
Abstract
Background:
Adverse childhood experiences (ACEs) increase the odds of alcohol use disorder (AUD).
Aim:
To study the ACEs, coping, and resilience in persons with AUD and their non-drinking siblings from high-density families.
Methods:
The study used a case-control study design. Using purposive sampling, 135 participants were selected; the sample consists of persons with AUD (n = 45), non-drinking siblings (n = 45), and healthy controls (n = 45), selected from out-patient and in-patient services from a government-run de-addiction centre in Bengaluru. Individuals were administered an ACEs questionnaire, Brief-COPE, and Connor-Davison Resilience scale. Descriptive statistics, Friedman’s test, and Bonferroni’s post-hoc test, Binary Logistic Regression were used for analysis.
Results:
ACEs, coping, and resilience significantly differ across the three groups. Persons with AUD and their non-drinking siblings are comparable in terms of ACEs and having dysfunctional family members. Non-drinking siblings and healthy controls have similar coping and resilience. None of the healthy controls had dysfunctional family members.
Conclusion:
ACEs are more prevalent and more frequent in persons with AUD. Individuals with AUD showed higher avoidant coping and lower resilience than their non-drinking siblings and healthy controls. Early identification of ACEs and interventions to build resilience and coping strategies could prevent individuals from developing AUD in high-density families.
Individuals with alcohol use disorder and their non-drinking siblings from high-density families have similar shared environments, such as adverse childhood experiences, whereas they are dissimilar in non-shared environments, such as coping and resilience. Healthy controls and non-drinking siblings are comparable in terms of coping and resilience. Coping strategies and resilience protected the siblings of persons with AUD from high-density families in developing AUD.Key Message:
Alcohol use disorder (AUD) is a chronic, recurrent and relapsing condition influenced by multiple factors, and about 50% of the risk for AUD is heritable. 1 Family history is a significant risk factor for AUD.1,2 Adverse childhood experiences (ACEs) increase the odds of undesirable health-related outcomes, particularly death and disability related to AUD. 3 Alcohol use is the most common consequence of ACEs.4,5 Childhood trauma is related to psychopathology, including the early onset of drinking in adolescence and in young adulthood. Alcohol use acts as maladaptive coping in anxiety and ACEs. 6
Significant levels of childhood trauma in the form of emotional, physical, and sexual abuse were found in alcohol and other drug-dependent women than men. 7 Higher emotional abuse was linked to alcohol abuse in men and physical abuse was related to problematic alcohol use in women. 8 Young adults with multiple ACEs account for more alcohol-related problems and psychological symptoms compared to those with fewer ACEs. 9
Coping mechanisms play a crucial role in the cause of AUD and various psychopathologies. 10 A variety of coping strategies were used by men with AUD.11-19 Women with AUD use more emotion-focused coping and less problem-focused coping than their male counterparts.20-23 Coping strategies mediate the relationship between childhood trauma, AUD, social anxiety and AUD, borderline personality.24-26 Coping is the single most common predictor across developmental transitions from adolescence to young adulthood, in addition to depressive symptoms in AUD. 27
Resilience may be defined as adaptation, thriving, resistance to illness and the ability to bounce back or recover from stress. 28 Resilience reduces the risk of AUD. The Cholesky model shows that the resilience-AUD relationship was attributed 57% to genetics and 36% to a shared environment. 29
Study Rationale
Very few studies examined ACEs, coping, and resilience in persons with AUD and their non-drinking siblings. There is limited literature on ACEs in the development of AUD and coping and resilience in preventing adult children of parents with AUD from developing AUD. Therefore, the study examined the reasons why individuals from the same high-density families (presence of AUD in more than one family member) do not develop AUD when the other sibling develops. We hypothesized that there would be no difference in ACEs (shared environment), coping, and resilience (non-shared environment) among persons with AUD, their unaffected siblings, and healthy controls.
Aim
To study the ACEs, coping, and resilience in persons with AUD, their non-drinking siblings, and healthy controls.
Methods
The study used a case-control study design to test the hypothesis. Participants were recruited using purposive sampling. Sample size was estimated using G Power software (version 3.1.9.4) with 80% statistical power and alpha was set at a 5% level of significance considering two groups (Persons with AUD and healthy control) Considering the mean and SD of childhood trauma questionnaire in persons with AUD (44.1 ± 17.1) and mean and SD of childhood trauma questionnaire in healthy controls (30.3 ± 6.7) from previous study, 30 sample size was calculated. The estimated sample size was 14 in each group. However, the researcher recruited more subjects for regression analysis (examining the predictors of AUD in patients compared to their non-drinking siblings) and for better generalizability of study findings. Therefore, the sample size of n = 45 was considered in each group. Persons with AUD n = 45 (male = 30, female = 15) unaffected siblings (n = 45), from high-density families of AUD. Healthy controls (absence of a family history of psychiatric disorders) n = 45 (male = 30, female = 15). The total sample size was 135 (Figure 1 ). The outcome parameters of the study were the predictors of AUD in patients and the non-development of AUD inpatient siblings and healthy controls. ACE, coping, and resilience were considered as predictors. Confounding variables (age and gender) and potential bias were controlled using a case-control design with age and gender-matched healthy controls.
Flow-chart Showing Sample Recruitment.
