
Abstract
Background:
Areca nut (AN) and AN products (ANPs) are commonly used as psychoactive substances with marked dependence potential. Scant information exists on the Indian mental health professionals’ (MHPs) knowledge of AN-ANPs, attitude toward AN-ANP use/users, and behavior regarding their clients’ AN-ANP use. To address this gap, a survey was undertaken to assess MHPs’ knowledge, attitudes, and behavioral responses toward AN-ANP use and addiction.
Methods:
We developed a pretested, customized questionnaire and conducted a cross-sectional online survey among a random sample of MHPs.
Results:
The 209 respondents included 91 psychiatrists, 105 clinical psychologists, and 13 other MHPs from diverse settings. Among them, 46.89% believed that AN-ANP use does not fit the definition of abuse/addiction as per the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition or International Classification of Diseases 10th Revision (ICD-10)/ICD-11. Among the psychiatrists, clinical psychologists, and other MHPs, 60.4%, 48.6%, and 61.5% were unaware of any AN-ANP cessation protocols. The addictive potential of AN-ANP with tobacco was rated as severe by 68.1% of psychiatrists and 51.4% of clinical psychologists; 46.2% of other MHPs rated it as moderate. The addictive potential of AN-ANP without tobacco was rated as moderate by 50.5% of clinical psychologists and mild by 46.2% of psychiatrists. Of the sample, 67.46% discussed the harmful effects of AN-ANPs with clients, while 74.6% said a few or none of their clients sought help for AN-ANP cessation.
Conclusion:
Major lacunae were detected in the understanding of Indian MHPs about the addictive potential of AN-ANPs, management aspects, etc. An urgent need has been revealed for sensitization programs on AN-ANPs and the development of evidence-based cessation protocols.
Keywords
This study among more than 200 Indian mental health professionals, mainly psychiatrists and clinical psychologists, revealed many lacunae in their knowledge about the addictive potential of areca nut and products containing it, the management of addiction to them, etc. Educational programs are required to address these findings.Key Messages:
Areca nut (AN) or betel nut, a phytoproduct, is the fourth most commonly used psychoactive substance globally. As of a 1990s estimate, approximately 600 million people worldwide use AN. 1 Since antiquity, its use has been socio-culturally sanctioned in Asia, particularly India and Southeast Asia. About 224 million Indians (23.9% of adult Indians) consume AN in diverse forms, often with tobacco, despite laws regulating the sale and consumption of AN, especially with tobacco.2, 3 As of recent reports, India’s cultivation and consumption of AN match that of tobacco.2, 4 The long-term health effects of habitual consumption of AN and products containing it (ANPs) range from tooth discoloration and inflammatory reactions to metabolic and endocrine disorders and potentially malignant as well as cancers.2, 5
AN has been varyingly reported as a psychoactive substance with significant addictive potential. Studies have shown varying degrees of addiction to AN, from harmful use to dependence, based on the definitions used.4, 6, 7 As per the last estimates, 38.8% and 40.8% of AN users fulfilled the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and the International Classification of Diseases 10th Revision (ICD-10) criteria for substance dependence. 8 Among those who use AN with tobacco, 79.5% satisfied the criteria for current dependent use according to both DSM-IV and ICD-10. 8 Addiction biology and mental health research has increasingly focused on the mechanisms of AN dependence, but results have been conflicting.9–11 Tobacco is an important addictive component in most Indian ANPs.2, 6, 12 Independently, AN has also been shown to have a distinct pathway to create stimulation and psychoactivity as well as dependence. AN contains several alkaloids, notably arecoline, arecaidine, guvacine, and guvacoline, which have stimulant, euphoriant, and addictive effects. In the brain, AN has been documented to interact with dopamine, gamma-aminobutyric acid (GABA), G-protein coupled receptor signaling pathway, and the reward pathway.9, 13 Globally, there is limited research on AN-ANP cessation; the few existing studies used tobacco cessation methodologies.12, 14, 15 To date, there is no focused, exclusive cessation or relapse prevention protocol for AN-ANP. 16 Most of the existing studies had explored behavioral interventions, which have been compared to a few nicotine-replacement therapies. However, research on pharmacological therapies is also emerging.12, 16, 17
AN-ANP dependence is a complex phenomenon influenced by biological, psychological, cultural, and social factors. Addressing AN-ANP dependence is challenging, as, in several parts of the world, the use of AN-ANP is culturally ingrained and socially accepted, the products are widely available and aggressively marketed, harm perception about AN-ANP is low, and most importantly, the availability of intervention strategies is limited. 2 Social perceptions may also contribute to the continued use of AN-ANP and deter individuals from seeking treatment. 1 It is common for smokeless tobacco to be used in conjunction with AN-ANP, which often leads to the erroneous attribution of dependence or misuse to tobacco rather than to AN-ANP.3, 6, 18
Once established, AN-ANP dependence may require treatment from a mental health professional (MHP).12, 16 In addition, particularly among children and adolescents, it is well documented that AN-ANP use may serve as a gateway to abuse of other substances. 8
To prevent the emergence of a huge health burden of AN-ANP use disorders, there is an urgent need to ensure that all persons with AN-ANP abuse/dependence seek MHP help. However, there is very limited research on the perception, particularly on the domains of knowledge, attitude, and behavior (KAB) of Indian MHPs toward AN-ANP use and users. Such details are needed to design a prevention and treatment delivery system for AN-ANP dependence in India, identify areas where MHPs need more training and support, and develop culturally appropriate interventions for the prevention and treatment of AN-ANP dependence. We aimed to address the gap by surveying Indian MHPs’ KAB toward AN-ANP use and dependence.
