
Abstract
Background:
Neurocognitive deficits have been reported consistently in euthymic bipolar disorder (BD) across studies. Endophenotype potential of such deficits have been reported in a few studies. However, data from the Indian subcontinent is sparse, and no studies had a sample (patients and high-risk group) aged 20-25 years, which is the actual risk period for developing BD. We studied cognitive deficits, as a potential endophenotype for BD, in recently diagnosed BD (FEM—first episode mania) in remission, young unaffected first-degree relatives (HR) of patients with BD, and healthy controls (HC).
Methods:
Cross-sectional study design using convenient sampling was employed. We recruited FEM (n = 25), HR (n = 25), and age-matched HC (n = 25) between 18 and 30 years. All HR subjects were <25 years of age, which is the period of vulnerability for BD. All the groups were screened using MINI Version 6. Neurocognitive assessments were done using the NIMHANS neuropsychology battery. The cognitive domains assessed were processing speed, attention, working memory, executive functions, and visual and verbal memory.
Results:
The three groups were comparable in age and sex (all P > 0.06). The mean (SD) age of the FEM subjects was 23.7 (3.47) years, and the mean duration of illness was 5.92 (2.94) months. Compared to the HC group, the FEM group performed poorly on multiple cognitive domains (all P < 0.05). Performance of the HR group was comparable to the FEM group, but they showed significantly poorer performance compared to HC on the verbal fluency test—controlled oral word association (COWA, F = 12.36, P = 0.001), and the visual learning and memory test—complex figure test-immediate recall (CFT-IR, F = 8.10 and p = 0.001).
Conclusions:
Cognition is impaired very early in the course of BD. Visual memory and executive function (verbal fluency) have endophenotypic potential. These findings are particularly important given that the HR group were still within the vulnerable period to develop BD. These findings imply a tremendous potential for early diagnosis and prevention by early interventions in BD.
Visual memory and verbal fluency have endophenotypic potential. These domains show deficits at a very young age (early 20s). Cognition in all the domains is affected in BD very early in the course of the illness (≤ 6 months).Key Messages:
Bipolar disorder (BD) affects >1% of the global population. 1 The National Mental Health Survey (2015-2016) showed an overall prevalence of 0.3%, which is around 4.5 million people in India. 2 BD is associated with cognitive impairment, even during euthymia. Specific domains of cognitive impairment include executive control, verbal learning and memory, working memory, and sustained attention. 3 Cognitive impairments are reportedly present early in the course of BD and are associated with functional impairment. The impact of this dysfunction is greatest in younger individuals, as BD disrupts the attainment of age-specific developmental, relationship, educational, and occupational milestones. 4 The most consistent cognitive findings in euthymic BD patients are deficits in verbal memory, executive function, and sustained attention. 5
Endophenotypes are intermediate phenotypes that are considered a more promising index of an underlying genetic liability than the illness itself, must be state-independent, and are demonstrable in remitted patients also. They should be more frequent in the unaffected relatives of patients than in the general population. 6 Studies from the west have reported that deficits in working memory, declarative memory, response inhibition, and processing speed might have some endophenotype potential.7–9 Only a few studies have investigated neurocognition as an endophenotype of BD, especially in the Indian context. A study by Kulkarni et al. suggested that deficits in verbal learning and memory and executive functions (planning) could be potential endophenotypes. 10 Pattnayak et al. also reported deficits in executive functions (set shifting) and memory. 11 Nehra et al. reported deficits only in verbal learning but not the executive functions. 12 A more recent study has shown that the unaffected siblings performed poorly in terms of memory functioning. 13 Considering the difference in the course of BD in the west (depression predominant) and India (mania predominant), 14 and since manic episodes have a more severe impact on cognition, we may say that our BD patients will have more severe cognitive deficits. 15 However, the cognitive domains that are affected do not differ between the western literature and ours, but the results vary across the studies. Another important observation is that all the studies done among the unaffected relatives have included people with a mean age of ≥30 years; the actual risk-group, people in their early twenties, have not been studied. As cognitive ability influences functioning and overall quality of life, and studies suggest deficits in BD patients and first-degree relatives (FDR), there is a need to further evaluate cognition as an endophenotype in at-risk subjects before they develop the illness. With the objective to investigate the endophenotype potential of neurocognition, we attempted to study the cognitive deficits in recently diagnosed BD patients (FEM) in remission (to decrease the confounding effects of neuroprogression and long-term medications) and the at-risk unaffected FDR of BD patients, in comparison with HC.
