
Abstract
Background:
Neurocognitive deficits are noted in anxiety disorders (ADs), albeit with several inconsistencies. The relationship between neurocognition and metacognition may have potential implications for understanding cognitive dysfunction but is poorly understood in ADs. This study aimed to examine the relationship between neurocognition and metacognition in ADs, with a cross-sectional design.
Methods:
The sample included ADs (n = 25) and nonclinical (n = 25) groups matched on age, gender, and education. Neurocognition was assessed using tests for intelligence, attention, working memory, fluency, flexibility, set-shifting, inhibition, planning, and memory; and metacognition using Metacognition Questionnaire-30 (MCQ-30) and Metacognitive Awareness and Regulation Scale (MARS).
Results:
Compared to comparison/normative scores, the anxiety group showed significantly poorer performance on zoo map test (low demand trial; P = 0.007), rule shift cards 1 (P ≤ 0.001), rule shift cards 2 (P ≤ 0.001), and logical memory immediate recall (P ≤ 0.001) and delayed recall (P ≤ 0.001); greater negative beliefs about worry (P = 0.005), and poorer metacognitive awareness and regulation (P = 0.01). Greater cognitive self-consciousness was correlated with better planning (Spearman’s rho = −0.509, P = 0.009).
Conclusions:
Individuals with ADs show neurocognitive difficulties in planning, set-shifting, and logical memory, dysfunctional metacognition, and reduced metacognitive awareness and regulation. Cognitive self-consciousness is linked to better planning. The interrelationships between neurocognition and metacognition may have potential implications for clarifying inconsistent findings and designing novel cognitive interventions in ADs.
Relative to a nonclinical comparison group, individuals with anxiety disorders demonstrate under-performance in planning, set-shifting, and logical memory; Individuals with anxiety disorders also show greater negative beliefs about worry and poorer metacognitive awareness and regulation; Cognitive self-consciousness was correlated with better planning.Key Messages:
Anxiety disorders (ADs) are characterized by intense and debilitating anxiety, 1 with high cooccurrence and shared vulnerability factors, emphasizing the need for a transdiagnostic approach. 2 They are associated with a significant burden and disability in social and occupational functioning.3 In other psychiatric disorders, neurocognitive deficits have been considered a significant contributor to disability.4, 5 However, neurocognition has received limited attention in ADs. Research has documented specific neurocognitive deficits in different ADs, as well as similarities across disorders. For instance, deficits in inhibition, set-shifting, and working memory have shown up as longitudinal risk factors for the severity of generalized anxiety disorder (GAD). 6 Social anxiety disorder (SAD) is linked to poorer working memory and set-shifting in general as well as during social stress.7, 8 However, there are several inconsistencies in neurocognitive findings in ADs, which are partly attributed to methodological heterogeneity. 10 For instance, verbal and visual memory have been implicated in SAD, panic disorder, and GAD in some studies9, 10 but not others. 11
In certain psychiatric disorders such as schizophrenia, obsessive-compulsive disorder (OCD), and depression, inconsistent findings on neurocognitive performance have been traced to factors such as stereotype threat, momentary negative influences, and attitudes to testing12–15—which point to the role of metacognition. Metacognition is the capacity to assess, reflect, control, and evaluate one’s cognitions. 16 Metacognition has been predominantly studied in psychiatric disorders as metacognitive experience/awareness of cognitive biases 17 and knowledge of one’s own and others’ mental states. 18 In relation to (neuro)cognitive abilities, metacognitive beliefs about uncontrollability and the need to control thoughts were related to set-shifting difficulties in a community sample with depressive and anxiety symptoms. 19 However, metacognitive monitoring of cognitive abilities/difficulties and regulatory strategies in line with goals (as originally described by Flavell, “you (unlike your brother) should use Strategy A (rather than Strategy B) in Task X (as contrasted with Task Y)” 20 )—has received attention in educational settings 21 but not in psychiatric disorders. In nonclinical samples, certain metacognitive processes have demonstrated an impact on cognitive abilities, for example, ruminations, “choking” (excessive self-focus on well-practiced tasks), and interpretations of one’s anxiety and ability.22–24
Despite the impact of anxiety and metacognitive factors on cognitive abilities, to the best of our knowledge, no studies have been published investigating these in a sample of ADs. The lack of such holistic investigations may hinder the understanding of cognitive dysfunction in ADs. This may be partly attributable to a lack of available scales to assess metacognitive monitoring of cognitive abilities. This study aimed to investigate the relationship between neurocognition and metacognition (awareness and regulation of cognitive abilities, as well as cognitive biases) in a sample of ADs. It was hypothesized that individuals with ADs would have greater difficulties with neurocognition and metacognition compared to a nonclinical comparison group and that neurocognitive and metacognitive variables would show significant associations.
