
Abstract
Background:
Schizophrenia is a chronic severe mental illness with heterogeneous clinical presentation, course, and outcome. Cognitive impairment is one of its core features. Retinal nerve fiber layer (RNFL) imaging using OCT (optical coherence tomography) could provide easy access for in vivo imaging of the retina, rendering it as a “window to the brain.” Studies done on schizophrenia have shown RNFL thinning. This study attempts to look into the association between cognitive impairment, disease duration, and RNFL abnormality in patients with schizophrenia using OCT.
Methods:
Patients diagnosed with schizophrenia meeting DSM 5 (Diagnostic and Statistical Manual of Mental Disorders) criteria and who were confirmed to be in remission for at least six months clinically and scoring less than three on PANSS-8 (positive and negative symptom scale-8) remission scale were included. They were administered the Montreal Cognitive Assessment Scale (MoCA) for cognitive assessment. RNFL measures were taken using spectral domain-OCT. Variables were compared using Pearson’s correlation test, one-way ANOVA test, and independent t-test as appropriate.
Results:
A total of 36 patients were studied. MoCA scores and RNFL thickness showed a positive correlation. Patients with schizophrenia had reduced average RNFL thickness and reduced RNFL thickness in superior, inferior, and temporal quadrants. Average RNFL thickness, Superior and inferior quadrant RNFL thickness showed a positive correlation with MoCA scores. No correlation was obtained between macular volume, macular thickness, duration of illness, and MoCA scores.
Conclusion:
Patients with schizophrenia have reduced average RNFL thickness. Patients with low MoCA scores have RNFL thinning.
Keywords
Using a noninvasive, economical technique of optical coherence tomography we could study the degenerative pathophysiology of schizophrenia. Reduction in the retinal nerve fiber layer could be considered an endophenotype of schizophrenia. Retinal nerve fiber thinning is associated with higher-order cognitive impairment.Key Messages:
Schizophrenia is a chronic severe mental illness that is diagnosed based on clinical features like the presence of delusions, hallucinations, etc. It affects around 1 in 300 (0.32%) people around the world. The reported prevalence of schizophrenia in India is 0.5% (current) and 1.4% (lifetime). 1 Even with low prevalence, schizophrenia is placed in the 12th position in the Global Burden of Diseases by WHO. 2
Cognitive impairment is one of the core features of this disease and it causes considerable disability. Cognitive dysfunction ranges in different domains including attention, working memory, verbal learning and memory, and executive functions. Most of the patients with schizophrenia have one or more manifestations of cognitive dysfunction. The severity and type of these symptoms vary across patients. Many retrospective studies in schizophrenia show cognitive decline even in the premorbid stage of the disease. 3 The course of cognitive decline is dependent on multiple factors like the onset of symptoms, premorbid IQ, genetic factors, treatment, etc. 4 These may remain stable throughout or progressively deteriorate. 5 Recent neuroimaging studies have shown a reduction in brain volume which points to neurodegenerative processes. 6 There is also a significant decrease in white and gray matter volume over time. 7
Patients with schizophrenia experience changes in visual functions like distortions in size, form, color, visual hallucinations, and visual processing abnormality including a low level of functioning in contrast sensitivity. 8 Visual impairments including deficits in visual acuity and contrast sensitivity are seen in the prodromal phase of schizophrenia. 9 Few studies have shown that visual impairments are associated with the severity of disease and chronicity. Retinal pathology is predictive of the illness severity, progression, and cognitive impairments in neurodegenerative diseases like Alzheimer’s disease, Parkinson’s disease and diffuse Lewy body dementia. 10 The retina is a part of the central nervous system and grows out of the same tissue as the brain in early development. It shares receptors and neurotransmitters. There are anatomical similarities between retinal and cerebral vasculature and there is feedback signaling between them. This suggests a possibility of the study of the retina for disease prediction in schizophrenia.
Optical coherence tomography (OCT) is a noncontact non-invasive in vivo method of imaging the retina. A study done by Ascaso et al. using TD OCT showed significant thinning of the retinal nerve fiber layer (RNFL) in patients with schizophrenia when compared to controls. 11 Macular volume and thickness were commented on in different studies by Ascaso et al. in chronic patients. 12 The neurodegenerative etiology of schizophrenia was pointed out in the study by Lee et al. which showed the relation between RNFL thinning and duration of illness. 13 The study by Liu et al. showed the correlation between RNFL thinning and cognitive functions like visuospatial and immediate memory in the Chinese population. 14 This article is a study on retinal nerve layer abnormalities in schizophrenia using spectral domain (SD)-OCT which is superior to TD OCT. Our study aims to find the correlation between RNFL thickness and cognitive impairment and duration of psychosis. Through this, we may be able to arrive at new endophenotypes that can be easily assessed using a non-invasive method. There are only a few OCT-based studies in schizophrenia to date, thus our study is an attempt from India.
