
Abstract
Background:
Cognitive impairment is usually associated with impairment in everyday activities. Scales to assess activities of daily living, like the Everyday Abilities Scale for India (EASI), have been employed as screening tools for dementia or major neurocognitive disorder. EASI had not been validated in Malayalam. This study’s objective was to validate the Malayalam version of EASI (M-EASI) in those aged ≥60 years.
Methods:
In a study undertaken in a tertiary care center, those aged ≥60 years attending psychiatry, neurology, or geriatric clinic of general medicine departments were evaluated using M-EASI and the Malayalam version of Addenbrooke’s Cognitive Examination (M-ACE). A total of 304 participants were recruited for this questionnaire validation. Information for M-EASI was obtained from a reliable informant.
Results:
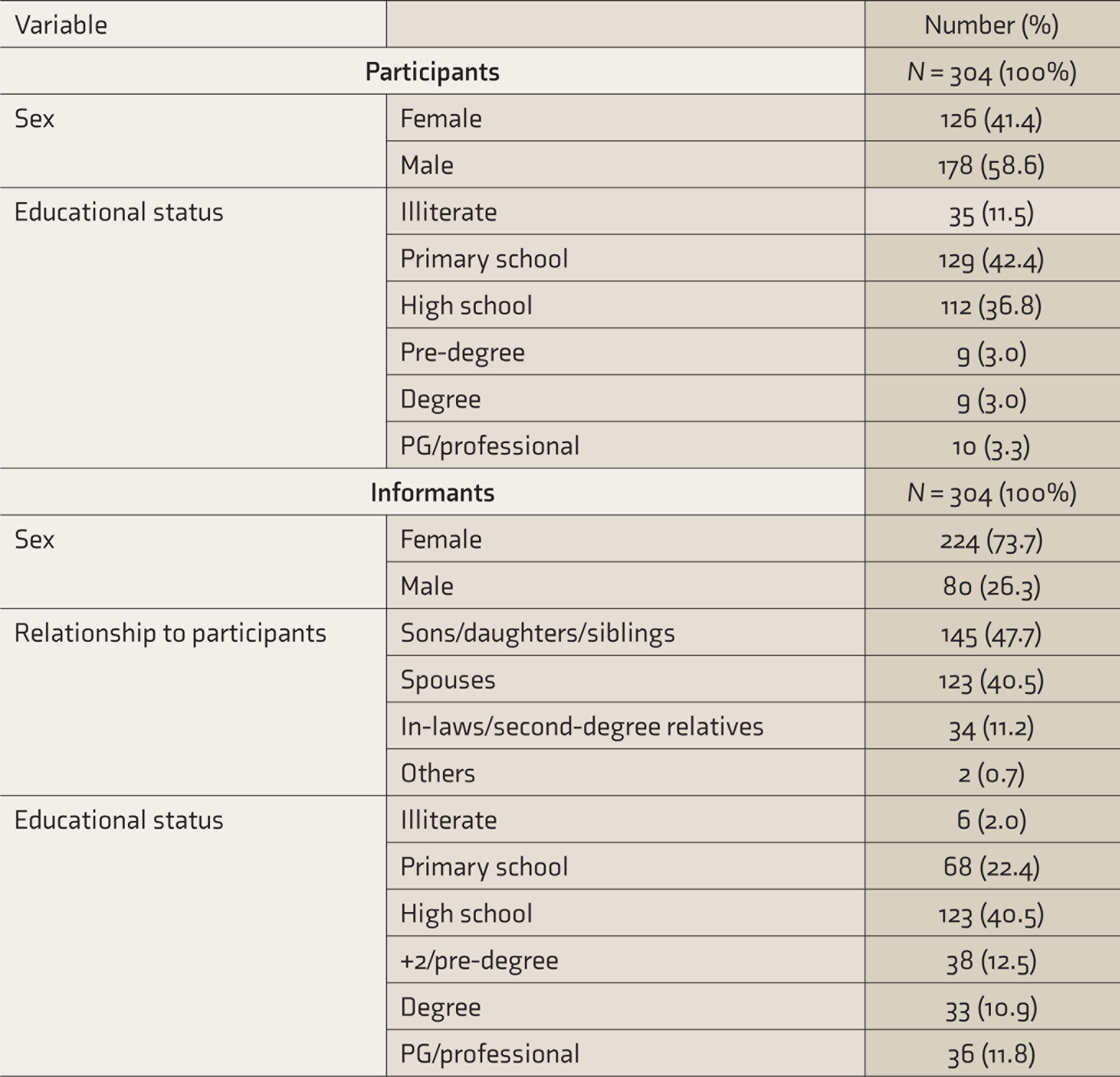
The mean age of the sample was 70.04 years (standard deviation—7.33). The majority of them were males (58.6%) and educated up to primary school (42.4%), while the majority of the informants were sons/daughters/siblings (47.7%) and were females (73.7%). Taking M-ACE scores as the gold standard for diagnosing MNCD according to Diagnostic and Statistical Manual of Mental Disorders—Fifth Edition criteria, there were 162 cases of MNCD and 142 normal controls. Cronbach’s α was 0.91. At an optimal cut-off of 4.5, adequate sensitivity (77.8%), and specificity (75.4%) were observed. The positive predictive value was 78.6%, and the negative predictive value, 74.5%.
