
Abstract
Background:
This study aimed to evaluate the clinical profile of adolescents aged up to 19 years who had received electroconvulsive therapy (ECT).
Methods:
A retrospective chart review was carried out to identify adolescents aged up to 19 years who had received ECT during the period 2012–2018. Details regarding their sociodemographic and clinical variables and ECT data were extracted from the records.
Results:
During the study period, a total of 51 adolescents received ECT, and complete records of 50 patients were available for analysis. 4.04% (51 out of 1260) of the patients who received ECT were aged up to 19 years. There was a decreasing trend of use of ECT over the years. The most common diagnosis was schizophrenia (42%), and this was followed by bipolar disorder (22%) and unipolar depression (20%). The mean number of ECTs administered per patient was 8.84 (SD: 5.34; range: 1–21). On the various rating scales, the percentage improvement in patients with psychotic disorders was 77.4%. For patients with depression, the percentage improvement was 77.2%, and that for mania was 80.3%. The percentage improvement in organic catatonia was 64.6%. The number of patients achieving ≥50% response ranged from 87.5% to 100%, and when the response was defined as ≥75% improvement, the proportion of patients varied from 50% to 76.9%. The majority of patients with depression (72.7%) and mania (77.8%) achieved remission. Immediate complications associated with the use of ECT included acute blood pressure changes (18%).
Conclusion: ECT is effective and safe in adolescents with severe mental disorders. The clinician should not hesitate and delay the use of ECT in adolescents who require it.
Adolescents form 4.04% of the patients who receive ECT. The most common diagnosis among adolescents who receive ECT is schizophrenia (42%), and this was followed by bipolar disorder (22%) and unipolar depression (20%). In general patients with different disorders show 64.6% to 77.4% reduction in symptoms with ECT.Key Messages:
Although electroconvulsive therapy (ECT) is useful in managing various psychiatric disorders, its use in children and adolescents has always been controversial.1–3 The Mental Healthcare Act, 2017 (MHCA-2017) has laid some restrictions for the use of ECT for people less than 18 years. Further, MHCA-2017 states that if ECT has to be administered, it can be given after obtaining informed consent from the guardian of the minor and prior permission of the Mental Health Review Board. 4 Many authors have criticized this approach and stated that clinicians should have the liberty to use ECT in clinical conditions in which it is indicated. 5
ECT is usually given to a patient with catatonia when other treatments don’t work and to patients of severe depression, mania, or psychosis who are suicidal, refuse food, do not respond to adequate medication trials, or have marked agitation.1–3 In 2004, the American Academy of Child and Adolescent Psychiatry published practice parameters for the use of ECT in adolescents. 6
Available literature across the globe suggests that ECT is infrequently used in children and adolescents. In Western countries, children and adolescents receive 0.2%–1.5 % of all the ECTs.7–9 Data from Asia also suggests that 1.4%–6% of ECTs are administered to subjects younger than 18 years of age.2,10,11 The response rate to ECT in children and adolescents is usually good. A systematic review concluded that ECT is highly effective and is associated with high remission rates in adolescents for treating several psychiatric disorders, with a few, relatively benign, adverse effects. It was further suggested that the use of the correct technique could reduce the risks of side effects. Overall, the side effects are considered minimal compared to the effectiveness of ECT in treating various psychopathologies. 1
There is limited data on the use of ECT from India.2,3,12–14 Hence, there is a need to expand the literature to understand ECT’s effectiveness and safety in adolescents. In this background, the present study aimed to evaluate the clinical profile of adolescents aged up to 19 years who had received ECT.
Materials and Methods
Setting and ECT Protocol
This retrospective study was conducted at a tertiary care hospital in North India. The Ethics Committee of the Institute approved the study.
At this center, ECT is given thrice a week. ECT is usually given after obtaining the written informed consent of the patient. However, if the patient is a minor (≤ 18 years) or is not competent to consent, written informed consent is obtained from the family members. For adolescents, written informed consent is obtained from the family members, and additionally, written informed assent/consent is obtained from the patient if they are clinically in a position to provide the same.