Materials and Method
Study Setting
Dept. of Psychiatry, Tertiary Care Center, Kerala.
Study Design
Cross-sectional study.
Study Sample, Procedure, and Tools
Patients between 18 and 50 years old with a diagnosis of schizophrenia (based on DSM 5 criteria) and on follow-up from the Psychiatry department between 2020 and 2021 were selected. Only those who were in remission for at least six months and had given consent were included for further data collection. The consultant Psychiatrist confirmed the remission status. Following this, PANSS-8 (Positive and Negative Symptom Scale-8 remission scale) was administered and a score of less than three on all eight items confirmed remission. 15 Patients with previous or concurrent systemic disease that may affect the eye, history of an ophthalmological or neurological disease known to affect the visual pathway, media opacification—such as cataract, corneal leukoma, or vitreous hemorrhage that may impede ocular or OCT examination, refractive errors over +2spheric diopters for hyperopic defects or -2spheric diopters for myopic defects, history of head injury with loss of consciousness, intellectual disability, and substance use were excluded. Fundus examination of each patient was done by an ophthalmologist before OCT to rule out optic disc cupping and any signs of glaucoma.
Sociodemographic details were collected on a data sheet developed and peer-reviewed for this purpose. Basic demographic variables and clinical variables like duration of illness, details of current medications, duration of remission, etc. were recorded. Montreal Cognitive Assessment Scale (MoCA 7.1 Malayalam version) was then administered. 16 Later these patients were taken up for OCT to assess the retina using SD-OCT (DRI OCT Triton plus-3D OCT).
