
Abstract
Background:
Neurocognitive deficits are well-documented in patients of schizophrenia and their first-degree relatives (FDRs). Metacognitive awareness of these deficits, called neurocognitive insight (NI), has been found to be poor in schizophrenia patients but has not been assessed in their FDRs. This study evaluated NI and its relationship with objective cognitive performance, a history of psychotic experiences (PEs), and social functioning in unaffected FDRs.
Methods:
This cross-sectional study was conducted at the outpatient department of a tertiary care teaching hospital. A total of 100 FDRs were assessed for PEs and evaluated for subjective cognitive complaints (SCC), objective cognitive performance, and social functioning using the Subjective Scale to Investigate Cognition in Schizophrenia, neurocognitive tests from the National Institute of Mental Health and Neurosciences battery, and SCARF Social Functioning Index, respectively.
Results:
Compared to normative data, episodic memory was the most commonly impaired domain (up to 72% of participants), followed by working memory, attention, and executive function. There was no correlation between SCC and neuropsychological test scores in the corresponding cognitive domains, implying poor NI. 15% of participants had a lifetime history of PEs. This group had significantly higher SCC as compared to those without PEs (U = 0.366, P = 0.009, r = 0.26). A regression analysis showed that the FDRs’ social functioning reduced by 0.178 units for each unit increase in SCC [F (1,98) = 5.198, P = 0.025].
Conclusion:
Similar to schizophrenia patients, FDRs also have poor NI. The severity and progression of SCC could be explored as a possible marker for screening and monitoring FDRs at an ultrahigh risk for psychosis. Importantly, even in unaffected FDRs, SCC could affect socio-occupational functioning and need further research.
Keywords
FDRs of schizophrenia patients have poor self-awareness of their cognitive deficits. FDRs who experience PEs have higher SCC as compared to those who do not. SCC could be explored as a marker for monitoring FDRs at a high risk of psychosis.Key Messages:
A lack of insight into illness is considered one of the characteristic features of severe mental illnesses such as schizophrenia. 1 Traditionally, this concept was used to explain a poor self-assessment or an “unawareness” regarding psychotic symptoms and was mainly explored in the context of positive symptoms (such as delusions, hallucinations, and thought disorder), negative symptoms (such as asociality and anhedonia), and general insight into illness.2,3 Subsequent research demonstrated that the “unawareness” was not just restricted to cardinal symptoms of the illness but affected various neuropsychological domains that were a part of everyday functioning. Recently, this impairment in self-assessment has also been conceptualized for deficits in social cognition (“I am bad at guessing if somebody looks sad or not”) and neurocognition (“I am bad with phone numbers”).4,5 Insight is now understood as a multidimensional construct mediated by a complex interaction between neurocognition, metacognition, and social cognitive abilities.6–8 Among these, the concept of metacognition particularly helps in understanding insight because the self-awareness is essentially of an introspective and autobiographical nature. 9
Metacognition involves cognitive processes that refer to, monitor, or control any aspect of cognition and is commonly referred to as thinking about thinking.10,11 Hence, for patients of schizophrenia who are known to suffer from neurocognitive deficits, 12 their metacognitive ability to be aware of these deficits effectively helps in knowing the limits of one’s cognitive resources. 4 This knowledge helps analyze the task at hand and direct one’s resources to perform the task with maximal efficiency. 8 For example, an individual who is aware that he has difficulty with remembering phone numbers might maintain a diary for noting them.