Methods
A cross-sectional design was employed and is reported below in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. 28
Participants
Based on sample availability and considering the study timeline, 30 individuals each were expected to be recruited in the clinical and nonclinical comparison groups. The clinical sample comprised individuals diagnosed with AD, confirmed by the Mini Neuropsychiatric Interview (MINI) Plus, 29 recruited from the psychiatric inpatient and outpatient services of the National Institute of Mental Health and Neuro Sciences, Bangalore, between July 2018 and March 2019. Participants were included if in the age range of 18 to 50 years, with a minimum of seven years education, fluent in English, willing for psychological testing, and right-handed as per the Edinburgh Handedness Inventory—Short Form. 30 Individuals were excluded if they had comorbid schizophrenia, bipolar affective disorder, psychosis, or OCD; substance dependence (other than nicotine) or behavioral addictions; history of tumors, epilepsy, stroke, traumatic brain injury, or degenerative disorders; developmental disorders such as autism spectrum disorder and attention deficit hyperactivity disorder; clinical evidence for intellectual/learning disability or any sensorimotor impairments that interfered with performance on assessments. Of the 49 individuals who met the inclusion criteria, 24 were not recruited (details in Figure 1), and 25 formed the final sample.
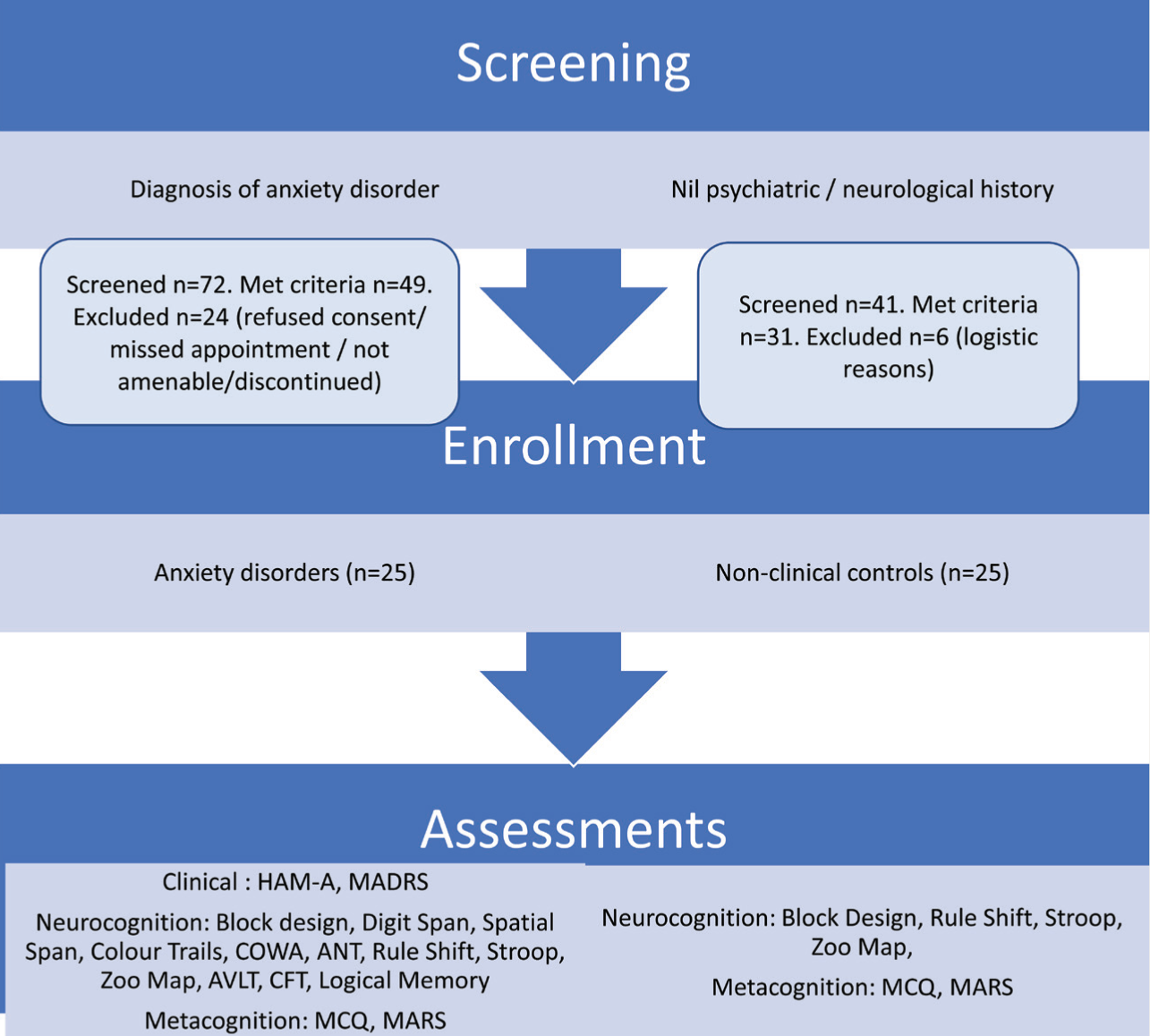
HAM-A – Hamilton Anxiety Rating Scale; MADRS – Montgomery Asberg Depression Rating Scale; COWAT – Controlled Oral Word Association test; ANT – Animal Names; AVLT – Auditory Verbal Learning Test; CFT – Complex Figure Test; MCQ – Metacognitions Questionnaire; MARS – Metacognitive Awareness and Regulation Scale.