The sample size was calculated using previous statistical data obtained as 35.1. 17 Hence the sample size for the study was approximately taken as 40. Soon after the start of data collection, COVID-19 hit the state and many patients on regular follow-up did not turn up. Hence, the study could recruit only 36 patients. Institutional ethics and Research committee approvals were obtained before recruiting study subjects. All the data were entered in MS Excel sheet version 10. Data was loaded to SPSS version 18 and analyzed. The socio-demographic data obtained are described as means and standard deviation for continuous variables and frequency and proportions for categorical data. The relationship between MoCA scores and RNFL thickness, macular volume, and thickness was analyzed using Pearson’s correlation test. The study variables are MoCA scores, RNFL thickness, macular thickness, macular volume, and duration of illness.
Results
Demographic and Clinical Characteristics
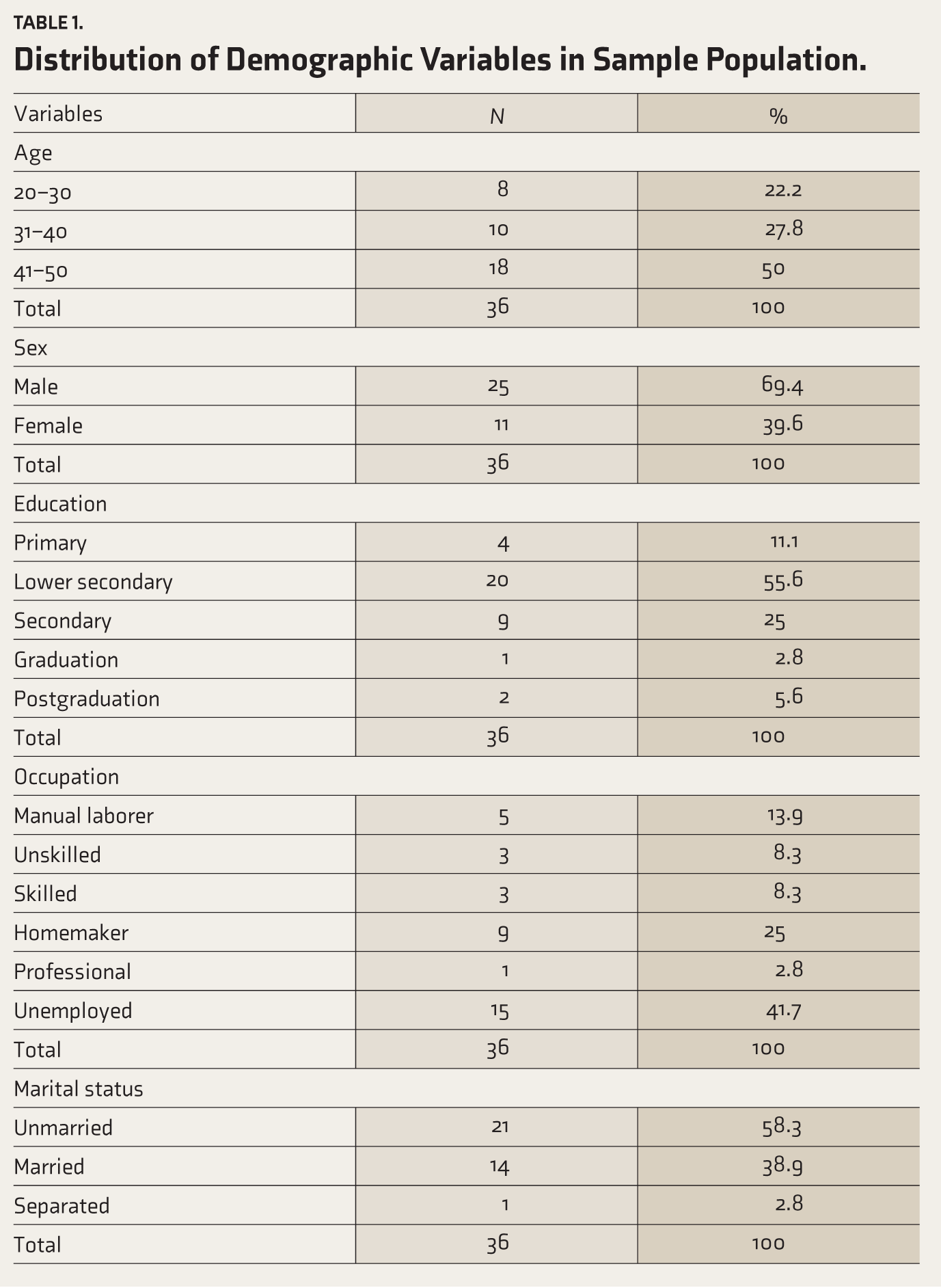
Table 1 shows the demographic details of the study population. The total duration of illness ranged between 5 and 30 years in the study population. Duration of remission ranged from 8 to 36 months.
Distribution of Demographic Variables in Sample Population.
MoCA Scores
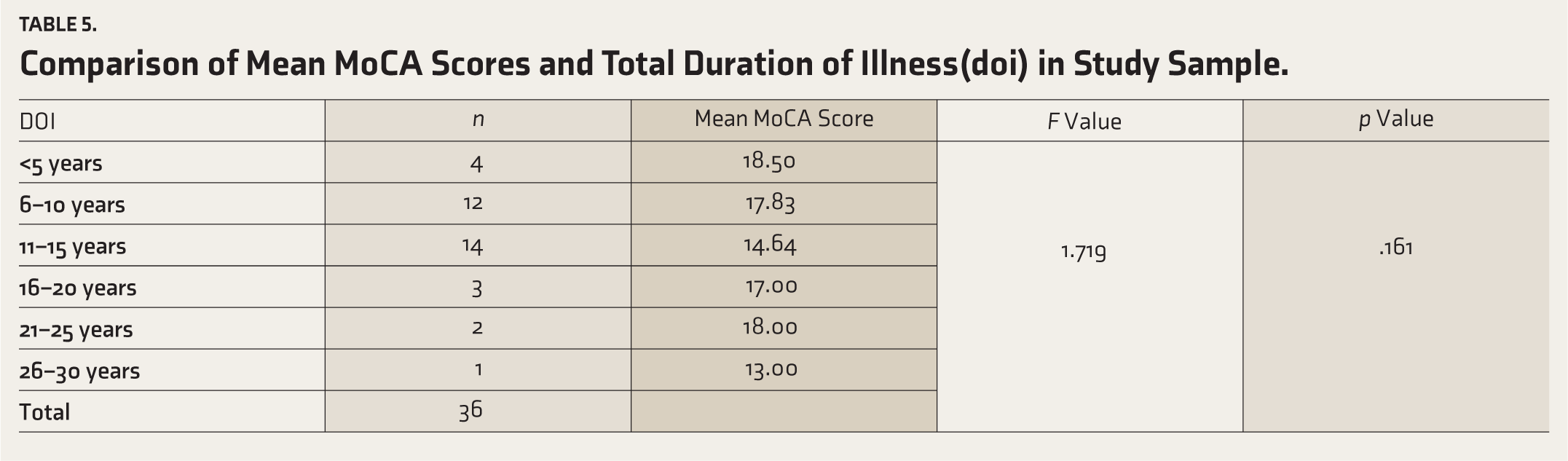
MoCA scores ranged between 11 and 23 with a mean of 16.7 (SD = 3.67). One-way ANOVA showed no significant association of MoCA scores with the duration of illness (F value = 1.832; p = .161) and level of education (F value = 1.719; p = .148) (Table 2). MoCA scores also had no correlation with age (p = .233), and the period of remission (p = .272) (Table 3). An Independent sample t-test was applied to assess any relation between MoCA scores and antipsychotics that patients were taking, which showed no statistical association between them.