Early studies assessing a metacognitive awareness of cognitive deficits in individuals with schizophrenia showed that their self-evaluation of cognitive deficits (hereafter referred to as subjective cognitive complaints, SCC) did not match with the objective findings of an assessment using neuropsychological tests, indicating a poor self-awareness of their cognitive status.13,14 In other words, while patients did complain of cognitive deficits, they did not seem to have a clear representation of its nature and extent. This entity was labeled as neurocognitive insight or NI—defined as an awareness of neuropsychological dysfunction. 15 Subsequent research has confirmed these findings16,17 and has also demonstrated NI to be independent of the severity of psychosis and even the level of insight into the mental illness (clinical insight).18,19 A meta-analysis of 22 studies assessing NI in 1609 schizophrenia patients has also shown a weak association between subjective and objective cognition. 20
While there has been a lot of research on NI in schizophrenia, the literature on NI in unaffected first-degree relatives or FDRs of patients (biological children or siblings) is sparse. FDRs have a shared biological vulnerability and are considered to be at a familial high risk (up to 10 to 15 times) for the development of schizophrenia. 21 Those experiencing attenuated forms of the positive symptoms or “psychotic experiences” (PEs) 22 have been particularly found to be at a higher risk of conversion to psychosis.23–26
It is now established that otherwise healthy FDRs also suffer from subtle deficits in neurocognitive, metacognitive, and neurophysiological parameters similar to those in schizophrenia patients. These are considered as “trait markers” and have been labeled as endophenotypes.27,28 However, these are thought to be more subtle as compared to those in schizophrenia patients. For example, it is now known that FDRs also suffer from deficits in neurocognition.29–31 Deficits have been prominently noted in attention, executive function, processing speed, verbal learning, and memory. 32 Similarly, metacognitive deficits such as those in theory of mind have also been demonstrated in FDRs.33–35 However, studies exploring a metacognitive awareness of neurocognitive deficits in FDRs are lacking.
Hence, the current study was planned to assess if FDRs had NI regarding their neurocognitive deficits. We hypothesized that FDRs would have poor NI similar to schizophrenia patients, judged by a lack of correlation between SCC and objective cognitive performance on neuropsychological tests. Because persistence and severity of PEs can be a pointer toward a high possibility of future conversion to frank psychosis, we wanted to assess whether there was an association between SCC and a history of PEs in FDRs. Lastly, it is also not known whether having a metacognitive awareness of cognitive deficits alters the functioning of FDRs in any way. Hence, we wanted to explore whether there was a relationship between SCC and social functioning.
Materials and Methods
The study was approved by the Institutional Ethics Committee (ECARP/ 2016/182). A cross-sectional study was conducted at BYL Nair Charitable Hospital, which is a tertiary care teaching hospital in Mumbai, India between 2017 and 2018. Unaffected FDRs (biological siblings or children) of patients diagnosed with schizophrenia as per Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) by a qualified psychiatrist were approached in the psychiatry outpatient clinic during their visit with the patients. While there are differences in vulnerability to psychosis between siblings and children of schizophrenia probands, previous studies have not shown any differences in the severity of cognitive deficits between these two groups of FDRs. 31 Hence, both these groups of FDRs were approached. Also, because there are no prior prevalence studies on subjective cognition and NI in FDRs, we employed a purposive sampling method for recruiting subjects. Sampling was conducted over six months, and only one subject (biological sibling/child) was recruited from the family of each proband.
All participants met the following inclusion criteria: (a) aged between 18 and 50 years; (b) spoke English, Hindi, or Marathi; (c) educated till at least the fifth grade; and (d) had adequate hearing and visual abilities. The exclusion criteria were as follows: (a) a current or a lifetime diagnosis of a major psychiatric disorder based on an interview as per DSM-5 criteria; Those fitting the diagnostic criteria of schizophrenia/ other psychotic disorders or mood disorders with psychotic symptoms as per DSM-5 criteria were excluded from the study. Those giving a history of visiting a healthcare professional for these symptoms and/ or getting treated were also excluded; (b) a current or a lifetime history of any medical illness that can impair neurocognition such as (but not limited to) hypothyroidism, hypertension, cerebrovascular diseases, as per the history or clinical examination; (c) any significant history of a head injury with loss of consciousness or documented cognitive sequelae; (d) clinically diagnosed mental retardation; and (e) a concurrent diagnosis of substance dependence (other than nicotine). Participants were recruited based on these criteria.
Assessment of the Participants
Prospective participants were assessed during their visit to the outpatient clinic. Written informed consent was then obtained by an investigator of the research team from those fitting the inclusion criteria. Sociodemographic and occupational details were recorded in a semi-structured pro forma.