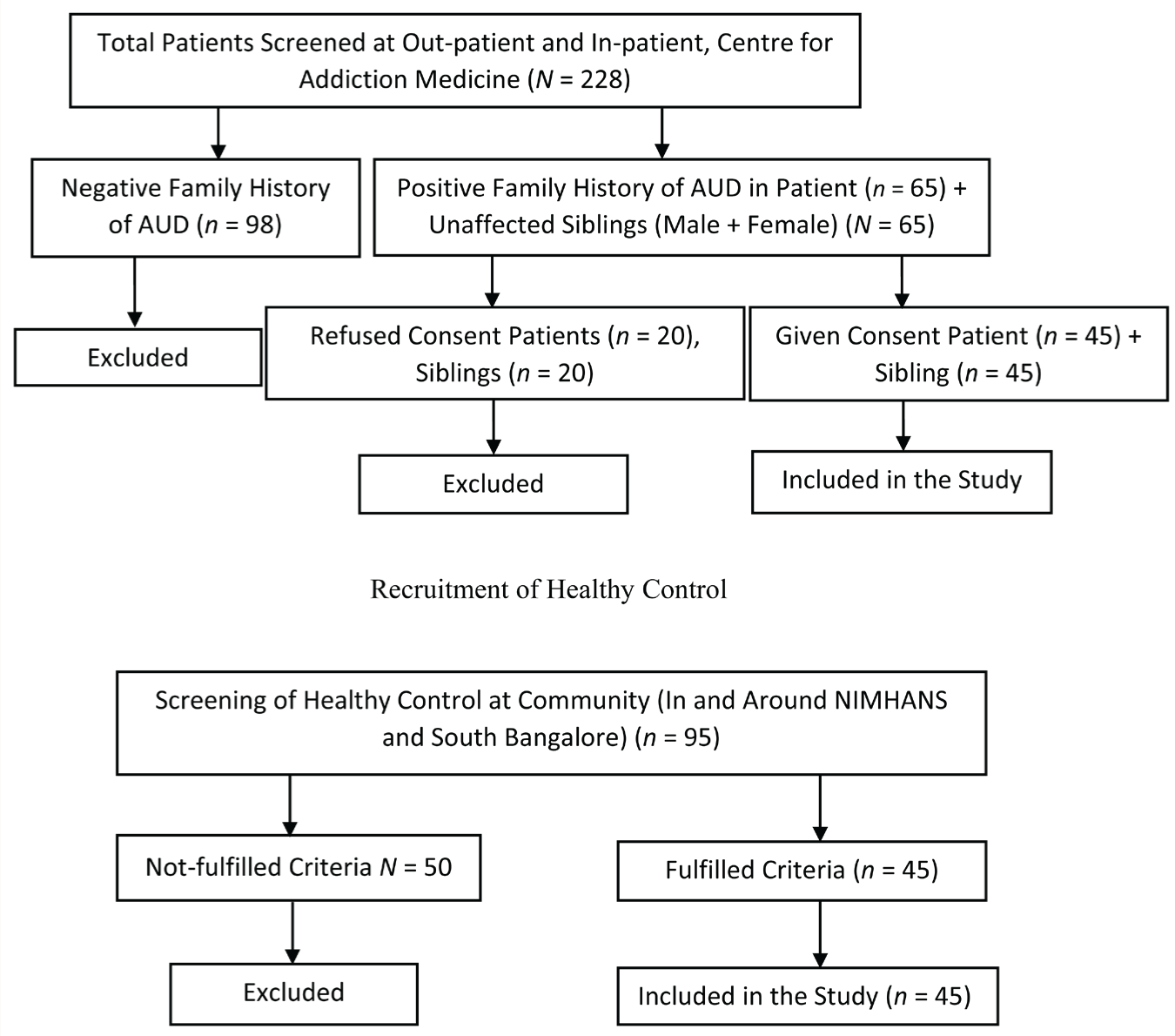
The study participants were recruited from a Government tertiary care teaching hospital in Bangalore. Persons with AUD sought treatment at out-patient and in-patient facilities (participants who were abstinent from alcohol for at least two weeks). Healthy controls were recruited from Bengaluru Urban and matched with age and gender of persons with AUD. Inclusion criteria for persons with AUD: Individuals (male & female) diagnosed with AUD (as per DSM-5), within the age group of 18–50 years, and high-density families with AUD (family history of AUD in more than one family member), and those who have a sibling (male or female) without AUD, who can speak English, Kannada, and Telugu were considered for the study group. Individuals with cognitive deficits were excluded from the study group. Inclusioncriteria for non-drinking siblings (comparative group): Individuals without substance use disorder aged between 18 and 50 years and any other major psychiatric illness were included in the comparative group. Non-drinking siblings who refused the consent for the study were excluded. Inclusion criteria for healthy controls: Individuals (male and female) without substance use disorder and absence of substance use in father and any other psychiatric illness, aged between 18 and 50 years, Exclusion criteria for healthy controls: Persons with a lifetime history of AUD or any psychiatric illness were excluded. Written informed consent was obtained from all the participants. Institute Ethical clearance was obtained for the study. Data was collected through the interview method using a semi-structured interview schedule and standardized research tools, data was collected within the ethical committed approval period from April 2019 to November 2022. Data collection was briefly interrupted owing to the COVID-19 lockdown.