Methods
This cross-sectional study was conducted between 2018 and 2020 using convenient sampling. Remitted FEM patients (n = 25), FDR of patients with BD (HR; n = 25), and age- and education-matched healthy subjects (HC, n = 25) were recruited from the outpatient (OP) services of a tertiary care hospital. HR subjects (siblings and offspring) were recruited from among the attendants of patients in the OP and inpatient (IP) services and word of mouth. HC were recruited from the general population by word of mouth; these were the bystanders of patients in IP or OP and hospital staff or their family members, who were matched for age and sex. Sample size estimation was done using standard methods with a moderate effect size, alpha error = 0.05, and 80% power. The total sample size as per the estimation was 69 subjects i.e. 23 subjects (n=23) in each group. Considering a 10% attrition rate we rounded off the total sample size to 75 subjects i.e 25 subjects in each group.
Patients diagnosed with Bipolar Affective Disorder, currently FEM with/without psychotic symptoms or FEM with/without psychotic symptoms (ICD-10) and currently euthymic (Young’s Mania Rating Scale [YMRS] score < 7 and Hamilton Depression Rating Scale [HDRS] score <8) were recruited. Subjects of both sexes were included if they were 18-30 years of age; right-handed; had an education of at least 8–10 years; were able to read and write in Kannada, English or Hindi, with IQ> 70, using the Wechsler Abbreviated Scale of Intelligence (WASI); and were on stable medication for the past one month and currently off benzodiazepines. Patients with more than one episode of mania, any other axis I psychiatric disorder, including substance dependence except nicotine, were excluded. Those with mental retardation, other clinically recognizable neurological conditions such as epilepsy or dementia or history of head injury and those who had received electroconvulsive therapy within the past two months, which may confound neurocognitive performance, were excluded. HR subjects were defined as people who have a FDR diagnosed with BD (either sibling or parent) but no history of any axis I psychiatric disorder. The study has been approved by the Institutional Ethics Committee. Written informed consent was taken from each participant.
Assessments/Tools
All subjects were assessed with Mini International Neuropsychiatric Interview (Version 6), 16 YMRS, 17 HDRS, 18 and Edinburgh Handedness Inventory. 19 IQ assessment was done, and only participants with IQ> 70, using the WASI, were included. 20 The purpose of the IQ test was only to determine that the scores are not <70 (which is an exclusion criterion for administering neuropsychology battery). Additionally, WASI was used as a screening process. Neurocognitive assessments were done using the NIMHANS neuropsychology battery21,22 on the domains of processing speed, attention, working memory, executive functions, and visual and verbal memory, in keeping with the domains recommended by the International Society for Bipolar Disorders—Battery for Assessment of Neurocognition (ISBD-BANC). 23
Raw scores obtained for the performance on the neurocognitive tests (observed values) were taken for analysis. With respect to the Stroop test, Digit Symbol Substitution Test (DSST), and Color Trials, the time taken to complete the tasks was taken as observed value. The higher the time taken, the higher the deficits. The number of words registered and recollected was taken as observed data for Auditory Verbal Learning Test (AVLT). The lesser the number of words recollected, the higher the deficits. The number of words produced was taken as the observed score for Controlled Oral Word Association (COWA). Here, again, the lesser the number of words, the higher the deficits. The zoo test score was calculated based on the path taken and errors. The same was taken as the observed value; the more the errors, the higher the deficits. The observed value for Complex Figure Test (CFT) was calculated based on correct responses; the lesser the number of correct responses, the higher the deficits.
Neurocognitive Test Procedures
Processing Speed (DSST)
DSST is a test of visuomotor coordination, motor persistence, sustained attention, and response speed. Rapid information processing is required in order to substitute the symbols accurately and quickly. The test consists of a sheet in which numbers 1–9 are randomly arranged in four rows of 25 squares each. The subject substitutes each number with a symbol using a number-symbol key given at the top of the page. Ten squares are for practice.