Conclusion:
M-EASI has adequate psychometric properties as a screening tool for MNCD.
The M-EASI has adequate psychometric properties. It can be used as a screening tool for dementia in clinical settings.Key Messages:
According to the Population Census 2011, those aged ≥60 years constituted 8.6% of India’s total population. Among the states of India, this proportion is the highest in Kerala (12.6%). 1 The Dementia in India 2020 report found that 5.3 million people above the age of 60 have dementia. In India, the diagnosis of dementia was observed to be infrequent in primary care settings, the diagnosis being made mostly by specialists like psychiatrists and neurologists. 2 The World Alzheimer Report 2015 found that more than 50% of dementia cases do not receive the diagnosis of dementia due to insufficient availability of specialists, even in high-income countries. It was proposed that identifying clinical practices to promote timely and accurate diagnosis of dementia in the primary care setting was important. 3 The 10/66 Dementia Research Group demonstrated that after training in recognition of dementia, using an informant-based approach, community health workers could identify dementia cases in the community with a positive predictive value of 64.7%. 4
Cognitive impairment due to dementia can lead to impairment in activities of daily living (ADL). ADL includes activities performed on a daily basis and are of two types: those involving the core tasks of daily life (such as eating, bathing, and dressing), termed basic ADL, and those involving higher-level tasks using instruments (such as cooking, shopping, and managing finances), termed instrumental ADL (IADL). 5 In mild cognitive impairment and early dementia, IADL is impaired, while impairment in basic ADL occurs in later stages of dementia. As cognitive functions worsen, there can be a hierarchy in the functional decline of ADL. Various studies have found impairment in basic ADL to be associated with a decline in memory, attention, executive functioning, and praxis. Informant-based ratings of ADL are used frequently in dementia-related research, although it is not free of bias. 6 Strategies to screen for dementia have included ADL assessment, which is not influenced by education or culture. 7 Studies have used impairment in ADL as a surrogate measure of cognitive disability. 8 Simple screening tools to assess ADL can be easily administered by community health workers with adequate training, to identify dementia. The Everyday Abilities Scale for India (EASI)—a measure of ADL—has been validated in Hindi for the North Indian population as a screening tool for dementia. 9 The objective of this study was to validate the Malayalam version of EASI (M-EASI) as a screening tool for dementia in those aged ≥60 years.
Materials and Methods
The validation of M-EASI was undertaken as a cross-sectional study in Government Medical College, Thiruvananthapuram, a tertiary care teaching hospital in South India, over a period of four years from 2015. This was done as part of a case-control study, for which approval of the Institutional Ethics Committee was obtained. The study population included older adults aged ≥60 years attending the departments of psychiatry (psychogeriatric clinic), neurology, or geriatric clinic of general medicine. The new terminology for dementia as per the Diagnostic and Statistical Manual of Mental Disorders—Fifth Edition (DSM-5) is major neurocognitive disorder (MNCD). The study sample constituted cases of MNCD—diagnosed as per the DSM-5 criteria, 10 having scores below the education-specified norms of the Malayalam adaptation of Addenbrooke’s Cognitive Examination (M-ACE)11,12 and subjects without MNCD having scores above the education-specified norms of M-ACE.11,12 Those who satisfied the diagnostic criteria for schizophrenia, bipolar disorders, or other psychotic disorders; those who were in delirium or uncooperative to participate in the interview; those who did not have a reliable informant; and those who/whose relatives refused to give consent were excluded. As per the rule of thumb of 10 cases per item, 120 cases were required for the study. Of the participants recruited for the case-control study, 304 were selected for this questionnaire validation. Informed consent was obtained from the participants and a reliable informant before recruiting them for the study.