Research Tools
The Mini-international Neuropsychiatric Interview (English Version 5.0.0)
It is a standardized diagnostic interview to diagnose mental health problems, including substance use disorders. The MINI evaluates the 17 prevailing mental health disorders. Test-retest reliability is between 0.52 and 1.00, with most disorders having a reliability coefficient above 0.75. The MINI can be administered in 20 minutes. Each item has a response ‘yes’, or ‘no’ type. The kappa values for concordance with the Structured Clinical Interview for DSM 3-R (SCID) are higher than 0.50. 31
ACEs-International Questionnaire 32
This scale has 43-item screening questions with 13 domains to determine the types of ACEs. ACE severity score can be calculated by adding the total number of adversity that was reported to have occurred more than once (frequency score). The ACE severity score is specific and detects more severe impactful adversity. The total ACE exposure score is sensitive and identifies the occurrence of any adversity. A total ACE exposure score can be calculated by adding the total number of adversity reported, irrespective of the frequency at which it might have occurred (Binary Score). The ACE questionnaire can be administered to individuals aged 18 years and above. The validity of the scale is evidenced by the correlation between subdimensions (phi = 0.20, p < .01), across subdomains (phi = 0.10, p < .01), and predictive validity (r = 0.35, p < .001). 33
Brief Cope Inventory
We used a shorter version of Brief Cope consisting of 28 items and 14 subscales. Subscales included behavioural disengagement, self-distraction, active coping, denial, substance use, use of emotional support, use of instrumental support, planning, positive reframing, humour, acceptance, religion, venting, and self-blame. Subjects rate the degree to which they use each strategy to cope with stressful events. Rating for each question has a 4-point Likert scale that ranges from 1 to 4. There is no overall score for this instrument. The psychometric properties of Brief Cope are well established, and Cronbach’s alpha ranges from 0.50 to 0.90. 34
Connor-Davidson Resilience Scale
The scale can be administered to community samples, primary care out-patients, and psychiatric out-patients. It has 25 items; each item is rated on a five-point scale (0–4). Higher scores indicate more resilience. The scale has five domains. Domain one consists of eight items to assess personal competence, high standards, and tenacity. Domain two comprises seven items on tolerance of negative affect, trust in one’s instincts, strengthening effects after overcoming stress. Domain three consists of five items examining positive acceptance of change and secure relationships. Domain four has three items assessing control. Domain five has two items on spirituality. The scale has high test-retest reliability (r = 0.36, p < .0001) and high internal consistency (Cronbach’s alpha of 0.89). 35 The Resilience Scale- English version was used in the study. 35 Written permission was obtained from the author to use the instrument. This scale is validated in the Indian setting. 36 All four scales were translated into Kannada and Telugu languages by language experts. The standard procedures for translation were followed, and the back translation was done for both the Kannada and Telugu language versions. We have not validated the Kannada and Telugu version scales.
We used the Shapiro-Wilk test to test the normal distribution of the data. Data were not normally distributed. Hence, non-parametric tests were used to analyse the data. Descriptive statistics were used to express continuous and categorical variables. Friedman’s test and Bonferroni’s post hoc test were used to compare the difference in study variables across three groups. Age and gender-adjusted Binary logistic regression analysis was applied to predict the outcome variables, that is, development and non-development of AUD.
Results
Table 1 reveals that the mean age of the AUD individuals and healthy controls is 37 years (±7.0) as both groups were age-matched. The siblings’ mean age was 35 years (±7.0). The mean years of education of patients were 7.8 (±4.1), siblings 8.6 (±4.7), and healthy controls 14 (±3.6), respectively. Healthy controls have more mean years of education than patients and their non-drinking siblings. Most patients (56%), siblings (76%), and healthy controls (73%) were married. Most patients and siblings (96%) and healthy controls (76%) belonged to lower socioeconomic status. All three groups (patients, siblings, healthy controls) were comparable in terms of age and economic status.
Among patients, 17 of them reported having depression and deliberate self-harm (DSH), and one patient reported having self-injurious behaviours. The age at onset of alcohol initiation among men with AUD was 19 (±4.1), the age at alcohol dependence was 24 (±5.4), age at treatment was 31(±6.3), respectively. Age at alcohol initiation among women with AUD was 25 (±8.2), age at dependence was 31 (±8.5), and age at treatment was 39 (±7.2), respectively (Table 1). Four patients, one sibling, and a healthy control have diabetes. Five patients and one sibling have hypertension, and 16 patients have seizures. Four patients and two siblings have Asthma. One sibling reported having an anxiety disorder.
Socio-demographic Profile of the Patients, Siblings, and Healthy Controls.