Methods
The authors developed a custom KAB questionnaire as there is no previous, pertinent, specific literature on this aspect. The authors included two MHPs with more than 30 years of combined experience in diverse settings and one oral pathologist with more than 20 years of experience interacting with patients who use AN-ANP. The questionnaire was developed after wide interaction with multiple specialists in several rounds. Content validation was sought from several like-minded experts. To prevent the issue of missing data, all questions in the KAB questionnaire were set up to require mandatory responses. As no similar previous studies are available, sample size estimation was not done.
This research did not involve invasive procedures and only collected pertinent data from MHPs anonymously and nonintrusively. Participation was voluntary, with consent, and without remuneration. The study was approved by the Institutional Ethical Committee.
The questions were in open-ended (for age and years of practice), multiple-choice (either single or more than one answer, as appropriate), or dichotomous (yes/no) format. No Likert, Guttman, Thurstone scale, or similar unidirectional or multidirectional scales were employed. No weightage or quantifying scores were awarded to the three domains.
The final questionnaire had 22 items, with the first part concerned with demographics of age (in years), sex (male/female/others), and the Indian state of domicile. The second part concerned with professional characteristics: type of MHP (Psychiatrist/Clinical Psychologist/Mental health nurse/Psychiatric social worker, as stipulated in the Mental Healthcare Act 2017), years of experience as an MHP, type of job (academic/private practice/both/no answer), practice location (urban/semi-urban/rural), and nature of the employer (government/corporate/others, including stand-alone, chain or group practice/no answer). The last part assessed the KAB and consisted of six multiple-choice items about knowledge, eight about attitude, and two about behavior regarding their clients’ AN-ANP.
Questions in the knowledge domain enquired about the knowledge of MHPs regarding whether AN-ANP fit the definition of abuse/addiction (as per DSM/ICD/Both/Neither), supposed therapeutic uses of AN (Yes/No/I do not know), whether habitual AN-ANP use interferes with prescription drugs (Yes/No/I do not know), the need to adjust medication for clients who regularly use AN-ANP (Yes/No/Not applicable), and the long-term health effects of AN-ANP (Carcinogen/Diabetogenic/Cause gastric ulcers/Alter blood pressure/ Nephrotoxic). To the best of our knowledge, there is no standard recommended/widely practiced protocols for the management of addiction to AN-ANP. Nevertheless, as there could be some assumptions and management practices, a question to the effect was framed as “Aware of existing protocol for the management of addiction to AN and products that contain it” with Pharmacotherapy/Psychotherapy/Other methods/Not aware as choices.
For this study, definitions were provided for psychoactive substances (all substances that, when taken, affect mental processes such as perception, consciousness, cognition, or mood and emotions), mood-altering substances (a subset of psychoactive substances that specifically affect mood and emotions, causing feelings of happiness, relaxation, or excitement) and addictive substances (any substances that can cause addiction). In the attitude domain, the first item pertained to the perception of the nature of AN-ANP. The choices provided were addictive only, mood-altering only, psychoactive but neither completely addictive nor mood-altering, and necessary for use in a socio-religious-cultural context. For this item, an option of “psychoactive and addictive” was not provided intentionally. It could trigger a bias in the responses to this and the subsequent items through subconscious anchoring. The other items in the attitude domain assessed whether they regularly probe the clients regarding AN-ANP use (Yes/No); the addictive potential of AN-ANP without tobacco (Nil/Mild/Moderate/Severe) and with tobacco (Nil/Mild/Moderate/Severe); the self-perceived confidence in the level of knowledge about AN-ANP (Confident/Not confident/Not sure), and the need they perceive for a cessation protocol for AN-ANP (Yes/No). The next question was whether their patients sought help to cease AN-ANP (None/Few/Some/Most/All). Though this question did not directly assess attitude, it was required as a basis for the subsequent question on their estimation of what proportion of their clients are motivated for cessation of AN-ANP (None/Few/Some/Most/All).
Questions in the behavior domain probed whether the respondents discussed the potentially harmful effects of AN-ANP with their clients (Yes/No) and whether they usually recommend stopping AN-ANP use (Yes/No).
