
Abstract
Background:
Emotion processing deficits have been described in patients with bipolar disorder (BD) and are considered one of the core cognitive abnormalities in BD with endophenotype potential. However, the literature on specific impairments in emotion processing cognitive strategies (directive/cortical/higher versus intuitive/limbic/lower) in euthymic adult BD patients and healthy first-degree relatives/high-risk (HR) subjects in comparison with healthy controls (HCs) is sparse.
Methods:
We examined facial emotion recognition deficits (FERD) in BD (N = 30), HR (N = 21), and HC (N = 30) matched for age (years), years of education, and sex using computer-administered face emotions–Matching And Labeling Task (eMALT).
Results:
The three groups were significantly different based on labeling accuracy scores for fear and anger (FA) (P < 0.001) and sad and disgust (SD) (P < 0.001). On post-hoc analysis, HR subjects exhibited a significant deficit in the labeling accuracy of FA facial emotions (P < 0.001) compared to HC. The BD group was found to have significant differences in all FA (P = 0.004) and SD (P = 0.003) emotion matching as well as FA (P = 0.001) and SD (P < 0.001) emotion labeling accuracy scores.
Conclusions:
BD in remission exhibits FERD in general, whereas specific labeling deficits of fear and anger emotions, indicating impaired directive higher order aspect of emotion processing, were demonstrated in HR subjects. This appears to be a potential endophenotype. These deficits could underlie the pathogenesis in BD, with possible frontolimbic circuitry impairment. They may have potential implications in functional recovery and prognosis of BD.
Adult euthymic bipolar patients have significant emotion–cognitive processing deficits. High-risk subjects have relatively specific deficits in emotion labeling subserving unique emotions, that is, fear and anger. The deficits in high-risk subjects indicate the potential endophenotype nature of these deficits.Key Messages:
Emotion processing is a complex cognitive task that involves identifying others’ emotions, processing these emotions, and responding optimally in a social realm. 1 A recent study on face emotion recognition deficits (FERD) in early adolescents has concluded that youth with increased psychological and/or somatic problems exhibited a processing bias for negative anger and fear expressions. 2 There is emerging evidence to suggest that emotion processing deficits may be a trait marker for bipolar disorder (BD). 3 BD is hypothesized to be an outcome of abnormal emotion processing. 4 FERD have been demonstrated in BD, relative to healthy subjects, during mania, 5 depression, 6 and remission. 7 These deficits may be the harbinger of pathological mood dysregulations and strained interpersonal relationships, leading to poorer long-term outcomes. FERD studies in remitted BD have reported mixed results. While most of them have reported a decrease in fear, anger, and disgust recognition in remitted BD, studies have also documented an extended reaction time (RT) for recognition of disgust, surprise, and neutrality, and confusion between fear and surprise, anger and disgust, disgust and sadness, and sadness and neutrality.8,9 Some studies have reported the impaired ability of BD patients to perceive the intensity of a facial emotion. 10 Other studies have reported no FERD in remitted BD relative to controls. 11
The specific abnormalities of FERD can be broadly divided into two conditions, namely automatic/intuitive processing limbic deficits and directive higher order cortical deficits. 12 These are demonstrated by the difficulties in matching and labeling facial emotions, respectively. This highlights the need to have a refined approach to study FERD for a clear delineation of its neural underpinnings. Studying the specific abnormalities (emotion matching and labeling) in FERD could throw light on the neural-cognitive substrates of BD.
FERD has also been investigated as a potential endophenotype in first-degree relatives (high-risk (HR) subjects) of BD patients. To consider a cognitive parameter as a potential endophenotype, it must be clearly heritable, be associated with the disorder in the population, be present in a remitted state, and be demonstrable in the unaffected family members. 13 Few of the available studies have shown that BD patients and their unaffected first-degree relatives both have deficits in FERD, whereas there are also studies that have not shown any emotion recognition deficits in the first-degree relatives.14,15 The available literature on the endophenotype potential of FERD in BD is scarce and with conflicting results and merits further investigation, particularly studies that look at specific abnormalities, which will help us identify the neural-cognitive substrates of emotion processing in HR subjects.
This study examines the specific processes of FERD in the remitted adult subjects with BD and first-degree relatives of subjects with BD (HR) compared to matched healthy subjects (HC). We hypothesized that there would be greater deficits in emotion processing among remitted BD subjects and HR of BD subjects than HC and that FERD could thus serve as a potential endophenotype in BD.
Materials and Methods
Subjects
This cross-sectional study was conducted at a tertiary care psychiatric institute in India. The Institute Ethics Committee approved the study. Three groups were included as a part of this study: 30 subjects with BD, 21 HR, and 30 HC. Written informed consent was obtained from all participants. The study recruitment happened between May 2011 and January 2014.