Bitemporal, brief pulse, modified ECT is administered using an indigenous machine (Medicaid India Ltd, Chandigarh, India). The electrical dose is calibrated in terms of millicoulombs. The device has the provision of adjusting the duration of current passed (0.1–5 seconds with increments of 0.1 second), the frequency between 20 and 90 Hz (settings of 20, 40, 50, 60, 70, and 90 Hz), the pulse width from 0.1 to 1.5 seconds (0.1, 0.2, 0.5, 1, 1.2, and 1.5 seconds), and the charge to be delivered. The amount of charge to be delivered is determined by keeping the frequency and pulse width constant. Usually, the first stimulus is given with 48–72 millicoulombs, and depending on the response, the further charge is adjusted to determine the seizure threshold. Usually, a maximum of two stimuli are given during the initial session, to determine the seizure threshold. The electrical dose is adjusted in the subsequent sessions to compensate for the rise in seizure threshold and fall in seizure duration.
Prior to ECT, patients receive atropine (0.2–0.3 mg) or glycopyrrolate (0.2–0.3 mg) as a premedication and thiopental sodium (150–450 mg) is usually used for induction. In some cases, propofol (50–200 mg) is also used for induction. Succinylcholine (30–60 mg) is used for muscle relaxation. The seizure duration is estimated by the cuff method, and a motoric seizure of at least 15 seconds is considered an indicator of therapeutic ECT. Before ECT, at least six hours fasting is ensured. After the ECT, vitals of the patients are monitored for 2 hours at least and longer if required.
Response to ECT is usually rated clinically and on one or more standardized scales. ECT is discontinued either when the patient achieves remission or when symptoms reach a plateau of improvement for two consecutive treatments. ECT is also discontinued if the patient does not show any response to the first 4–6 treatments or develops significant complications (e.g., delirium and switch of polarity) during ECT. All the treatment details are documented in the patient’s case notes and the ECT register, by the psychiatrist administering ECT.
ECT register has the provision for recording the demographic and clinical variables and ECT details, including reasons for using ECT, types of symptoms ECT is considered for, and reasons for stopping ECT.
For this study, the ECT register of the department was screened for the period January 1, 2012, to December 31, 2018. For inclusion into the study, a person was required to have received ECT at the age of ≤ 19 years. No exclusion criteria other than the age cut-off was used. Treatment records of such patients identified from the ECT register were reviewed, and the relevant data was extracted. Additionally, the data was extracted from the ECT register. At our center, all the diagnoses are made as per the International Classification of Diseases, Tenth Revision (ICD-10). All the patients who receive ECT are usually rated on standard rating scales by the trainee resident, under the supervision of a senior resident. The ratings are reviewed weekly by the consultant incharge of the case.
During the study period, a total of 51 patients aged ≤19 years received ECT. Complete records were available for 50 patients. These case notes were taken up for the study, and details of sociodemographic, clinical, and ECT data were extracted for analysis. Information on the rating scales was also extracted, to understand the effectiveness of ECT.
Data were analyzed by using Statistical Package for the Social Sciences, version-14 (SPSS-14). Mean and standard deviation were computed for the continuous variables, and frequency and percentages were calculated for the categorical variables.
Results
During the study period, 1260 patients received ECT, of whom 4.04% were aged up to 19 years. If one looks at the yearly distribution of the number of patients who received ECT, the proportion of adolescents came down from 9.6% in 2012 to only 1.8% in 2018 (Table 1).
