
Abstract
Background:
Patients with substance use disorders are common in general medical practice and are a major risk factor for several non-communicable diseases. Appropriate screening is a vital step for providing brief interventions which can provide a good opportunity to tackle this crisis and in achieving target 3.5 of the sustainable development goal which includes strengthening the prevention and treatment of substance abuse.
Objectives:
To study the magnitude of substance use and factors associated with it among people seeking health care services at primary care settings.
Methods:
The cross-sectional study recruited people seeking services at primary care settings to screen for substance users (SU) and determine the associated factors. The data was collected using a pretested semi-structured questionnaire including socio-demographic characteristics, health status and the Alcohol, Smoking and Substance Involvement Screening Test tool.
Results:
The study showed that 43.4% of the participants were SU. The current use of smokeless tobacco was higher compared to tobacco smoking (21.3% and 4.7%). The multivariate logistic regression showed that advancing age (AOR: 2.61 and 95% CI of 1.01–6.79), male gender (AOR: 705 and 95% CI of 4.25–11.70), primary and middle school (AOR: 3.24 and 95% CI of 1.52–6.92) literacy status, unemployed (AOR: 0.49 and 95% CI of 0.25–0.95), religion and other backward caste (AOR: 2.42 and 95% CI of 1.37–4.30) were significant correlates of SU.
Conclusion:
Substance use was reported by two-fifths of the participants seeking services at primary care centres in our study and stresses the need for incorporating brief interventions to prevent higher degrees of dependence and its complications.
Previous research has established that substance use is a significant public health concern affecting individuals seeking health care services. This current study provides a comprehensive assessment of substance use patterns. It provides an understanding of the prevalence and severity of substance use among individuals seeking primary health care services. Additionally, it investigates the factors influencing substance use within primary care settings.Key Message:
Substance use is a significant public health issue as it remains a prominent cause of morbidity and mortality. 1 It is also a leading contributor to preventable deaths, making it a global concern. About 5% of the global population aged 15–64 years has used substance at least once, and an estimated 0.6% of this population is affected by substance use disorder (SUD). 2
According to the World Health Organization’s (WHO) global status report on alcohol and health, an estimated 2.3 billion individuals consume 32.8 g of pure alcohol daily. The percentage of current drinkers worldwide, defined as individuals who have consumed alcohol in the past 12 months, has increased from 45% in 1990 to 47% in 2017. 3 In addition to alcohol, the United Nations Office on Drugs and Crime’s World Drug Report 2022 indicates that approximately 284 million individuals globally use drugs, a 26% rise over the past 10 years. According to the Ministry of Social Justice and Empowerment, 14.6% of Indian adults consume alcohol, and the latest Indian Global Adult Tobacco Survey 2 (GATS-2) indicated that over 28.6% of all Indian adults use tobacco. 4
Several substances such as alcohol, tobacco, heroin, prescription stimulants and methamphetamine have been linked to an increased risk for non-communicable diseases (NCDs). According to the WHO, approximately 38 million people die each year from NCDs, and nearly 85% of these deaths occur in low- and middle-income countries. Providing brief interventions for quitting substance use has been identified as one of the ‘best buys’ for tackling NCDs. 5 The tobacco epidemic poses one of the most significant public health threats globally and is associated with NCDs like ischemic heart diseases, cancers, diabetes and chronic respiratory diseases which are the leading causes of death worldwide. Tobacco use is also a significant risk factor for cardiovascular and respiratory illnesses, over 20 different types or subtypes of cancer, and a number of other deteriorating health disorders due to the extremely addictive nature of nicotine. 6 Alcohol is a causal factor in 60 types of diseases and injuries and a component cause in 200 others. 7 Stimulants like cocaine can have an immediate and direct impact on blood pressure, increasing the risk of cardiac arrest. Other substances are also associated with health issues, including an increased risk for hypertension, cardiovascular problems, and heart disease. 8
Screening is the application of a simple test to determine if a patient has a certain condition. An international team of researchers and clinicians developed the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) for the WHO as a technical tool to facilitate early identification of substance-related health risks and SUDs in primary health care, general medical care and other settings. The ASSIST screening tool is used to identify individuals using substances so that appropriate brief intervention or referral can be provided. 9 Hence, the present study was conducted to assess substance users (SU) using the ASSIST tool among people seeking health care services and to identify factors associated with them in primary care settings and plan for suitable interventions, and is a novel attempt in this region of the country.