Assessments
Patients were assessed using MINI 5.0, 16 and those who fulfilled DSM IV criteria for BD type I were recruited under the BD group. HR and HC groups were screened for psychiatric disorders using MINI 5.0 screener.
Edinburgh Handedness Inventory was used to assess the handedness in all the three groups; only right-handed individuals were included, as studies show a consistent relationship between lateralization of affective processing motor dexterity and language in individuals with clear right-handedness 17 .
Family Interview for Genetic Studies 18 was used to assess the family history of psychiatric illnesses in the BD, HC, and HR groups.
Clinical Global Impression (CGI) scale was used to assess the severity of illness. For inclusion, the following criteria have been considered. 19
Inclusion Criteria
All participants were in the age range of 18–50 years
Right handed
Had at least seven years of formal education
No Neurological and other medical disorders
All patients with BD had to be in remission as assessed using the CGI severity rating (CGI score of 1)
HR subjects did not have a family history of psychiatric illness in the first-degree relatives other than BD
HC did not have a family history of psychiatric disorder among their first-degree relatives
Three groups were matched for age, years of education, sex, and handedness
Unaffected siblings/offspring of identified BD probands formed the HR group. Consenting individuals matched for sociodemographic parameters and without any current or lifetime psychiatric illness formed the HC group. The details related to illness were carefully ascertained by clinical interview of patient and also by reliable information obtained from an adult first-degree relative.
Emotions–Matching and Labeling Task (eMALT) Method
The experimental paradigm consisted of human faces depicting fear, anger, sadness, and disgust emotions obtained from a validated tool culturally appropriate for Indian subjects—Tool for Recognition of Emotions in Neuropsychiatric DisorderS (TRENDS). 20 To explore the complex emotion processing function with relevance to the frontolimbic circuitry, the TRENDS experiment was modified to incorporate emotion matching and labeling tasks, based on pre-existing studies. 21 In this experiment, the subjects performed three tasks: matching facial emotions, labeling facial emotions, and control tasks. The task was designed and delivered using E-Prime (Psychology Software Tools, Pittsburgh, PA, USA) running on a laptop. Images were displayed at a resolution of 1024 × 768 pixels via an LCD screen kept about 45 cm away from the subject. In the matching task, subjects were presented with a target face along with two other faces (of different individuals) on the same screen. They were asked to select which one of two faces presented on the same screen expressed the same emotion as that of the target face, by pressing the laptop’s buttons. In the labeling task, subjects viewed the same target face but had to judge which of the two labels (the words—fear/anger or sad/disgust), given below the target, best described the target facial emotion. The paradigm consisted of 16 experimental blocks: 4 blocks each of matching and labeling emotions, interleaved with 8 control blocks. For each affect condition, 32 different images were used: 8 per block, 2 of each gender, 2 of old age, and 2 of young. For the control task, six different geometric forms were used. Each matching and labeling block consisted of eight stimuli of 10-s duration (of the maximum display), and the control block consisted of four stimuli of the same duration. The stimuli were presented in a random manner within each block. The paradigm was counterbalanced across subjects with respect to the type of emotions, the intensity of emotions, and the gender and age of the subjects in the images.
The sample size in each group required was estimated as 19 for the RT, considering a moderate effect size for ANOVA statistic (f = 0.025) for a power of 0.8 and alpha value of 0.05. The accuracy and RT values were normally distributed (Shapiro–Wilk P > 0.05 on all measures). One-way ANOVA was used to examine the differences in age and years of education between the BD, HR, and HC groups. To examine the difference in sex distribution, a chi-square test was employed. All the FERD parameters were analyzed using ANOVA. The differences in accuracy and RT for matching and labeling tasks for FA emotions and SD emotions were analyzed between the three groups. Bonferroni corrected P value of <0.006 was considered as a statistically significant difference, based on at least eight tests of association to examine the intergroup differences. In addition, Pearson’s correlation was employed to examine the relationship of various FERD measures and variables like age, age of onset, years of education, and the number of mood episodes.
Results
The demographic characteristics of the three groups are described in the table below (Table 1)
Demographic Characteristics of the Three Groups

HR: high-risk subjects, HC: healthy controls.
Clinical characteristics of BD group: The mean numbers of manic episodes, depressive episodes, mixed episodes, and total episodes were 3.10 ± 3.03, 0.59 ± 0.78, 0.03 ± 0.19, and 3.71 ± 3.13, respectively. Family history of BD among the first-degree relatives was present in 2/30 BD subjects. The HR group comprised 15 siblings and 6 offspring of BD probands. Five of the HR subjects belonged to genetically loaded families with two or more first-degree relatives having BD. All the recruited subjects completed the experiment.
