
Abstract
Background:
Anorexia nervosa is one of the least studied mental health conditions in the Indian setting. The objective of this study was to assess the course and outcome of anorexia nervosa in adolescents who had presented to a tertiary care child and adolescent psychiatry center over a period of 10 years.
Methods:
The present study is a retrospective chart review of adolescents (up to the age of 18 years) with a diagnosis of anorexia nervosa, coded as F50.0 or F50.1 according to ICD 10, from 1st April 2009 to 31st March 2019. Data were extracted from the case records using standardized abstraction forms and evaluated using descriptive and nonparametric statistics.
Results:
The average age at presentation and the average age at onset were 14.1 years and 13.1 years, respectively. The male-to-female ratio of the sample who got admitted was 1:9. The average duration of hospital stay was about 30 days. The duration of in-patient care and weight gain were positively correlated, with severe to extremely ill adolescents improving even in less than one month of in-patient care. Seventy per cent of the admitted adolescents followed up. The functional outcome as measured by a ‘return to school’ improved in 57.1% of the sample.
Conclusions:
The present study highlights the collaborative multidisciplinary and individualized treatment approach employed for adolescents diagnosed with anorexia nervosa within an inpatient mental health facility in India. Adolescents who presented with more severe illness at the initial assessment, such as an early onset of symptoms and a low BMI, experienced substantial weight gain that exhibited a positive correlation with the length of their stay in the inpatient facility.
Anorexia nervosa in adolescents may have a favorable clinical and functional response when an individualized and multidisciplinary approach is followed in a tertiary care setting. However, it’s important to note that causal attribution is not possible due to the retrospective nature of the study. Duration of inpatient care can determine clinical outcome. The longer the duration, the better the weight gain. The review reflects the need for prospective studies using standard outcome variables to assess the course of anorexia nervosa in adolescents in the Indian context.Key Messages
Anorexia nervosa is a psychiatric condition that usually has an onset in adolescence. 1 Literature suggests a steady rise in its incidence the world over since the 1930s, 2 and even in India in recent times. 3 While some diagnosed with it achieve complete recovery, others may experience a chronic course. The natural course and outcome of the illness are poorly understood due to the inherently complex nature of the condition and the paucity of long-term follow-up studies. 4 However, a review of 119 study series covering 5,590 patients with anorexia nervosa reported a 46% recovery, about 33% partial remission, and 20% chronicity. 5 The clinical variable that best predicted complete remission was the duration of untreated illness, reflecting the importance of early detection and intervention. 6
Despite the need for research in this area, anorexia nervosa has been one of the least studied mental health conditions in the Indian setting. A scoping review of literature focusing on Indian research in eating disorders suggests majority of the available literature are case reports and case series and few hospital-based studies. This could be due to the fact of the low prevalence of anorexia nervosa coupled with a lack of awareness of the condition among the general population and most importantly health care professionals. There have been some cultural variations in presentation which could underestimate actual prevalence leading to less research focus. 7 A review of hospital records by Prasad et al. (2021) focusing on adolescents diagnosed with anorexia nervosa/other specified eating and feeding disorder (OSFED) over a 13-year eight months period and reported a favorable outcome in 78.5% of the 15 adolescents who were followed up for a minimum duration of one year at a tertiary care center in India. 8 In a retrospective chart review of adolescents diagnosed as having any eating disorder, Preethi et al., reported that nine out of the twelve adolescents received a diagnosis of anorexia nervosa and one adolescent was diagnosed with atypical anorexia nervosa. The outcome of the eating disorder was not known in eight subjects (66.7%). All four subjects who followed up no longer fulfilled the criteria for anorexia nervosa. 9
Although there are guidelines for parents by the Indian Academy of Paediatrics (IAP), 10 there are no national guidelines for clinicians on the management of anorexia nervosa in adolescents and adolescents or any specialist national center exclusively for the treatment of anorexia nervosa in India. In this context, there is a need to understand the clinical course of the condition particularly the treatment protocol followed and the overall prognosis in the Indian context. Therefore, we reviewed the case records of all the adolescents diagnosed with anorexia nervosa over a period of 10 years from a tertiary care national mental health center located in the southern part of India with the objective of studying the clinical profile, course and outcome of childhood anorexia nervosa. The sociodemographic, clinical, and treatment profiles were discussed in detail in a separate article. 3 In the present article, we briefly outline the clinical profile and discuss the course and outcome of these adolescents and adolescents during their inpatient care and subsequent follow-up periods.