Methods
Study Design
A cross-sectional study was conducted from January 2021 to December 2022.
Settings
The recruitment of sample was from seven primary care centres from a southern district in India. Prior ethical approval was taken before beginning the study.
Participants
All patients above 18 years of age visiting the primary care centres were screened for substance use. After explaining the study’s objectives and purpose, a detailed information sheet was provided to each participant, and written informed consent was obtained. In the case of illiterate participants, a witness’s signature was also taken.
Operational Definition
Ever use was defined as ‘A person who consumed any of the substances currently or has/had consumed substances at some time during his lifetime’.
Current user: Individuals who are SU at the time of the study and have used it in the last 30 days.
Former users: Individuals who quit substances for a period of three months or more.
Never user: An individual who has not consumed a particular substance in his or her lifetime.
Chronic morbidities: If any study participant is diagnosed with hypertension, diabetes mellitus, dyslipidemia, had Ischaemic Heart Disease (IHD), asthma, stroke, cancer, liver disease, CKD (chronic kidney disease) and other conditions that include hypothyroidism, tuberculosis and autoimmune diseases is meant to have chronic morbidity.
Data Sources
Patient data collection involved administering a questionnaire to collect socio-demographic characteristics and health status. The ASSIST questionnaire, developed by WHO commonly used for early identification of substance use-related health risks was also used. It was designed to be cross-culturally adaptable and culturally neutral. It is an eight-item questionnaire designed to be administered by a health professional that takes between 5 and 10 minutes to administer. The risk level was noted among patients reporting the use of specific substances to classify their dependence as lower, moderate and high. Details on the definition of levels of risk for each substance, administration, scoring and interpretation are provided in the tool’s manual. 9
Data Collection
The study was carried out among the patients coming to the seven primary care centres, connected to the medical college. Though the centres were chosen based on convenience, the participants who gave consent were randomly recruited from those centres and screened using questionnaires intended to collect socio-demographic characteristics, health status and status of substance use. Participants were assured of confidentiality in order to ensure true responses. The data collection tool took approximately 10–15 minutes to administer and was collected using Kobo Collect v1.28.0 on a mobile handset. 12 The researcher (fluent in both English and regional language), recorded and analysed the data.
Sample Size
The prevalence of tobacco in the general population in the state of Karnataka, as per GATS-2 report 11 is 22.8%. Therefore, the sample size required for a margin of error of 15% at a confidence interval (CI) of 95% and adding a 15% non-response rate works out to be 690. We included 710 patients who visited the healthcare facility seeking primary care in the Udupi district in our study.
Statistical Methods
Statistical analysis was performed using Statistical Package for Social Science (SPSS) licensed version 16.0 for Windows (SPSS Inc., Chicago). For continuous data, summary statistics such as mean and standard deviation were used when the data were normally distributed, while the median and interquartile range were used when the data showed skewness. To examine the association between categorical variables, the chi-square test was used. Multiple logistic regression was used to identify factors associated with SUDs like age, gender, religion literacy, occupation, marital status, cast, socio-economic scale and chronic comorbidities. The results were described in terms of proportions and their 95% CIs.
Results
Socio-demographic Characteristics
The key socio-demographic parameters and the overall prevalence of chronic morbidities of the study participants are depicted in
Univariate and Multivariate Analysis for Association of Socio-demographic Characteristics and Comorbidities with Substance Use (N = 710).