Table 2 and Figures 1–4 show the differences in the matching and labeling accuracy scores between the groups. The three groups were found to be significantly different based on labeling accuracy scores for FA (P < 0.001) and SD (P < 0.001). On post-hoc analysis, HR subjects exhibited a significant deficit in the labeling accuracy of FA (P < 0.001) compared to HC. The BD group was found to have significant differences in all FA (P = 0.004) and SD (P = 0.003) emotion matching as well as FA (P = 0.001) and SD (P < 0.001) emotion labeling accuracy scores compared to HC. While both BD and HR groups demonstrated deficits in labeling accuracy of FA relative to HC, there were no differences between BD and HR based on any FERD parameters (all P > 0.05). There were no differences in the RT (in seconds) between the three groups, as shown in Table 3.
Comparison of Emotion Matching and Labeling Accuracy Between Subjects With Bipolar Disorder (BD), High-Risk Subjects (HR), and Healthy Controls (HC)
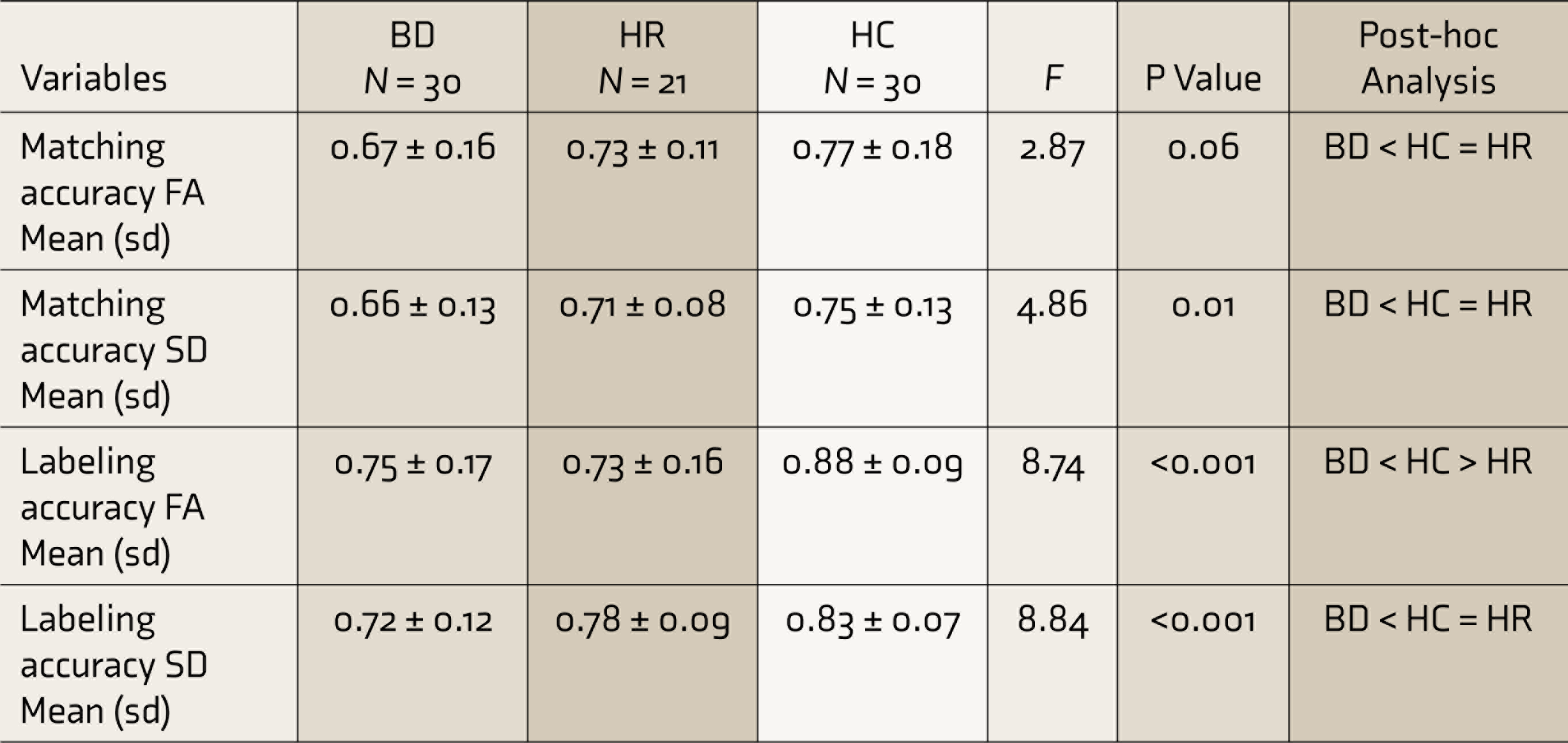
F: ANOVA, FA: fear/anger, SDL: sad/disgust, sd: standard deviation. P < 0.006 is statistically significant.