Material and Methods
Operational Definitions
Course
The clinical course is measured by the clinical global impression scale severity [CGI-S] and clinical global impression scale improvement [CGI-I] scores, which were calculated based on the case records by the authors [LS, AP] independently using the recorded baseline severity assessment and condition at the time of discharge and during the follow-up period respectively. The raters were qualified psychiatrists with substantial experience in using CGI scales, collecting and analyzing clinical data. Scaled score conversion is a valid outcome measure and an acceptable practice. The CGI has been used to retrospectively rate patient improvement in chart reviews.11,12
Outcome
The ‘mean weight gain’ during the inpatient care and follow-up was used as an indicator of clinical outcome and ‘return to school’ was used as a criterion to assess the functional outcome. We categorized the mean weight gain of the sample based on the level of improvement assessed by the CGI-I score at discharge into three broad categories for the purpose of analysis and interpretation. Weight gain of less than 3 kg, between 3 and 5 kg and more than 5 kg was considered as less gain, a moderate gain and high gain respectively for the purpose of evaluating and tracking the clinical progress during the inpatient stay.
It is noteworthy that the mean weight gain of the entire sample was 5 kg and the sample was categorized based on the mean weight gain taking 5 kg as a cut-off. This arbitrary division was done based on statistical analysis and was agreed by all the authors based on their clinical experience as weight gain reflected the clinical progress observed. The decision on ‘return to school’ was a collaborative decision made by involving the parent, child and the clinician in charge. It was guided by the following parameters—child’s stable physical health, positive progress on weight trajectory and eating patterns, and child’s readiness to go to school. Clinicians also supported the family by working in liaison with the school to provide additional assistance to ensure a smooth return to school.
Study Design
The present study utilized a retrospective chart review design. Data were derived from case records of patients with a diagnosis of anorexia nervosa, coded as F50.0 or F50.1 according to the International Statistical Classification of Disorders (ICD-10) over a 10-year period (from 1st April 2009 to 31st March 2019). The center follows a standard operating procedure for providing individualized and multidisciplinary in-patient care, the details of which have been described in the previously published article by the same team. 3 The multidisciplinary team consists of consultant child and adolescent psychiatrists and residents, clinical psychologists, family therapists, psychiatric social workers, trained mental health staff nurse, and a dietician. Standardized data abstraction forms developed for the purpose of this study were used to extract the data. The case records had information on areas related to socio-demographic data, psychosocial profile, clinical presentation, and treatment details including follow-up care.
Model of Medical Care & Service Delivery
The inpatient center provides a model of care where the child is admitted along with parents for comprehensive management which aligns with the common practice of the healthcare delivery model in India. It is a well-known fact that patients with anorexia nervosa have significant medical complications. Adolescents who were diagnosed with any of the eating disorders including anorexia nervosa were referred for a baseline pediatric assessment to a tertiary care pediatric center. Only adolescents with a stable cardiac and general physical health profile were admitted to our center for mental health interventions. Every patient admitted was monitored for any fluctuation in their general physical health and blood parameters.