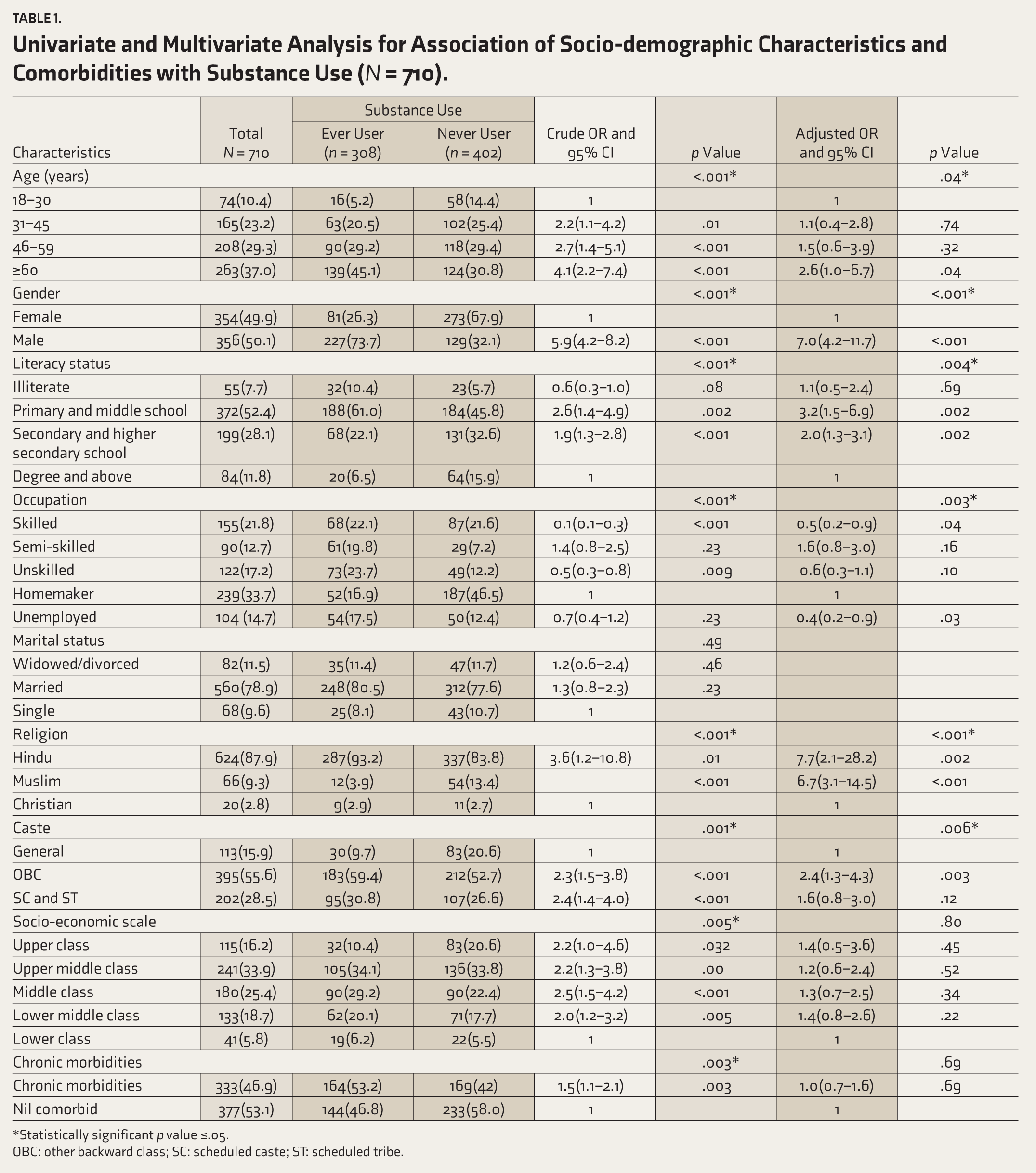
*Statistically significant p value ≤.05.
OBC: other backward class; SC: scheduled caste; ST: scheduled tribe.
Factors Associated with SU
Univariate and multivariate logistic regression analysis is depicted in Table 1. The age, gender, literacy status, occupation, religion, caste, type of family, socio-economic scale and chronic morbidities were found to be the significant determinants of SU on univariate analysis. SU was significantly associated with male gender, more than 60 years of age, primary and middle school, semi-skilled, SC and ST and middle-class socio-economic scale.
