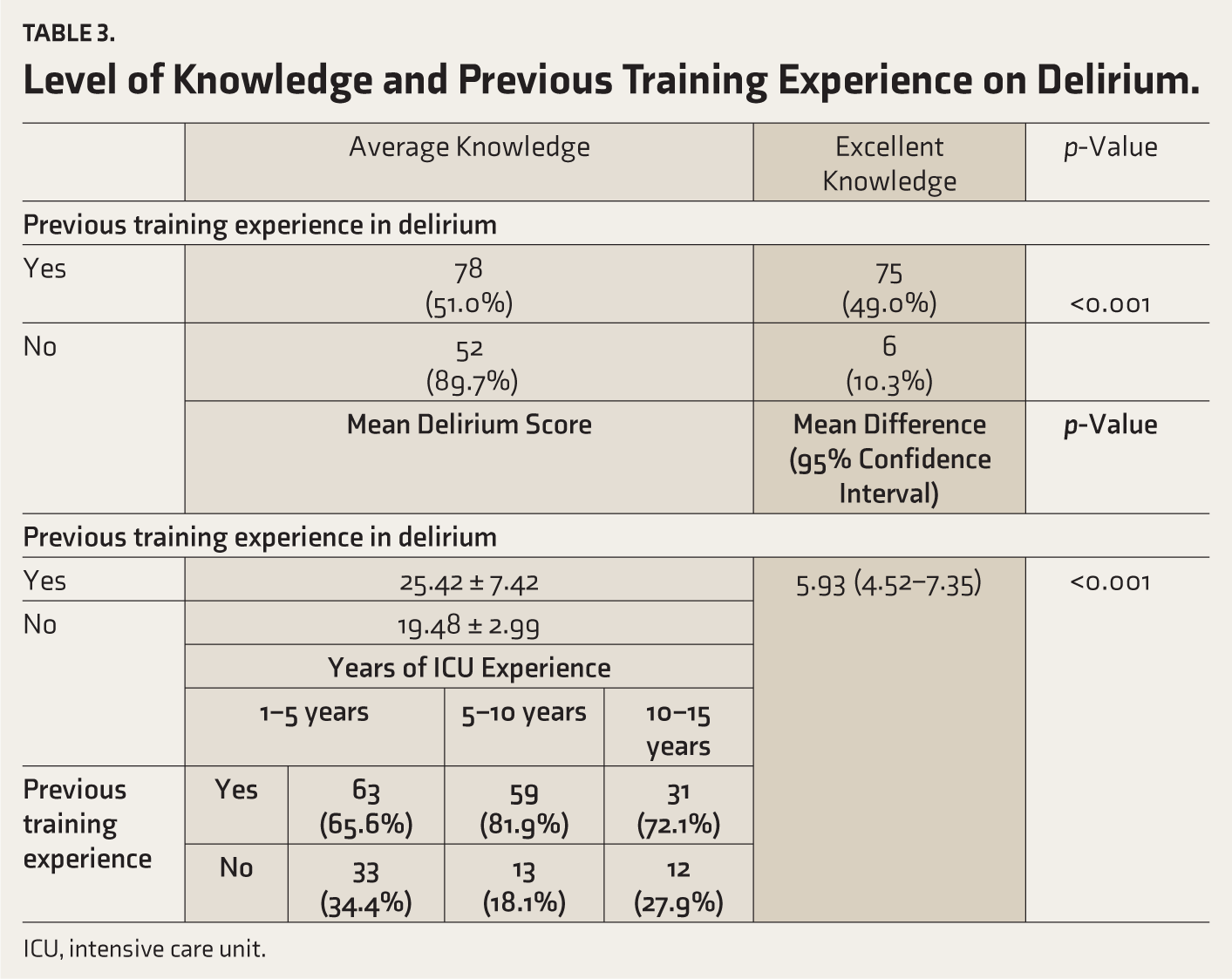
ICU, intensive care unit.
Knowledge of Delirium: Subdomain Wise.