Statistical Analysis
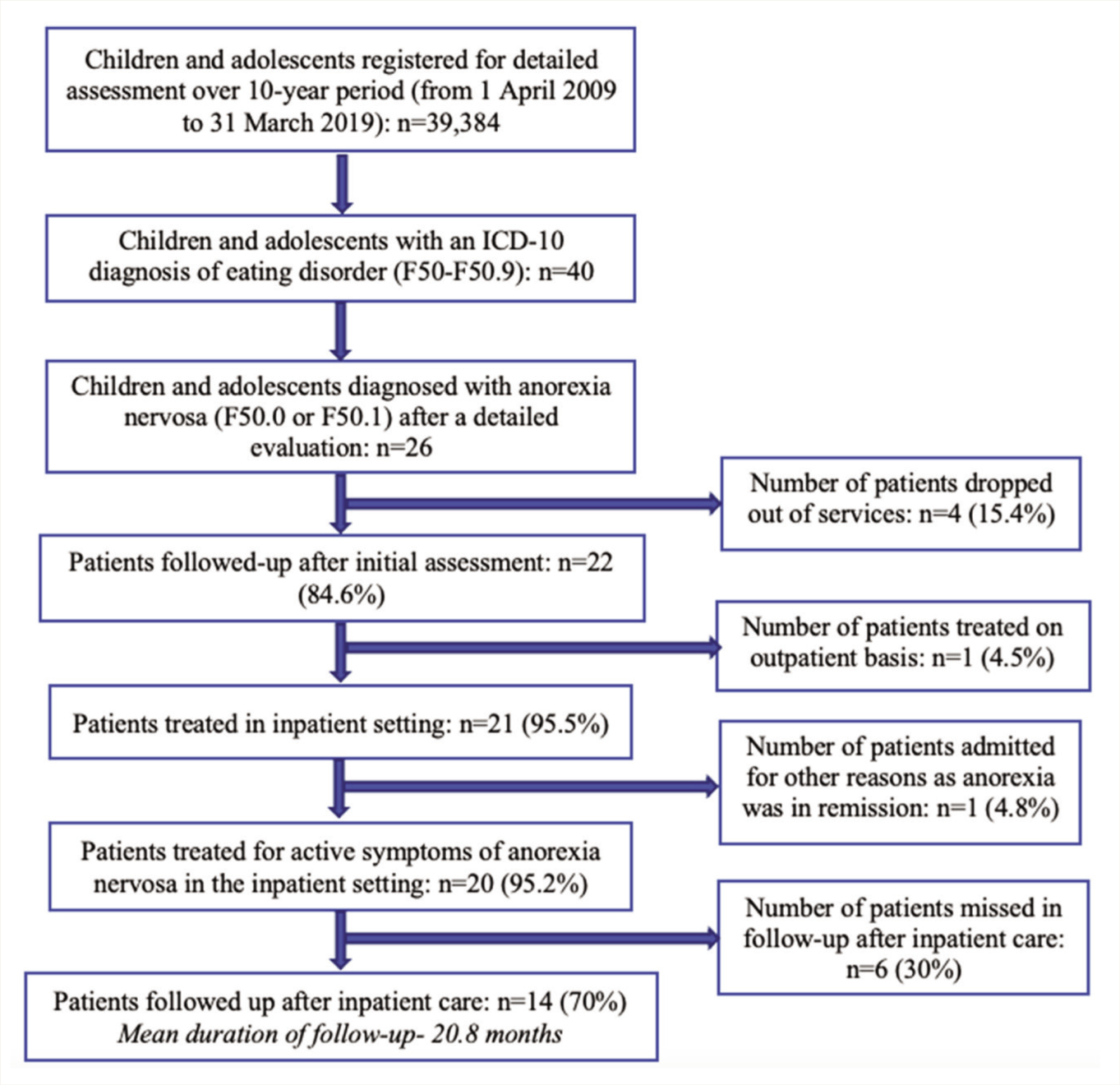
Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 21.0 for Windows using descriptive statistics. Nonparametric statistical tests (Wilcoxon signed-rank test and Spearman’s rank correlation coefficient) were used to study the association and correlation between the duration of in-patient care and weight gain. Figure 1 depicts the process of chart selection.
Process of Chart Selection.
Ethical Considerations
Institute’s ethics committee approval was obtained for conducting the study. Informed consent was exempted due to the type of the research (retrospective). The process of pseudo-anonymization ensured confidentiality.
Results
Of the 39,384 adolescents registered for clinical services during the 10-year period (1 April 2009 to 31 March 2019), 26 were diagnosed as having an ICD-10 diagnosis of anorexia nervosa. Over 80% (n = 21) of them received inpatient care and the common indications for admission were poor progress with ongoing treatment and a lack of comprehensive treatment services in the community setting across different parts of the country. Clinical and socio-demographic profile, treatment modalities followed and subsequent course and outcome of the illness for the adolescents who were treated in the inpatient setting (n = 20) and later followed up are discussed in the section below. Twenty adolescents were treated in the inpatient setting for active symptoms of anorexia nervosa, out of whom 30% (n = 6) did not follow up whose data were excluded from the analysis of follow-up and long-term outcome.
Sociodemographic and Psychosocial Profile
The majority of the adolescents (n = 15; 75%) were from an urban background and belonged to upper socio-economic status (n = 10; 50%). The majority were Hindus (n = 10, 50%) followed by Muslims (n = 5; 25%). Illness was triggered by a stressful event in 14 adolescents (70%). Eleven (55%) adolescents reported being bullied/body-shamed and six (30%) adolescents reported that the trigger was an academic stressor. Parenting style was authoritarian and permissive in 11 (55%) and 5 (25%) of the families, respectively. Interpersonal relationship issues were present in 7 (35%) and sibling rivalry was reported in 11 adolescents (55%). Enmeshed family dynamics were recorded in the charts of 13 (65%) adolescents.
Clinical and Treatment Profile
The average age at presentation and the average age at onset were 14.1 (±2.2) years and 13.1 (±2.0) years respectively. The male-to-female ratio of the sample (n = 20) who got admitted was 1:9 and that of the sample who followed up post-discharge (n = 14) was 1:13. The average duration of illness was 1.7 (± 0.8) years. The mode of onset was insidious in 13 (65%) adolescents and sub-acute in the rest. Baseline weight ranged from 20 kg to 46 kg [mean(SD) = 33.1(± 6.4) kg) and baseline BMI from 11.1 kg/m2 to 17.9 kg/m2 [mean (SD) = 14.2 (± 1.6) kg/m2]. Seven adolescents (35%) were noted to have an easy temperament and another seven (35%) had a difficult temperament. Fourteen (70%) adolescents had anankastic traits, eight (40%) were sensitive to criticism and another eight (40%) had high internalized self-expectations. Thirteen (65%) adolescents had one or more psychiatric comorbidities. The most common psychiatric comorbidity was major depressive disorder (n = 8; 40%), followed by obsessive-compulsive disorder (n = 4; 20%). Suicidal ideations were recorded in the charts of six (30%) adolescents.