The National Institute of Mental Health and Neurosciences (NIMHANS) neuropsychological battery was used to assess neurocognitive performance. It is a comprehensive tool consisting of popular neuropsychological tests adapted and standardized for the Indian population. 36 From the battery, Digit Vigilance Test assessing attention, 37 verbal N-back test assessing working memory, 38 Stroop test assessing executive functions (cognitive flexibility, processing speed, and response inhibition), 39 and logical memory passage/passages test assessing episodic memory40–42 were used. The scores on neuropsychological tests were compared to appropriate Indian normative data as per age, gender, and education, and then percentile scores were calculated. Neuropsychological tests including the NIMHANS neuropsychological battery generally employ 1 SD as the cutoff for detecting a significant cognitive impairment. Additionally, using a dimensional approach, the DSM-5 has categorized the cognitive impairment in schizophrenia into “equivocal” (within 0.5 SD from the mean), “mild” (0.5–1 SD from the mean), “moderate” (1–2 SD from the mean), and “severe” (>2 SD from the mean) based on the scores on neuropsychological tests. 43 Hence, in the current study, the number of FDRs with a cognitive impairment were calculated based on all three cutoffs—0.5 SD, 1 SD, and 2 SD from the mean.
Subjective Scale to Investigate Cognition in Schizophrenia (SSTICS) was used to evaluate SCC. It is a 21-item questionnaire used to examine SCC in both clinical and nonclinical populations and has been validated in Hindi and Marathi for use in the Indian population. 44 SSTICS asses not the cognitive deficits itself but the self-awareness of problems in working memory, explicit memory (comprising of episodic and semantic memory), attention, executive function, language, and praxis. A global score between 0 and 84 is computed, with higher scores signifying higher SCC. 13
To explore the history of PEs, participants were interviewed by two qualified psychiatrists. The interview was focused on establishing a history of two types of hallucinatory experiences (auditory and visual) and four types of delusional experiences (thought insertion/withdrawal, mind control/passivity, ideas of reference, and plot to harm). 45 If the participants gave a positive reply, they were then asked to elaborate on the same to rule out any association with sleep or substance use. Once these causes were ruled out, individuals who reported to have experienced any one of these were considered to have had a PE.46,47
Schizophrenia Research Foundation India-Social Functioning Index (SSFI) was used to evaluate social functioning. It is a 17-item scale that assesses social functioning in the domains of self-care, occupational role, role in the family, and other social roles. 48 It has a total score of 85, with higher scores signifying better social functioning.
An assessment of PEs, SCC (SSTICS), and the level of social functioning (SSFI) was done, followed by a neuropsychological assessment (NIMHANS neuropsychological battery). All assessments were done in a single sitting by two of the investigators who were psychiatrists and had received training in neuropsychological testing. The entire process was done in a fixed sequence in a quiet room.
Statistical Analysis
A statistical analysis was performed using the SPSS version 20 software for Windows (IBM Corp., Armonk, NY). For the comparison of scores on scales/tests between groups, an independent t-test or a Mann–Whitney U-test was used based on the distribution of the scores. A correlation between SSTICS, SSFI, and neuropsychological test scores was analyzed using Pearson’s or Spearman’s correlation coefficient. Based on the results of the correlation analysis, a simple linear regression was performed. The significance level was set at 0.05. In case of any missing data related to the aforementioned tests/scales, it was decided to not include those participants in the final analysis.
Results
Of 145 FDRs were approached, of whom 45 could not be enrolled because of various reasons such as not fitting the educational or language criteria, the presence of comorbid medical or psychiatric conditions, and the refusal of consent. Excluding these, 100 FDRs met the inclusion criteria and consented to be a part of the study. Table 1 summarizes the sociodemographic characteristics of the participants. Because there was no missing data, all 100 participants were taken for the final analysis.