However, the multivariable logistic regression model showed that advancing age, gender, literacy status, religion, occupation and caste were significantly associated with SU. The results showed that there is a significant association (p value = .043) of advancing age with ever users (AOR: 2.61 and 95% CI of 1.01–6.79).
There is a statistically significant association found between males and SU (p < .001). Results showed that males have 7.05 times more ever users than female participants (AOR: 7.05, 95% CI: 4.25–11.70). There was a statistically significant association found between (p value: .002) primary and middle school literacy status participants and SU. They have 3.24 times more ever users when compared to people with higher literacy status (degree/post-graduation) (AOR: 3.24, 95% CI of 1.52–6.92). OBC caste was identified as a significant factor associated with SU (p value = .006) and showed that OBC caste has 2.42 times more ever users when compared to the general category (95% CI is 1.37–4.30).
Risk Level of SU
Table 2 reports the pattern and dependence of substance use among study participants attending primary care. Of the total 710 participants, current use of alcohol was higher (23.1%), followed by current use of smokeless tobacco (SLT) (21.3%) and current users of tobacco smoking (n = 33, 4.6%) as depicted in Table 2.
Proportion of Substance Use Among Study Participants Attending Primary Care Setting (N = 710).
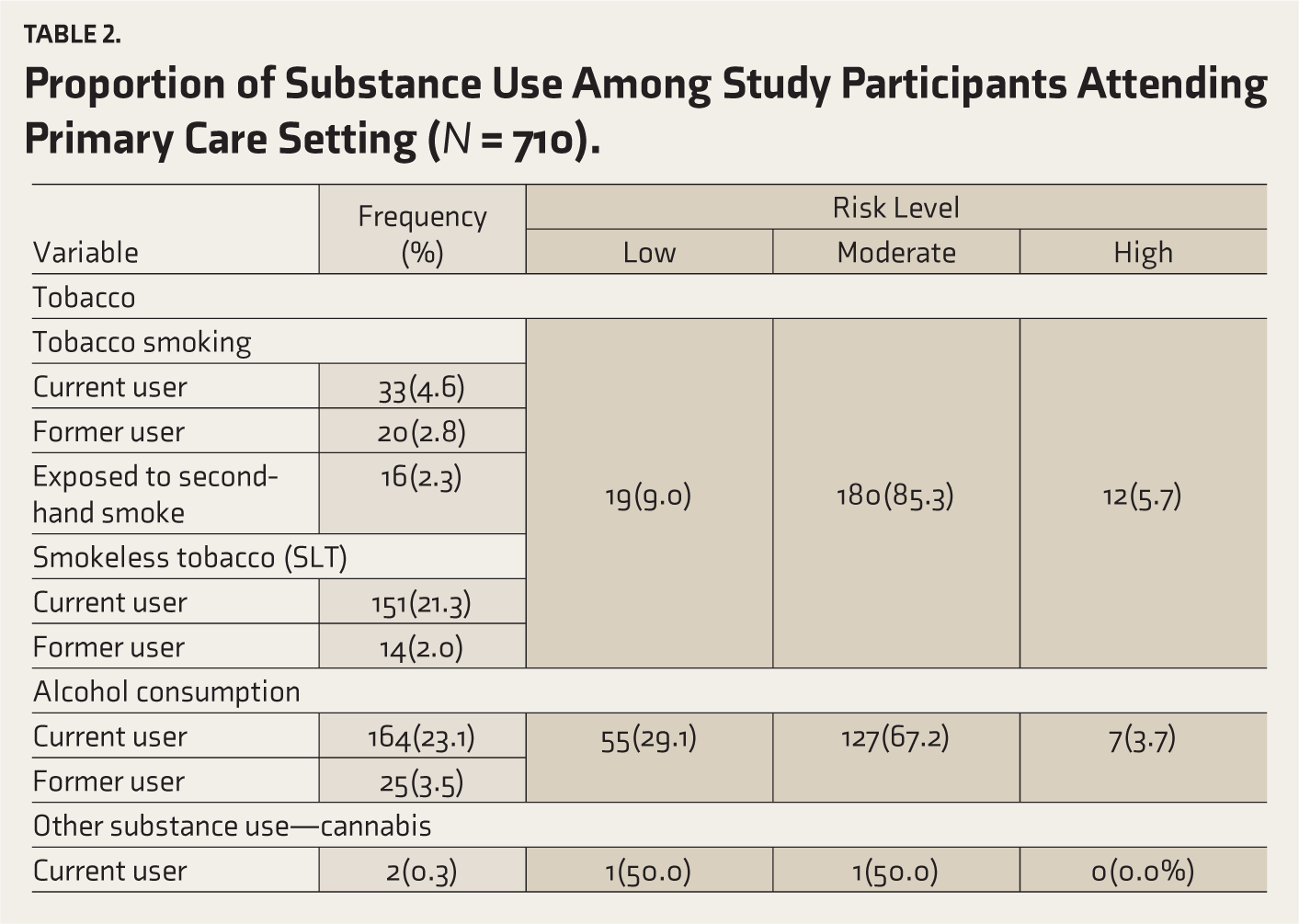
Alcohol risk level: ASSIST scores revealed that among the alcohol ever users, more than half were a moderate risk (67.2%), more than a quarter, were lower risk (29.1%) and around 3.7% were high-risk alcohol users who required referral to higher centre for de-addiction.
Tobacco risk level: Among the tobacco-ever users, the majority (85.3%) were moderate risk, followed by lower risk (9.0%) and high-risk of tobacco users (5.7%).
Cannabis risk level: ASSIST scores revealed that among two cannabis-ever users, one participant was at lower risk and the other was a moderate-risk, cannabis user.
Discussion
The study investigated the proportion of SU among individuals seeking health care services in primary health care settings, and its association with sociodemographic factors and morbidities. In the study, we found that 43.4% of the participants had a history of substance use. Several socio-demographic factors such as age, gender, literacy, occupation and caste were found to be significantly associated with substance use. It was observed that more than half of the participants who were consuming alcohol and tobacco were classified as being at moderate risk, indicating a potential concern. A similar pattern of substance use was observed among patients seeking care at primary care clinics, with prevalence rates ranging from 35.8% to 69.9% in previous studies.13–15 These findings suggest a substantial proportion of SU in this setting, highlighting the importance of integrating brief interventions for identification and quitting substance use in primary care settings.