Attention (Color Trails Test)
Focused attention was checked for through the Color Trails test. It is an analogue of the Trail Making Test and is considered to be free from the influence of language. It has two parts: Part 1 requires sustained attention, perceptual tracking, and simple sequencing, while Part 2 requires mental flexibility in addition to the above. The test is considered a measure of focused attention because, in both parts of the test, the subject has to ignore irrelevant numbers while scanning for the number that is next in sequence. This test cannot be given to illiterate subjects who cannot recognize numbers.
Visuospatial Working Memory (Spatial Span)
The Spatial Span Test consists of a board on which ten cubes of the same size are fixed. One side of the cube shows the numbering of the blocks in a predetermined fashion. These numbers would not be visible to the subject. In the spatial span-forward condition, the examiner touches a few blocks, and the subject has to touch the same blocks in the same order once the examiner is done. In spatial span backwards, the subject has to touch the same blocks in the reverse order once the examiner is done. Both forward and backward conditions have eight items, and every item has two trials.
The details of the tests for executive functions are presented next.
Verbal Fluency (COWA)
The subject has to generate as many words as possible from a given consonant, within a minute. The words should not be proper nouns or extensions of words said earlier. A total of three consonants are used. This test has been validated to assess verbal fluency in schizophrenia. We used the original consonants (F, A, and S) for those who were fluent in English; for those who were not fluent in English, we used consonants ka, pa, and ma as an Indian adaptation.
Planning (Zoo Map Test)
This test assesses the ability to independently formulate and implement a plan (high-demand condition) and follow a pre-formulated plan (low- demand condition). It involves plotting or following a route through a map without contravening a set of rules. The score is based on the successful implementation of the plan, with penalties imposed for rule breaks. The test consists of two parts. In the first part, patients are required to plan their route through the zoo map, visiting a section of locations while actively disregarding others. While planning the route, they also have to obey certain rules. The second part consists of the same map with the same locations that must be visited, but this time instructions are provided about the precise order in which the locations must be visited. Therefore, in contrast to the first part, the second part consists of a highly structured setting that strongly reduces the involvement of planning.
Response Inhibition (Stroop Test)
Stroop test measures the ease with which a perceptual set can be shifted based on the changing demands, by suppressing a habitual response in favor of an unusual one. The prefrontal areas are essential for response inhibition abilities. The subject is asked to read the stimuli column-wise as fast as possible. The time taken to read all 11 columns is noted down. Next, the subject is asked to name the color in which the word was printed. This time also, the subject proceeds column-wise. The time taken to name all the colors is noted down. The words were presented in the mother tongue of the subject. The time taken to complete the second task is subtracted from that taken for the first reading, and the time difference thus obtained forms the score.
Verbal Learning and Memory (AVLT)
AVLT consists of words designating familiar objects such as vehicles, tools, animals, and body parts. There are two lists, A and B, with different words in each list. The words were translated into four Indian languages: Kannada, Tamil, Telugu, and Hindi. Words in List A are presented at a rate of one word per second, during five successive trials. Immediate and delayed recall are assessed. We also assessed the ability to recognize the words in List A, which is scored based on the number of hits the subject does when a random list of words are presented to them interspersed with the words in List A.
Visual Learning and Memory (CFT)
Rey developed the CFT in 1941. It consists of a complex design that is abstract and cannot be named easily. It has an overall structure and multiple subcomponents within it. The complex figure has to be first copied by the subject and then recalled to draw it from memory. The patient is asked to recall the figure twice: the first time is an immediate recall three minutes after the copying is completed; the third is a delayed recall taken after 30 minutes.
Statistical Analysis
Observed values obtained in the neurocognitive tests were used for comparison between the groups. Normality distribution was analyzed using the Shapiro Wilk Test. The equality of variance was checked using Levene’s test. Based on the results of these, parametric tests were used for analysis. ANCOVA (analysis of co-variance) was used to compare the means, and Tukey post-hoc test was used to assess differences between the groups. The effect sizes were estimated using partial eta squared (η2). The effect sizes were defined as small (η2 = 0.01), medium (η2 = 0.06), and large (η2 = 0.14) effects. 24 For categorical variables, chi-square test was performed.