A pilot study was conducted with a small, diverse sample size of 20, of whom 16 responded. The mean ± SD age of the respondent pilot sample was 43.19 ± 10.2 [range: 28–67] years, with a mean of 15.06 ± 9.93 [range: 3–36] years of mental health practice after their qualifying degree. It included 11 psychiatrists, two clinical psychologists, and three mental health nurses. There were eight male and eight female respondents. The KAB items showed a Cronbach α of 0.85, reflecting reliable internal consistency.
We randomly selected 5,646 Indian MHPs from the professional organization websites (of Indian Psychiatry Society and its Zonal and State Chapters; Indian Association for Geriatric Mental Health; Indian Association for Social Psychiatry; Indian Association for Clinical Psychologists; Rehabilitation Council of India; Indian Society of Psychiatric Nurses; Association of Psychiatric Social Work Professionals as well as from conference proceedings) and personal contacts of the authors (AMA and SA) and sent them personalized invitations, through email or WhatsApp, to participate in this study. No bulk messages were sent to online groups of any sort. We used
Statistical Analysis
The responses were analyzed using descriptive statistics. All returned responses were included. No comparison between the MHPs was conducted as the analyses would be exploratory, and the proportions of different MHPs differed. All entries and analyses were performed using PSPP software (Free Software Foundation. GNU PSPP, MS Windows Version 3, June 29, 2007, Boston, MA, USA)
Results
Of the 5,646 invitations sent, 635 bounced, and 47 recipients opted out, resulting in 4,964 eligible invitations (Supplemental File 1). Of these, 209 responded within the time frame of 20 days. The response rate was 4.2%. The sample consisted of 105 (50.24%) clinical psychologists, 91 (43.54%) psychiatrists, and 13 (6.22%) other MHPs (mental health nurses and psychiatric social workers). The domicile state of the respondents is depicted in Supplemental File 2 (17 participants did not mention their state of domicile). Most of the respondents were from Kerala (n = 26), followed by Maharashtra (n = 17), while there were only single MHPs answering from Chhattisgarh, Goa, Jammu and Kashmir, Ladakh, Meghalaya, Puducherry, and Tripura.
Males (70.3%) were predominant among psychiatrists, and females (77.1%) among clinical psychologists (Supplemental File 3). Psychiatrists had a higher mean age (44.59 ± 11.32 years) than clinical psychologists (34.23 ± 9.06) and other MHPs (38.15 ± 9.13).
Psychiatrists reported the longest mean duration of practice (15.7 ± 11.51 years), followed by other MHPs (11.62 ± 10.53 years) and clinical psychologists (6.9 ± 7.92 years). Most clinical psychologists and psychiatrists practice in urban settings (Supplemental File 3).
In the knowledge domain, 98 (46.89%) respondents—including 45.1% of psychiatrists, 46.7% of clinical psychologists, and 61.5% of other MHPs—believed that AN-ANP does not fit the definition of abuse/addiction as given in DSM-5/DSM-5TR or ICD10/ICD-11 (Table 1, Supplemental file 4). In the different groups, 15%–16% responded that AN has known therapeutic uses. In comparison, the remaining respondents (83.74%, n = 175) in the sample either replied “do not know” or believed that AN has no therapeutic value. Most respondents in each of the three groups acknowledged the possibility of habitual AN-ANP use potentially interfering with prescription drugs, the rate being 69.99% (n = 170) for the whole sample. Among the psychiatrists, 73.6% did not feel the need to adjust medication dosage for patients habitually using AN-ANP. Regarding awareness of existing protocols for managing AN-ANP use disorders, 114 (54.5%) of MHPs were not aware of any protocols, and 70 (35.89%) of them were aware of psychotherapy. Forty-eight (45.7%) clinical psychologists expressed familiarity with psychotherapy protocols, while 55 (60.4%) psychiatrists denied awareness of any protocols. While 82.4% of psychiatrists and 71.4% of clinical psychologists knew that AN-ANP is a carcinogen, 61.9% and 71.4% of them, respectively, knew that AN-ANP can cause gastric ulcers. Among other MHPs, 61.5% knew that AN-ANP can alter blood pressure. Awareness of the other assessed physical consequences was less than 60% in the three groups.
Response to the Knowledge Items (N = 209).