In this study, we found that the prevalence of alcohol use was the highest, closely followed by SLT. On the other hand, the prevalence of smoking tobacco was lowest among current users. Comparing our findings to the National Family Health Survey-5, we noted that the national prevalence for alcohol consumption was reported to be 18.8% among males and 1.3% among females aged 15 years and above. 16 The difference in the prevalence rates could be attributed to the fact that our study was conducted in a hospital setup and included individuals with occasional alcohol use, which may have contributed to higher rates. Regarding SLT consumption, the result from our study is similar to the national prevalence reported in the GATS-2 (2016–2017) among Indians. 17
Our study findings contrast with a study conducted in Nagaland, which reported current SLT users to be the highest, followed by tobacco smoking and alcohol consumption. 18 The variations in the prevalence rates in comparison to the present study could be due to the high prevalence of SLT, the implementation of the Nagaland Liquor Total Prohibition Act 1989, along with National Tobacco Control Programme then not being adopted in the Mokokchung district of Nagaland. Additionally, contrasting results have also been observed in another study conducted across the globe, where the most common substance using the ASSIST tool was tobacco, followed by alcohol and marijuana. 19
The use of ASSIST scores and categorization into low, moderate and high-risk levels proved valuable in identifying individuals who required different levels of intervention such as health education and brief intervention, or further referral for evaluation and specialised treatment. Our study revealed that among the alcohol-ever users, more than a quarter, that is, 29.1% were low-risk alcohol users, while more than half (66.7%) were at moderate risk levels, and only 3.7% were high-risk alcohol users. In contrast, a study conducted in Kerala by Sukumaran et al. 18 reported half (50.5%) of alcohol ever users were at low risk, followed by more than a third (37.8%) as moderate-risk users, and 11.7% as high-risk individuals. The variation in the results could be due to the rural setting where this study was conducted, while our study was conducted in both urban and rural areas. These findings emphasize that most of the participants have lower and moderate risk levels, and may benefit from brief interventions provided at primary care settings. It is known that brief advice provided by physicians in primary care to tobacco users may enhance cessation rates. 20 A study done in primary care settings in two high tobacco burden states of India not only revealed a high prevalence of tobacco users, 11 but also demonstrated the scope for continuing and strengthening cessation services by the health care providers for people who are at risk.