Results
Sample Description
All the 75 participants, 25 in each group, completed the clinical and neuropsychological assessments. The mean (SD) age of the sample was 23.9 (3.56) years; 67% were male and 33%, females. The age (P = 0.70) and sex (P = 0.65) distributions were not statistically significantly different across the groups. The number of years of formal education was significantly different among the groups, with the HC group having higher education compared to HR and FEM groups. Significantly more subjects in the HC group were employed compared to HR and FEM groups.
Clinical Characteristics of the FEM Group
The mean age was 23.72 (3.47) years. Most had an onset of BD in their early adulthood, with the mean age of onset being 23.68(3.47) years. Only two patients had a history of depression before FEM. The mean duration of the manic episode was 3.44 (2.04) months. The mean duration of illness was 5.92 (2.94) months. The mean duration of remission from illness at the time of recruitment was 4.80 (1.41) months. The mean YMRS and HDRS scores were 0.24(0.73) and 0.72(0.77), respectively. Of the 25 patients, only one was on a mood stabilizer, and 24 were prescribed atypical antipsychotics.
Neurocognitive Test Performance
The mean IQ scores of the FEM group was 78.68 ±7.74, HR group was 81.68 ±11.05, and HC group was 89.00 ±8.09. These were not statistically significantly different (F = 1.4, P = 0.15). The neurocognitive functioning was compared between the groups, keeping the years of education as a covariate.
FEM Group
On DSST, CT, COWA, and Stroop tests, the group performed worse when compared to HC. In the AVLT recognition trial (the number of hits) the FEM group performed worse than the HC group. Regarding the number of misses, the FEM group missed a significantly higher number of words compared to both HC and HR groups. In CFT, copying and delayed recall scores were lower in the FEM group than in HC.
HR Group
They had scores similar to the FEM group, while both these groups performed worse compared to HC in the COWA test and immediate recall scores of CFT. The HR group did not separate significantly from the HC group on performance of other tasks (Table 1).