The comparison sample consisted of individuals from the community recruited through the snowball technique from hospital staff and their friends and acquaintances, who were screened for psychiatric disorders using the MINI Plus. They were group-matched to the clinical sample in terms of age and gender (same number of individuals within each age subgroup as the clinical sample: 18–20 years, 21–25 years, 26–30 years, 31–35 years, 36–40 years, 41–45 years, 46–50 years; males and females). The two groups were caliper-matched with regard to education (± 2 years). All participants were fluent in English, willing for psychological testing, and right-handed as per the Edinburgh Handedness Inventory – Short Form. Exclusion criteria were any neurological, developmental, or psychiatric disorders, substance dependence (other than nicotine), clinical evidence of intellectual disability, specific learning disability, or sensorimotor impairments that interfered with performance on assessments. Of the 31 individuals who met the criteria, 25 formed the comparison sample (details in Figure 1).
Materials
Screening and Clinical Assessments
Apart from Edinburgh Handedness Inventory and MINI Plus, the clinical sample was administered the Hamilton Anxiety Rating Scale (HAM-A) 31 and the Montgomery-Asberg Depression Rating Scale (MADRS) 32 to assess the severity of anxiety and depression symptoms. All assessments were conducted in English.
Assessment of Neurocognition
A battery of assessments was used to assess neurocognitive variables.
Block design test (Wechsler Abbreviated Scale of Intelligence II) 33 for intelligence: This assesses participants’ visuospatial and organizational abilities and nonverbal problem-solving skills, using a set of blocks to replicate a design printed on a card, within a time limit. The correctly reproduced designs are scored according to certain criteria, with time bonuses.
Color trails test 34 for focused attention, scanning, and mental flexibility: The participant is required to find numbers from 1 to 25 in sequence, from randomly arranged color circles on a sheet and on Color Trails 2, in alternating colors. The score is the time taken for each condition.
Digit span (Wechsler Memory Scale III – India [WMS III – India]) 35 for verbal working memory: This test requires participants to recall a series of digits in the presented and reverse order. The final score is the total number of correctly recalled items in both conditions.
Spatial span (WMS III – India) 35 for visual working memory: This test requires participants to tap select blocks on a board in the presented and reverse order;
Controlled oral word association test (COWAT) 36 for phonemic fluency: The participant is required to spontaneously produce words beginning with a particular letter. The final score is the average number of words produced for.
Animal naming test (ANT) 36 for category fluency: In this test, the participant is instructed to provide words belonging to a given category within a time limit.
Stroop test 37 for response inhibition: The test involves three conditions—color naming (XXXX printed in different colors), reading color names (all printed in black), and naming the print color for different color names (e.g., RED printed in green ink). The time taken and the number of errors made on the final condition are noted and used to calculate the interference score, that is, the inhibition of prepotent responses.
Rule shift cards (Behavioral Assessment of Dysexecutive Syndrome or BADS) 38 for set-shifting: This test uses playing cards in red and black with different rules for different parts of the task. It assesses the ability to shift to a new rule and ignore a previous rule. Scoring is based on the time taken and the number of errors.
Zoo map test (BADS) 38 for planning: This assesses the ability to profit from feedback and formulate and implement a plan. The subject is instructed to indicate the path they would take when visiting a zoo while following certain rules. Scoring is based on the successful implementation of the plan. Penalties are imposed for rule violations and lack of speed.
Auditory verbal learning test (AVLT) 36 for verbal learning and memory, by assessing the ability to reproduce 15 words from a presented list: The test includes (a) learning phase with five successive presentations of a list followed by an immediate recall from the participant, (b) interference condition with the presentation of a different list, (c) delayed recall after a delay of 30 minutes, and (d) recognition of presented words amongst unfamiliar words.
Logical memory test (WMS III – India) 35 for verbal logical memory: This assesses the ability to recall two short stories, with a delayed recall after 30 min, and recognition of facts with yes/no responses.
Complex figure test (CFT) 36 for visual learning and memory, The test consists of an abstract complex design that cannot be named easily. It involves (a) copy phase, (b) immediate recall after 3 min, and (c) delayed recall after 30 min. Scoring is based on the number of figural elements correctly drawn and correctly placed.
Assessment of Metacognition
Metacognition was assessed with regard to cognitive biases (Metacognition Questionnaire-30 [MCQ-30]) and cognitive abilities (Metacognitive Awareness and Regulation Scale [MARS]).