Course in the Hospital
Except for one child (5%) who was admitted to the emergency medical ward and later shifted to the regular ward, the rest of the adolescents (n = 19; 95%) were admitted after an evaluation in the outpatient clinic to the regular ward. The duration of hospital admission ranged from 3 to 66 days, with an average duration of about 30 (±21.1) days. Regular weekly BMI and general physical health condition monitoring, and monitoring of feeding patterns and blood parameters were carried out by the psychiatrists and the ward nursing staff.
Pharmacotherapy
Most adolescents (95%) received pharmacotherapy (selective serotonin reuptake inhibitors, antipsychotics or both) and all received individual psychotherapy. A combination of SSRIs (Selective Serotonin Reuptake Inhibitors) and antipsychotics was instituted for eight adolescents (40%), SSRI monotherapy for nine (45%) and antipsychotic monotherapy for two (10%) adolescents. The major indications for starting SSRI included managing co-occurring depressive disorder, OCD and subsyndromal anxiety symptoms associated with problematic eating patterns in the study sample. A low dose of olanzapine was started for 50% (n-10) of adolescents as an adjunct to improve the eating pattern and weight trajectory. Ryle’s tube feeding was provided for three (15%) adolescents.
Parental Psychoeducation, Support and Family Therapy
Regular parental psychoeducation (two to five sessions/week) and group sessions (twice a week) were conducted to address the distress and burnout of caregivers by treating team members from the department of psychiatric social work. Parental education and support also involved daily meal plan, taking charge of the meal plan for the adolescents and monitoring the progress towards weight restoration. Parental psychoeducation about the impact of starvation in bodily systems, physiological effect of anorexia in bodily systems, significance of restoring to supervised meal plan with adolescents were discussed. In addition, about 50% (n = 10) of the families received structured family therapy sessions.
Individual Psychotherapy
All adolescents admitted received individual psychological support based on the Cognitive-Behavioral therapy approach. It was planned to deliver three sessions every week, and the sessions were planned considering the needs of individual child and their family based on the planned duration of stay in the ward. From the records we could observe the sessions were mostly eclectic focusing on emotional regulation skills, distress tolerance skills, individual psychoeducation and cognitive restructuring. Number of sessions ranged from 3 to 16 depending on the duration of stay and level of therapeutic engagement.
Medical Care
Three adolescents (15%) required naso-gastric feeding. One child (5%) had a fall and sustained a fibular fracture during the treatment process which was managed under the guidance of orthopedic team and later transferred to our center. Additionally, one child (5%) had anemia and three adolescents (15%) had nutritional deficiencies. They were referred on an outpatient basis to a pediatrician.
Clinical course, weight gain and CGI progress:
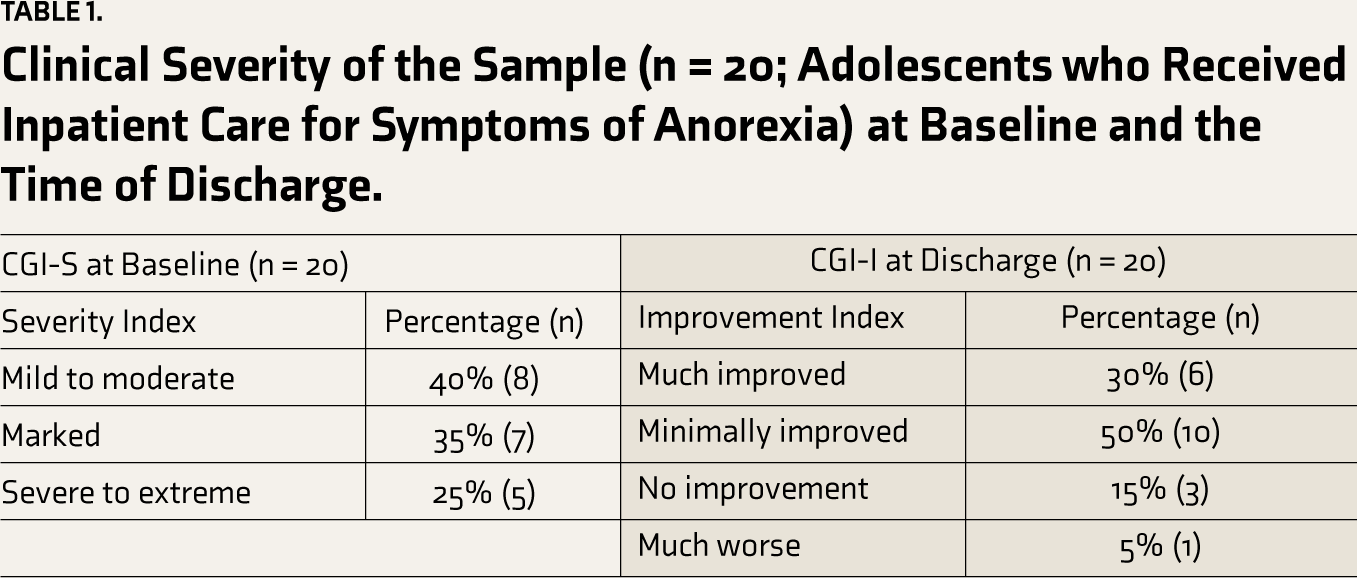
Table 1 illustrates the CGI-S and CGI-I scores at baseline and at the time of discharge respectively.