Sociodemographic Details.
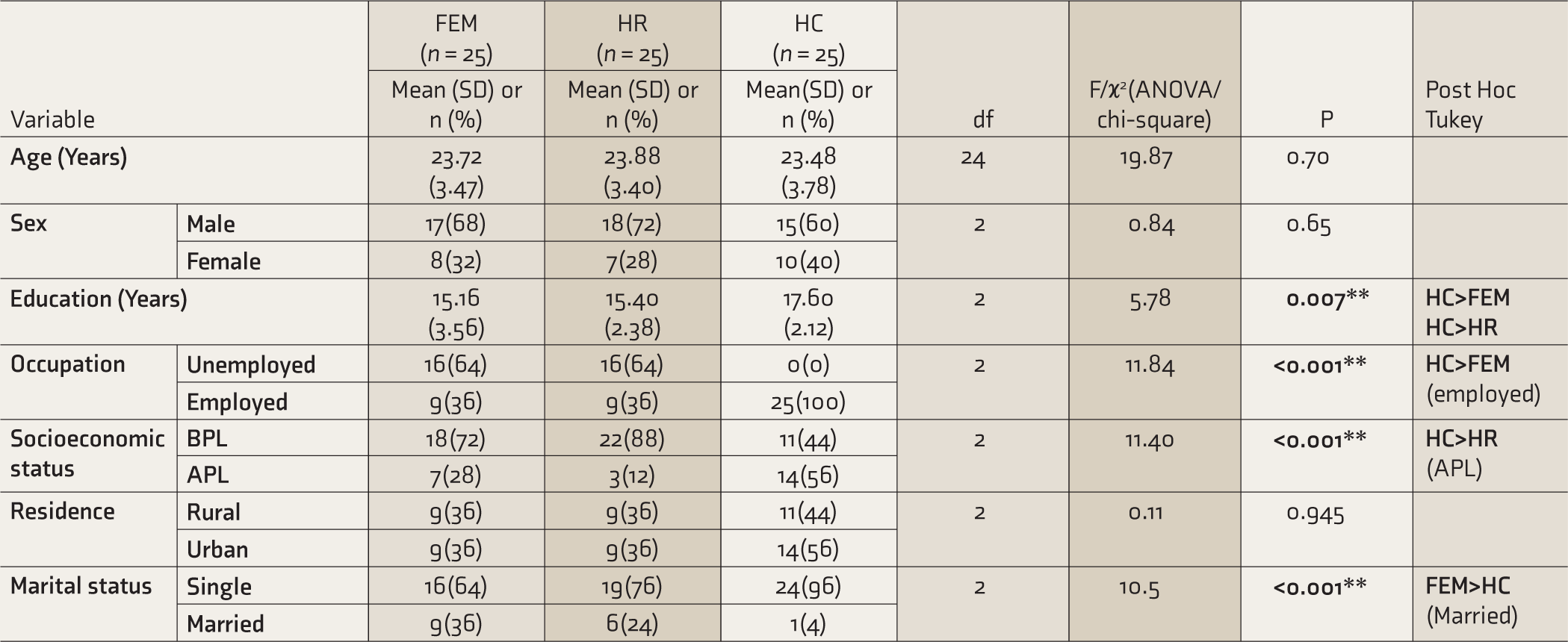
FEM, first episode mania; HR, first degree relatives (high risk); HC, healthy controls; SD, standard deviation; ANOVA, analysis of variance; BPL, below poverty line; APL, above poverty line. P < 0.05 is statistically significant.
Comparison of Neurocognitive Functioning Between Groups with Years of Education as Co-variate (ANCOVA).
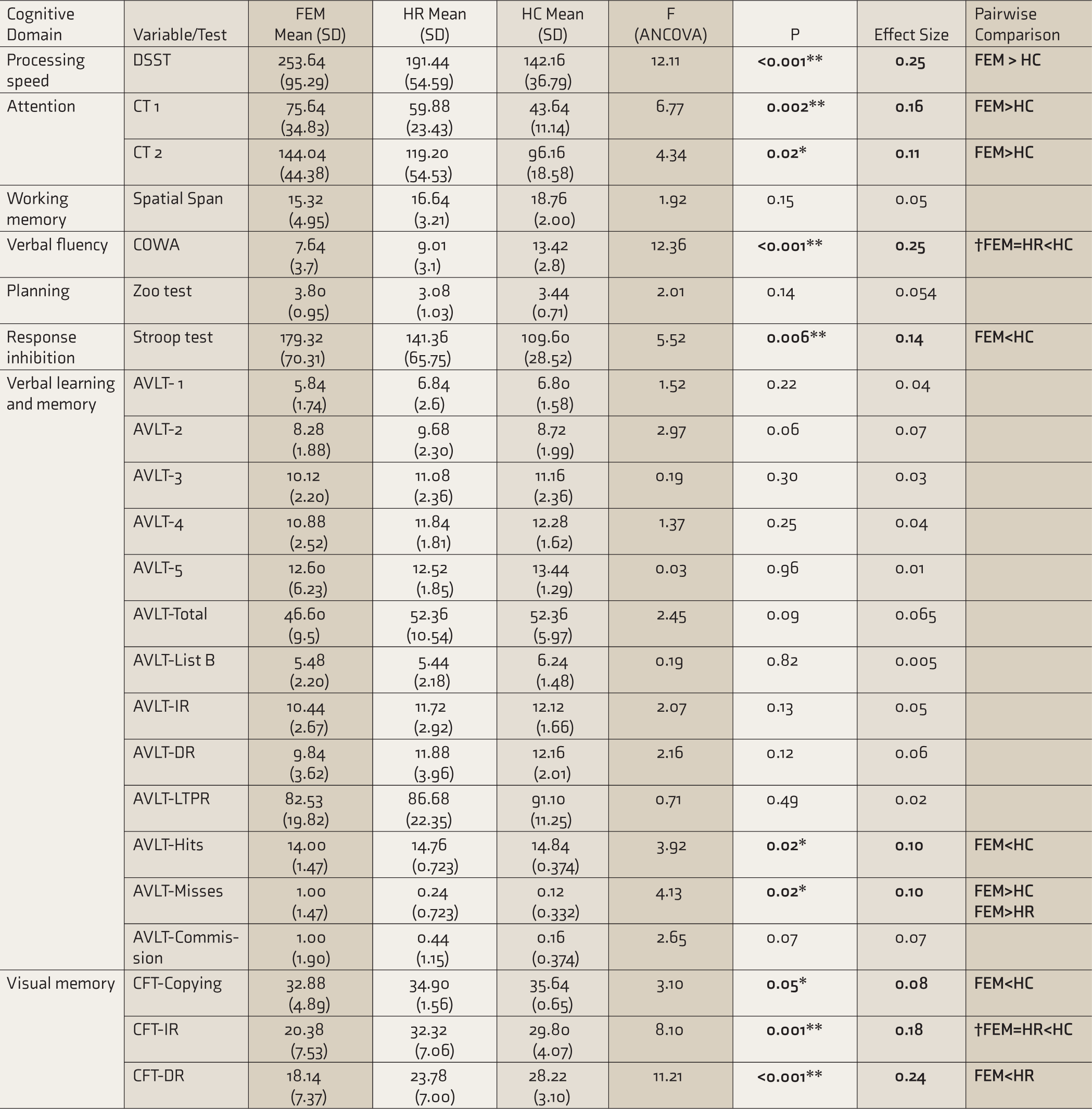
FEM, first episode mania; HR, first degree relatives (high risk); HC, healthy controls; SD, standard deviation; ANCOVA, analysis of covariance; DSST, digit symbol substitution test; CT, color trails; COWA, controlled oral word association; AVLT, auditory verbal learning test; CFT, complex figure test; IR, immediate recall; DR, delayed recall; LTPR, long term percent retention. P < 0.05 is statistically significant, †Cognitive domains with endophenotypic potential.
Discussion
The identification of objective endoph- enotypes such as measures of pathophysiological processes can inform us about the aetiology of BD and further provide targets for the development of new and personalized treatments that reduce cognitive dysfunction by early interventions, thereby preventing progressive illness-related functional impairments. In this context, our main findings are as follows.
Deficits were noted in processing speed, attention, verbal fluency, response inhibition, verbal learning and memory, and visual memory. Another study that looked at cognitive deficits after FEM has reported similar results. 25 A meta-analysis reporting the cognitive deficits early in the course of BD documented that the most consistent finding was a deficit only in the working memory domain, unlike what we found. 26 Another recent Indian study that compared the cognitive deficits in FEM and multi-episode BD showed no difference between the groups; both had significant deficits in executive functions compared to HC. 27 It is interesting to note that the FEM group had deficits in multiple domains vis-à-vis healthy subjects despite the total duration of mania being <4 weeks and the total