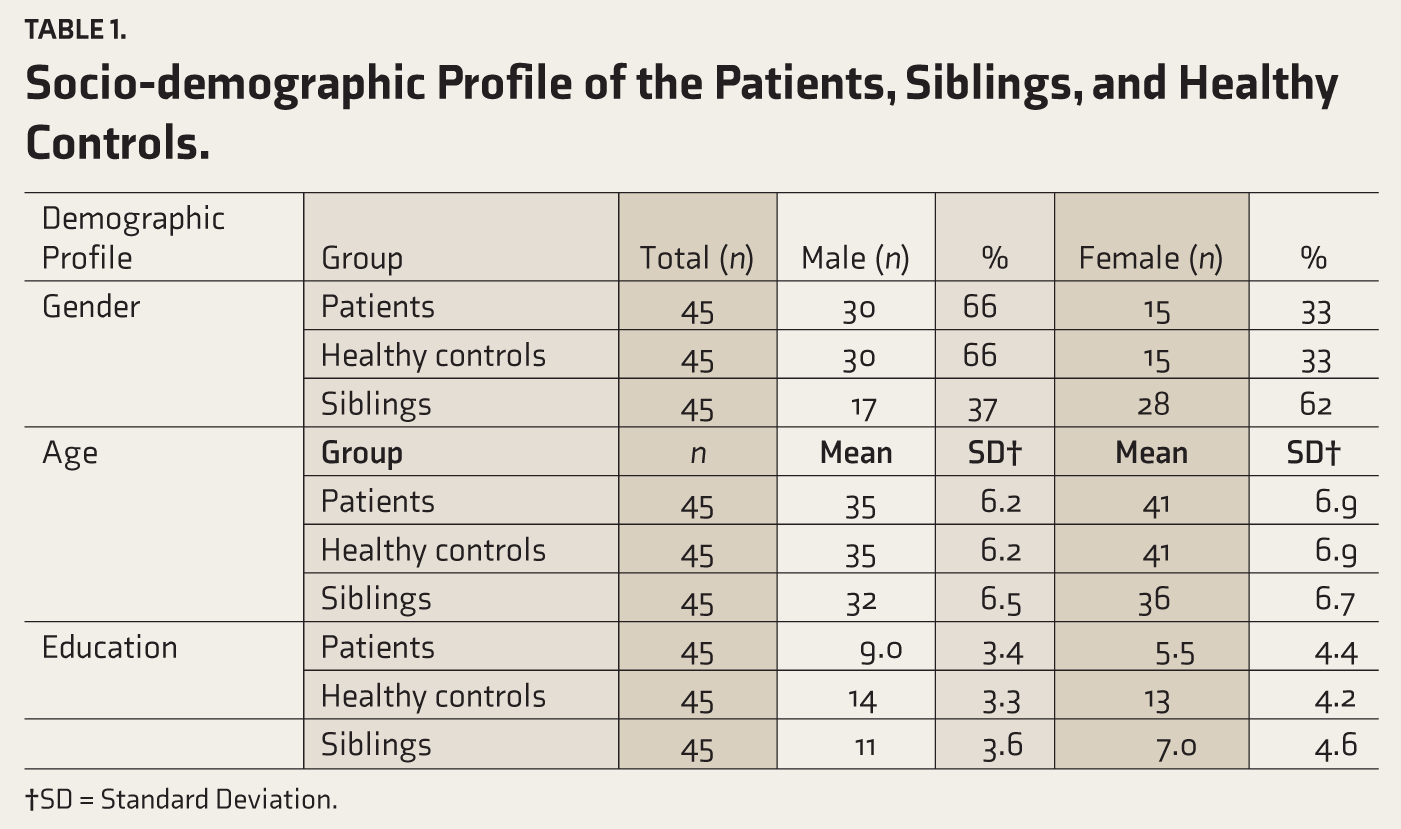
†SD = Standard Deviation.
Table 2 revealed that most (93%) of the persons with AUD reported that they had experienced emotional, physical and sexual abuse (24%) at least once, and 22% of them experienced more than once. Siblings reported physical abuse (69%) and emotional abuse (69%) at least once. Healthy controls reported physical abuse (64%) and emotional abuse (16%) at least once and more than once (2%). Persons with AUD (24%), siblings (13%), and healthy controls (7%) experienced sexual abuse more than once. Almost all the persons with AUD and their siblings lived with a dysfunctional family (dysfunctional family refers to having any of the following dysfunctional aspects such as incarcerated family member, mentally ill family member, family members having SUD, absence of one or both the parents, family member being treated violently, parental divorce). Among healthy controls, none of them have dysfunctional family members. ACE was more frequent and highly prevalent among persons with AUD than their non-drinking siblings and healthy controls.
Adverse Childhood Experiences in Patients, Siblings and Healthy Controls.
