
Abstract
Background:
Studies focusing on assessing social cognition deficits in schizophrenia have been expanded to bipolar disorder considering the similarities shared between the two conditions. Existing research has identified significant deficits in social cognitive skills independent of mood states and neurocognitive deficits, which could indicate the potentiality of this domain to be an endophenotype for bipolar disorder.
Methods:
The current study assesses the impairments in social cognition in patients with bipolar disorder and their first degree relatives, simultaneously testing for neurocognition as well, and comparing their performance to healthy controls. Fifty four participants were recruited, with 18 participants in each group. MATRICS Consensus Cognitive Battery was used to test neurocognition and Social Cognition Rating Tool in Indian Setting was administered for testing social cognition.
Results:
Significant deficits were found in social cognition and neurocognition (at p<.01) in the patient group when compared to both probands and healthy controls but no difference between probands and healthy controls. This finding established impairments in socio-cognitive functioning in remitted patients. Conclusion: The study has identified persistent deficits in social and neuro-cognition despite remission, having significant clinical implications in terms developing remediation programs for social cognition and planning early intervention as social cognition deficits have been identified as potential risk factors.
(1) Bipolar disorder patients (currently in remission) have significant neurocognitive and socio-cognitive deficits, indicating it could be an under recognized symptom domain. (2) The lack of difference in performance of the first degree relatives and healthy controls on the tests, indicate that social cognition and neurocognition may not be an endophenotype in bipolar disorder.Key Messages:
There is substantial evidence 6 that patients with BPAD suffer problems in cognitive and social cognitive functions in euthymic and remitted states. 5 A combined assessment approach is mandatory in understanding the deficits. 6 Recent research implies a moderate impairment in cognitive functioning in BPAD, with coexisting sociocognitive deficits. 9 Studies also found that these functions deteriorate over the course of the disorder and the outcomes appear to be unfavourable.7, 8
As deficits in neurocognition and social cognition have been well established mostly in schizophrenia, psychological management for these is focused only on that population. An Indian study assessing the neurocognitive functioning in stable patients with BPAD reported that compared to controls, the patients performed poorly overall in frontal functions, with lower scores in Mini Mental State Examination and Trail Making A and B, indicative of deficits in general cognitive abilities. 20
Currently, deficits with clinical significance have been identified only in symptomatic patients, but these impairments persist even in the remission phase, leading to poor prognosis.9–11 It has been observed that cognitive abilities such as executive functioning and attention are compromised in first-degree relatives (FDR) of patients with BPAD when compared to healthy controls. 12 Further research is mandatory in studying these variables in the context of BPAD, as examining whether there is a persistence of deficits in social cognition is necessary to determine whether it can be understood as a trait marker of the illness. 13
Discrepant findings in the current understanding of the level and nature of cognitive and sociocognitive impairment in BPAD patients in remission as well as their FDR posit a major need for the assessment of the said variables. The need to identify sociocognitive and neurocognitive impairments in FDR and BPAD patients in comparison to healthy controls is vital to investigate whether the said domains could be a premorbid marker. It would aid in the efforts of finding risk-related genes for the illness alongside therapeutic strategies and early intervention.
Materials and Method
This study employed a cross-sectional design. The participants consisted of patients with BPAD, their FDR, and healthy controls. Data collection was done in a single phase, and it was spread over a period of four months from January 2019 to April 2019. The study was conducted in a hospital setting (Kasturba Medical College, Manipal), from where the patients and FDR were recruited. The healthy controls were taken from the researcher’s neighborhood.
The objectives of the study were to assess social and nonsocial cognition in patients with BPAD, their FDR, and healthy controls and to compare the social and nonsocial cognition in patients with BPAD, their FDR, and healthy controls.
Ethical clearance was obtained from the Institution Ethics Committee, and the CTRI number (CTRI/2019/01/016845) was obtained.