duration of illness <5 months, of which four months were in remission, and the age of the subjects being <24 years, highlighting that the pathophysiological processes that underlie BD are operational probably even before the onset of illness or become manifest very early in the course. Hence, the search for neurocognitive endophenotypes assumes significance.
Our HR group had a mean age of 24 years. All other studies that compared the cognitive deficits in HR and BD had subjects in the age range of 34-40 years,13,28–30 by which age, the risk for BD probably becomes much lesser. Our HR group had deficits similar to FEM and significantly separated from the HC group in the domains of verbal fluency (executive function) and visual memory. Other endophenotype studies had shown deficits in executive functions and verbal memory.13,28,29 A meta-analysis evaluating cognitive endophenotypes identified response inhibition (executive function) as a potential endophenotype. 6 A study in multiplex multigenerational families identified measures of processing speed, working memory, and declarative (facial) memory as candidate endophenotypes for BD. 30 An Indian study that compared unaffected siblings with controls reported deficits in the memory domain. 13 Studies that looked at specific cognitive domains had shown that in BD, language structure had alterations in semantic contents, impaired verbal associations, and discrepant prosody or speed of verbal production. 31 This finding has been considered as evidence of impaired semantic activation/inhibition, insufficient spreading across the semantic network, or possibly an impairment affecting the control of these functions (executive control). 32 Studies on visual memory in BD have shown that executive dysfunction may mediate the visual memory deficits in early-onset BD. These results also indicate that the cognitive domains are interrelated and that deficits in one domain can lead to deficits in others. 33 Although different cognitive domains have been identified as endophenotypes, executive function and memory domains have been the most replicated, which is reflected in our results too.