Tools Used
The M-ACE is a global cognitive screening battery adapted to Malayalam. It can be administered in 15–20 minutes. The maximum score is 100; at a cut-off score of 83, it had a sensitivity of 82% and specificity of 96%. The internal consistency reliability was good (Cronbach’s α—0.78). Education-stratified norms have been developed for this questionnaire for the local population.11,12 This was taken as the gold standard in diagnosing MNCD.
EASI is an 11-item scale (with an additional item on mobility) used to measure ADL. Scoring is done in yes/no format and coded 0/1, a higher score indicating greater disability. It had been validated in Hindi for the North Indian population, with a Cronbach’s α of 0.82 and test–retest reliability of 0.92. 9
Permission was obtained from the authors for using these questionnaires for the study. EASI was translated to the local language and back-translated by two experts each in the subject as well as the language, and the final version decided. This final version was pilot tested in about 10% of the study sample. Sociodemographic data of the participants and informants were collected using a pro forma designed for the same. M-ACE was administered to the participants, and M-EASI, to the informants—as this questionnaire was meant for evaluation of older adults with probable cognitive impairment. Fillenbaum et al. had relied on the informant’s version to validate the Hindi version of this questionnaire. 9 M-EASI was re-administered to 26 (8.6%) informants over the telephone within a span of 2–4 weeks of the first interview.
The data was entered in MS Excel version 2019 and prepared for analysis which was done using SPSS version 21 for Windows. 13 Descriptive statistics of the study sample is provided. Mean and standard deviation (SD) are provided for continuous variables and proportions for discrete variables. Average inter-item and item-total correlations were estimated. The intra-class correlation was assessed for test–retest reliability and Cronbach’s α for internal consistency reliability. For evaluation of criterion validity, M-ACE was taken as the gold standard. The receiver operating characteristic (ROC) curve provides a means of determining the criterion validity of a screening tool as measured against a gold-standard outcome.14,15 Hence, an ROC curve was drawn and the optimal cut-off score determined. Sensitivity, specificity, positive predictive value, and negative predictive value were determined for the cut-off score. Correlation of sociodemographic variables and M-ACE scores with the score of M-EASI was also estimated using Spearman’s rank correlation coefficient.
Results
There were 304 participants. Based on the M-ACE scores, there were 162 cases of MNCD and 142 cognitively normal controls. The mean age of the study sample was 70.04 years (SD—7.33) and that of the informants was 49.60 years (SD—12.85). The mean score of M-EASI was 5.21 (SD—4.09) and that of M-ACE was 44.04 (SD—21.06). The majority of the participants were males (58.6%) and informants were females (73.7%). Most of the informants were first-degree relatives (sons/daughters/siblings, 47.7%), followed by spouses (40.5%). The mean duration for which the informants had stayed with the participants was 25.61 years (SD—18.48). The majority of the participants had studied up to primary school (42.4%) and belonged to Below Poverty Line (BPL) socioeconomic status (59.5%). Most of the informants had studied up to high school (40.5%). See Table 1 for details.