MCQ-30 17 is a 30-item rating scale that assesses five metacognitive factors (higher scores indicating greater dysfunction): cognitive confidence, positive beliefs about worry, cognitive self-consciousness, negative beliefs about the uncontrollability of thoughts and danger, and beliefs about the need to control thoughts. Subscale-total correlations range between 0.30 and 0.83, with Cronbach’s alpha between 0.72 and 0.93. The MCQ has been validated in India and shows acceptable internal consistency, and confirmatory factor analysis shows a good fit for the five sub-scales. 26 It has also been used in previous studies in India. 25
MARS: Since no appropriate tools were available in the literature to assess metacognitive monitoring of cognitive abilities in adults with psychiatric disorders, the authors developed a new tool in accordance with scale construction procedures. 39
Item generation: The domain identified for the scale was metacognitive monitoring of cognition, including cognitive deficits (e.g., attention, memory, executive functions—flexibility, updating and inhibiting, planning, and decision-making) and biases (negative attentional bias, error monitoring, need for perfection, uncertainty tolerance, worry, and rumination). Item generation was done by consulting available scales on cognitive dysfunction and metacognition17, 21, 40–43 and writing new items to accommodate all identified constructs. Ensuring that the initial pool was roughly double the intended number of items, 39 51 items were generated, with five-point Likert responding, from “Always” to “Never.”
Item analysis: Qualitative item analysis for content relevance, representativeness, and technical quality 39 was done by four clinician experts (>15 years’ experience in cognition and psychiatric disorders). The experts rated each item on: (a) Does the item measure the construct? (b) Is the content suitable for individuals with psychiatric disorders with ≥7 years of education? (c) Is it appropriately worded?
Item selection and modification: Item modification was done iteratively in several steps. After removing items violating item-writing rules (e.g., double negatives, compound statements, lack of clarity) or showing repetitions or lack of relevance, 30 items were selected. Based on suggestions from experts, 11 items were modified, and 8 were replaced by new ones, to ensure appropriate representation of the initially identified domain. To guard against response choice bias, 16 of the 30 items were worded negatively. The resulting items were re-checked for clarity of stem and response; further modification/simplification was done following trial administration with five end-users.
Inter-rater agreement: Four of the investigators assessed item scoring determinants (stems, anchors, and reverse scoring). Items with <75% inter-rater agreement were removed.
The final tool comprised 26 items (Table S1). Items are scored 5 to 1 (with 16 reverse-scored items), with a minimum score of 26 and a maximum of 130, with higher scores indicating better metacognitive awareness and regulation. On pilot testing, MARS showed moderate correlations with MCQ (convergent validity—MCQ-30 total, −0.38; negative beliefs about worry, −0.45; need to control thoughts, −0.29) and satisfactory internal consistency (Cronbach’s alpha of 0.74). 44
Procedure
The study was approved by the Institute Ethics Committee, and written informed consent was obtained from all participants. Participants were tested individually, with a preset sequence of tests, and breaks were offered as per participant’s preference, in order to minimize fatigue. The comparison group (n = 25) was assessed on MCQ-30 and MARS and only selected neurocognitive tests for which Indian normative scores were unavailable (details in Figure 1). For the remaining tests of neurocognition, the clinical group’s performance was compared with the existing normative scores.
Statistical Analysis
The data were analyzed using the Statistical Product and Service Solutions (SPSS; Version 20.0. Armonk, NY: IBM Corp.). Means and standard deviations (SD) were calculated for continuous variables and frequencies and percentages for categorical variables. The clinical group scores were compared to normative scores (mean values) where available, using the one-sample t-test. For the other tests employing comparison group comparisons, the Mann–Whitney U test was used (since the Shapiro–Wilk test for normality showed nonnormal distribution). In view of the number of variables compared, a conservative significance of P < 0.01 was chosen to minimize type I error. The relationship of neurocognition with metacognition was investigated using Spearman’s correlation.
Results
Sample Characteristics
As expected in matched samples, the clinical and comparison groups were similar on age (mean ± SD: comparison group 27.52 ± 7.81, clinical 28.32 ± 7.99, P = 0.71), gender (10 females and 15 males), and years of education (comparison group 15.32 ± 2.23, clinical 15.44 ± 2.31, P = 0.79). All participants were from middle socio-economic strata, urban background.
The clinical group included 23 outpatients and two inpatients, with a diagnosis of SAD (n=11), panic disorder (n=8), GAD (n=6), specific phobia (n=5), agoraphobia (n=2), hypochondriasis (n=2) and adjustment disorder (n=1)., with nine individuals meeting the criteria for more than one AD. The clinical group had moderate levels of anxiety and depression (HAM-A mean 18.60 ± 5.21, MADRS mean 11.44 ± 6.04), and had a few comorbidities (mean number of comorbid ADs = 1.44 ± 0.65 and mean number of other co-morbid disorders = 0.6 ± 0.76). The mean duration of illness was 98.20 ± 69.59 months (mean age at onset 20.08 ± 7.34 years), with 12 individuals on pharmacological treatment and 23 individuals undergoing psychotherapy (predominantly cognitive behavior therapy). Of the 12 individuals on medications, 10 were on selective serotonin reuptake inhibitors (SSRIs; Escitalopram, n = 5; Sertraline, n = 4; Paroxetine, n = 1), and one individual each was receiving Bupropion and Mirtazapine.