The sample of the study comprised three different groups. The first group included patients diagnosed with BPAD (currently in remission), the second group consisted of FDR of patients with BPAD, and the third group included healthy controls who had no diagnosable mental health condition.
Inclusion Criteria
Exclusion Criteria
The sampling procedure was convenient sampling. The sample size was determined by a consultation with the Statistics Department of Manipal Academy of Higher Education, using GPower software. The statistician assessed the proposed hypotheses and chose mean difference calculation (multivariate analysis) as the appropriate inferential statistics to be used to analyze the data. The difference value was set at 5 and the power value was set at 0.9, to arrive at the sample size of 90. The obtained sample size was only 54, owing to the difficulty in collecting sample meeting criteria. This has been accounted for as a limitation.
A total of 54 participants inclusive of 18 participants with a diagnosis of BPAD (currently in remission), 18 FDR, and 18 healthy controls were recruited for the study. Participants meeting the inclusion and exclusion criteria for BPAD (currently in remission) and their FDR were recruited from the Department of Psychiatry, KMC, Manipal, and A. V. Baliga Memorial Hospital, Udupi, by the principal investigator. FDR would denote parents, offspring, and siblings. In case of refusal of participation by either the patient or their FDR, neither of them was included in the study. The principal investigator recruited the healthy controls from Manipal neighborhood as well as the general staff, housekeeping staff, and students, after due consent. It was ensured that the participants from the Department of Medicine do not have any acute physical illness.
Following their agreement to participate, an informed consent (presented as a written document and signed by the patient) was obtained. The author had attended training workshops for both MATRICS Consensus Cognitive Battery and Social Cognition Rating Tools in Indian setting. The questionnaires and tests were then administered to the participants, with adequate breaks given upon requirement. The measures used in the study were as follows:
Tools Used
Statistical Analysis
Data were analyzed using computerized Statistical Package for Social Sciences (SPSS23.0). Normality testing was done using the Shapiro–Wilk test. Descriptive statistics was used to analyze and understand the sociodemographic data. As the small sample size of 54 did not correspond to a normal distribution, the non-parametric tests of Kruskal–Wallis and Mann–Whitney U were employed to measure the same. Bonferroni correction was used for controlling for error owing to multiple hypothesis testing. P values were divided by 3, and significance was based on the corrected P value. The cutoff values for eta-squared was set at 0.01 (small), 0.06 (medium), and 0.14 (large). Cohen’s d was set at 0.2 (small), 0.5 (medium) and 0.8 (large).
Results
The mean±SD age of the sample for patients with BPAD (currently in remission) is 37±10.30 years. With respect to FDR, the mean age was found to be 38±13.75 years. The healthy controls group had a mean age of 37±11.95 years. Amongst the sample obtained, the percentage of males and females were equal with regard to BPAD patients and healthy controls, but the FDR group had twice the number of males as compared to females. Overall, the participants from all three groups were from a similar socioeconomic background.