Clinical Severity of the Sample (n = 20; Adolescents who Received Inpatient Care for Symptoms of Anorexia) at Baseline and the Time of Discharge.
The weight gain was significant for adolescents who received in-patient care for more than one month (n = 9) when compared with adolescents who received for less than or equal to one month (n = 11) (Wilcoxon signed rank test; p = .008; Table 2).
Association Between Duration of In-patient Care and Weight Gain.
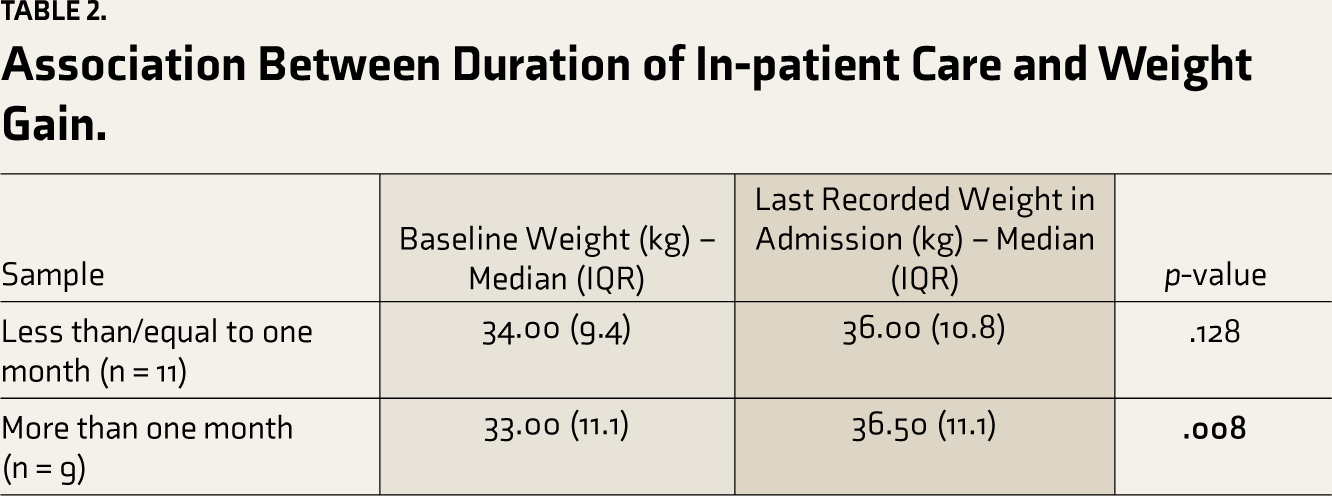
On studying the association between the duration of in-patient care and weight gain as an indicator of improvement, they were positively correlated (rs = 0.681, p = .004). It is worthwhile noting that the improvement was not correlated to the age of onset (the value of Spearman’s Rho correlation coefficient (ρ) or rs was 0.260; Sig. (2-tailed) – 0.298).
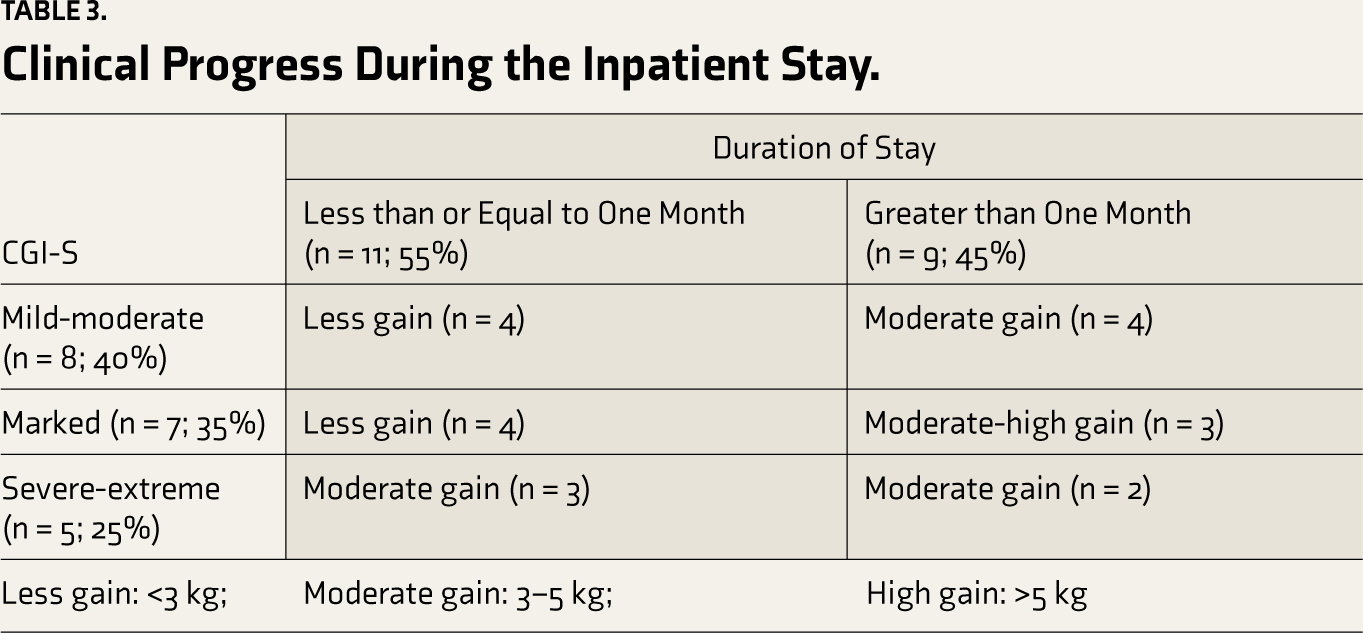
By categorizing the sample based on clinical severity at the time of admission using CGI-S and assessing progress in terms of weight gain noted during in-patient care, it was noted that severe to extremely ill patients had moderate weight gain even in less than a one-month whereas mild to moderately ill and markedly ill individuals gained above the mean weight after one-month timeline (Table 3).
Clinical Progress During the Inpatient Stay.
Outpatient Follow-up Care
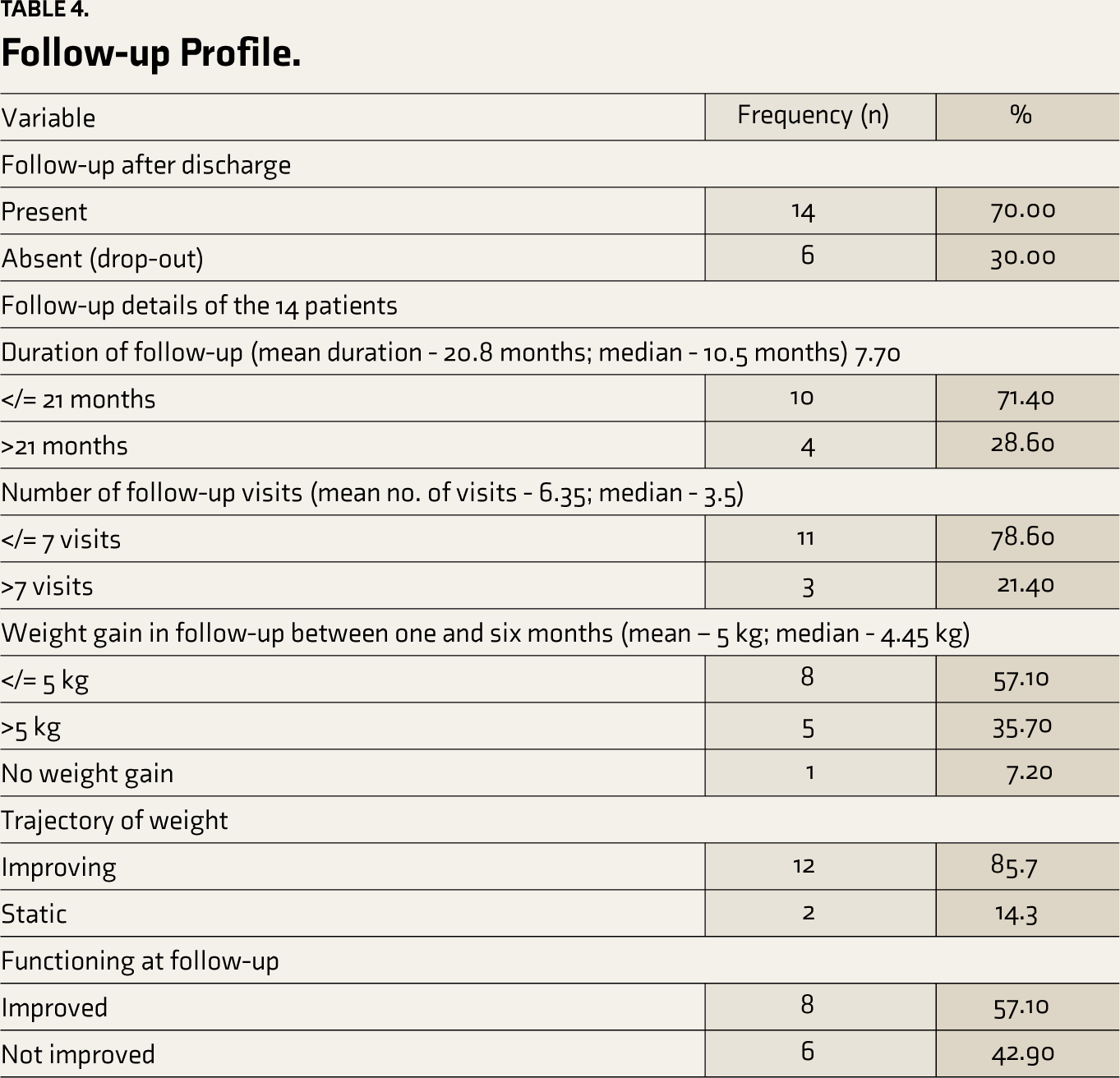
Mean duration of follow-up was 20.8 months (range of one month to 89 months). 25% (n = 5) required a re-admission in view of poor functioning or inadequate progress in treatment. Three (21.4%) out of the 14 adolescents who were followed up had a change in diagnosis during follow-up—one to eating disorder (NOS) (7.15%), one to bulimia nervosa (7.15%) and one to avoidant restrictive feeding disorder (7.15%). Overall, the clinical course and functional outcome were favorable in our sample as evident from the positive weight gain trajectory with 35.7% (n = 5) of the sample having a mean weight gain of more than 5 kg. Only one patient (7.2%) had a static trajectory with no weight gain observed during the follow-up. A positive functional outcome as measured by the indicator of ‘return to school’ was observed in 57.1% (n = 8) of the sample. The follow-up profile of the course variables studied is presented in Table 4.