Performance of the Clinical and Comparison Groups on Neurocognitive Tasks
The clinical group was slower than the comparison group on Zoo map test (specifically, the low demand trial) and rule shift cards; and obtained lower scores on logical memory (Table 1). However, the clinical group performed better on COWAT, ANT, digit span, and spatial span in comparison to normative scores.
Performance of Clinical and Comparison Groups on Neurocognitive Tests
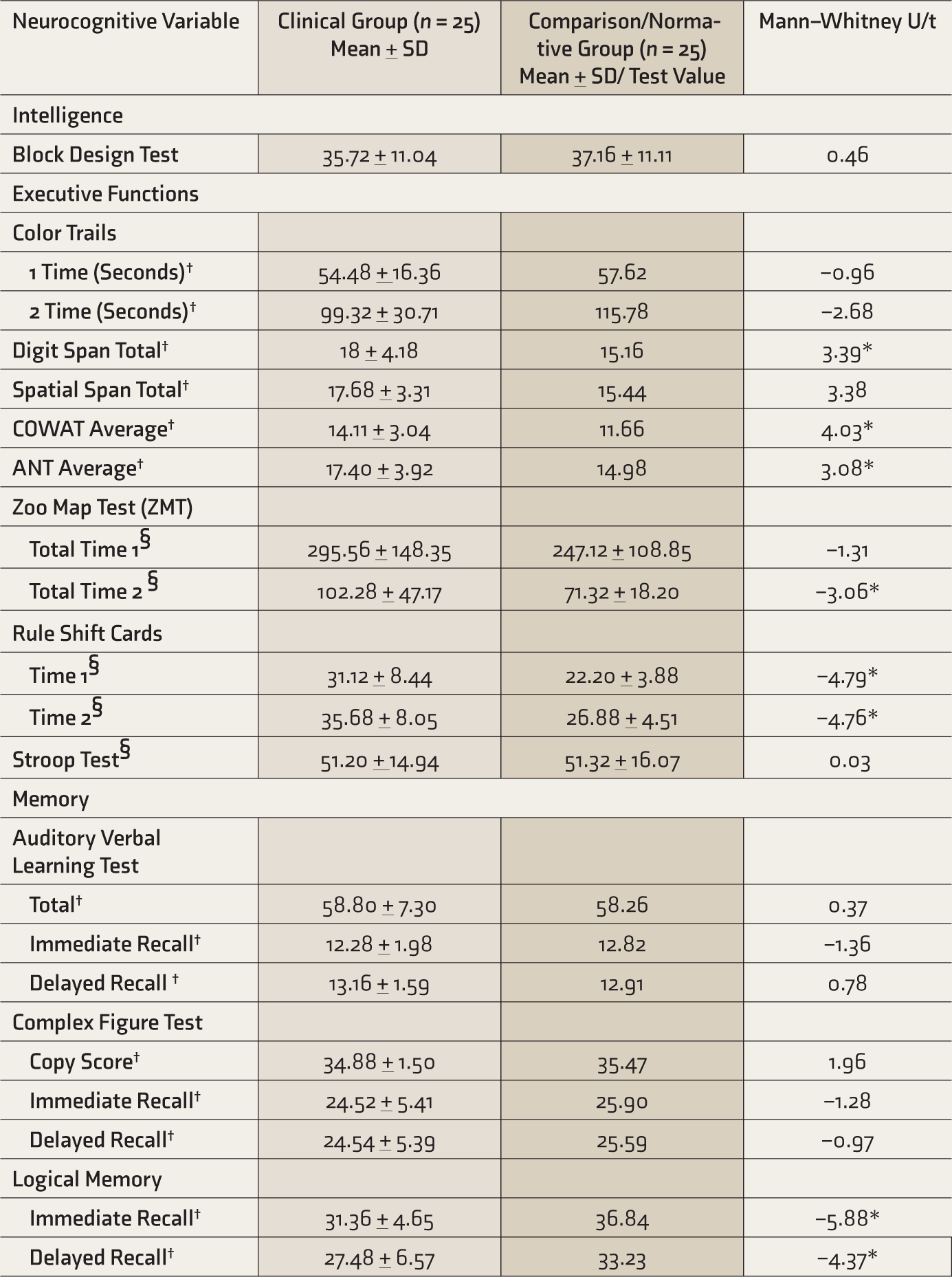
COWAT, Controlled oral word association test; ANT, Animal names, †Compared to normative data, using one-sample t-test, §Compared with control group using Mann–Whitney U test, *significant at 0.01 level.
Performance of the Clinical and Comparison Groups on Metacognitive Variables
Table 2 shows that the clinical group had significantly higher negative beliefs about worry (MCQ) and lower scores on metacognitive regulation (MARS).