Characteristics of the Participants
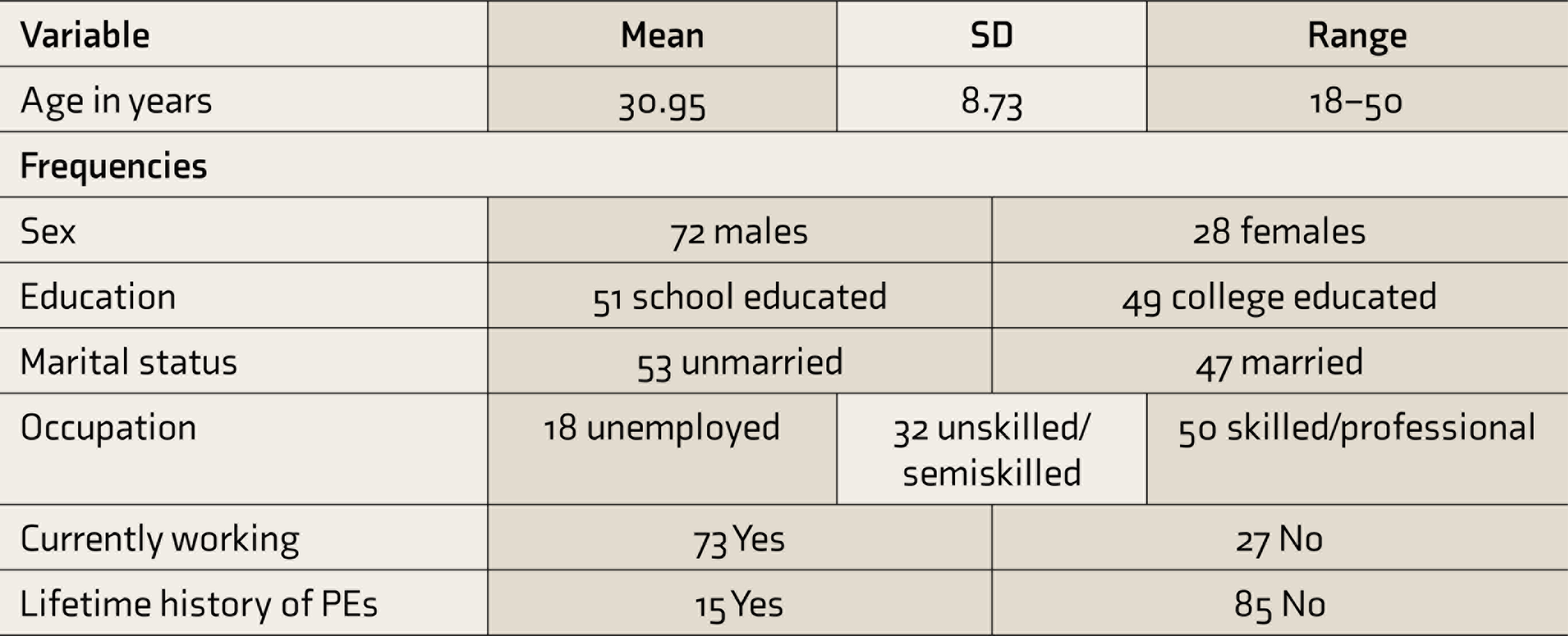
PE, psychotic experience.
The mean age of the participants was 30.95 years (ranging from 18 to 50 years), signifying a young-age group. They were fairly well educated, with 49% being college educated (above the tenth grade), while the rest were school educated (till the tenth grade). 18% were unemployed. However, 27% were not working at the time of assessment. 15% participants reported a lifetime history of at least one type of PEs, with delusional experiences (11%) being more commonly reported than hallucinatory (7%). 12 out of these 15 FDRs were in the 18-30 age group, had experienced psychotic experiences within the last one year. Table 2 describes the mean scores on the different assessment tools along with the standard deviation and range.
Scores of Subjective Cognition, Neuropsychological Assessment, and Social Functioning
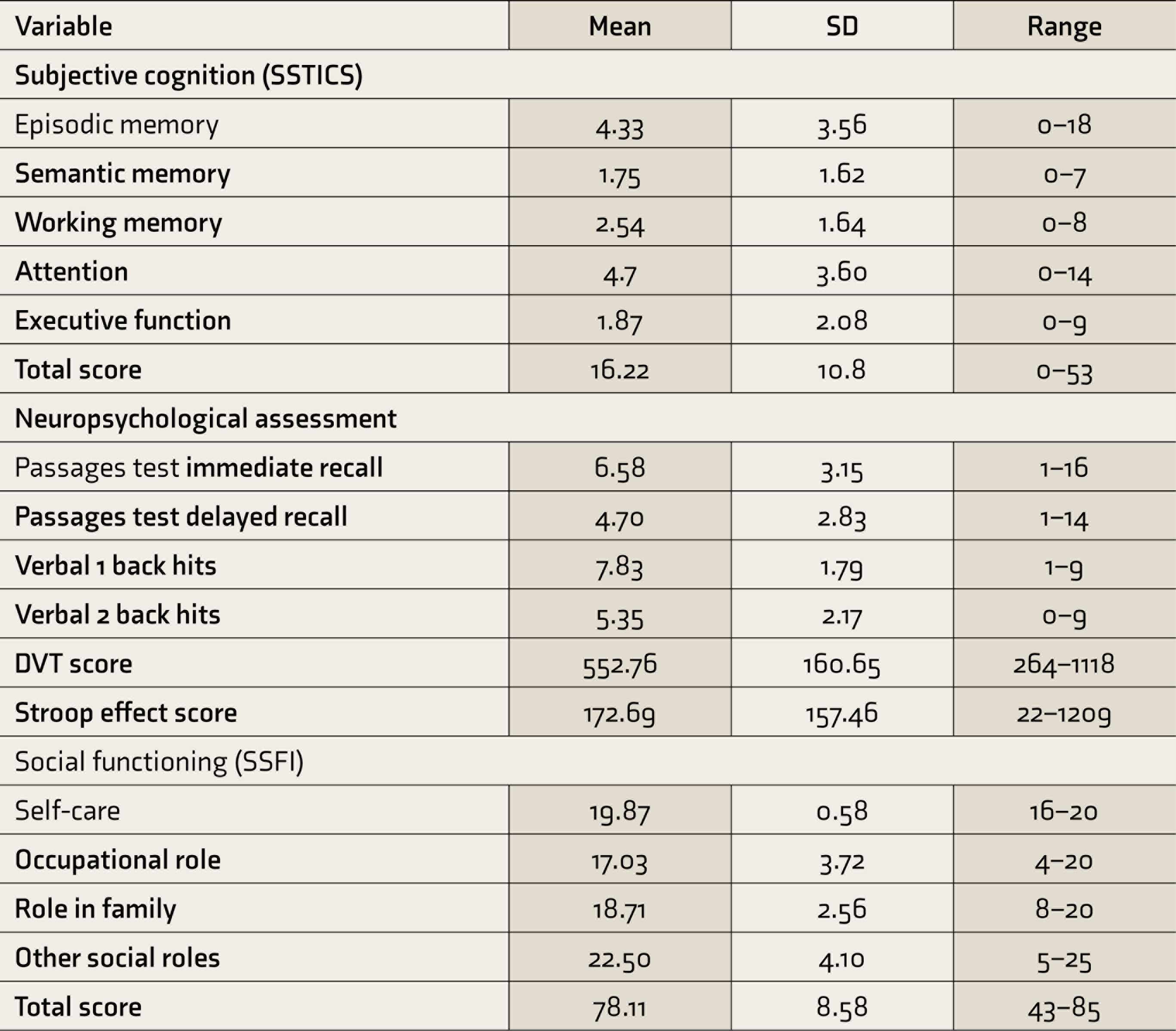
SSTICS, Subjective Scale to Investigate Cognition in Schizophrenia; DVT, Digit Vigilance Test; SSFI, SCARF Social Functioning Index.
Objective Cognitive Performance and Its Relation to Subjective Cognitive Complaints
When 0.5 SD was used as the cutoff for ‘mild’ cognitive impairment, 85% and 94% showed impairment in episodic memory, followed by working memory (52% and 74%), attention (37%), and executive function (34%). Using the 1 SD cutoff for ‘moderate’ impairment, 64% and 72% FDRs were found to have impairment in episodic memory, followed by working memory (24% and 32%), attention (23%), and executive function (18%). Using the 2 SD cutoff signifying a ‘severe’ cognitive impairment, 39% and 51% FDRs showed impairment in episodic memory, followed by working memory (18% and 23%), executive function (6%), and attention (4%). Spearman’s rank correlation demonstrated no relationship between neuropsychological test scores and SSTICS scores of corresponding cognitive domains, implying poor NI (Table 3). The only positive relationships seen were between verbal 1 back hits score and SSTICS semantic memory subscale (rs = –0.199, P = 0.047), and between verbal 1 back hits score and SSTICS executive function subscale (rs = –0.205, P = 0.040), implying that worse the working memory, higher are the SCC regarding semantic memory and executive function.