The patients’ mean duration of illness was 8±2.17 years, and the mean number of episodes was 4±3.81. Their education level was mismatched across the groups, as the healthy controls group had a significant amount of graduate level participants, whereas the patient group had a larger number of primary and secondary educated people. However, the levels were not significantly disproportionate while comparing patient group and FDR (
Socio-demographic Characteristics
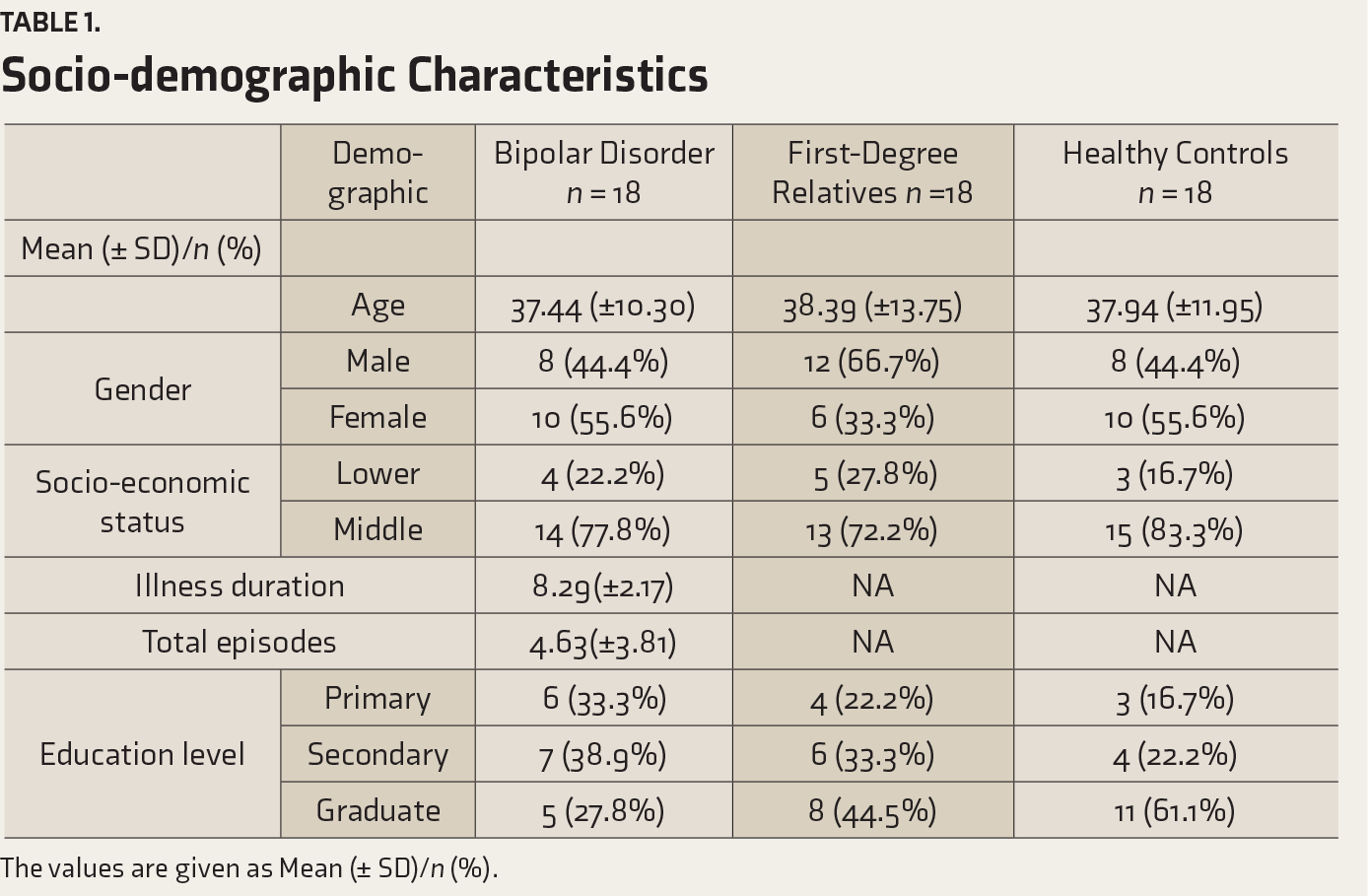
The values are given as Mean (± SD)/n (%).