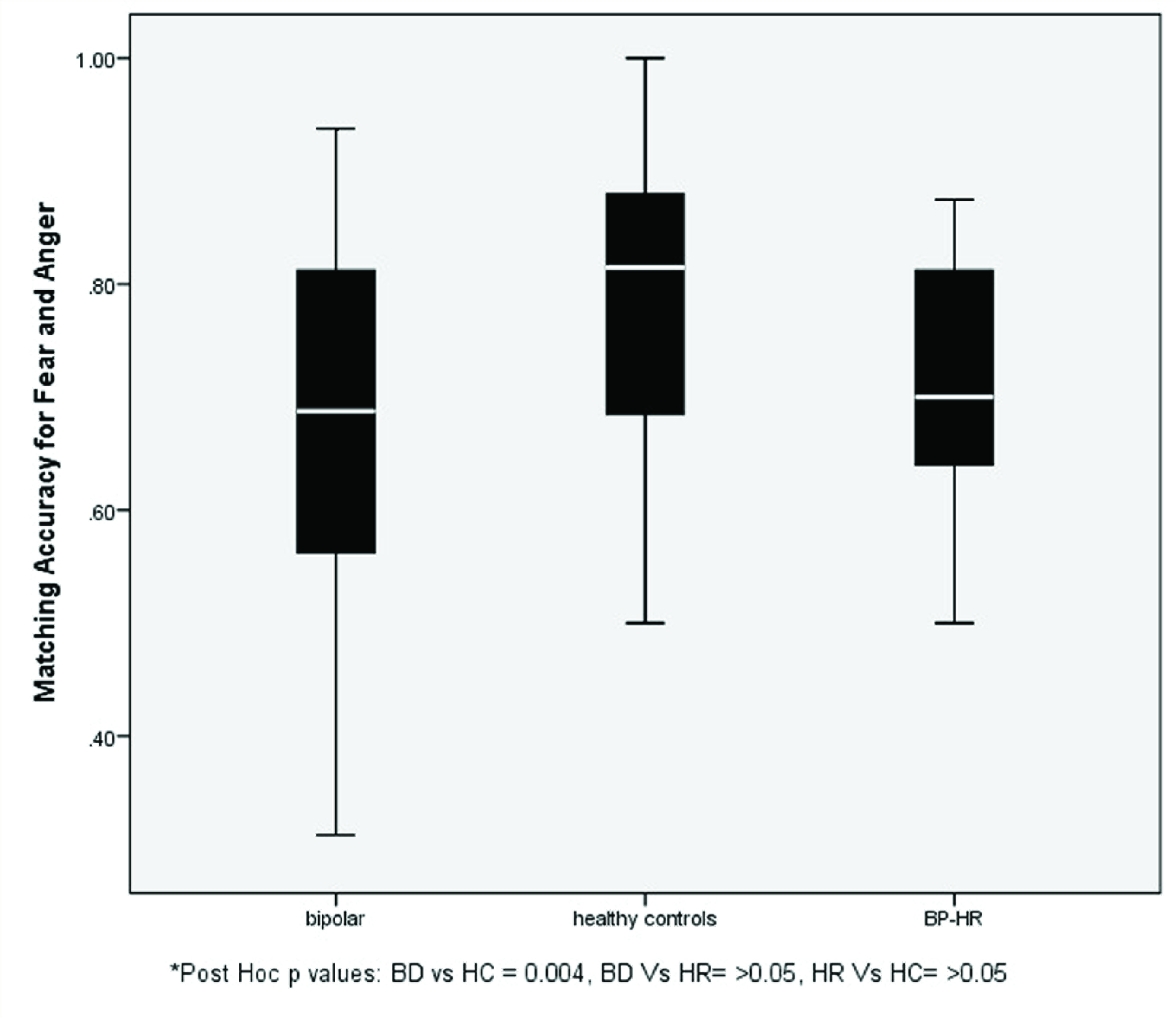
BP-HR: high-risk subjects. Error bars depicting matching accuracy scores of fear and anger emotions of the groups.