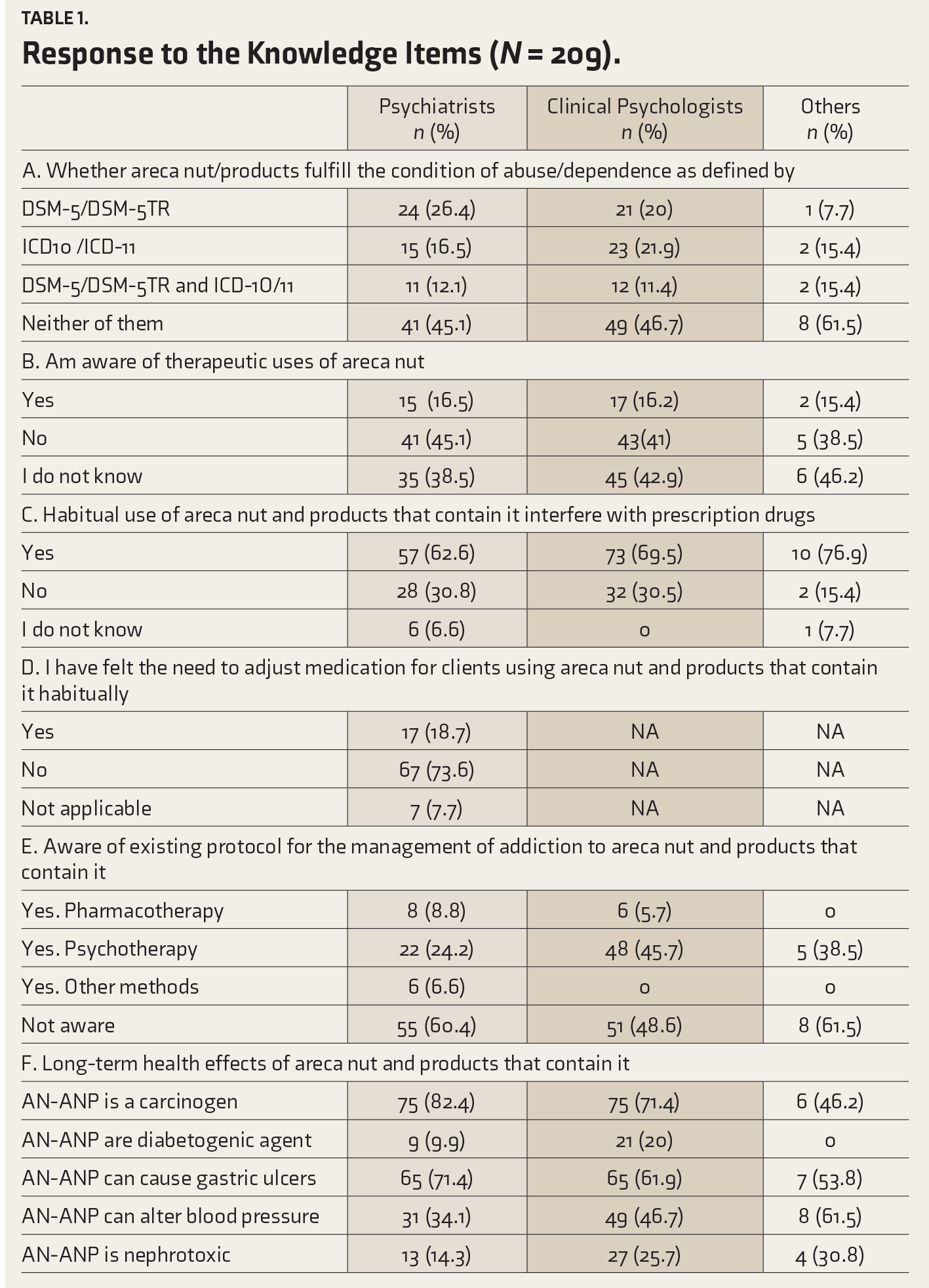
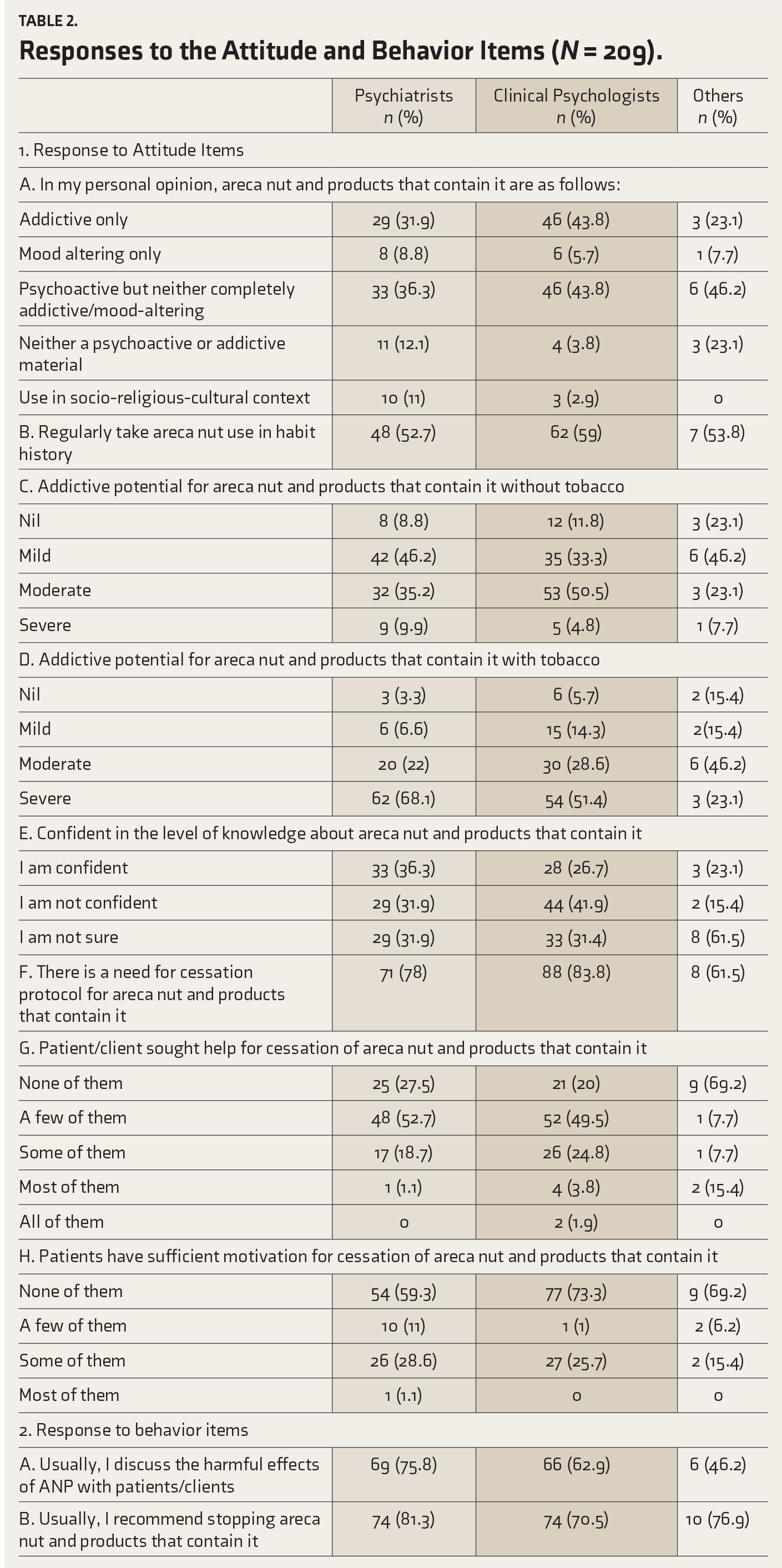
Table 2 features the analysis of the attitude and behavior items. In each group, the majority characterized AN-ANP as “psychoactive but neither completely addictive/mood-altering” (36.3% of psychiatrists, 43.8% of clinical psychologists, and 46.2% of other MHPs). Only two respondents(psychiatrists) felt AN-ANP to be a psychoactive substance with addictive potential and communicated personally, though they answered the question to their best understanding. More than half of the participants in each group (52.7% of psychiatrists, 59% of clinical psychologists, and 53.8% of other MHPs) regularly enquired about AN-ANP use during case interviews or history taking.
Responses to the Attitude and Behavior Items (N = 209).
In terms of the addictive potential of AN-ANP without tobacco, while 50.5% of clinical psychologists rated it as moderate, 46.2% of psychiatrists and other MHPs rated it as mild. When AN-ANP is combined with tobacco, the majority of psychiatrists (68.1%) and clinical psychologists (51.4%) rated the addictive potential to be severe. In comparison, 46.2% of the other MHPs rated it moderate (Figure 1).
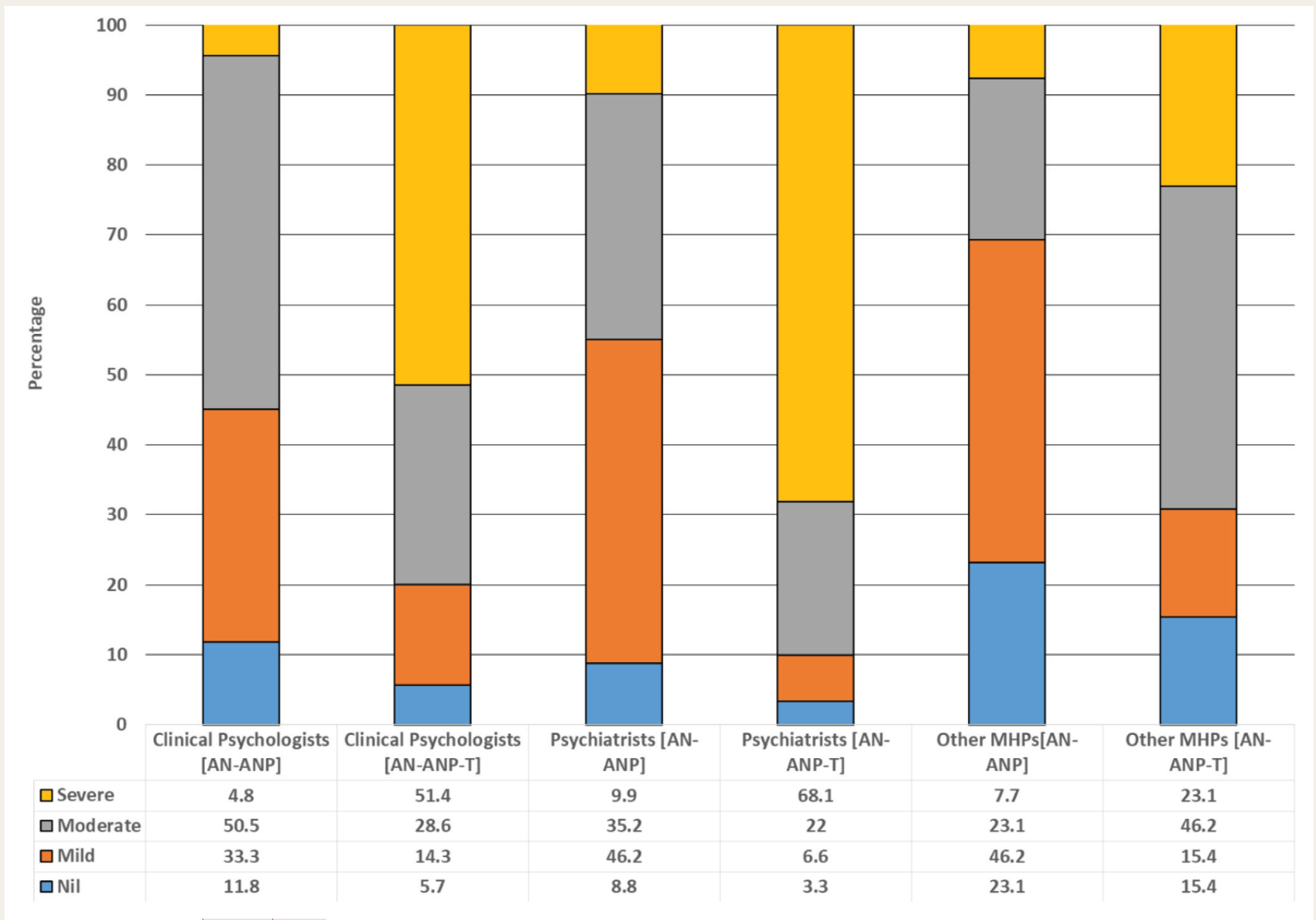
AN-ANP, areca nut and products containing it —without tobacco; AN-ANP-T, areca nut and products containing it —with tobacco.