Correlation Between Subjective Cognitive Complaints and Objective Cognitive Performance
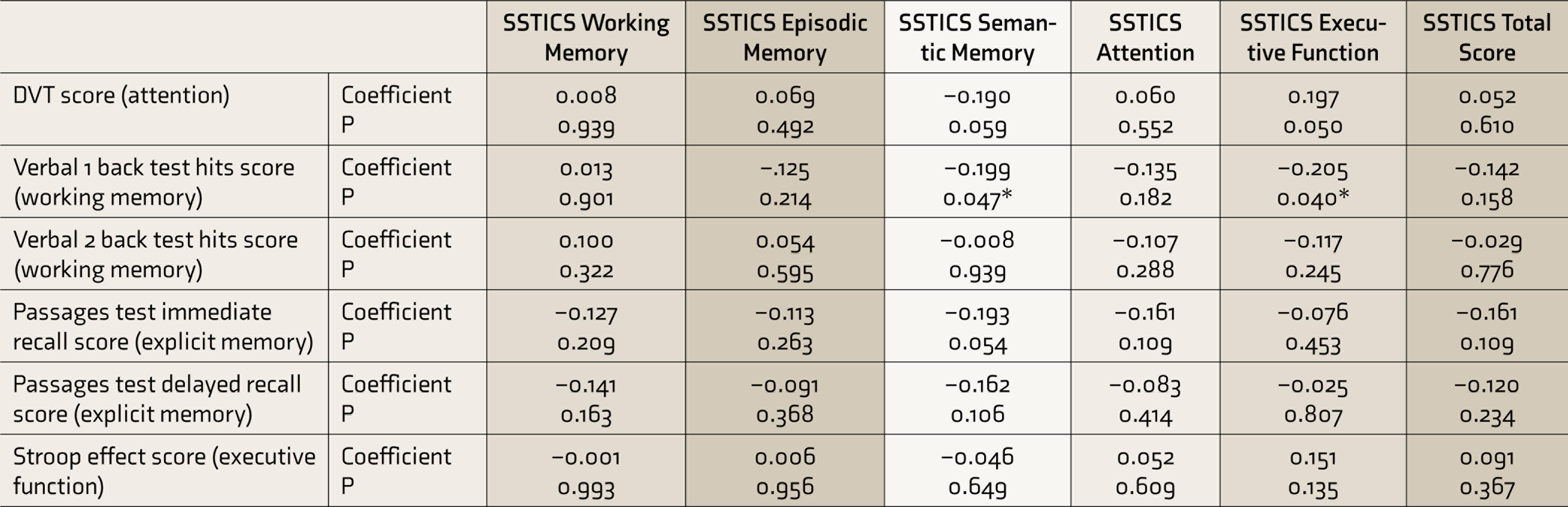
*P < 0.05.
SSTICS, Subjective Scale to Investigate Cognition in Schizophrenia; DVT, Digit Vigilance Test.
Relation Between Subjective Cognitive Complaints and Psychotic Experiences
The SSTICS scores had a nonparametric distribution. Furthermore, because of unequal sizes of the groups based on the history of PEs (15 out of the total 100 reported to have experienced a PE), a Mann–Whitney U-test was used to compare SSTICS scores among the subgroups. Those with a history of PEs had significantly greater SSTICS total scores (Median = 20) than those who did not have a history (Median = 14), U = 0.366, P = 0.009, r = 0.26, implying greater SCC. Significant differences were also noted for SSTICS attention subscale (U = 0.295, P = 0.001, r = 0.33) and SSTICS executive function subscale scores (U = 0.424, P = 0.034, r = 0.21).
Relation Between Subjective Cognitive Complaints and Social Functioning
An exploratory analysis was done using Spearman’s rank correlation to assess the relationship between SSTICS scores and SSFI scores (Table 4). While this did not show any significant correlation between SSTICS and SSFI total scores, there was a trend toward a negative correlation between multiple domains of SSTICS and SSFI “occupational role” domain scores, implying that more the SCC, worse was the social functioning with respect to occupation. A simple linear regression was then calculated to predict social functioning (SSFI total scores) based on subjective cognition (SSTICS total scores). A significant regression equation was found [F (1,98) = 5.198, P = 0.025], with an R 2 of 0.050. Participants’ social functioning reduced by 0.178 units for each unit increase in SCC.