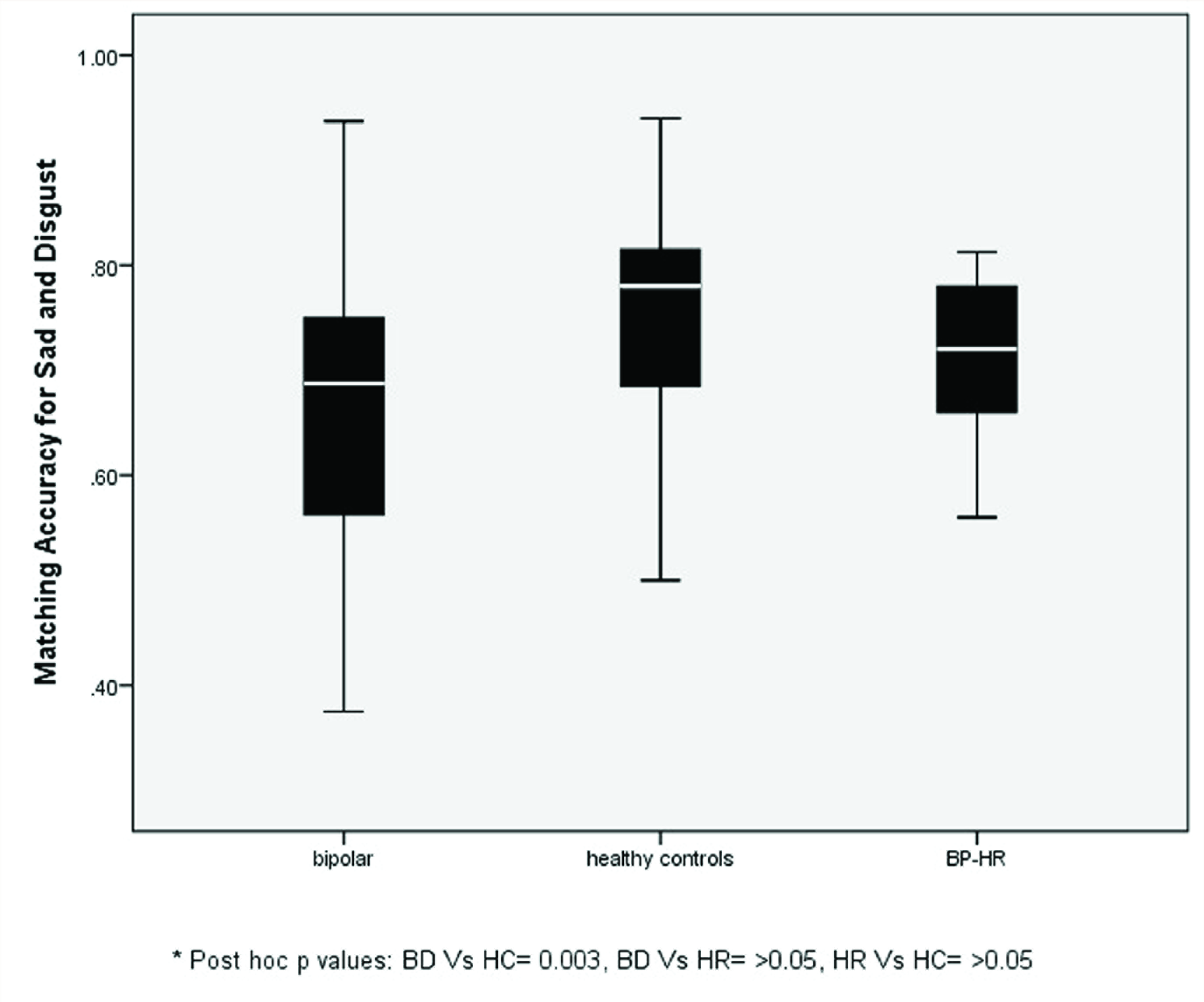
BP-HR: high-risk subjects. Error bars depicting matching accuracy scores of sad and disgust emotions of the groups
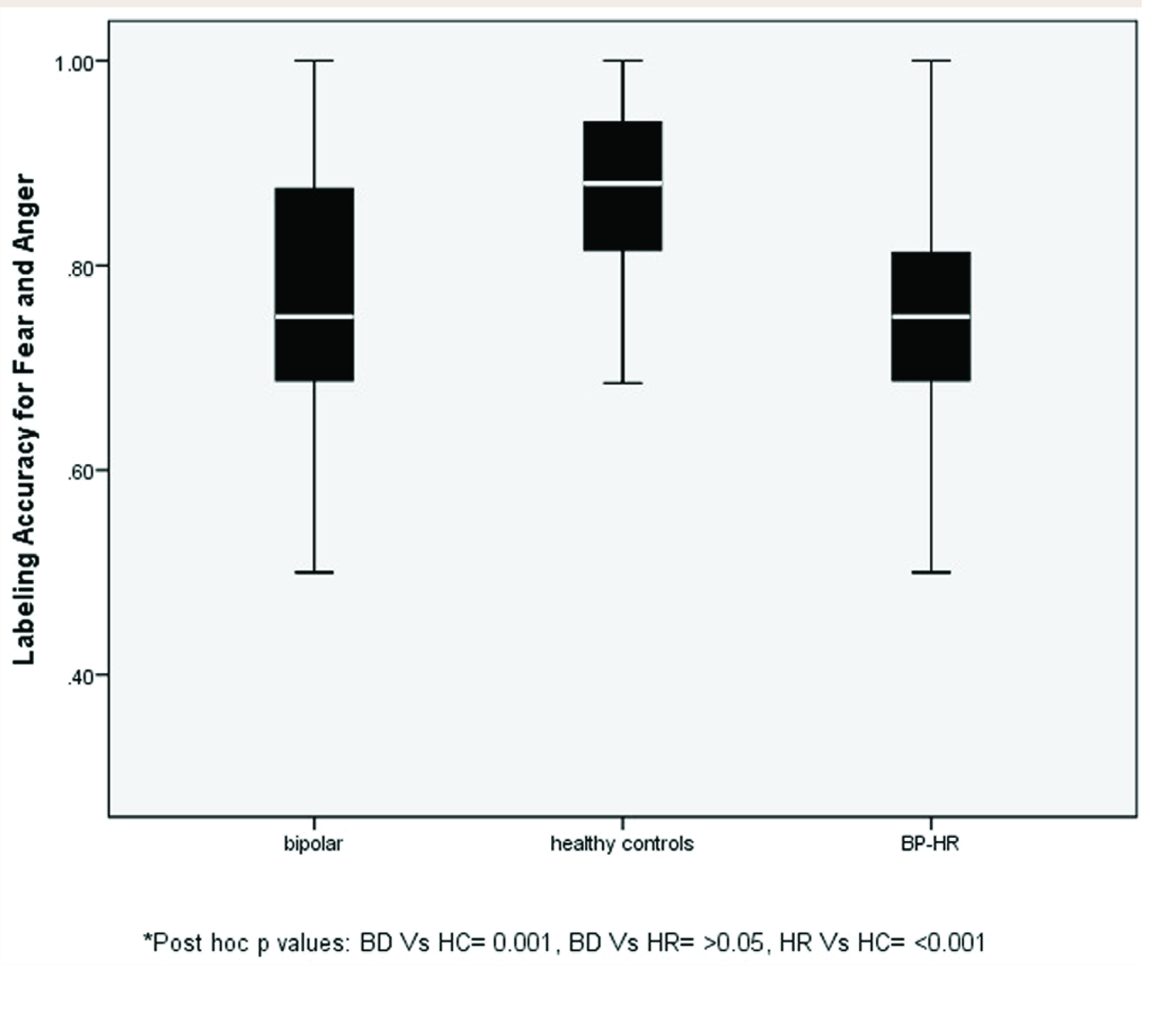
BP-HR: high-risk subjects. Error bars