Regarding their confidence regarding their knowledge of AN-ANP, only 64 (30.62%) in the sample, including 36.3% of psychiatrists, 26.7% of clinical psychologists, and 23.1% of other MHPs, expressed confidence. Most of the sample (n = 167, 79.9%) agreed on the need for a focused cessation protocol for AN-ANP. However, the majority of psychiatrists (52.7%) and clinical psychologists (49.5%) commented that only a few of their clients sought help for AN-ANP cessation, while according to the majority of other MHPs (69.2%), none of their clients did so (Table 2. Also, most respondents in each group (59.3% of psychiatrists, 73.3% of clinical psychologists, and 69.2% of other MHPs) replied that their clients needed more motivation for cessation.
In the behavior domain (Table 2), compared to the other two groups, a higher proportion of psychiatrists discussed the harmful effects of AN-ANP with patients (75.8%) and also recommended the cessation of AN-ANP (81.3%).
Several participants requested literature about the subject from us.
Discussion
Many facets and adverse health consequences of AN-ANP use have been reported.2, 4, 5 However, there is a lacuna about the KAB of MHPs about AN-ANP, which this study tried to fill. Slightly less than half of all the respondents believed that AN-ANP would not fit into abuse/dependence definitions of DSM/ICD, while slightly more than half were not aware of any cessation protocol. Difference was observed among different groups of MHPs on how they estimated the addictive potential of AN-ANP with and without tobacco (Supplemental File 4).