Performance Of Clinical And Comparison Groups On Metacognitive Variables
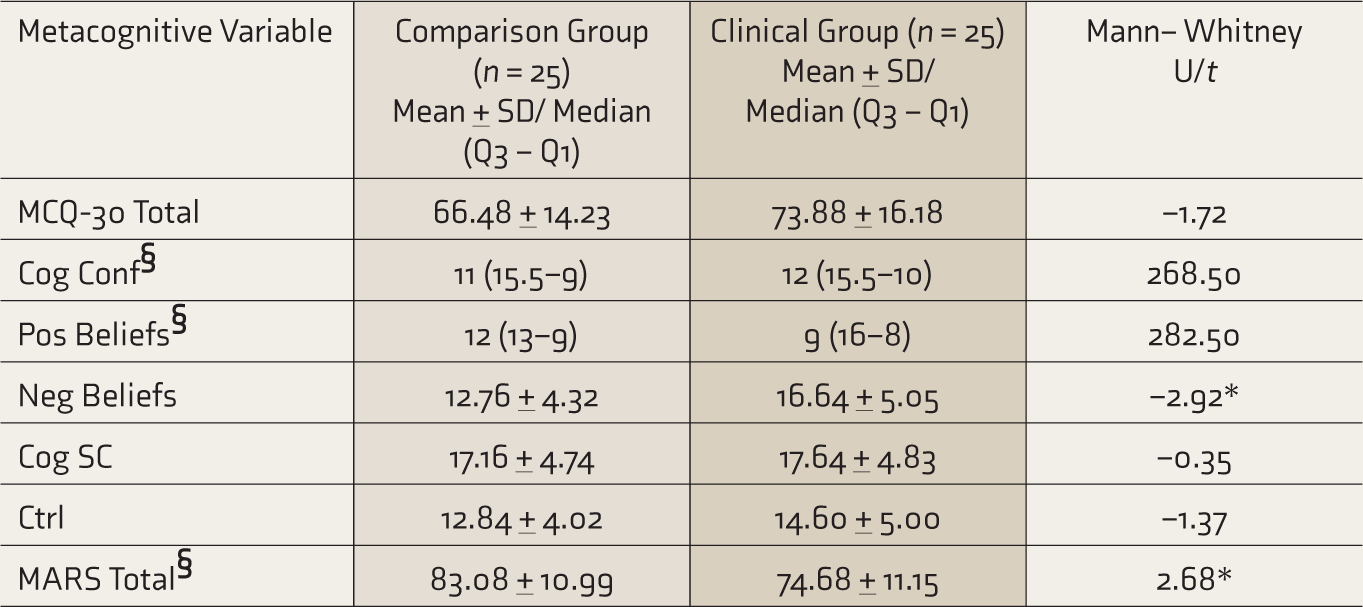
MCQ-30, Metacognition questionnaire-30; Cog Conf, Cognitive confidence; Pos Beliefs, Positive beliefs about worry; Neg Beliefs, Negative beliefs about worry; Cog SC, Cognitive self-consciousness; Ctrl, Need to control thoughts; MARS, Metacognitive awareness and regulation Scale. §Non-normally distributed variables, Mann–Whitney U test reported, *significant at 0.01 level.
Correlation between Neurocognition and Metacognition in the Clinical Sample
Higher cognitive self-consciousness on the MCQ was associated with lower time on the Zoo map test (P = 0.009). In addition, a few other associations showed trends toward significance: cognitive self-consciousness with lower time on color trails 1 (P = 0.046) and higher scores on digit span (P = 0.047) and block design (P = 0.02), and MCQ negative beliefs about worry with higher time on rule shift cards 2 (P = 0.03) (Table 3).