Total Number of Patients Receiving ECT and Proportion of Children and Adolescents
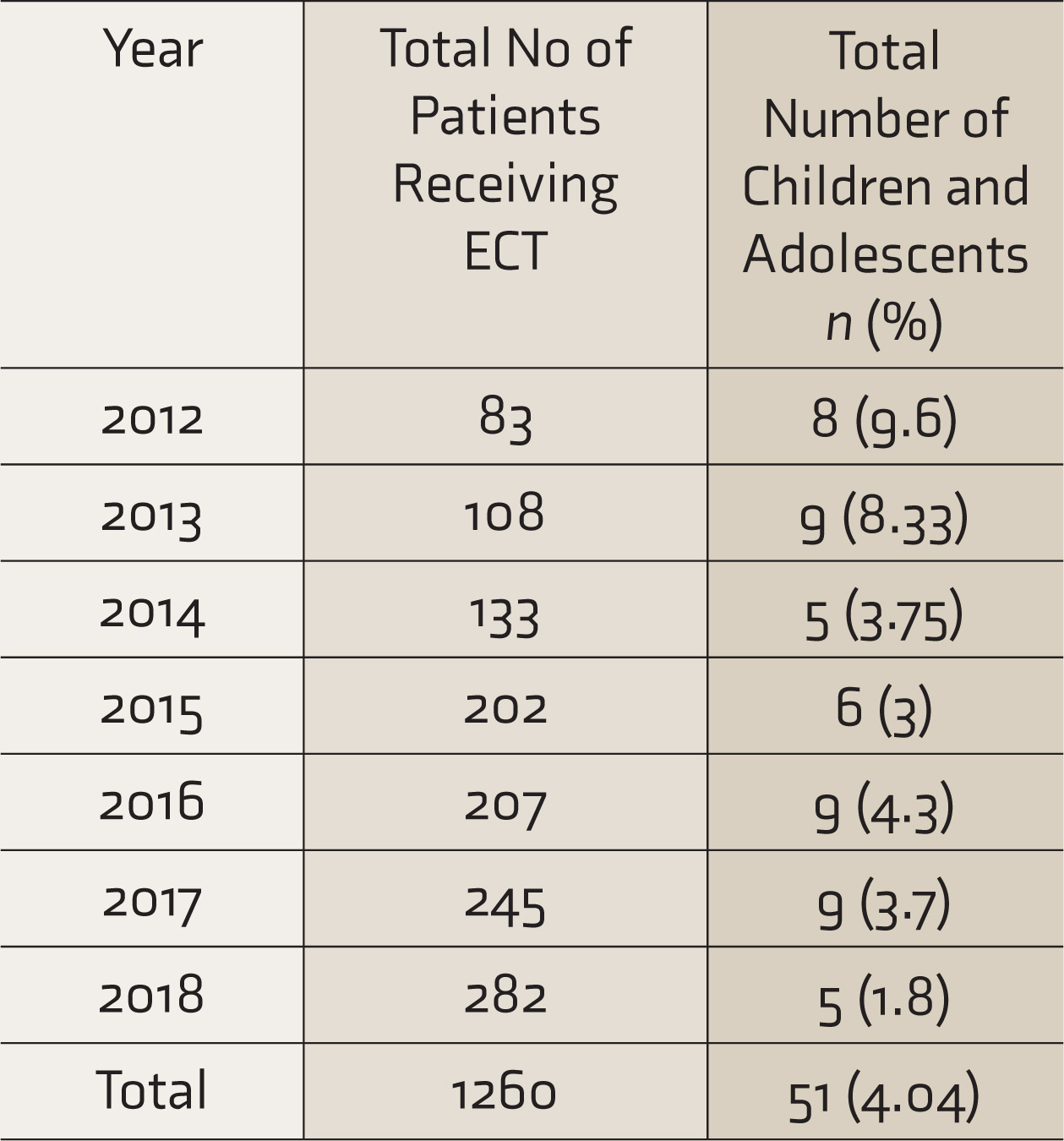
ECT: electroconvulsive therapy.
The mean (SD) age of the study sample was 17.84 (1.20), with a range of 14–19 years. A total of 18 (36%) patients were aged 19 years, 16 (32%) were aged 18 years, 9 (18%) were aged 17 years, and 5 (10%) were aged 16 years. Only one patient was aged 15 years, and another patient was aged 14 years. All of the patients who received ECT in the year 2018 were aged 19 years. For the year 2017, 2 patients were aged 17 years, three were aged 18 years, and 4 were aged 19 years. No patient aged ≤17 years was given ECT after May 2017.
The majority of the patients were male (68%, n = 34), from middle socioeconomic status (66%, n = 33), and Hindu (60%, n = 30) by religion. The mean duration of the education of the participants was 10.1 (SD: 3.24) years. The majority of the patients received ECT as an inpatient (60%, n = 30).
The clinical profile of the study sample is shown in Table 2.