Follow-up Profile.
Discussion
The sociodemographic and clinical characteristics including the temperamental, psychosocial and treatment profiles of the subset of the sample admitted (n = 20) are similar to that of the total sample (n = 26) discussed in our previous article that reported the baseline sociodemographic and clinical profile of the total sample of adolescents diagnosed with anorexia nervosa at baseline in detail. 3 The clinical profile of the sample suggested an early-onset illness, low baseline BMI, high level of comorbidities and presence of psychosocial stress. 3 The overall dropout rate of those who registered and were diagnosed as having active symptoms of anorexia nervosa (n = 25) was 40% (n = 10). Fourteen (70%) of adolescents admitted (n = 20) followed up regularly post-discharge. The mean duration of follow-up was 20.8 months. Other hospital record reviews from southern India reported that 41.8%–66.7% of patients were lost to follow-up.8,9 However, a literature review of western studies reported a mean dropout rate of 12.3% for 105 patient (adolescent and adult) series. 5 An in-depth analysis of the six (30%) admitted adolescents who were lost to follow-up in our study revealed that they hailed from a wide geographical distribution and the clinical team suggested the families follow up in regional mental health centers with a referral note and specific plan to ensure regular supervision.
The diagnosis of anorexia nervosa persisted in 78.6% (n = 11) of the patients who followed up. Diagnostic conversion is a common phenomenon, especially among the group of eating disorders. 