Correlation Between Neurocognition and Metacognition in the Clinical Sample
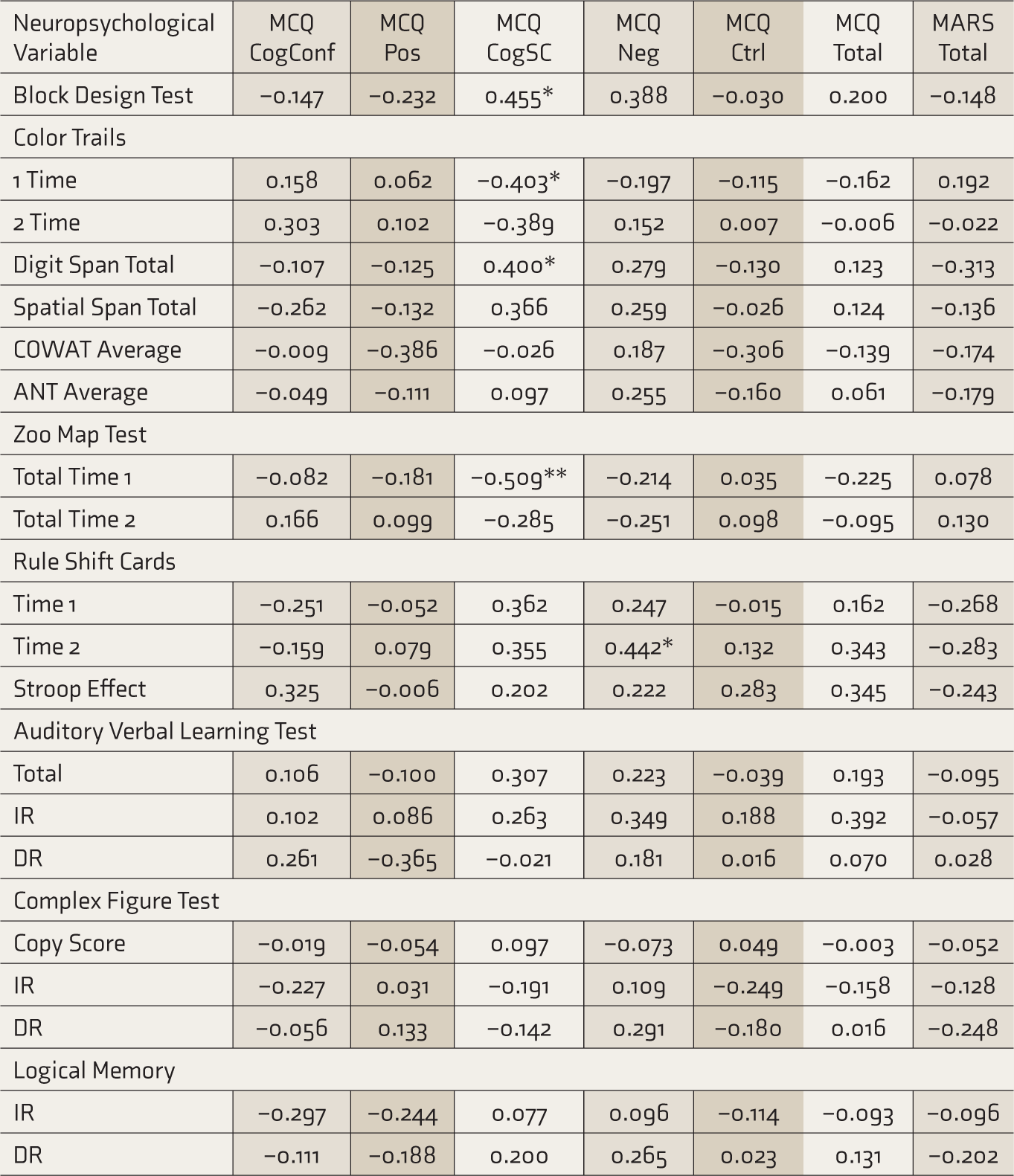
MCQ, Metacognition questionnaire; CogConf, Cognitive confidence; Pos, Positive beliefs about worry; CogSC, Cognitive self-consciousness; Neg, Negative beliefs about worry; Ctrl, Need for control; MARS, Metacognitive awareness and regulation scale; COWAT, Controlled oral word association test; ANT, Animal names. *significant at 0.05 level, **significant at 0.01 level.
Discussion
We aimed to examine neurocognition and metacognition in ADs and investigate the relationship between the two. The study’s main findings are that individuals with ADs (relative to nonclinical comparison group) exhibit significantly poorer performance on neurocognitive measures (planning, set-shifting, and logical memory), poorer metacognitive awareness and regulation of cognition, and greater negative beliefs about worry. Neurocognitive and metacognitive variables were interrelated: greater cognitive self-consciousness was associated with better performance on planning.