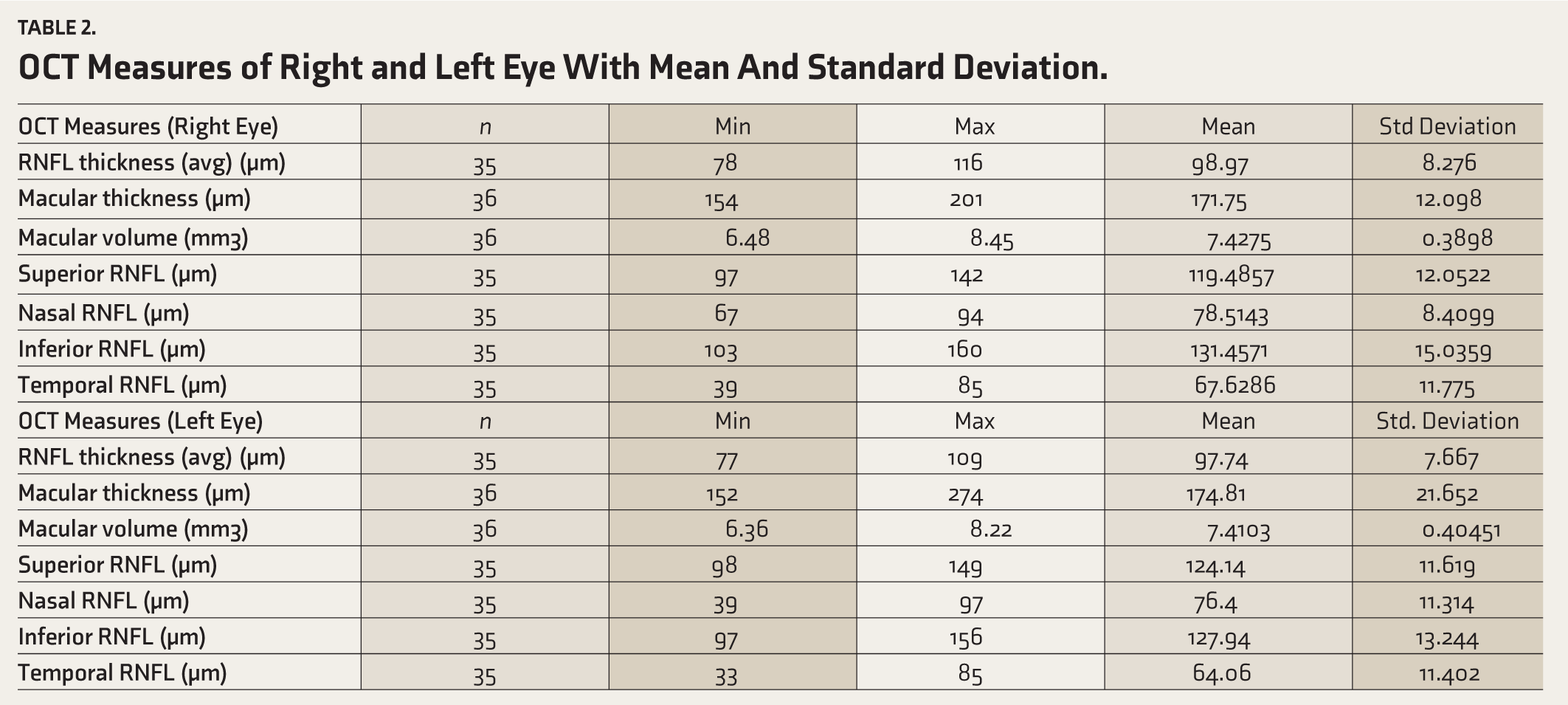
OCT Measures of Right and Left Eye With Mean And Standard Deviation.
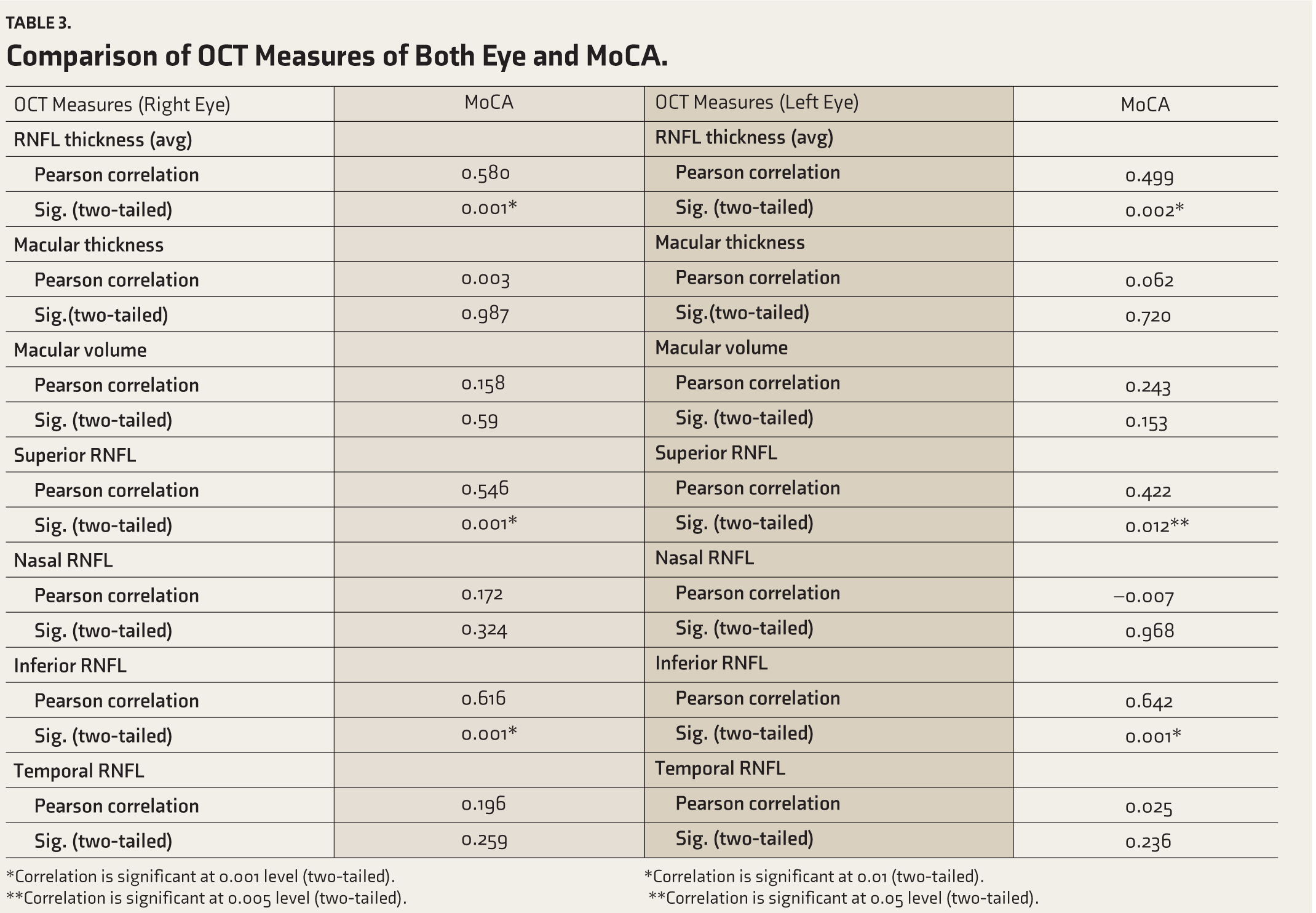
Comparison of OCT Measures of Both Eye and MoCA.
*Correlation is significant at 0.001 level (two-tailed).
*Correlation is significant at 0.01 (two-tailed).
**Correlation is significant at 0.005 level (two-tailed).
**Correlation is significant at 0.05 level (two-tailed).
OCT Measures
Table 4 shows the OCT measures of the right and left eye which include mean values of