Descriptive Statistics of the Participants and Informants
Psychometric Properties of the Scale
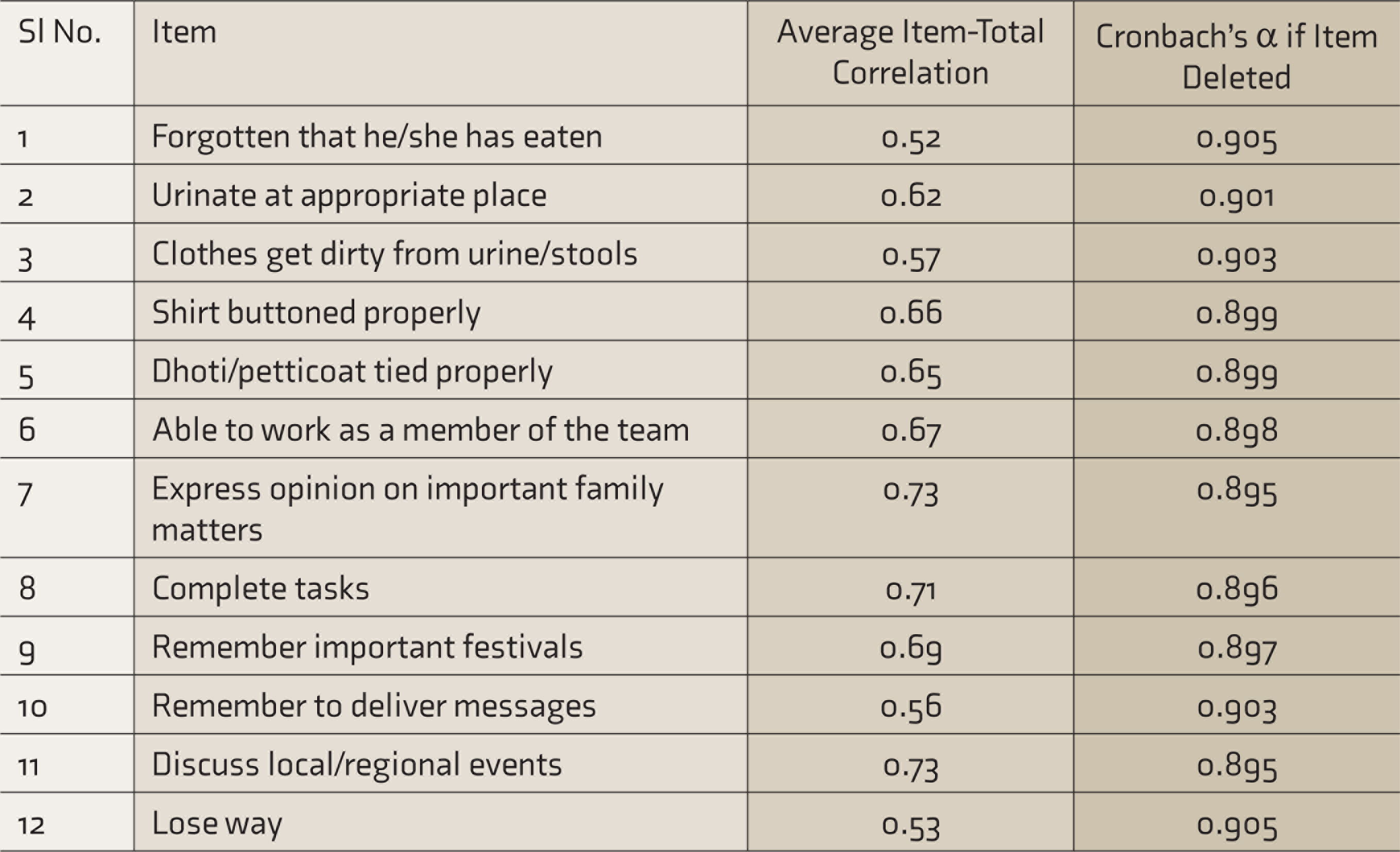
The average inter-item correlation was 0.45 and the average item-total correlation was 0.64. See Table 2 for the average item-total correlation of each item of the questionnaire. The internal consistency reliability was good (Cronbach’s α—0.91). Using absolute agreement, two-way, mixed-effects model, the average measures test–retest reliability was 0.95.