Correlation Between Subjective Cognitive Complaints and Social Functioning
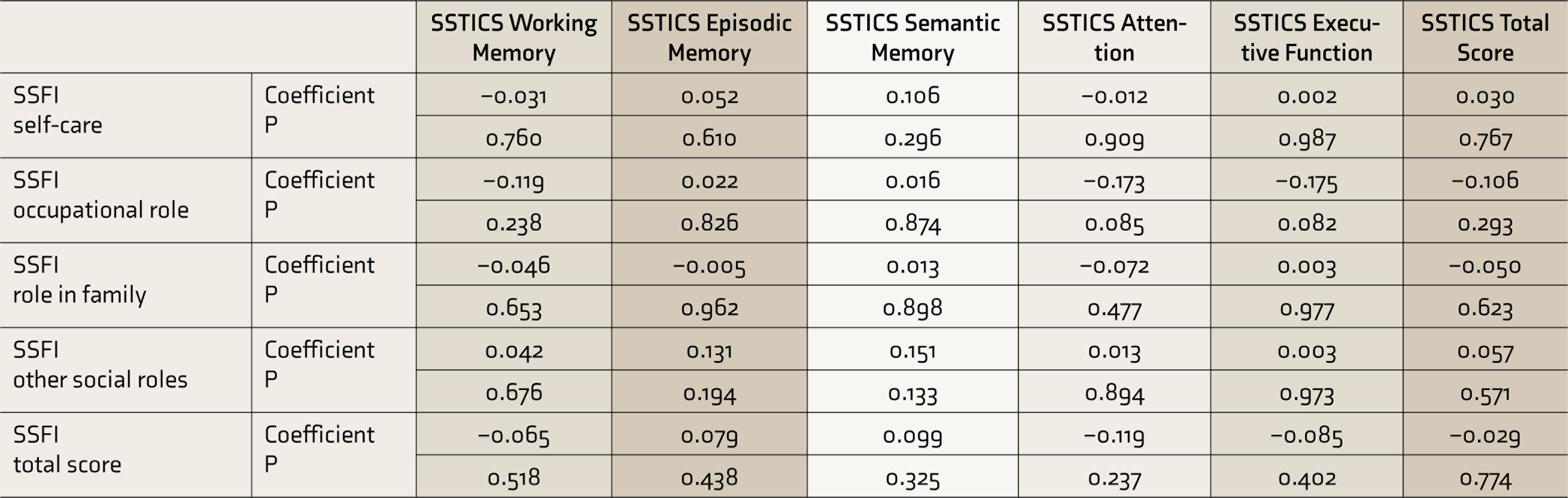
*P < 0.05; **P < 0.01.
SSTICS, Subjective Scale to Investigate Cognition in Schizophrenia; SSFI, SCARF Social Functioning Index.
Discussion
The current study demonstrated no correlation between SCC and objective cognitive scores between corresponding domains, suggesting that FDRs had a poor metacognitive awareness of their cognitive deficits, or poor NI. We also found that FDRs with a prior history of PEs had more SCC and that more SCC correlated with poorer occupational functioning.
Compared with normative data, verbal memory was the most commonly impaired cognitive domain, followed by working memory, attention, and executive function. Verbal memory has also been consistently shown to be the most affected domain in FDRs30,31 and even suggested as a promising predictive marker for future psychosis in those at a genetic high risk. 49 An important finding was that on using the 0.5 SD cutoff, many more participants showed subtler impairments, particularly in the domains of working memory and executive function.
The FDRs’ scores on the SSTICS scale were similar to those reported in the normal healthy population in the previous literature. 13 However, there was no correlation between SCC and objective cognitive scores between corresponding domains, suggesting poor NI. To the best of our knowledge, this study is the first to demonstrate poor NI in FDRs of schizophrenia patients. Poor NI in schizophrenia is known to be independent of the severity of psychotic symptoms and has been demonstrated even in patients in remission, making it a trait marker.11,24 In the light of current findings, poor NI could be explored as a possible endophenotype in schizophrenia. 28
FDRs with a lifetime history of PEs had significantly greater SCC than those without such history. Their SSTICS scores were in fact as high as that of schizophrenia patients described in previous studies.13,50 Many of these 15 FDRs could have been at an ultrahigh risk (UHR) for the development of psychosis, 51 although they were not formally assessed for the same. Also, eight of these individuals were not working at the time of assessment. Considering that FDRs with a history of PEs have strong biological vulnerability to psychosis, they are likely to share similar metacognitive deficits as seen in schizophrenia patients. This could thus explain greater SCC in them. This is in line with a recent research that explored the association between SCC and PEs in adults from low- and middle-income countries which found SCC to be associated with a 1.17 (95% CI = 1.16–1.18) times higher odds for PEs and suggested the possibility of a common biological mechanism. 46
Participants had a mean SSFI total score of 78.11 ± 8.5. Considering that 85 is the maximum possible total score and that higher scores signify better social functioning, it can be said that FDRs in general had good social functioning. However, 18% of the FDRs were unemployed, which was much higher than the national unemployment rate of 6.1% during 2017 to 2018. 52 The current study also showed that with higher SCC, there was a trend toward lower social functioning. The domain of “occupational role” (regularity at work, quality of occupation, quality of work performance, and occupational interests) particularly showed a significant negative relationship with multiple subscales of SSTICS. This brings to mind the hypothesis whether the subjective awareness of experiencing cognitive difficulties could influence one’s daily functioning. A linear regression also demonstrated this finding, though the proportion of variance in social functioning explained by SCC is low.