Assessment of Social Cognition Across the Groups
Analysis of scores on SOCRATES showed that there was a significant difference in first-order TOM and second-order TOM. There was a significant difference in the faux pas recognition index as well. With regard to attribution, a significant difference in personalizing bias was observed. For the last domain of affect processing, there was a significant difference in the social perception index. Medium effect size was present for the second-order TOM and faux pas composite index while there was no significant effect size for the other domains (
Kruskal–Wallis Test Comparing all the Subdomains of Social Cognition and Neurocognition Based on the Groups
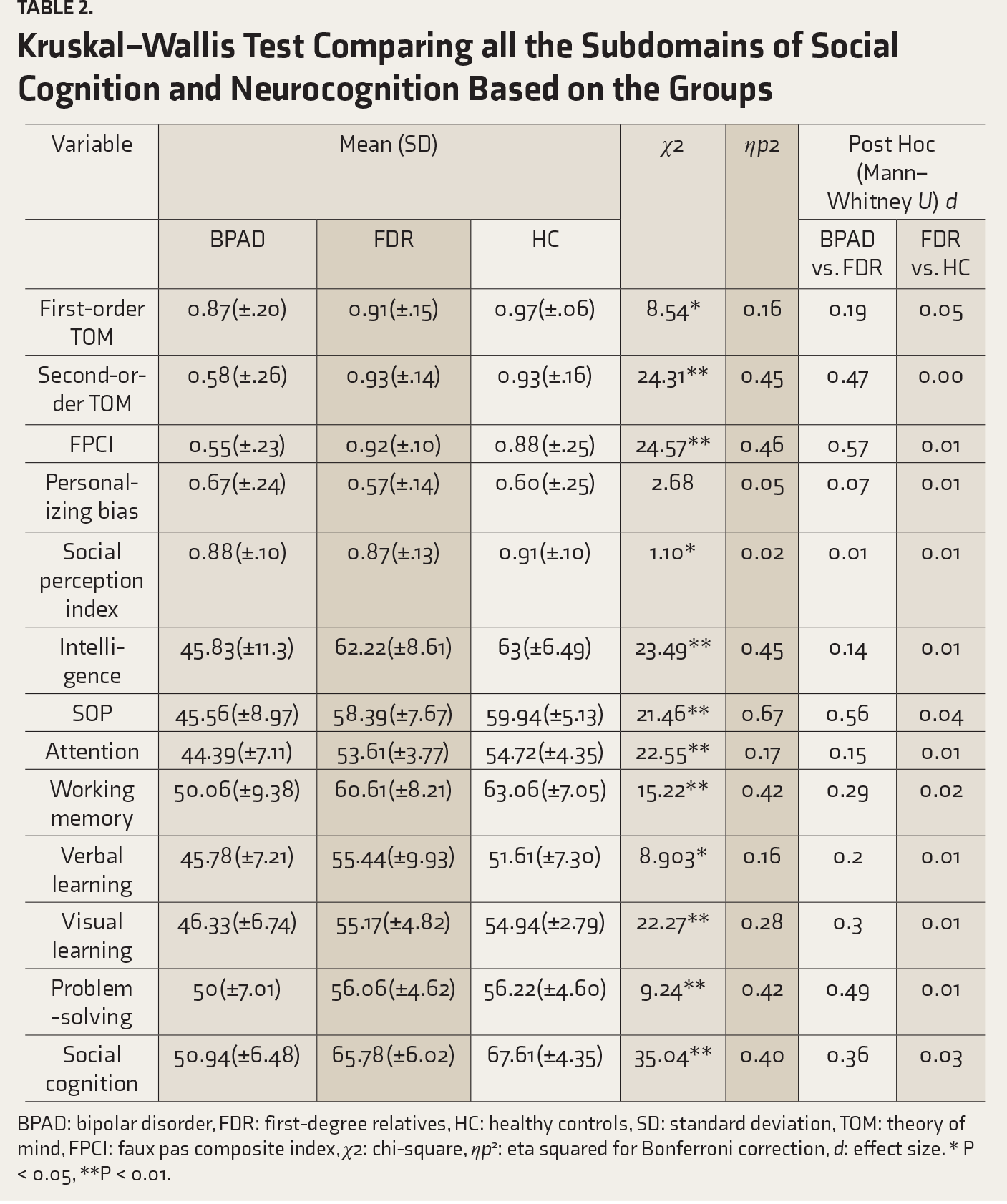
BPAD: bipolar disorder, FDR: first-degree relatives, HC: healthy controls, SD: standard deviation, TOM: theory of mind, FPCI: faux pas composite index, χ2: chi-square, ηp 2 : eta squared for Bonferroni correction, d: effect size. * P < 0.05, **P < 0.01.