With regard to neurocognition, the anxiety group demonstrated poorer planning than the comparison group, but only in low-demand conditions. Previous studies have also noted poorer performance on lower-level tasks, with preserved performance on higher-level tasks in panic disorder 45 and OCD.46, 47 This has been linked to heightened performance monitoring, proposed as a transdiagnostic marker in anxiety. 48 Set-shifting reductions noted in our study were mainly on timed tasks, which may explain the inconsistencies observed across studies.7, 45, 49, 50 This study found poorer memory relative to the comparison group on a story task but preserved memory for list-learning and complex figure tasks. These findings are corroborated by other studies.7, 11, 51–53 The discrepancies across memory tasks could be related to the varying task demands (story tasks have more densely packed information, whereas list-learning tasks provide multiple trials, facilitating rehearsal) but may also be impacted by metacognitive factors. For instance, the story task appears to trigger anxiety and metacognitive beliefs about own abilities (e.g., anxious patients often remarked, “It’s too much, I blanked out”); in contrast, list-learning tasks may regulate anxiety through habituation over multiple trials. The use of concurrent assessments of metacognition during neurocognitive tests may help empirically investigate these possibilities. 54
Interestingly, the anxiety group performed better than the normative scores on tests of working memory (verbal and visual) as well as fluency (phonemic and categorical). This may have several explanations. The mean age of the anxiety group was lower than that of the normative sample for the fluency tasks — younger age is known to be associated with better performance on tasks of attention, working memory,55, 56 and verbal fluency.57–60 It is also possible that better scores in the anxiety group may converge with the improved attention control observed in GAD and attributed to metacognitive re-allocation of attention. 61
In consensus with the literature in ADs,62–66 this study found greater negative beliefs about worry on MCQ. The MCQ scores our nonclinical sample obtained are largely comparable to a previous Indian study. 25 Further, greater negative beliefs about worry on MCQ were correlated with set-shifting difficulties in this study, corroborating previous findings in a mixed psychiatric and community sample. 19
Cognitive self-consciousness (the tendency to observe one’s own cognitive processes) on MCQ was correlated with better performance on planning. Cognitive self-consciousness appears similar to the construct of metacognitive monitoring. 20 Flavell observed that metacognitive monitoring might help facilitate cognitive performance in children or be unhelpful “if used in excess or nonselectively.” Our findings appear to illustrate the adaptive and maladaptive aspects of metacognitive monitoring. Adaptive metacognitive monitoring/greater cognitive self-consciousness may have facilitated performance on planning, perhaps through better error detection, conflict resolution, attention allocation, and strategy selection. 67 The slower performance on the easier condition of planning (with preserved speed on the difficult condition) might indicate excessive cautiousness and “unhelpful” monitoring in easier conditions, as suggested by other authors.45, 47 Such excessive, explicit performance monitoring has been shown to interfere with performance, particularly on automatized lower order tasks.48, 68 Contrastingly, individuals with psychiatric disorders may also lack metacognitive awareness and regulation of task performance. For instance, poorer metacognitive awareness of attentional abilities has been demonstrated in individuals with Attention Deficit Hyperactivity Disorder (ADHD), in the form of a discrepancy between objective neurocognitive assessments and self-evaluation of performance. 69 Other research has shown that individuals with depression, OCD, and schizophrenia report greater negative momentary influences and fear about test outcomes during neurocognitive test performance12–15 —it has been emphasized that such factors must not be merely considered “noise” but may provide important insights into neurocognitive impairments. 70 Such influences may be reported to a greater extent by individuals with psychiatric disorders, as they may be unable to metacognitively regulate the impact of these factors on task performance; nevertheless, the “metacognitive” aspect of such factors has not received much attention. In contrast, research on nonclinical populations has indicated the metacognitive impact of anxiety, stereotype threat, and ruminations on task performance.22, 24, 71 In line with the above findings,12–15, 69 this study also provides evidence for poorer metacognitive awareness and regulation in ADs and a new quantitative measure, the MARS. The development of the MARS represents an important step in the empirical investigation of metacognition in relation to cognitive abilities. However, further investigation of the psychometric properties of MARS is pending.
The small samples limit the present findings. Although the sample size was originally estimated based on availability, posthoc power analysis of set-shifting (a variable implicated in previous studies as well as statistically significant in this study) indicates that a sample of 16 in each group would be sufficient to detect a significant difference between the two groups at 95% power. While the heterogeneous clinical sample makes it difficult to rule out confounding factors, it contributes to the generalizability of findings and is in line with transdiagnostic approaches to anxiety—multiple cooccurring ADs being closely representative of the population. Consideration of a continuum of anxiety among healthy and clinical participants might have enhanced generalizability. The severity of anxiety and depression and ongoing treatment (pharmacotherapy, psychotherapy, or both) may have affected neurocognitive and metacognitive findings. Other medical comorbidities (apart from neurological conditions, which were excluded) were not documented and may also have affected neurocognitive performance. Considering the large number of variables and associations studied, employing a Bonferroni correction may have reduced the chances of a Type I error. However, differences between the clinical and comparison groups on neurocognitive variables have been considered at a more conservative 0.01 level. Comparison with normative data was not possible for all the neurocognitive assessments. Hence, a matched nonclinical comparison group was used for some tests; a uniform comparison group might have been ideal. Lastly, the newly developed MARS was utilized in this study since there were no other existing tools. However, further research is needed on its psychometric properties.
Conclusions
This study found neurocognitive difficulties, dysfunctional metacognition, and reduced metacognitive awareness and regulation in individuals with AD, compared to a nonclinical comparison group. Our findings also suggest that certain metacognitive variables are linked to better neurocognitive performance, which may have implications for interventions. The study provides evidence for the inter-relationship between neurocognitive and metacognitive variables, which may explain the puzzling inconsistencies in cognitive performance found within subjects and across studies. Consideration of the neurocognitive and metacognitive deficits in ADs may have potential implications for designing novel cognitive interventions or modifying existing ones.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors would like to thank the expert raters of the new tool—Professor YC Janardhan Reddy, Professor Paulomi Sudhir, Prof Shyam Sundar Arumugham, and Dr Marcelo Batistuzzo.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by a Junior Research Fellowship to Ashwini Vishwanathan from the University Grants Commission, Government of India. The funding agency had no involvement in the study design, data collection or preparation of manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.