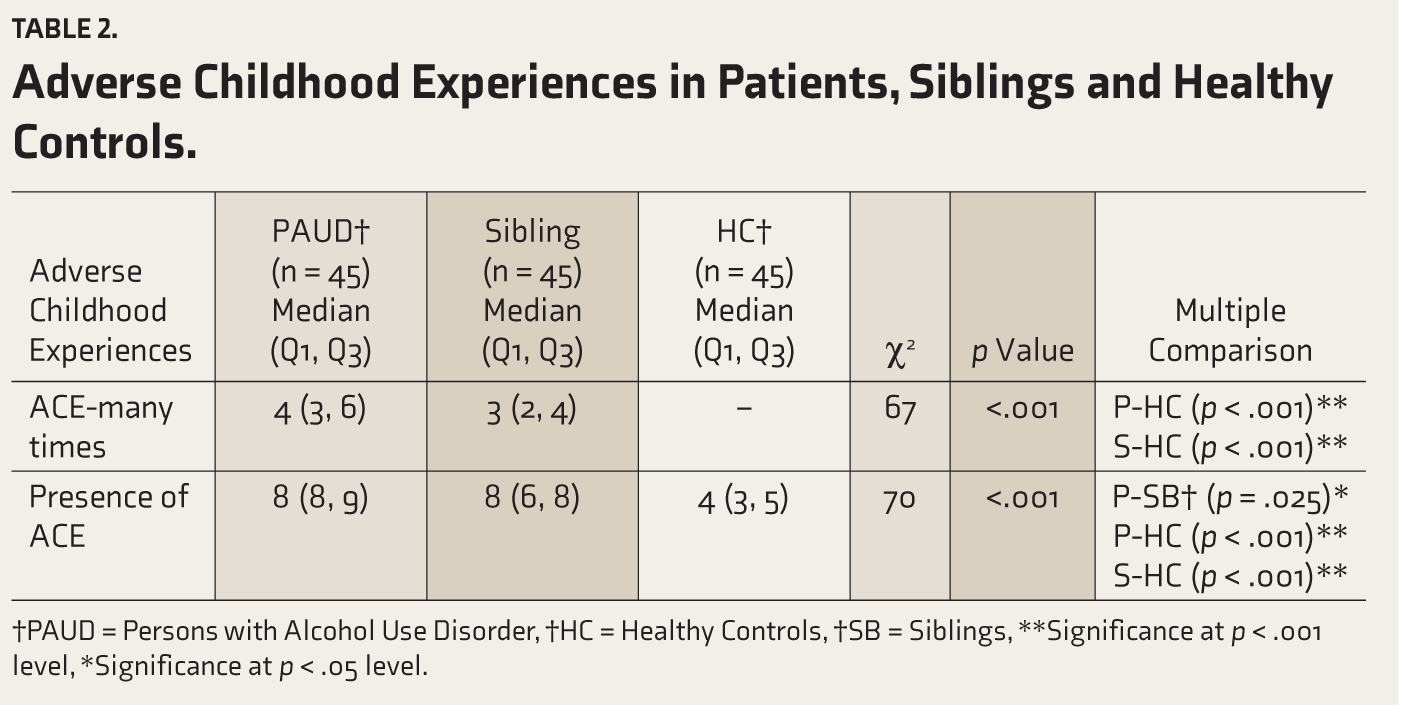
†PAUD = Persons with Alcohol Use Disorder, †HC = Healthy Controls, †SB = Siblings, **Significance at p < .001 level, *Significance at p < .05 level.
Friedman test indicated that there is a significant difference (χ2 = 66.96 and p = < .001) between persons with AUD and their non-drinking siblings regarding ACE frequency (Child Abuse, child neglect, and having dysfunctional family members). The Bonferroni posthoc test indicates that ACE scores of persons with AUD (p < .001) and siblings (p < .001) significantly differ. ACE scores were higher for persons with AUD, followed by their siblings, and none of the healthy controls reported having ACE more than once. Hence, the null hypothesis (H1) that there would be no difference in ACEs (shared environment) in persons with AUD and their non-drinking siblings compared to healthy controls is rejected.
Table 3 reveals that there is a significant difference between patients and their siblings’ groups regarding coping. Bonferroni’s post hoc test results indicated that non-drinking siblings’ and healthy controls’ coping median score is similar. Persons with AUD differed in all the domains of coping when compared to the other two groups indicating coping (non-shared environment) is dissimilar between the persons with AUD and their non-drinking siblings.