The results of the Mann–Whitney U test, comparing FDR and healthy controls, revealed no significant difference in the performance of the two groups on the domains of the first-order TOM or faux pas index. The lack of difference was consistent across other domains of the second-order TOM, personalizing bias, and social perception index. No significant effect size was obtained (not even a small effect size) for any of the subdomains (
Analysis of scores between BPAD patients and FDR revealed a significant difference in the performance of the two groups on the domains of the first-order TOM, the second-order TOM, and faux pas index, with a medium effect size for both second-order TOM and faux pas index. The scores on personalizing bias and social perception index were not significant and neither were the effect sizes (
Assessment of Neurocognition Across the Groups
Nonsocial cognition was tested for the overall composite score as well as the seven subdomains. There was a significant difference in intelligence. With regard to the speed of processing (covering subtests of brief assessment of cognition in schizophrenia, trail making test, and fluency) across all three groups, there was a significant difference in speed of processing and attention, which had a statistically significant difference and a medium effect size. For the domain of working memory (comprising of Weschler Memory Scale and Letter Number Span), there was a significant difference in working memory, with a medium effect size observed. A significant difference was observed in verbal learning and visual learning, as well. There was also a significant difference in problem-solving and reasoning. With respect to the last domain of social cognition, there was statistically significant difference observed across three groups. Both problem-solving and social cognition had medium effect size (
Analysis of total scores of MATRICS and their subdomains amongst BPAD patients and their FDR revealed a significant difference in overall neurocognition performance, but the effect size was small. On the other hand, there was a lack of significant difference in the scores amongst the FDR and healthy controls, and the lack of good effect size adds further to the finding. A medium effect size was observed between the performance of BPAD patients and FDR on the subdomains of the speed of processing and problem-solving, whereas there was no significant effect size observed for any of the subdomains on comparison of FDR and healthy controls.
Discussion
Social Cognition
Analysis of the overall data obtained for social cognition revealed that there was a statistically significant difference in performance across patients with BPAD, their FDR, and healthy controls. The difference in scores of the first-order TOM and social perception were significant at the 0.05 level, while the second-order TOM and faux pas were significant at the 0.01 level. No statistically significant difference was observed in attribution. Though the deficits were pronounced even in basic mentalization and emotion decoding, they remained as subtle impairments. This could indicate that TOM (inclusive of first order and second order) and social perception are definitive trait markers in the context of BPAD.
According to Gottesman and Gould (2003), for a construct to be called an endophenotype, the trait marker has to be associated and heritable with the disorder and should be demonstrable in asymptomatic patients. Furthermore, the variable that is being considered as a potential trait marker should be present in the unaffected family members also, in a milder form. 11 This study’s findings are concurrent with those of previous studies, wherein deficits in social cognition have already been consistently established in symptomatic patients across different episodes. 17 The analysis revealed statistical significance at the 0.01 level with regard to BPAD group and FDR indicating that there was a significant difference in impairment between the groups. On the other hand, there was no significant difference in performance in social cognition between FDR and healthy controls. If social cognition deficits were a premorbid marker for BPAD, there would be significant impairments in asymptomatic FDR. Hence, this domain is questionable as a vulnerability marker for developing the illness.