The health burden associated with the long-term consumption of AN-ANP, particularly in India, has reportedly been on the rise recently. 4 Several studies have investigated the addictive potential of AN-ANP.2, 3, 6 Several tools have been developed to assess AN-ANP use and dependence, including the reasons for chewing and barriers to quitting.2, 19, 20 Despite the widespread use of AN-ANP by a huge percentage of the global population, the DSM-5/5-TR or the ICD-11 has not classified AN-ANP as a potential substance of abuse or dependence. 2 Nevertheless, a few reports suggest otherwise. 21
A growing body of literature has explored the need for structured, evidence-based protocols and guidelines for AN-ANP cessation.12, 14–16 Most of these studies underscored the need for further research and the development of an exclusive, comprehensive protocol for treating AN-ANP dependence or abuse.12, 16 Even if such a protocol is established, its implementation at the population level would not be possible unless MHPs are aware of such a protocol and perceive AN-ANP to be a substance of abuse/dependence. 22 In this background, we aimed to investigate the KAB of Indian MHPs toward AN-ANP.
The response rate of 4.2% in this study reflects the challenges associated with survey research among MHPs, the demanding nature of their profession, or even their indifference toward AN-ANP.23, 24 This may also be an indirect reflection of either a lack of interest in the topic, poor awareness, or a notion of the less addictive/psychoactive potential of these widely used substances.