Average Item-Total Correlation of the Items of M-EASI
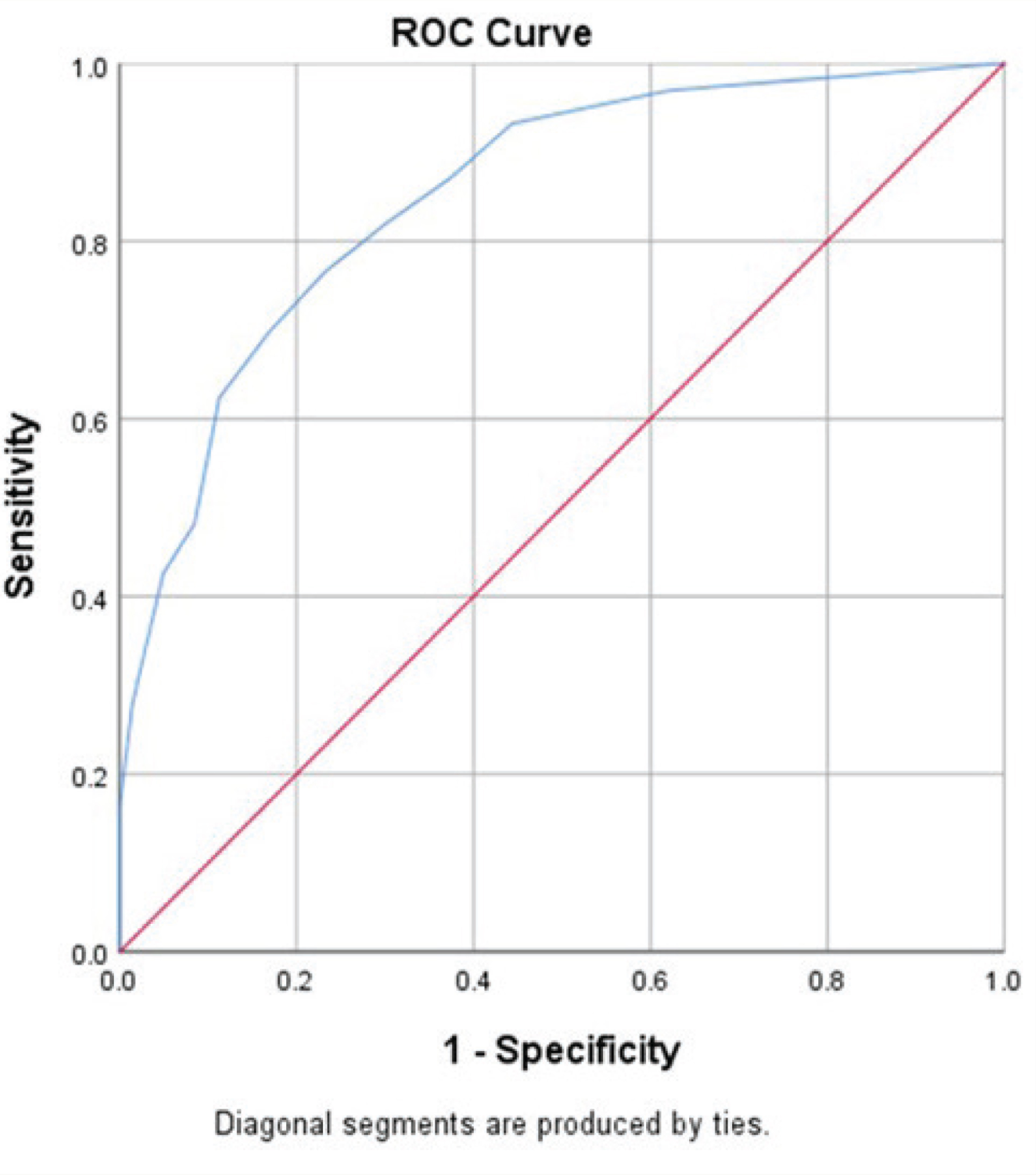
Face and content validity were already established for this questionnaire. ROC curve was drawn, taking M-ACE as the gold standard. The area under the curve was found to be 0.85 (95% CI = 0.81–0.90) (see Figure 1). At an optimal cut-off score of 4.5, there was a sensitivity of 77.8% and specificity of 75.4%. The positive predictive value was 78.6%, and the negative predictive value was 74.5%.
Receiver Operator Characteristic Curve for Malayalam—Everyday Abilities Scale for India with Malayalam Addenbrooke’s Cognitive Examination as the Gold Standard
Correlation of the sociodemographic variables with the M-EASI score was assessed. The educational status of the participants (ρ = −0.15, P = 0.008) was found to have a significant negative correlation with the M-EASI score. Using Mann–Whitney U test, the M-EASI score was found to be significantly higher in the BPL group (median score = 6, inter-quartile range [IQR] = 1–9.75) compared to the Above Poverty Level (APL) group (Median score = 4, IQR = 1–8) (P = 0.03). This suggested that at a higher educational status and socioeconomic status, functional disability was less. There was a significant negative correlation between the scores of M-EASI and M-ACE (ρ = −0.661, P < 0.001). That is, functional impairment worsened with an increase in cognitive impairment. M-ACE score showed a significant positive correlation with the educational status of the participants (ρ = 0.462, P < 0.001). The median score of M-ACE was significantly lower for BPL group (median score = 39.00, IQR = 26.00–54.5) compared to APL group (median score = 49.00, IQR = 33.00–69.00) (P < 0.001). This suggested greater cognitive impairment with poorer educational and socioeconomic status.