RNFL thickness, macular thickness, and macular volume. RNFL values of the right eye of one of the patients and the left eye of another patient could not be obtained due to technical reasons. Means values of RNFL thickness, macular thickness, and macular volume of right and left eyes in the study sample were comparable. RNFL was assessed in four quadrants namely superior, nasal, inferior, and temporal for each patient.
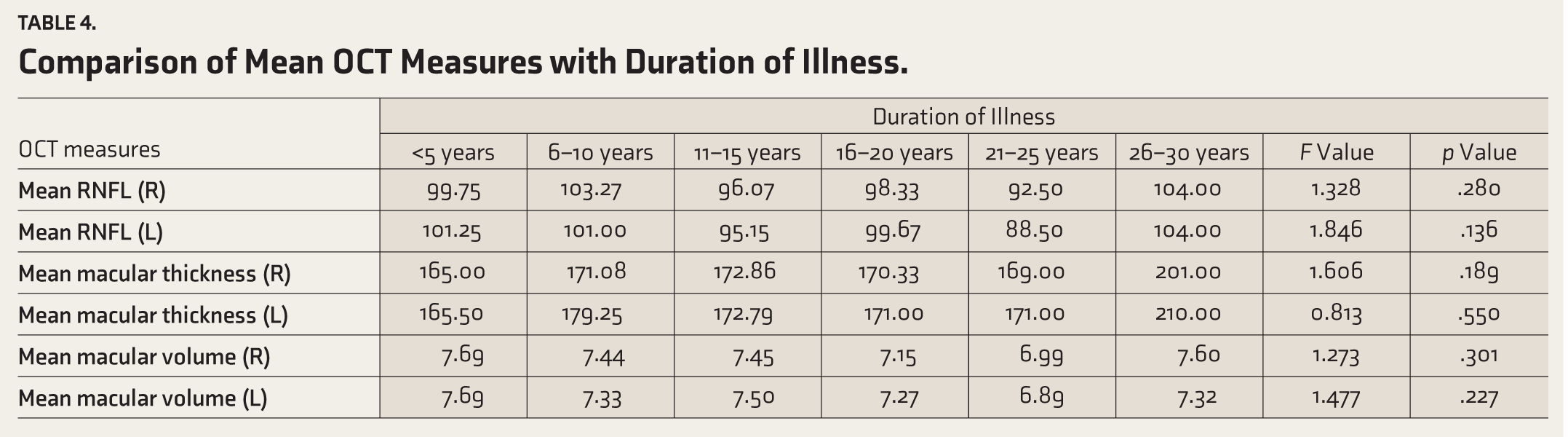
Comparison of Mean OCT Measures with Duration of Illness.