Coping Among Persons with AUD, Siblings, and Healthy Controls.
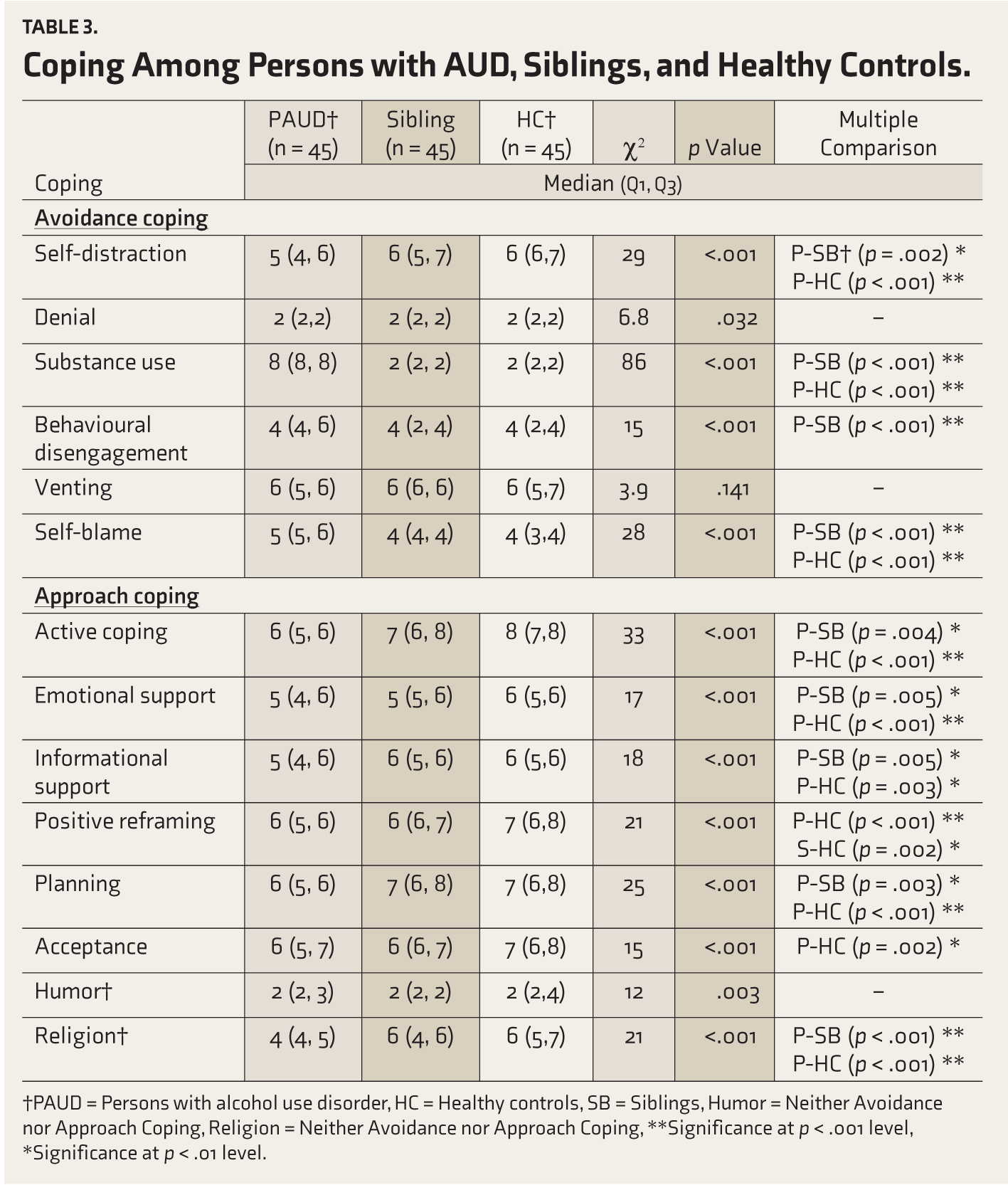
†PAUD = Persons with alcohol use disorder, HC = Healthy controls, SB = Siblings, Humor = Neither Avoidance nor Approach Coping, Religion = Neither Avoidance nor Approach Coping, **Significance at p < .001 level, *Significance at p < .01 level.
Table 4 shows that there is a difference between persons with AUD and their non-drinking siblings regarding resilience score. Bonferroni’s post-hoc test results indicated that healthy controls and non-drinking siblings are similar in resilience when compared to persons with AUD difference. Hence null hypothesis that there would be no difference in coping and resilience (non-shared environment) across the three groups is rejected.
Resilience Among Persons with AUD, Siblings, and Healthy Controls.
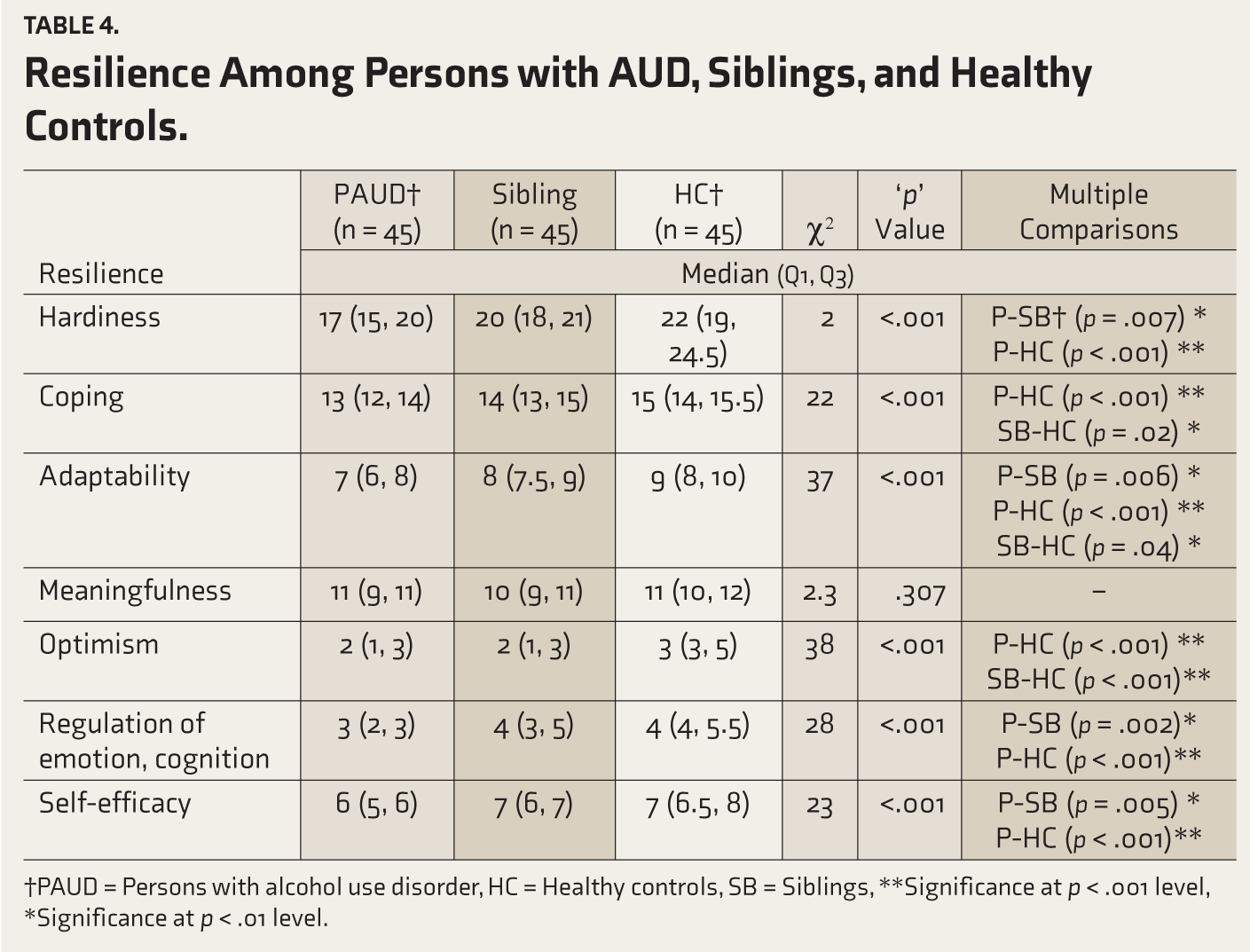
†PAUD = Persons with alcohol use disorder, HC = Healthy controls, SB = Siblings, **Significance at p < .001 level, *Significance at p < .01 level.