Clinical Profile
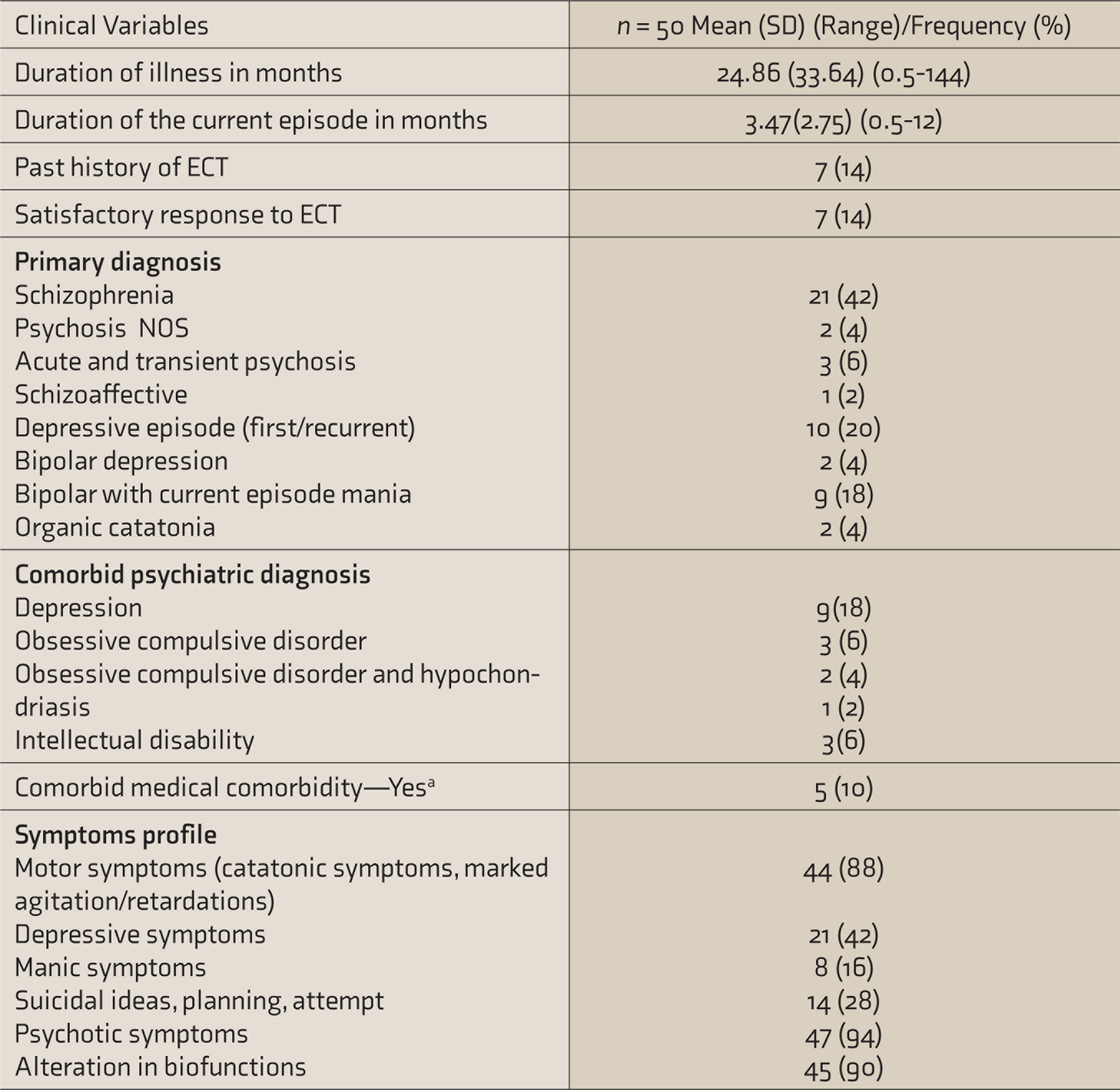
ECT: electroconvulsive therapy.aComorbid medical illnesses: celiac disease (N = 1), hypothyroidism (N = 1), type 1 diabetes mellitus (N = 1), tinea cruris (N = 1), malnutrition (N = 1).
ECT Details
The ECT details are provided in Table 3. Less than half (n = 20) of the patients had received more than eight ECTs and one patient had received maintenance ECT.
In 3 (6%) patients, complications led to the stoppage of ECT. For one of these patients, the reason was delayed recovery, attributed to low pseudocholinesterase levels. For one patient, the reason was delirium, and for the third patient, the reason was cognitive deficits that led to the withdrawal of consent (Table 4).
An overall clinical improvement of >50%, as judged by the treating clinician, was noted for 86% (n = 43) of patients. Information on various rating scales was available for 42 patients, with four patients rated on more than one scale (Table 4). On Hamilton Depression Rating Scale (HDRS) and Young Mania Rating Scale (YMRS), 72.7% and 77.8% achieved remission. In the Bush Francis Catatonia Rating Scale (BFCRS), the percentage improvement in psychopathology was 78.85 (SD: 24.8)%. On Positive and Negative Symptom Scale (PANSS), the percentage improvement was 50.61 (SD:8.7)%, when the ratings of PANSS were considered in the form of 1–7. However, when the rating was adjusted to 0–6, the percentage improvement increased to 74.66 (SD: 11.4)%. On the Brief Psychiatric Rating Scale, the mean percentage improvement in the rating scale was 68.01 (SD: 22.1)%.