13 Milos et al. (2005) carried out a prospective study of individuals with an eating disorder for 30 months. They reported diagnostic stability of 56% at 12 months and 49% at 30 months in 55 individuals with an initial diagnosis of anorexia nervosa and noted that anorexia nervosa was the most stable diagnosis followed by bulimia nervosa and then eating disorder NOS. It is interesting to note that length of history was positively associated with greater diagnostic stability. 13 This probably explains the higher stability in our sample as over half of the adolescents had a duration of illness of more than one year. 3
The criteria for admission and treatment protocol were tailored not only to the individual clinical profile but also considering the unmet needs of the service users as a majority of the patients came from a resource-scarce demographic background. This was different from the Western studies where the criterion for inpatient care is determined based on indicators of illness severity like baseline BMI, refusal to feed, and associated complications and community-based care was generally preferred for mild to moderately severe illness.14,15,16 Duration of hospital admission ranged from less than one week to about 3.5 months, with an average duration of one month. Fosson et al. reported that 42% got discharged by three months and 75% by six months. 17
All the individuals and their families received support for safe-refeeding, family psychoeducation and individual sessions with the adolescents, which is a recommended practice. 18 They were also supported by adjunct pharmacotherapy primarily in view of comorbidities. Although structured and intensive family therapy was instituted in only half of our sample with severe family psychopathology, psychoeducation and group family sessions focusing on meal plan control, and weight restoration were provided for all the families. Family Therapy-Anorexia Nervosa is an approved approach for the initial management of anorexia nervosa that helps the young person and their families with weight restoration and empowers the families in supporting the adolescents. 19 We adhered to similar principles but with an eclectic individualized and group approach where individual CBT-based sessions were considered alongside the family-based sessions.