Table 5 shows that ACE, coping, and resilience were used as predictors of outcome (AUD and Non-AUD). These three variables were considered in the model because they are significantly different in patients and siblings. The results of binary logistic regression indicated that age, more ACEs, poorer active coping, self-blame, poor emotional regulation and cognition, and lower self-efficacy predict the development of AUD. In the female gender, higher the hardiness predicts lesser chances of developing AUD. The Hosmer-Lemeshow test showed that the model fits the data (χ2 = 10.65, p = .22), and the correct classification percentage is (85.6).
Binary Logistic Regression Showing Predictors of Alcohol Use Disorder.
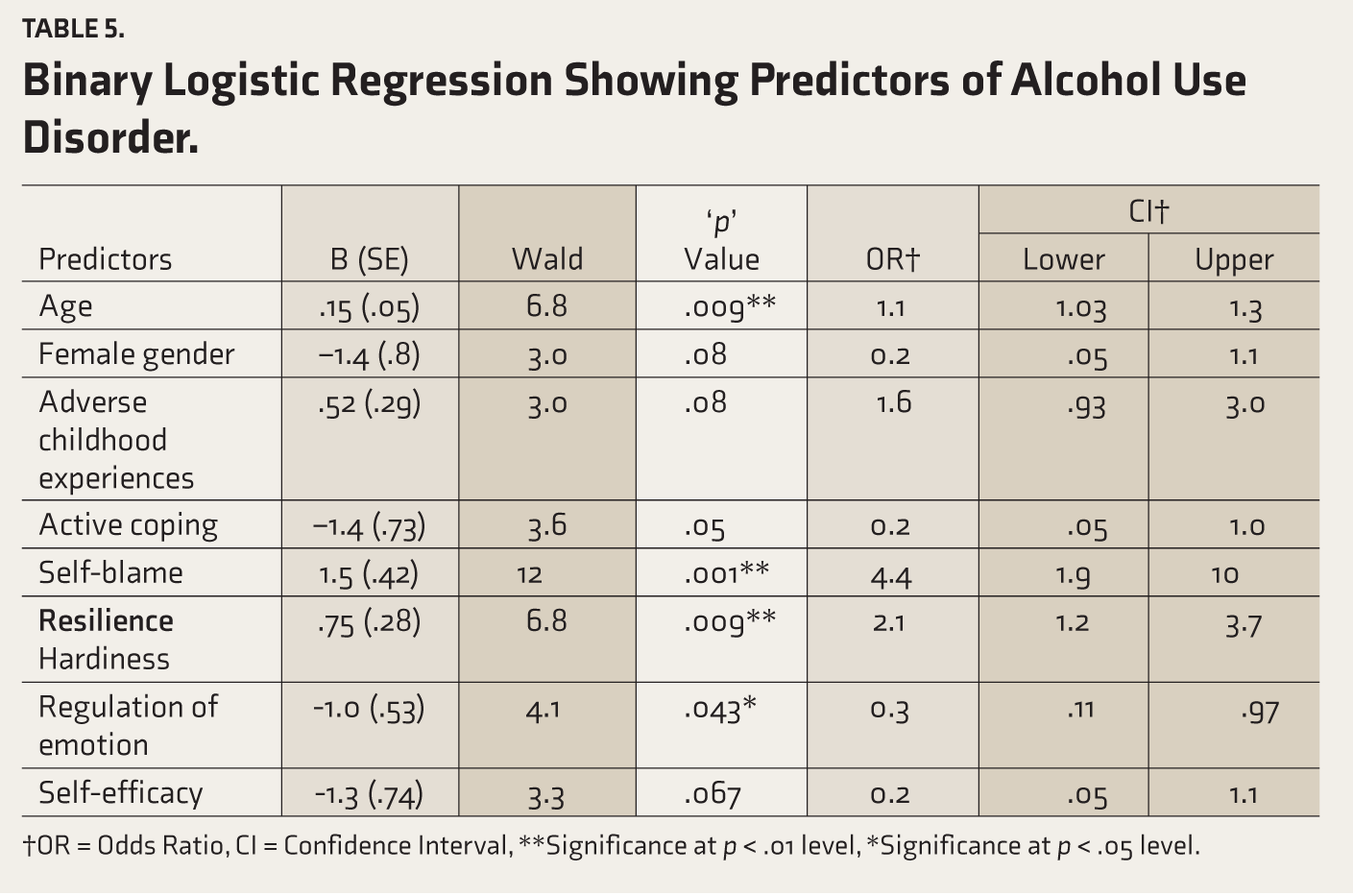
†OR = Odds Ratio, CI = Confidence Interval, **Significance at p < .01 level, *Significance at p < .05 level.