A recent study explored SCC and its relation to the quality of life in patients with schizophrenia and found that those who reported self-perceived SCC experienced a reduced quality of life in the physical and psychological domains. 53 Another study in schizophrenia patients explored the role of self-esteem in SCC and demonstrated low self-esteem as the strongest predictor of higher SCC, after controlling for other variables. 54 The study hypothesized that high self-esteem might only be preserved in the context of a denial of cognitive deficits. In FDRs as well, lower self-esteem in the context of greater SCC could have had an impact on occupational functioning. However, it is also possible that impaired occupational functioning could have affected their self-esteem, something which needs further exploration.
An observation made while interviewing participants was that they described resorting to strategies such as using diaries at their workplaces for making lists when assigned multistep tasks, telling their superiors to not give them certain types of work which they found difficult to focus on, entrusting the task to someone else, or even avoiding certain types of work. Thus, despite having a vague self-awareness of their cognitive deficits, the use of such compensatory strategies could have led to better social functioning. However, it is worth noting that 27% of participants were still not working at the time of assessment, implying poor occupational functioning. In such instances, interventional strategies focusing on increasing awareness, improving NI, and learning compensatory strategies could possibly help in improving their occupational functioning.
While being interviewed, some participants described avoiding certain social interactions as they could not recognize their past acquaintances when they crossed them or could not recollect past conversations and thus tended to get intimidated. It is possible that this self-awareness could have played a role in causing lower social functioning. This is particularly important because 64% to 72% participants had demonstrated a moderate impairment in episodic memory. However, because of a lack of sufficient literature, these interpretations related to SCC and social functioning are primarily observational and have to be taken cautiously.
Limitations
Our study has several limitations worth consideration. First, a healthy comparison group would have given more details of the extent of cognitive impairment in FDRs and also would have helped in nullifying the effect of reporting errors. Second, with regard to neuropsychological tests, only four cognitive domains out of those implicated in schizophrenia were chosen for evaluation as these were the ones that were explored in detail by the SSTICS scale. Because of this, the subjective awareness of deficits in other domains could not be explored. Also, two of the four neuropsychological tests required that the participant be able to read and write. Because of this, we could not enroll uneducated FDRs into the study. Third, self-esteem and its relation to SCC and social functioning were not assessed separately, which could be done in future studies. Deficits in social cognition were not assessed, and these might also have had an independent influence on social functioning. Finally, because a random sampling method was not employed, this study’s findings may not be generalizable.
Clinical Implications
Pending future research, a spectrum-based approach could be considered clinically, consisting of (a) screening all FDRs for SCC and PEs; (b) monitoring those at UHR for their progression; and (c) improving socio-occupational functioning in those who have an impairment by improving their NI and by teaching them compensatory strategies. Further interventional studies are necessary.
Conclusion
Previous research has shown that schizophrenia patients have poor NI. The findings of current study support that even FDRs of schizophrenia patients have poor NI. FDRs with a lifetime history of PEs have higher SCC, possibly reflecting higher metacognitive deficits than seen in schizophrenia patients. Importantly, even in unaffected FDRs, SCC can affect their socio-occupational functioning, especially occupation and social relations. Future studies could focus on understanding the prevalence of poor NI in the general healthy population. As schizophrenia patients and their FDRs both have poor NI, comparing this with the general population will help establish a lack of NI as an endophenotype in schizophrenia. The severity of SCC and its progression could be explored for monitoring and screening FDRs at UHR for psychosis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.