Despite this limitation, our sample of 209 respondents, which included clinical psychologists, psychiatrists, and other MHPs, offered a representative glimpse into the field. The demographic characteristics revealed differences in sex distribution, practice locations, and years of practice among the professional groups. Notably, male psychiatrists and female clinical psychologists predominated. The variation in practice locations and experience underscores the diverse contexts in which MHPs operate (Supplemental File 3).
This is the first published study exploring the KAB of Indian MHPs toward AN-ANP. As such, our findings could not be refuted or accepted in the context of previous research, as there is none. Therefore, most of this discussion is centered on the implications of our observations.
As per the literature, AN-ANPs are psychoactive substances with varying addictive potential.6, 25 However, to the first knowledge item question, only two MHPs responded that AN-ANP fulfills the condition of dependence/use disorder as laid down by recent editions of DSM or ICD. On the other hand, 46.89% responded that AN-ANP does not fulfill the condition. These responses reflect the need for proper education and sensitization of the MHP community about AN-ANP.
Alternative medicine believes that AN has several curative properties, while there is none in modern medicine.5, 26 In this background, 4-in-5 (83.74%) of our respondents acknowledged that AN-ANP has no therapeutic uses or that they are unaware of such claims. This reflects that MHPs need more sociocultural insights about AN-ANP (Table 1).
As AN-ANP contains biologically active ingredients that can cross the blood-brain barrier and reasonably alter normal homeostasis, they could potentially interfere with various therapeutic agents. 27 Though about two-thirds of the psychiatrists opined that AN-ANP could interfere with prescription drugs, three-fourths of them did not adjust the dose when there is AN-ANP use. This indicates the need for further sensitization about the pharmacodynamic properties of AN-ANP.
Based on tobacco cessation models, a few pharmacological and several nonpharmacological approaches have been described in the literature to treat AN-ANP use and dependence.12, 14, 16 But none are recognized or reported as standard protocols exclusive to AN-ANP. There are stark differences among MHPs regarding their knowledge of the availability of management protocols for AN-ANP dependence. More than half were unaware of such existing approaches, while more than one-third were aware of psychotherapy, and only 7% were aware of pharmacotherapy methods. Only about one in four psychiatrists were aware of the psychotherapy approach. Clinical psychologists and psychiatrists exhibited low levels of familiarity with the availability of psychotherapy approaches, emphasizing the need for targeted sensitization educational interventions to provide necessary knowledge and skills to MHPs about AN-ANP cessation.
AN-ANP is known to be carcinogenic (odds ratio of 7.9 for those who use AN-ANP vs. those who do not), diabetogenic (odds ratio of 1.47–1.62), gastric ulcer promoting (2.62 times higher risk), blood pressure altering (1.45 times higher risk) and nephrotoxic (odds ratio of 1.44 for chronic kidney disease).28–32 In our study sample, about 75%, 14%, 66%, 42%, and 21% considered AN-ANP carcinogenic, diabetogenic, gastric ulcer promoting, blood pressure altering, and nephrotoxic, respectively. This finding highlights the urgent need to educate the MHPs about the potential health hazards of AN-ANP. It is also pertinent to note that about 5% of all AN-ANP users develop a debilitating, potentially malignant state called oral submucous fibrosis, which severely affects their quality of life and causes psychiatric morbidity or decreased psychological well-being.33–35
About 59% of clinical psychologists and 53% of psychiatrists inquired about AN-ANP use during case interviews or history taking. This indicates differences in awareness or priorities in clinical assessment. These variations merit further exploration to enhance the integration of substance-related inquiries within the mental health assessment framework. AN-ANP can influence executive function and personality assessments, both of which are an integral part of mental health examination.36–37
Literature delineates the addictive potential of tobacco in AN-ANP.3, 6, 9 Our study uncovered significant differences in perceptions of the addictive potential of AN-ANP with and without tobacco.3, 6, 8 More than half (106 MHPs) of our sample viewed AN-ANP without tobacco to have nil or mild addiction potential, while about 175 (83.73%) believed that AN-ANP with tobacco had moderate or severe addiction potential. These response patterns for the two items are a very important finding, as when read together, it is easy to conclude that most of the MHPs perceive tobacco to be the strong causative agent for addiction and AN-ANP to be inherently only mildly addictive. On the contrary, AN-ANP without tobacco also causes a considerable level of addiction.2, 3, 6, 25 This divergence in views, particularly with many psychiatrists rating the addictive potential as severe only when AN-ANP is combined with tobacco, reflects the need for targeted education and awareness campaigns. Understanding these variations is vital for developing sensitization and education programs for MHPs and developing interventions that align with the perspectives of different MHP groups.
Only about 30.62% of MHPs felt confident about their knowledge regarding AN-ANP. This, too, underlines the potential need for continuing education initiatives to enhance MHPs’ understanding of the complexities surrounding AN-ANP use, including its addictive nature and associated health risks.