Evidence from functional MRI (fMRI) studies suggests that aberrant intrinsic network activity is associated with the cognitive impairment in BD. The main networks identified are the default mode network (DMN), central executive network (CEN), and salience network (SN). Studies have shown that there is a failure to recruit key regions in the CEN to suppress task-irrelevant DMN activity during the cognitive performance, and also disrupted SN recruitment in the frontoparietal region. 34 Interpreting the results from an etiological perspective, the above findings, taken together, appear to suggest that brain dysfunction and, thus, cognitive deficits in several domains, may exist even before the onset of the first episode in patients with BD, supporting the neurodevelopmental hypothesis. Compelling evidence of cognitive dysfunction in the unaffected and apparently healthy relatives of patients with BD also strongly supports this hypothesis.
Our patient group was on stable medications. Previous studies have shown that lithium has a small negative effect on psychomotor speed and verbal memory, but there is improvement and stabilization in other cognitive domains, especially in bipolar depression and late-life mood disorders. Among the anticonvulsants, lamotrigine has a better cognitive profile than carbamazepine, valproate, topiramate, and zonisamide. A slight negative impact of atypical antipsychotics on cognitive functioning in BD is also reported. 35 The above evidence does suggest that the medication can have a mild effect on the cognitive functions. Since all our patients were on medications, this could be one of the confounding factors. However, it is important to note that the HR group, who were not on any medications, also showed a significant difference compared to the HC and that the deficits were similar to those in the FEM group.
The strength of our study is that the mean age of the HR group was <24 years, which could imply that these subjects are still in a period of risk for BD. In contrast, other endophenotype studies had subjects in a higher age range; hence, their findings may not accurately reflect the risk of developing BD or may rather reflect resilience to the disorder. We included patients early in the course of the illness (FEM) and in remission, thereby avoiding confounding factors such as the effects, on cognition, of the duration of the illness, age, active symptomatology, prolonged exposure to psychotropic drugs, and multiple affective episodes. A single investigator administered all the tests and scales, avoiding inter-rater bias. All the necessary measures such as: same person performing the assessments for all the subjects, keeping the timing similar, using the same assessment room, and avoiding stimulants such as coffee/tea/nicotine before the assessments were taken to avoid possible confounding effects while administering cognitive tests.
Limitations include the study’s cross- sectional nature, potential confounding effects of the psychotropic medications on the cognitive performances in the BD group, and the sample being hospital-based, which might include patients who are more severely ill. A comprehensive IQ testing could not be conducted. Further, if premorbid IQ could be utilized to screen patients (instead of current IQ), it would be a better indicator to tell us if it is a low baseline IQ or a general decline in neurocognition due to the illness that is currently giving us the lower IQ scores (this would eliminate the confounding effect of the onset of illness). Although neurocognitive deficits were apparent in high-risk subjects, they were more prominent in certain domains in early BD. Studies comparing multi-episode BD groups or with longitudinal evaluation may provide evidence of neuroprogression over the course of the illness.
In conclusion, our study shows that all the cognitive domains evaluated (processing speed, attention, visuospatial working memory, verbal memory, visual memory, verbal fluency, and planning) are impaired in BD very early in the course of illness: as early as within six months of onset. This emphasizes the impact of BD on cognitive functions and, in turn, the individual’s overall functioning. Visual memory and verbal fluency (executive function) are potential endophenotypes, thereby emphasizing the need for early cognitive screening and the institution of early interventions. These could be in the form of individualized cognitive remediation and some aspects of interpersonal social rhythm therapy. Along with these, regular follow-ups with the mental health team will help prevent relapses and thus improve the functionality of these individuals. Studies need to evaluate the effectiveness of cognitive remediation in this population. An integrated approach might be beneficial, which in turn could impact the course and outcome of the illness.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.