depicting labeling accuracy scores of fear and anger emotions of the groups.
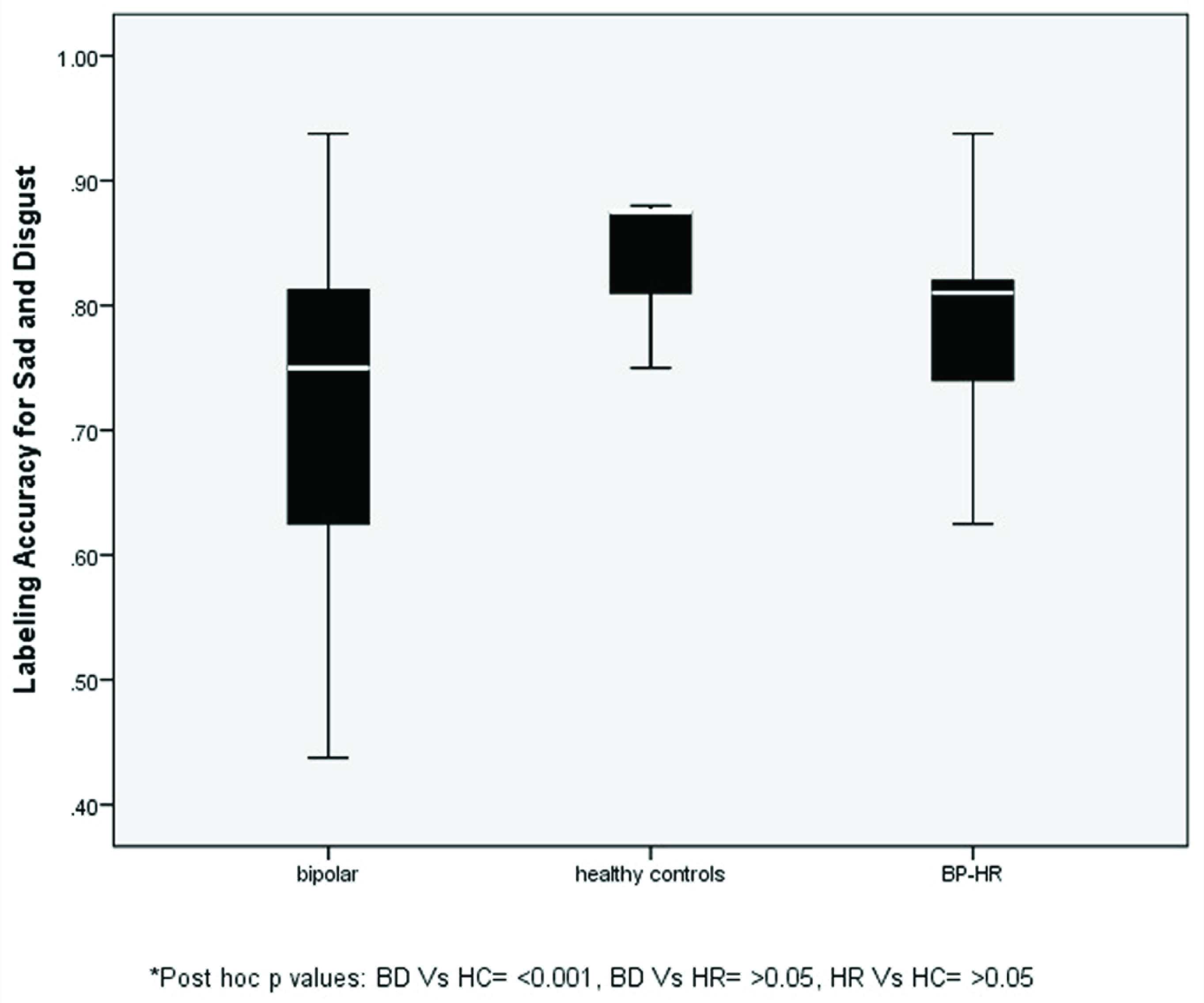
BP-HR: high-risk subjects. Error bars depicting the labeling accuracy scores of sad and disgust emotions of the groups.