When the improvement was evaluated in terms of diagnosis (if the patient was rated on more than one scale, the lower percentage of improvement was considered; for PANSS, 0–6 rating was considered), for patients with psychotic disorders, the mean percentage improvement in severity of symptoms was 77.4 (SD: 16.2)%; for patients with depression, the mean percentage improvement was 77.2 (SD: 20.5%)%; and that for mania was 80.3 (SD: 17.1%)%. The mean percentage improvement in organic catatonia was 64.6 (SD: 14.3)%. In terms of response (defined as ≥50% reduction in psychopathology), the number of patients varied from 87.5% to 100%, depending on the diagnosis (Table 5). In terms of clinical remission for depression and mania (defined as HDRS and YMRS score of ≤ 7), 72.7% and 77.8% of the patients, respectively, achieved remission (Table 5). When the response was considered as ≥75% reduction in psychopathology, the proportion of patients varied from 50% to 76.9% (Table 5).
Discussion
There is limited data on the use of ECT in adolescents, especially from India. The present study was an attempt to expand the literature. We found that only 4.04% of patients who receive ECT are aged ≤ 19 years. When one compares this data with the existing literature, it is evident that this figure is in the range of 1.4–6% reported for subjects <18 years of age.2,10,11 However, one important thing to note is that in the present study, 36% of patients were actually aged 19 years. If this is taken into account, it can be said that the proportion of patients in the present study is close to the lower end of the reported range in the existing literature. However, when one looks at the proportion of patients receiving ECT, it is evident that the proportion of patients has reduced significantly from 9.6% in 2012 to only 1.8% in 2018. Further, a closer look at the data suggests that the reduction in the proportion has been mainly from the year 2014, and in the year 2018, it reduced further. Moreover, if one takes the patient’s age into account, it is evident that none of the patients aged ≤17 received ECT after May 2017. These changes in practice could be due to MHCA-2017, which emphasizes restrictions in ECT for children and adolescents.
ECT Details of the Study Sample
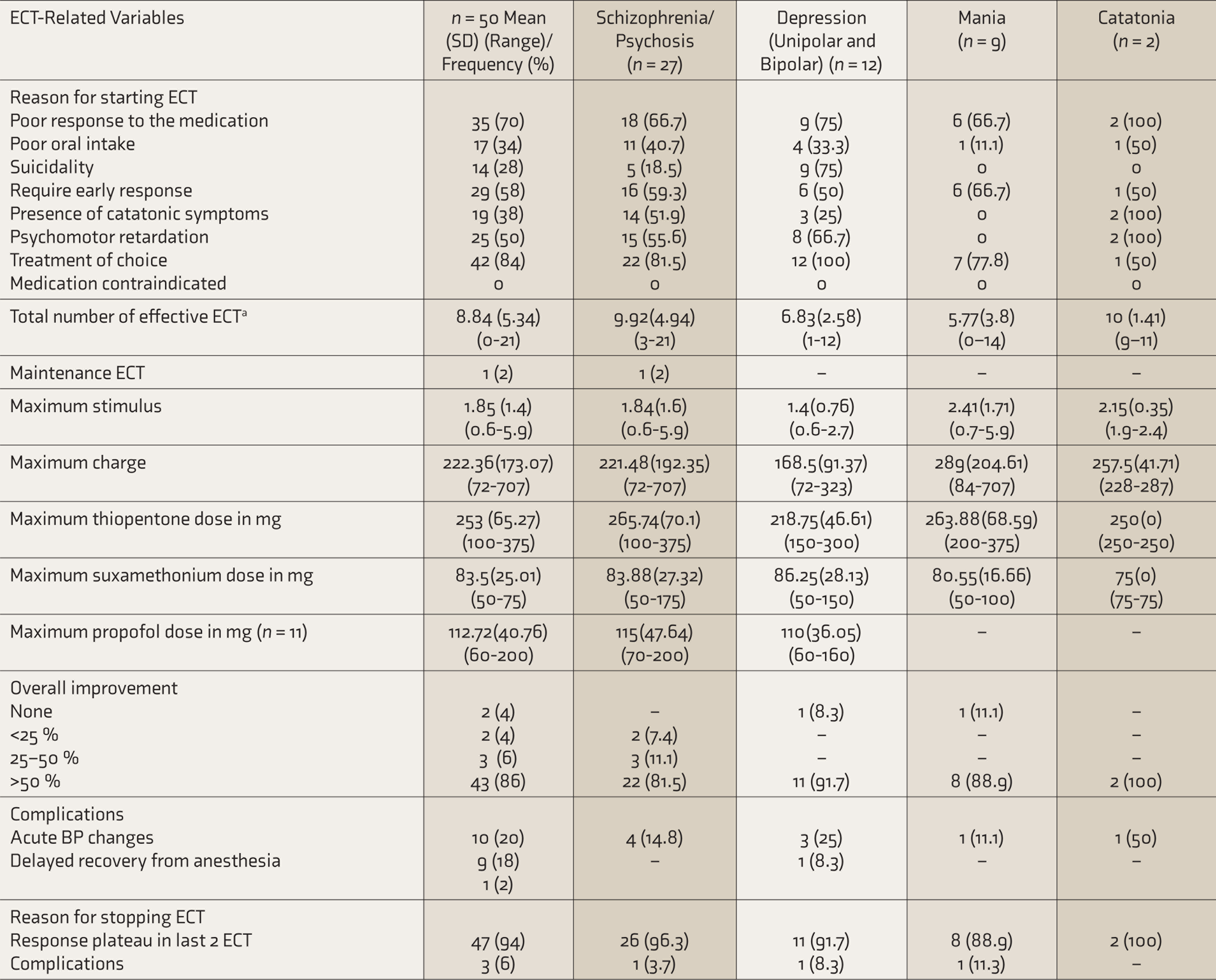
ECT: electroconvulsive therapy. a Effective ECT: A motoric seizure of at least 15 seconds.