OCT Measures and MoCA
Table 5 shows the association between OCT measures and MoCA scores in the study sample. Pearson correlation test was used to look at the relation between OCT measures of both eyes and MoCA scores. There was a significant positive correlation between the average RNFL thickness of both eyes and MoCA scores. A positive correlation was obtained between the superior and inferior quadrants of RNFL of the right and left eye with MoCA scores. Figure 1 shows a positive correlation between MoCA scores and the average RNFL thickness of both eyes. No correlation was obtained for macular volume or macular thickness with MoCA scores.
Comparison of Mean MoCA Scores and Total Duration of Illness(doi) in Study Sample.
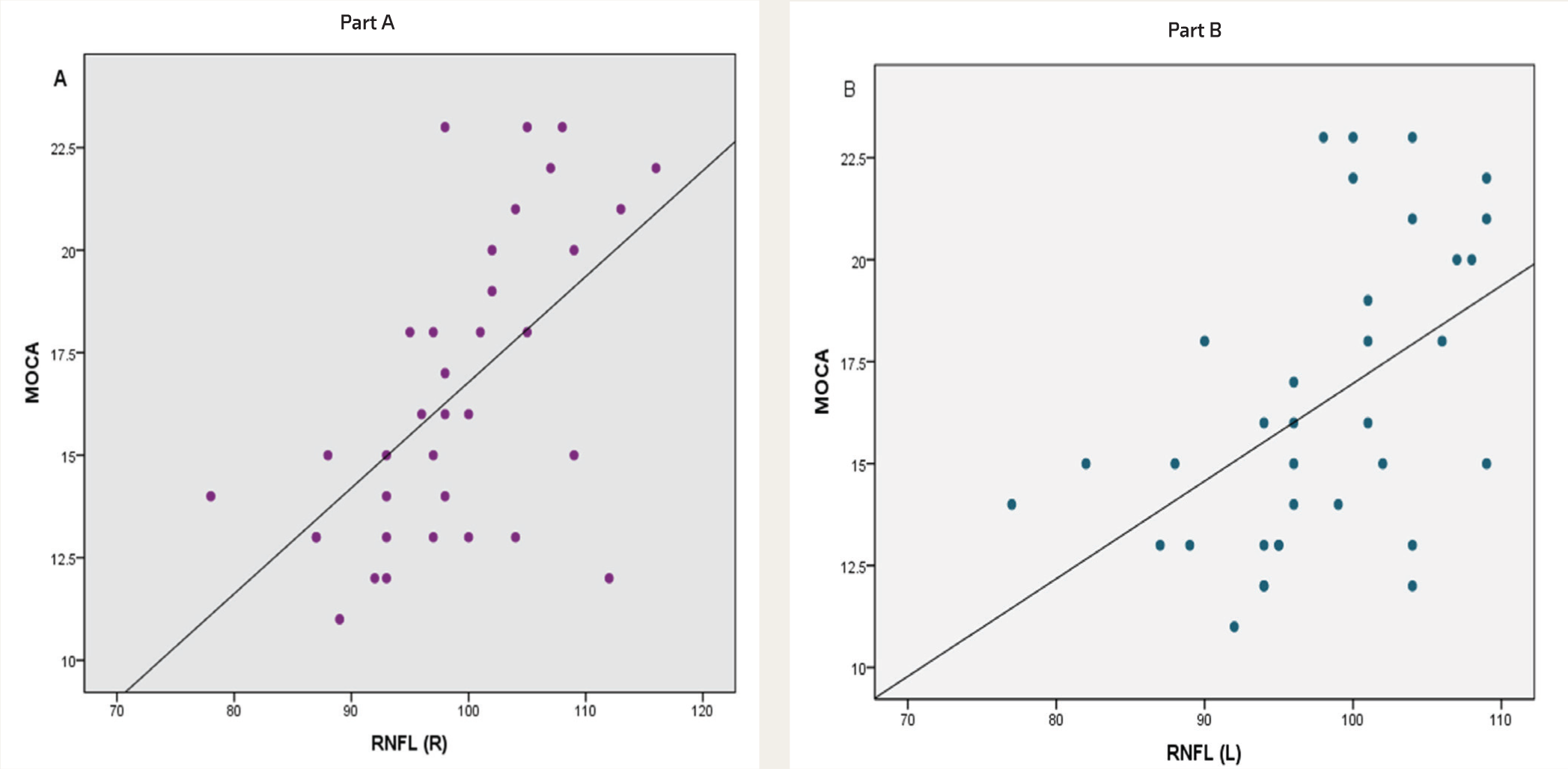
Part A shows positive correlation between MoCA scores and Avg RNFL thickness of right eye.