Comparison of eMALT Reaction Time (in Seconds) Between Subjects With Bipolar Disorder (BD), High-Risk Subjects (HR), and Healthy Controls (HC)
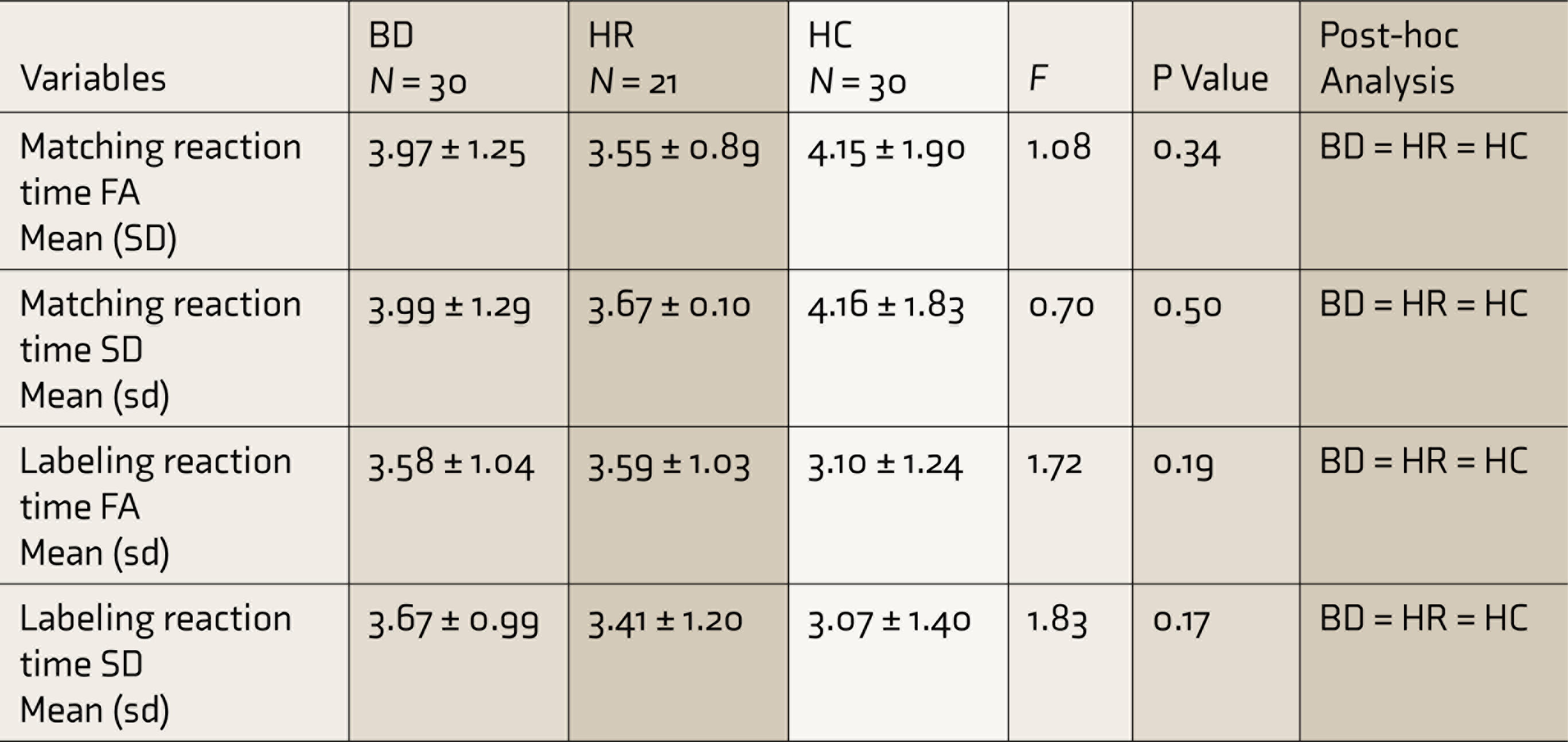
F: ANOVA, FA: fear/anger, SD: sad/disgust, sd: standard deviation. P < 0.006 is statistically significant.