In this study, the most common diagnostic indicator for the use of ECT was schizophrenia, followed by depressive disorder and mania. Overall, 54% of patients who received ECT had a psychotic illness. A previous study from our center on the use of ECT in children and adolescents reported that schizophrenia/psychotic disorders form the biggest diagnostic category, followed by depressive disorders. 2 Our finding is also supported by the available surveys from India and developing countries, which suggest that schizophrenia is the most common indication for ECT.10,15 However, data from the West suggests that depression is the most common indication for ECT in children and adolescents.1,5,6,15–19 These differences may be due to the variations in clinical practice. This becomes evident when one evaluates the reasons we found for giving ECT, with ECT considered as a treatment of choice for the diagnosis in 84% of cases, inadequate response to medications in 70% of cases, and need for early response in 58% of cases. Since in adolescents mostly the parents or primary caretakers make decisions regarding ECT, the aforementioned reasons are understandable in the background of financial constraints and the impact of illness on the family functioning and family wages.
The mean numbers of ECTs administered per patient in this study were 8.84 (SD: 5.34), with a range of 1–21. When we compare these findings with the previous studies from India, which have reported a mean of 10.1 (SD: 4.87) ECTs per patient during the ECT course, the results of this are comparable. 2
A systematic review of the literature concluded that ECT use in adolescents is a highly efficient option, associated with high remission rates, for treating several psychiatric disorders. 1 In this study, ≥50% of clinical improvement was noted in 86% of patients. The mean improvement on rating scales in terms of severity of symptoms varied from 68.01% to 81.1% in different diagnostic groups; the mean percentage improvement in psychopathology ranged from 64.6% to 77.4%. The number of patients achieving ≥ 50% response varied from 87.5% to 100%. When the response was evaluated in terms of ≥75% response, the proportion of patients ranged from 50% to 76.9%. In patients with depression, 72.7% achieved remission, while 77.8% of patients with mania achieved remission. When one compares these overall response and remission rates with the existing literature from the West and India, findings of this study are comparable.1–3,6,7,16 Rates of improvement for depression is 63%, mania is 80%, schizophrenia is 42%, and catatonia is 80%. A 20-year practice review of ECT for adolescents showed that almost 77% were much or very much improved based on the Clinical Global Impressions–Improvement scale at the end of the acute treatment. 16 The findings of this study support the same.