OCT Measures and Duration of Illness
One-way ANOVA was done to find an association between RNFL thickness, macular thickness, and macular volume with duration of illness. No significant association was obtained between the variables. Table 6 shows the above results. Pearson correlation showed no correlation between OCT measures and duration of illness (p = .243, .187, .118, .448, .060, .059).
Comparison of Remission and Age with MoCA Scores.
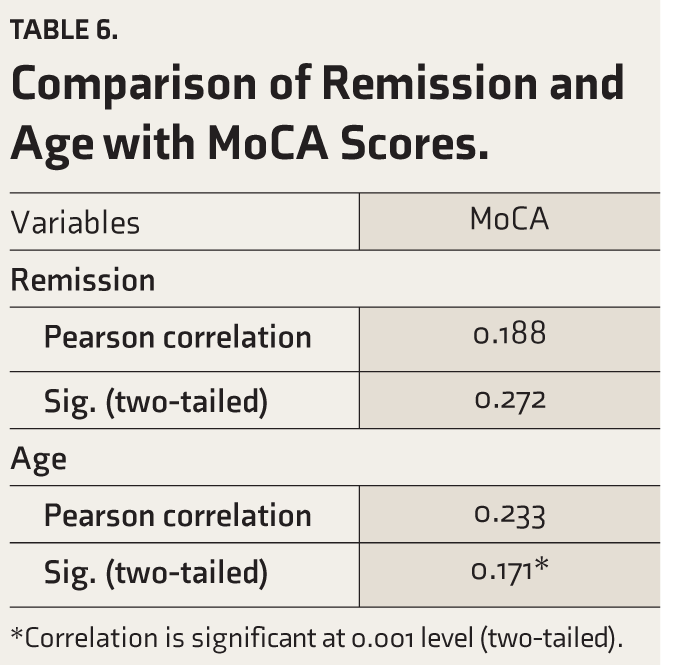
*Correlation is significant at 0.001 level (two-tailed).
Discussion
A total of 36 patients with schizophrenia with remission of more than six months were taken up for cognitive screening by MoCA and later OCT was done to study the RNFL thickness, macular volume, and macular volume. In our study, we found that 41.7% of patients were unemployed even though they all were in remission. They had difficulty maintaining full-time jobs, maintaining a relationship, and taking up responsibilities in the family. Overall, 58.4% of the sample were unmarried pointing to the same fact.
All the patients scored less than 26 in MoCA, the highest was 23, and the lowest was 11, indicating a cognitive impairment in all of them. Even after remission of positive and negative symptoms, cognitive symptoms remain in the patient which in turn affects the functional outcome of the patient. A study by Green et al. had found specific cognitive domains related to functional outcomes in schizophrenia. Card sorting, verbal memory, vigilance, and verbal fluency were found to be the cognitive domains mostly affecting the community outcome and activities of daily living, social problem-solving and instrumental skills, and psychosocial skills. 18 Most of the patients in our sample scored less in visuospatial tests, attention, concentration, verbal (semantic) fluency, abstraction, and delayed recall which was comparable to the study by Green et al. The same study showed that cognitive impairment is independent of the duration of psychosis and our study also showed similar results. Further, a study conducted on the longitudinal course of cognitive impairment noted cognitive impairment even before the onset of illness. 3 Our study observed no relation between cognitive impairment and the period of remission of symptoms.
We observed that patients with high MoCA scores had higher levels of education but cognitive impairment and level of education showed no association in our study. This differs from an earlier study done by Rannikko et al. that noted that premorbid school performance is an endophenotype for schizophrenia. 19
A thinning of RFNL was observed in our study sample. A study conducted by Liu et al. in the Asian population has shown thinning of the RNFL in a patient with schizophrenia. 14 The mean average of RNFL thickness in our study was obtained as 98.97 µm (right eye) and 97.74 µm (left eye) which is low compared to values obtained in the Handan eye study. 20 The Handan eye study gives us an extensive comparison of RNFL thickness in different age groups and mentions about other similar studies conducted in various parts of the world. It is a population-based cohort study done in the rural Chinese population. The study gives the average thickness of RNFL for <39 years as 115.22 + -10.88 µm and 115.90 + -10.25 µm for the 40–49 years of age group. Similar studies have been done in the Indian population which shows an average RNFL thickness of 101.07 µm. 21 Another study by Sony et al. in the Indian population showed an average RNFL thickness of 104.27 µm. 22 Thus, we can conclude that RNFL thickness is decreased in patients with schizophrenia in our study. The neurodegenerative course of schizophrenia has been an ongoing debate since Kraepelin. 23 The RNFL consists of unmyelinated fibers which are the first axons of the visual pathway; also from an embryological point of view, these fibers could be considered an extension of the brain.