Our results indicate no significant difference in performance on social cognition tasks between healthy controls and unaffected probands, which is supported by the mixed findings of existing literature, wherein a few studies reported that there was no deficit in social cognition in FDR.6, 18 A meta-analysis conducted by Bora in 2017, assessing social cognition domains of TOM and affect perception, revealed that most of the studies reported no impairments in FDR of patients with BPAD. A few studies had a small effect size of 0.25 for TOM deficits in FDR. The authors concluded that emotion processing and social perception might not be trait markers for BPAD, as there were nil effect sizes for these domains across studies. 19 No definite conclusions can be made about attribution styles as it has not been studied in FDR. TOM could be a potential endophenotype. The non-significant results of the current study could be a result of the small sample size. In addition to the above-stated reasons, most of the FDR who were recruited for the study belonged to a better education status when compared to the patient group. This could have acted as a confounding variable in detecting deficits as even though there might be a genetic vulnerability, the manifestation occurs in the context of the environment as well. Owing to such limitations of this study, the effects may have been harder to identify.
Furthermore, though the SOCRATIS tool was developed primarily for patients with schizophrenia, in recent times, it has been proven to be effective in identifying deficits in BPAD patients, with small effect size. 16 Having identified that FDR of BPAD patients have less pronounced sociocognitive deficits than the patients, it is possible that the tool is not sensitive to subtle impairments.
Neurocognition
The neurocognition domains are represented by a composite intelligence score as well as the subdomains of the speed of processing, attention, working memory, verbal and visual learning, social cognition, and problem-solving. Comparing the mean scores of all these subdomains across patients, FDR, and healthy controls yielded a significant difference amongst the three groups. These findings are in concordance with literature that states that there is persistent cognitive impairment in the domains of attention, memory, and executive functions in BPAD patients in the euthymic state. 20 Executive functions, memory, and tasks involving mental flexibility and psychomotor speed are specifically affected in patients with BPAD, 11 which is in concurrence with our finding that speed of processing and problem-solving are two domains that have yielded medium effect size in performance amongst patients and FDR.
The difference in the performance of patients versus their FDR was significant at the 0.01 level, which is consistent with the existing literature. The FDR-healthy controls comparison, though devoid of statistically significant difference, does differ in the magnitude of mean scores reported. We found no significant impairment in the domains of attention/vigilance, problem-solving, speed of processing, and social cognition, which is in concordance with the current literature and meta-analytic reports. 21
The lack of difference in neurocognitive test scores between patients with BPAD and FDR is opposite to the findings of another meta-analytic study where there were significant deficits in the domains of processing speed, working memory, and executive functioning. 22 The contradictory findings may be attributed to the limitations discussed later in the article. Furthermore, it has been argued that the verbal learning task, with just 12 words to remember, is simpler than other tests like California Verbal Learning Test, and hence, not sensitive to subtle impairments. 23 Our problem-solving tasks included Letter Number Span and NAB-Mazes, which have been criticized for not being an adequate representation of the higher-order cognitive processes of problem-solving. 23 With all the given reasons, an objective lack of difference in performance between FDR and healthy controls could point to the fact that cognitive deficits may not be a vulnerability marker with regard to BPAD and are possibly subject to the influence of the development of the disorder itself.
Limitations
The sample size was small, and we were not able to meet the estimated sample size of 90. The sample was recruited from a limited geographical location, prohibiting any generalizability of the results. The patients continued psychotropic medications, whose details were not collected, and the effects were not accounted for. The participants were not matched on educational qualifications, as it was difficult to obtain the sample size meeting the existing criteria itself, and this would have served as a confounding factor in assessing cognition. Other disorder-specific factors such as the total number of episodes, length of each episode, and duration between each episode and their correlation to the scores obtained could have given further insights into the pattern of the deficits. The correction for multiple comparisons to reduce the risk of Type-1 error was not used. The tools used for measuring social and neurocognition do not provide an exact measure of the underlying phenomenology of the variables, due to which the deficits may not have been completely identified.
Conclusion
The study has identified persistent deficits in social and neurocognition despite remission, having significant clinical implications in terms of developing remediation programs for social cognition and planning early interventions for patients who may develop cognitive deficits associated with BPAD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.