Improvement in Symptoms as per the Rating Scales
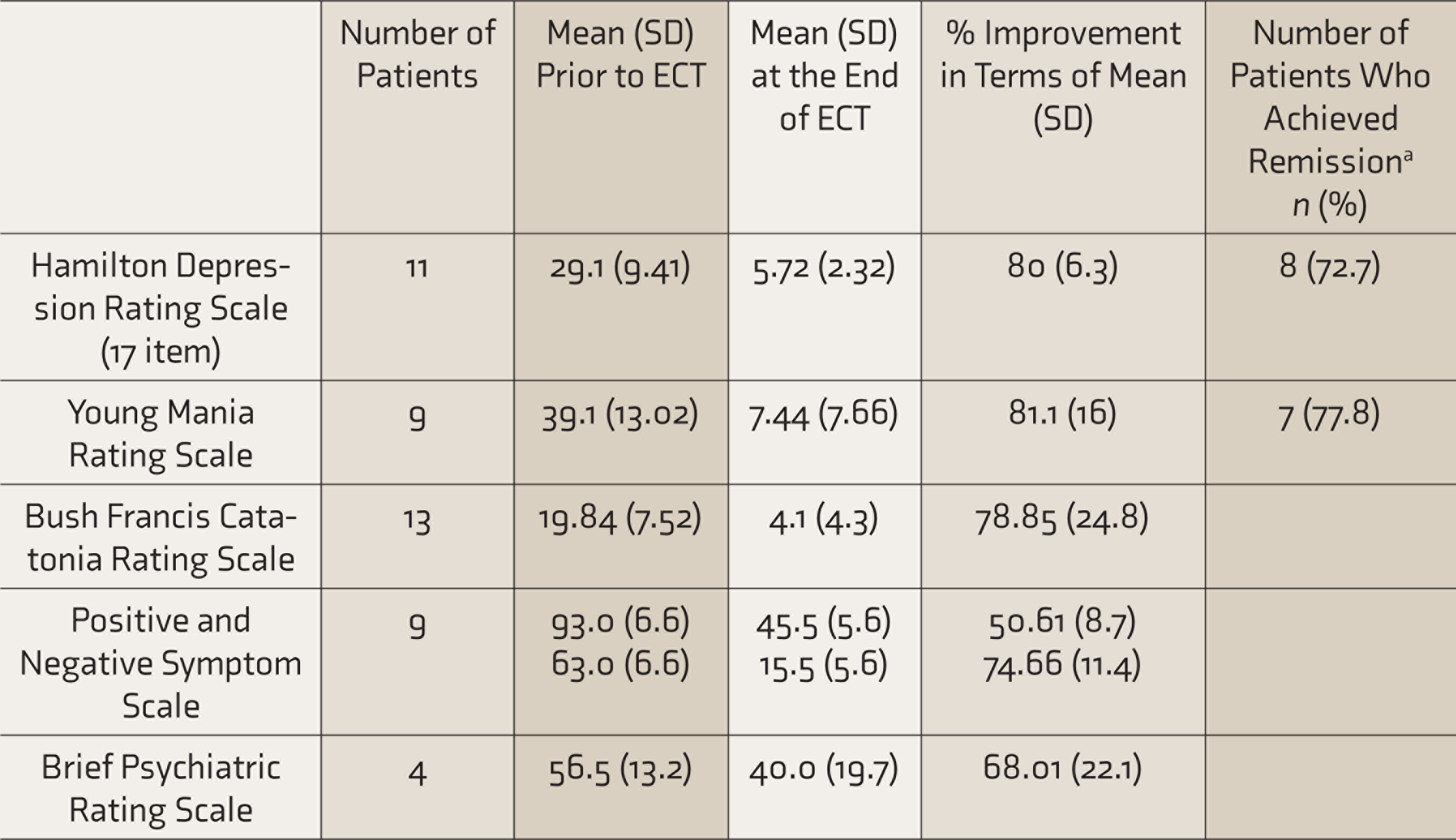
ECT: electroconvulsive therapy. aRemission on Hamilton Depression Rating Scale and Young Mania Rating Scale was defined as a score of ≤ 7.