The unanimous agreement among MHPs on the need for a cessation protocol underscores a shared recognition of the importance of addressing AN-ANP use within mental health settings.12, 16, 38 However, clinical psychologists and psychiatrists’ stark observation that most patients did not seek help for cessation and were not motivated to quit emphasizes the barriers to translating awareness into action. This finding calls for targeted strategies, including motivational interviewing, to promote help-seeking behaviors among individuals using AN-ANP.
In the behavior item analysis, the observed difference in the proportion of different professional groups discussing the harmful effects of AN-ANP with patients highlights the variations in communication practices among MHPs. Psychiatrists were more likely to engage in such discussions. This discrepancy could stem from variations in training, awareness, or perceived relevance of discussing the harmful effects of AN-ANP within different mental health practice settings.
No major differences were found between the professional groups recommending the cessation of AN-ANP. This suggests a shared recognition among these professionals regarding the importance of recommending cessation, irrespective of their primary area of expertise, or it may indicate a universal acknowledgment of the health risks associated with AN-ANP use. Also, the observed differences in discussing the harmful effects aligns with studies on substance use discussions within mental health settings emphasizing the need for standardized practices and training to ensure consistent communication across professional groups.14, 15, 21, 39 The universal agreement among MHPs on the importance of recommending cessation echoes broader literature emphasizing the critical role of healthcare providers in promoting substance cessation.
Limitations
The findings of this study should be interpreted in light of its limitations. The self-reported survey design is inherently prone to biases such as social desirability, memory or recall, acquiescence, and framing. The diverse backgrounds of the MHPs, the absence of an in-depth cultural exploration, and the limited literature for comparison further limit the interpretations. The response rate of 4.2% may restrict the generalizability of the findings and could have impacted the accuracy and representativeness. The MHPs who participated might have been more interested in or knowledgeable about AN-ANP than the remaining Indian MHPs, potentially skewing the results.
The study did not explore the MHPs’ understanding of the neurobiology of AN-ANP addiction. The role of sociocultural factors on the use of AN-ANP and the perception of MHPs toward such harmful practices have not been captured. The study also failed to comprehensively quantify the knowledge gap or assess the quality of existing knowledge. Given the wide variations in the use of AN-ANP and the prevalence of AN-ANP use/abuse across India, the study did not gather data on the frequency of AN-ANP use encountered by the MHPs. The study did not gauge the MHPs’ attitudes toward using AN-ANP. The behavior domain was limited to only two questions, providing minimal insight from MHPs who discuss the harmful effects of AN-ANP with their patients. A more detailed exploration of interactions with AN-ANP users in their practice could have provided deeper insights into the subject matter.
Future Directions
Well-designed comprehensive survey instruments based on current findings could help capture various influencing factors. Direct investigation of patients’ perspectives and lived experiences and an in-depth exploration of cultural factors could provide valuable insights into AN-ANP use. Future studies should aim for a better sample size across the nation to enhance the generalizability of findings.
To better assess MHPs’ knowledge of AN-ANP, future studies should include questions on neurobiology, abuse patterns, and gaps in existing awareness campaigns. Future research should also explore how sociocultural factors, such as prevailing beliefs and norms, influence MHPs’ attitudes toward AN-ANP use. This includes cessation recommendations and discussions about its harms with patients. Also, MHPs’ perceptions of AN-ANP’s public health burden and their confidence in addressing it should be investigated. Future studies should investigate the factors influencing communication practices, differences in training across disciplines (such as psychiatry, clinical psychology, etc.), and their impact on communication approaches. They should also consider time constraints during patient consultations, how they influence discussions about AN-ANP use, and the perceived severity of the health risks associated with AN-ANP and its influence on communication priorities.
Impact on Policies
This study underscores the need for AN-ANP education for Indian MHPs, including the integration of AN-ANP into the substance abuse curriculum and standardized communication training in this aspect. Standardized communication interventions that promote effective discussions about AN-ANP use within mental health assessments are needed. The results also support policy efforts for AN-ANP cessation protocols, resource access, and communication standardization.
Conclusion
The present study provides valuable insights into the knowledge, attitudes, and behavioral responses of MHPs toward AN-ANP, highlighting both areas of consensus and divergence in a sample subset of Indian MHPs. The findings underscore the importance and need for sensitization about AN-ANP, tailored educational interventions, and the development of evidence-based cessation protocols that align with the perspectives of diverse MHPs. Addressing these nuances is crucial for developing effective interventions and enhancing the role of MHPs in mitigating the impact of AN-ANP use on mental and physical health and well-being. The observed differences in the KAB among the MHPs, coupled with a shared commitment to recommending cessation, highlights areas for targeted interventions, training, and policy development. As we move forward, it becomes imperative to delve deeper into the nuances of knowledge, attitudes, and behavioral interventions within Indian mental health care settings, ensuring a unified and impactful approach to addressing AN-ANP use.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethical Approval
This research was earlier approved by the institutional ethical committee of the St. Thomas Institutions of Healthcare and Medical Education, Kerala, India vide its communication dated September 28, 2023 letter dated STH/ETCL/RES/2023/09.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.