In our study, duration of in-patient care and weight gain were positively correlated, with severe-extremely ill individuals improving even in a short period. Weight gain was noted to be rapid in adolescents with anorexia nervosa as compared to adults and in those who received inpatient treatment. 13 Although the remission rate couldn’t be calculated from the retrospective analysis the weight gain measure showed that 35.7% (n = 5) of adolescents had a weight gain of more than 5 kg over six-month period and more than half of the sample had weight gain less than or equal to 5 kg. The trajectory of weight gain showed improvement in 85.7% (n = 12) of patients in follow-up. Prasad et al. (2021) also reported a favorable outcome in 78.5% of the 15 adolescents who were followed up for over one year at a tertiary care center in India. They reported that one child had died after 18 months due to complications of electrolyte imbalance, coagulopathy, shock, and hemodynamic instability. 8 Fosson et al. noted that 80% of their sample who underwent treatment in the hospital gained significant weight. 17 Many Western studies report a chronic course and poor prognosis with a high risk of mortality.20-23 However, there is also Western literature including an epidemiological study substantiating a favorable outcome of adolescent anorexia nervosa despite its prolonged course.24,25 Viricel et al. reported that early-onset anorexia (during adolescence) was associated with a good prognosis with 55.8% and 25.7% attaining full and partial recovery respectively. 26 The overall functional improvement of our sample as assessed by the return to school was positive in 57.1% (n = 8) of our sample.
A comparison of the baseline clinical parameters of our sample with established prognostic factors,5,25,26 suggests that the patients admitted had a severe form of illness with poor prognostic factors such as long duration of illness, poor response to initial treatment, high level of psychiatric comorbidities, high level of adverse psychosocial factors, and high level of baseline CGI-S. But, the duration of inpatient care positively correlated with weight gain and overall weight gain trajectory, the rate of weight gain during inpatient care and overall functional improvement noted during follow-up were positive. These findings can be attributed to the intensive inpatient services provided to the patients and their families. Another important factor that can explain this is that only medically stable patients are admitted to this tertiary care mental health center. Kermarrec et al. (2014) highlighted the importance of integrated treatment for ensuring a good prognosis. 25 The favorable prognosis of the sample may indicate that in a low-resource setting like India, a flexible treatment approach should be adopted rather than a strict criterion for service provision. As a clinical team, we should be considering the factors beyond the clinical parameters, particularly the unmet needs of service users while providing care.
Conclusion
The current review highlights the treatment model for adolescents with anorexia nervosa followed at a tertiary care inpatient mental health setting in India that was a collaborative multidisciplinary approach, individualized to the patient’s needs. Adolescents with a higher severity of illness at baseline like early age of onset and low BMI showed significant weight gain which was positively correlated with the duration of the inpatient setting.
Strengths and Limitations
The study has the major limitations of a retrospective chart review which include missing data, observer bias and misclassification bias. Our findings are based on the cases detected through our health care system which may bias our understanding of the disorder’s incidence and natural course and lack generalizability. The study site is a tertiary care mental health setting with a separate child and adolescent psychiatry department. The multi-disciplinary approach followed in the center needs modification for its generalization across the country due to a lack of trained manpower resources.
Most importantly the study results focus on the mental health aspect of management of anorexia nervosa. This is a significant limitation as anorexia is a disorder with medical complications and always has been treated as a medical emergency but in our sample, only medically stable patients were admitted. There was periodic monitoring of general physical health, blood parameters and ECG but we were not able to observe a standard protocol and it was difficult to extract the results from our case records. It is essential that a standard operating protocol be developed in the institute for incorporating medical care along with mental health treatment. Even though weight is not a standard measure of clinical outcome in anorexia as per Morgan and Russell’s modified criteria, for convenience of statistical analysis we agreed on choosing weight gain which also closely reflected the clinical progress and the use of CGI score further supported this. Therefore, further research should be based on standard variables. The outpatient follow-up was very variable and based on the wide demographic distribution of the sample it might not be reflective of the actual course of the disorder as such. Despite all the limitations which make the results specific to the tertiary care mental health center, this is one of the first few articles to study the longitudinal course of anorexia in the Indian context. The data was meticulously collected and analyzed giving insights into an average 20-month course of this limitedly researched condition.
Future Directions
The current model of care in the study center is a preliminary step that needs to be explored, adapted and refined to address the lacunae. There is a need for prospective observational studies to address the limitations highlighted in this retrospective review and also to study the effectiveness of a standard treatment model using standardized outcome measures.
Footnotes
Acknowledgements
The authors thank Dr. Mariamma Philip for her input on statistical analysis and the staff of the Medical Records Dept. of the Institute for their cooperation and support.
Data Availability Statement
The data supporting the findings of this study are easily available from the corresponding author, upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Name of the Department and Institution to which the Work should be Attributed
Dept. of Child and Adolescent Psychiatry, National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, India
Presentation
Part of the data was presented orally at the ASCAPAP-2019 conference held at Chiang Mai in Thailand (9-11 Oct 2019).