The present study found several correlates of SU, including advancing age, gender, literacy status, occupation, religion and caste. The burden of substance use, especially among elderly men in India is further underscored by findings of Study on Global Aging and Adult Health-India Wave 1 and other research papers.21,22 Similar findings have been reported in a study done by Sau et al. 23 in Kolkata which showed a significant association between age and ever use of substances. Both regional 24 and global 25 studies point towards the link between unemployment and SU, thus supporting our study findings. The results of our study are similar to the study by Saikia et al., 26 which showed that SU was significantly higher among male adults and those with lower education levels. Despite research supporting the link between SU and conditions like cardiometabolic disease, pain and COVID-19, 27 our study found chronic morbidities were a significant factor for SU only at univariate analysis. This could be due to a smaller sample size for the present study. OBC and religion (Hindu and Muslim) were found to be factors significantly associated with substance use. On comparing with studies based on nationally representative data,28–30 we found supporting evidence for religion, while we also found studies where ST was a significant factor, which is in contrary to our results.
The strength of the study lies in being the first of its kind in South India to comprehensively screen for substance use among people seeking health care services in primary health centres. This study also lends support to achieving the targets of sustainable development goal (SDG) 3.5 which includes strengthening the prevention and treatment of substance abuse, including narcotic drug abuse and harmful alcohol use, as well as SDG target 3.a, which addresses the importance of tobacco control. 31
Our research emphasizes the importance of assessing the burden of substance use among people attending primary care settings. Although certain risk factors are non-modifiable, early detection allows for timely intervention and support, which can prevent the escalation of substance use problems. It also contributes to public health, highlighting efforts by increasing awareness and education about SUDs to make informed decisions regarding prevention and treatment. Policies that address social determinants and create supportive environments can have a significant impact on mitigating SUDs, especially among individuals with non-modifiable risk factors.
However, as the participants were recruited using convenience sampling from primary care settings, and represented only the patients receiving care, the study participants may not be representative of the burden in the population, thus being a limitation of the study. Furthermore, the use of self-reported information increases the possibility of under-reporting due to social desirability bias.
To conclude, more than two-fifths of the healthcare users had substance use, and it was associated with increasing age, male gender, lower literacy levels, unemployment and among OBC. To enhance the integration of substance use, screening and interventions in primary care settings, adopting the Screening, Brief Intervention and Referral to Treatment model can be highly beneficial. Implementing opportunistic screening using the ASSIST tool followed by appropriate interventions such as brief intervention in the primary care setting needs further evaluation. This will enable the development of evidence-based practices to address substance use in primary care settings more efficiently and comprehensively.
Footnotes
Author Contributions
MMK and AV conceptualised the study. The research plan was strengthened by SKP and AD. Data collection in the field was coordinated by AV and supervised by MMK, SKP and AD. The analysis was done by AKP. Interpretation of data and drafting of the manuscript were done by AV and PB. It was refined by MMK, SKP and AD. Final approval of the version was read and approved by all authors.
Consent for Publishing Data
Written informed consent was taken from the participants. It has been mentioned under participants in methods section.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
All patients above 18 years of age who were willing to provide written informed consent were included in the study. Ethics approval for the study was granted by Kasturba Medical College and Kasturba Hospital Institutional Ethics Committee, Manipal Academy of Higher Education (MAHE IEC: 148/2021).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Prior Presentation
Second State Conference of Indian Association of Preventive and Social Medicine, Karnataka Chapter (2022) at Yenepoya Medical College, Deralakatte Mangalore.