Discussion
The study aimed to examine the ACEs, coping, and resilience among persons with AUD and their unaffected siblings and healthy controls. We hypothesized that there would be no difference in ACEs, coping, and resilience among persons with AUD, their unaffected siblings, and healthy controls. We found that ACEs are higher among persons with AUD and their unaffected siblings when compared with healthy controls. Persons with AUD have more ACEs than their unaffected siblings, even though they share a similar environment. Persons may use alcohol and drugs to cope with traumatic childhood experiences and to relieve negative mood states, and physical, sexual and emotional abuse were positively correlated with higher substance use. 37
Previous studies reported similar findings that experiencing more adverse childhood events significantly increased the risk of developing AUD.37-41 and worsened mental health conditions like depression, anxiety, and stress disorders. Longitudinal studies have shown that these mental health conditions continue for longer periods and are less responsive to treatment and interventions.41,42 ACEs impair emotional, behavioural, logical thinking, and other cognitive aspects and thereby make people take up health risk behaviours, including alcohol and drug use. 42 ACEs are linked to alcohol use and substance use disorder.43-47 Persons with different mental illnesses have different levels of ACEs. Nearly one-third (26%) of persons with substance use disorders reported childhood adversities, which was higher than the other mental disorders (Obsessive Compulsive Disorder, Bipolar Affective Disorder, Schizophrenia, and Depression). Emotional abuse was predicted the severity of all psychiatric disorders. Higher childhood trauma was associated with more severity of mental disorders.47-49
Emotional and physical neglect was related to depression, anxiety, and stress. 50 There is strong evidence that ACEs increase the risk for SUD. Preventing ACEs leads to a 28% reduction in SUD, and Population-attributable risk proportions for SUD remain stable across countries and all life stages. 51
We found that avoidant coping is higher and approach coping is lower among persons with AUD when compared with their unaffected siblings and healthy controls. Previous studies reported similar findings that persons with AUD use avoidant approaches and multiple coping strategies (avoidance, substitution, distraction, and religious practices).10-20 More relapsed individuals use escapism and fatalism as coping strategies. Coping strategies differ between abstinent and relapsed alcohol dependents. Abstinent individuals used multiple coping strategies including optimism and interpersonal coping, avoidance, positive re-appraisal, self-control, and seeking support, use cognitive control, avoidance, distraction, seeking social support, and positive and negative thinking than relapsed individuals with AUD.51-60 These coping strategies are frequently used by younger persons with AUD more than older adults with alcohol dependence. 51 Well-motivated alcohol dependents use multiple coping behaviours to avoid relapse. 52 Persons with AUD attending an alcoholic anonymous group used coping strategies of positive thinking, whereas persons under de-addiction treatment used more avoidance, distraction, seeking social support, constructive use of leisure time, changing friends circle, involving more with family, and sharing their experiences.53-62
Present study findings indicate that resilience is lower among persons with AUD when compared with their unaffected siblings and healthy controls. It may be said that lower resilient individuals from high-density families are at risk for developing AUD. This finding is supported by a previous study that reported that substance users have lower resilience.29,63
An earlier study indicated that individuals with resilience have lesser chances of consuming alcohol. 64 Our study findings showed that lower resilience indicates a risk factor for AUD. An earlier study showed that resilience is strongly associated with reduced chances of using substances and protects individuals from alcohol consumption. 29 The lower resilience predicts substance use. Greater resilience decreases substance use and childhood trauma. 64 Individuals who were in sobriety for three or more months had shown higher resilience, which protected them from substance use. Another important finding is that social support is linked with resilience. 65 This study found that more female siblings did not develop AUD, as most male siblings developed AUD in families with a high density of alcohol use. Gender and cultural factors in coping and resilience would have prevented the female siblings from the development of AUD.
Limitations
The study results cannot be generalized owing to the different reasons. The AUD men and women were selected from a tertiary care government hospital and not from the community. However, healthy controls were selected from the southern part of a Bangalore metropolitan city. Hence, the sample selected was not a true representation of the universe. Most of the samples selected were from social class IV (upper lower socio-economic strata).
Conclusion
ACEs are more prevalent and more frequent in persons with AUD. Individuals with AUD showed higher avoidant coping and lower resilience than their non-drinking siblings and healthy controls. Early identification of ACEs and interventions to build resilience and coping strategies could prevent individuals from developing AUD in high-density families.
Footnotes
Acknowledgements
The authors would like to thank ADBS Collaborators and Dr. Mariamma Philip, Additional Professor, Department of Bio-Statistics for Sample size calculation and Regression Analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Institutional Review Board clearance has been obtained for the study.
Funding
Dept. of Bio-Technology, Govt of India, Grant No: BT/PR17316/MED/31/326/2015.
Informed Consent
Written informed consent was received from the participants prior to data collection.