Dopamine dysregulation is involved in positive and negative symptoms in patients with schizophrenia. Dopamine is one of the major neurotransmitters of the retina and is synthesized in subsets of amacrine cells. Amacrine cells are involved in lateral connectivity and integrate signals from bipolar cells to ganglion cells. One of the major functions of amacrine cells is the adaptation of the retina according to environmental stimulus, motion sensitivity, and color sensitivity. Dopaminergic deficiency could lead to the destruction of amacrine cells which causes abnormalities in visual processing. 24 It could be concluded that dopamine dysregulation not only causes functional deficits but also structural deficits. 13 Based on these findings studying the RNFL could be considered a marker for degeneration of the brain. Therefore a significant reduction of retinal fiber layer thickness could be proposed as a biomarker for schizophrenia. 12
There was a significant reduction in superior, inferior, and temporal quadrants of the peripapillary RNFL when compared to the average quadrant values in the Handan eye study. Figure 2 shows the SD-OCT results of one of the patients in our sample showing a significant reduction in the temporal quadrant of the RNFL. Superior and inferior quadrants are composed of magnocellular cells whereas the temporal quadrant is composed of parvocellular cells. A study by Butler and Javitt had shown deficits in visual-evoked potentials and behavioral tests in patients with schizophrenia implying that a selective impairment of the magnocellular pathway is responsible for object motion and assessing spatial relationships. 25 There is a defect in motion processing in schizophrenia indicating a defective magnocellular response. A study conducted using ssVEP (steady-state visual-evoked potentials) showed decreased activity of the magnocellular pathway in patients with schizophrenia. 26 Thus, reduction in superior and inferior quadrants of RNFL could be considered as an endophenotype of schizophrenia.
Spectral Domain Optical Coherence Tomography (SD-OCT) Result of One of the Patients in Our Study Sample Showing Decreased Peripapillary RNFL Thickness in Temporal.

The black line shows retinal nerve fiber layer (RNFL) measures for each quadrant (N = nasal, S = superior, T = temporal, I = inferior). The colors represent normal distribution percentiles where, green = 95-5%, yellow = 5-1%, red = 1-0%.
The significant correlation between the average thickness of RNFL and MoCA scores shows that patients with more thinning RNFLs have a higher degree of cognitive impairment. A positive correlation was noted between the superior and inferior quadrants of RNFL and MoCA scores. The results are similar to a study conducted by Lee et al. which examined 30 patients and 30 controls using SD-OCT and found a decreased peripapillary RNFL thickness, as well as a reduction in macular volume and macular thickness in patients relative to the controls. 13 All quadrants except the nasal one were affected by the thinning of the RNFL.
Superior and inferior quadrants of RNFL consist of magnocellular cells. Perceptual and cognitive dysfunction including impairment in visual attention in schizophrenia is been related to deficits in the early stages of sensory/perceptual processing, particularly within the magnocellular/dorsal visual pathway. A study using fMRI and VEP (visual-evoked potential) showed early visual processing dysfunction in schizophrenia with preferential deficits being found in the magnocellular pathway. 27 Behavioral and electrophysiological studies done in the past show defects both in magnocellular and parvocellular pathways with more defects in magnocellular pathways. 27 Thus we can conclude that superior and inferior quadrant RNFL thinning could be associated with higher-order cognitive deficits.
The study by Lee et al. found an inverse correlation between the duration of illness and RNFL thickness, 13 which our study did not. In our study, we have not included patients of age more than 50 years which could have be a confounding factor while assessing the RNFL thickness. However, the study by Ascaso et al. has found no association between the duration of illness and RNFL thickness necessitating further study to examine this association. 12
This study shows that the RNFL thickness was significantly reduced in patients with schizophrenia. The superior, inferior, and temporal quadrants of RNFL thickness were reduced in patients with schizophrenia. There is a relationship between RNFL thickness and cognitive impairment. The study also throws evidence that superior and inferior quadrant RNFL thinning could cause higher-order cognitive deficits. Currently, only very few studies are available based on OCT in schizophrenia. Among them, most of the studies have found a reduction in the RNFL in these patients except for the study conducted by Chu et al. in 2012 28 and Topcu-Yilmaz et al. in 2019. 29 Our study was limited by the reduction in sample size, due to COVID-19 and the fact that no structured tools were used to diagnose schizophrenia. The use of antipsychotics could also influence the RNFL thickness which is another limitation of our study. Therefore larger studies with robust methodologies are needed to confirm the observation that retinal nerve fiber thinning, could be taken as an endophenotype of schizophrenia.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was conducted after approval from Institutional Ethics Committee, Government Medical College, Kozhikode, Ref. No.:GMCKKD/ RP 2020/IEC/520.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.