Improvement as per the Diagnostic Categories
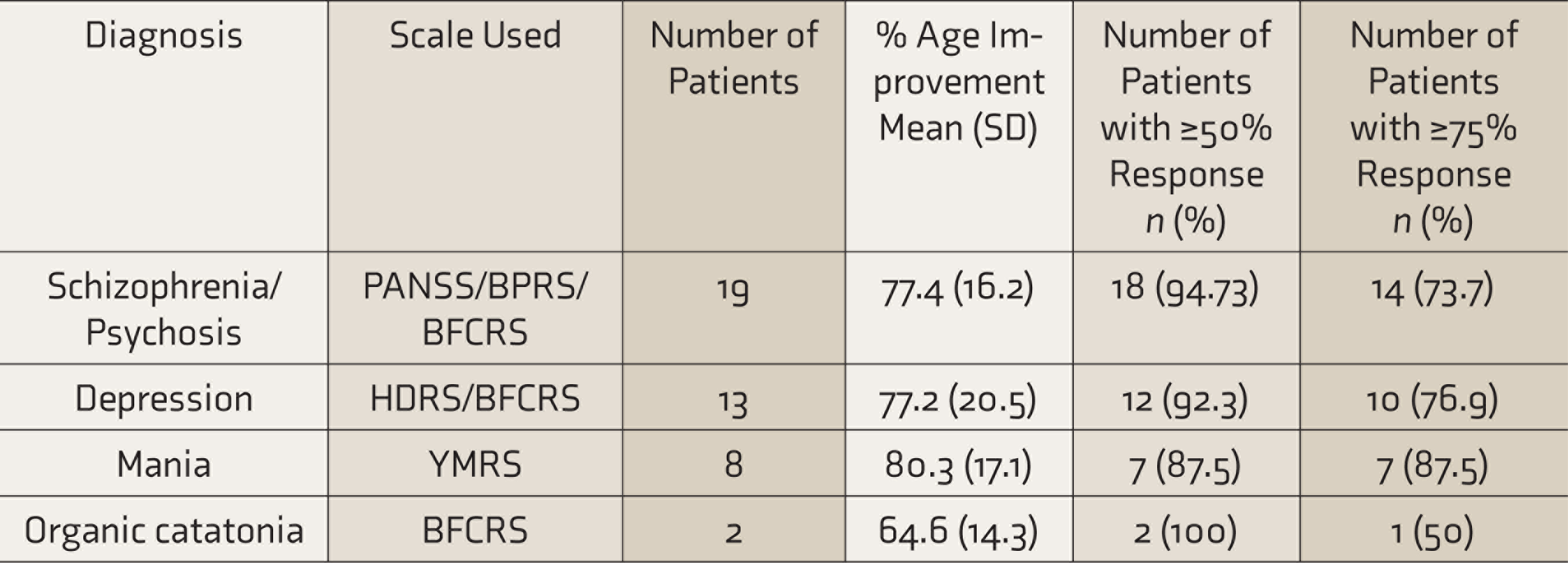
HDRS: Hamilton Depression Rating Scale, YMRS: Young Mania Rating Scale, BFCRS: Bush Francis Catatonia Rating Scale, PANSS: Positive and Negative Symptom Scale, BPRS: Brief Psychiatric Rating Scale.
In our study, 10 patients were reported to have side effects, out of which nine were acute changes in blood pressure during ECT administration, and one was delayed recovery from general anesthesia in a patient who had low cholinesterase levels. None of the patients in this study experienced prolonged seizures. These profiles of side effects are slightly different from those reported in the literature, which suggests headache, nausea and vomiting, and cognitive deficits as the common side effects associated with ECT.1–3,5,15 These differences could be attributed to methodological differences.
This study supports the notion that ECT is useful in adolescents with severe mental disorders and is effective in a large proportion of cases. Further, this study suggests that adolescents form a small percentage of patients receiving ECT. It can be said that there is a need to change the recommendation of MHCA-2017, and the clinicians should be allowed to decide about starting ECT timely without having to go through the review board, which can lead to delay in the beginning of the treatment.
This study should be interpreted in light of its limitations, which include the retrospective study design and small sample size. Further, the study did not include a comparison group. The side effects were not recorded systematically, and some of the side effects could have been missed or underestimated. While receiving ECT, some patients also undergo a change of medications, and hence, all the improvement seen may not be attributed to ECT alone. Future studies must attempt to overcome these limitations.
To conclude, this study suggests that ECT is safe and effective in adolescents with severe mental disorders. Accordingly, clinicians should not abandon the use of ECT in adolescents where it is required. If an indication for ECT exists, clinicians should follow the MHCA-2017 and give ECT to adolescents to improve the overall outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.