Discussion
The Malayalam version of EASI was found to have adequate psychometric properties. At an optimal cut-off score of 4.5, adequate sensitivity and specificity were observed. Fillenbaum et al. had validated this scale with 11 items, excluding item 12, for use as a screening tool for dementia in illiterate, rural older adults in North India. 9 In the Indo-US Epidemiology Study, at a cut-off score of 3, EASI was found to have a sensitivity of 62.5% and specificity of 89.7%. 16 The 12-item M-EASI has been validated now for a highly literate population of South India. As per the Census 2011, Kerala has an effective literacy rate of 94%, the highest in India. 17 In this study, the educational status of the participants was found to have a significant negative correlation with M-EASI scores, which suggested better functioning for higher educational status, but the strength of correlation was weak. Higher educational status of the participants also correlated with better cognitive functioning. Tripathi et al. had observed that education was the strongest determinant of performance on neuropsychological testing in normal older adults. 18 The higher educational status of the study sample could be the reason for the higher cut-off observed in our study.
The diagnostic criteria for MNCD in DSM-5 include impairment in everyday activities. 10 Cognitive impairment is associated with impairment in ADL, which has led to functional impairment being used as a surrogate measure of dementia. A study done in Himachal Pradesh had observed a significant negative correlation between scores in EASI and the Hindi Mental State Examination (HMSE) and suggested that EASI may be used as an alternative to HMSE and as a screening tool in identifying cases of dementia. 19 It was also reported that EASI had the added advantage that it could be administered to informants of cognitively untestable subjects. In two-phase surveys to estimate the prevalence of dementia in the community, EASI can be used as the first-phase screening tool, to be followed up with a detailed cognitive assessment. 19 The 10/66 dementia research network had demonstrated that informant-based screening methods could be used as a simple, cost-effective case-finding method for providing community-based dementia care services and research. They had also demonstrated that community health workers, with adequate training and using such informant-based screening tools, could identify a significant number of dementia cases in the community. 4
In our study, M-EASI was validated in a tertiary care setting for use by trained clinicians. As highlighted in the World Alzheimer Report 2015, many dementia cases remain undiagnosed due to a lack of specialist services. 3 It becomes imperative that these cases are identified earlier for proper management and supportive care. As the M-EASI has been validated in a clinical setting, clinicians can use it in primary care settings to screen for dementia cases.
There are some limitations to this study. The inter-rater reliability of the questionnaire has not been assessed. As the study was undertaken in a tertiary care setting, the generalizability, especially of positive predictive value, is limited. At the cut-off score of 4.5, adequate positive and negative predictive values were observed in this sample with a high prevalence of dementia (53.3%). Prevalence being the most determining factor for predictive values, when the questionnaire is administered to the general population with a low prevalence of dementia, the positive predictive value can be reduced. 14 However, in this study, the tool was found to have adequate psychometric properties for use by clinicians in clinical settings. There is scope for this questionnaire to be used by community health workers as a screening tool in the community. Further studies can be undertaken to validate this tool for use in the community by such healthcare workers.
Conclusions
The M-EASI has adequate psychometric properties as a screening tool for dementia, with a Cronbach’s α of 0.91 and test–retest reliability of 0.95. At an optimal cut-off score of 4.5, it showed adequate sensitivity (77.8%) and specificity (75.4%); the positive predictive value was 78.6%, and the negative predictive value was 74.5%. This tool can help clinicians in busy primary care settings to identify dementia cases for further evaluation and management.
Footnotes
Acknowledgements
We express our gratitude to Dr Thomas Mathew, Principal, Government Medical College, Thiruvananthapuram, and the Professors and Heads of the departments of psychiatry, neurology, and general medicine of the institution for permitting us to conduct the study in those departments. We also are indebted to Dr Sreekumari K, Former Joint Director of Medical Education, Kerala, for facilitating the conduct of this study at Government Medical College, Thiruvananthapuram.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.