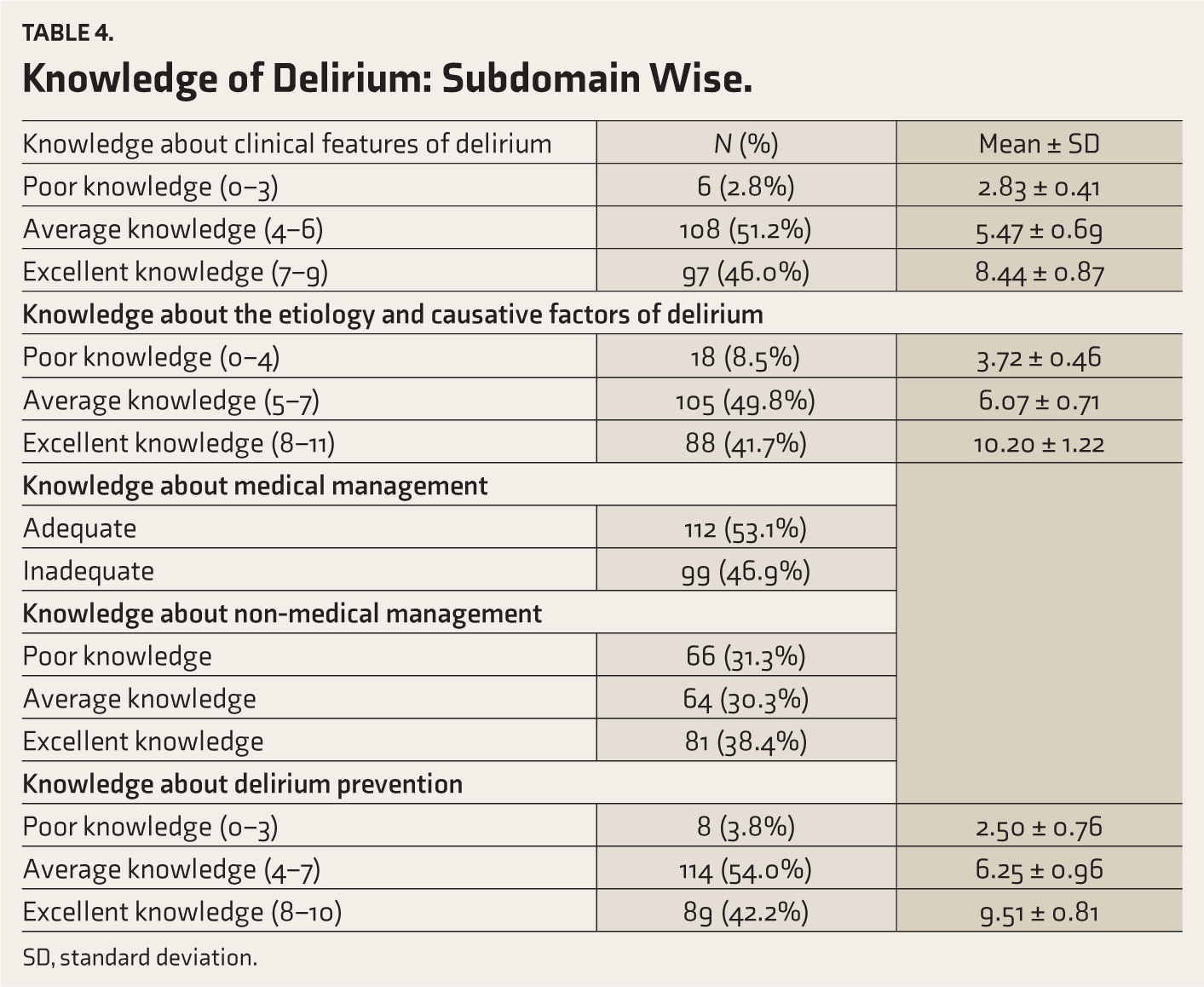
SD, standard deviation.
Level of Knowledge per Question.
In this study, nurses working in the surgical ICUs had better knowledge of delirium. This could be due to higher rates of postoperative delirium. Studies from India have shown that the incidence of perioperative delirium ranges between 17.5% and 21%.30,31
The findings of the present study may help in formulating a module to educate nurses about the clinical features, etiology, and management of delirium. As quoted from the study by Papaioannou et al. 5 the better the knowledge regarding delirium, the more positive attitude the nurse will have toward patients with delirium. When nurses are educated about a condition, they will be equipped to deal with it.
The present study has certain limitations. The study sample was chosen by convenience sampling and a cross- sectional study design. Since the data were collected from a single hospital, the results cannot be generalized. Since a questionnaire was used for the purpose of this study, respondent bias might have occurred. This questionnaire was circulated as a Google Form and hence sample bias would have occurred.
The findings of the present study reveal that nurses have only average knowledge regarding delirium. Different studies have proven that inadequate knowledge about delirium results in negative attitudes and poor clinical practices. Addressing this knowledge gap can be done through continuing education sessions on the management and prevention of delirium. Training sessions on the practical aspects of managing delirium are essential. There should be amendments to hospital policies related to managing delirium. Improving the nursing staff’s knowledge regarding delirium not only reduces the duration of hospital stay but also reduces the economic burden.
Footnotes
Consent for Publication
This work has not been published, simultaneously submitted, or already accepted for publication elsewhere.
This manuscript has been read and approved by all the authors, that the requirements for authorship as stated have been met, and that each author believes that the manuscript represents honest work. To the best of our knowledge, this manuscript does not infringe upon any copyright or property right of any third party. AI was not used in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
This study was approved by the Ethics Committee of Caritas Hospital (Approval No. CH/EC/APR2023/02).