There were no significant correlations between FERD parameters and other variables like age, age of onset of illness, years of education, and the total number of mood episodes (all P > 0.05). Additionally, there were no sex effects among the FERD measures observed based on independent samples t-test performed between the genders in each of the three groups (all P > 0.05).
Discussion
The paradigm used in this study allows examination of FERD during two diverse types of facial affect assessment: a matching situation, which is based on automatic/ intuitive processing, and a labeling situation, which is dependent on directive superior cognitive processes, such as judgment and interpretation. This study’s main finding is that both BD and HR subjects demonstrate specific deficits in fear and anger emotion labeling compared to HC, which could be a potential endophenotype for BD. There were no differences in the emotion processing between BD and HR subjects, whereas BD subjects in remission exhibited other FERD deficits, too, in addition to FA labeling, compared to HC.
In further attempts to elucidate the “trait” status of FERD, studies have demonstrated poor performance of FERD among remitted BD subjects (both adult and pediatric samples) in comparison with HC7,22–24 as shown in the present study. A meta-analysis reveals that impairments in BD are associated with abnormality in facial affect recognition, highlighting the importance of this parameter. 25 A study that compared the FERD among childhood-onset BD and adult BD showed that those with childhood-onset BD had higher deficits; this might interfere with the developmental trajectory itself. 26 A recent study attempted to look at emotion recognition by a task that used point-light displays of human full figures moving in a manner indicative of a basic emotion; results showed that individuals with BD (I and II) had significant impairment in the ability to perceive emotions. The impairment was global, that is, affecting all emotions. 27 Studies have also shown that patients with BD tend to overestimate the intensity of certain facial expressions; this may lead them to interpret social cues erroneously and to engage in dysfunctional behaviors and cognitive patterns. 10 Our findings are in line with these previous studies wherein we have found significantly higher FERD in BD compared to HC. This finding is of clinical importance because BD patients, even during remission, have psychosocial problems. These could be related to cognitive deficits and difficulties in recognizing emotions in human faces and the residual symptoms. This highlights the importance and applicability of interventional approaches such as social cognition and intervention training (SCIT) 28 in BD at an early stage.
Emotion processing is a prototypical function in the path of mood regulation, and it can thus be considered as a crucial clinical characteristic of BD. Meticulous examination of these functions can offer a heuristic understanding of the aberrations in the cognitive substrates of emotion processing in BD. In the present study, among the HR subjects, compared to HC, the emotion labeling task was predominantly affected. As mentioned earlier, the labeling task requires higher cognitive processes. A previous study on the first-degree relatives of children with BD demonstrated a labeling deficit as an important finding. 29 This indicates that deficits in facial emotional labeling may be a risk marker for developing BD in the future. Studies in pediatric BD have shown the ventral affective system, which encompasses the Ventrolateral Prefrontal Cortex (VLPFC) and limbic regions, especially the amygdala, as the regions implicated in FERD. 30 Another recent study, which looked at the telomere length as a predictor of emotional processing in the brain, compared BD, HR, and HC groups on fMRI-based FER tasks. That study reported that the effective connectivity in BD patients, compared with healthy individuals, was associated with reduced connectivity between inferior occipital gyrus (IOG) and Ventral Prefrontal Cortex (VPFC) but increased connectivity between amygdala and VPFC. The reciprocal endogenous connectivity between the IOG and the fusiform gyrus was higher in HR compared with both other groups. 31 The telomere length did not show any differences. These neural systems have complex emotion processing functions that appear deranged even in first-degree relatives, 32 which could thus be conferring a genetic vulnerability to develop BD. In this way, these deficits may be conceptualized as an endophenotype of the BD, and the present study demonstrates such cognitive deficits in adult samples.
The finding of differential FERD of fear/anger compared to sad/disgust among the HR subjects in this study also seems interesting. The inability of BD patients to correctly identify fearful faces have been reported previously. 33 In mania, BD subjects had poor ability to recognize fear and disgust. 5 In contrast, while in the euthymic state, BD subjects recognized disgust better. 34 Malhi et al. reported the differential brain activation patterns for fear compared to disgust in BD and HC. 7 Two recent studies showed that the HR subjects have more FERD, especially in recognizing the emotions of sadness, anger, and fear.35,36 Euthymic bipolar patients responded largely to fear, whereas healthy subjects responded almost exclusively to disgust in that study. Fearful facial expressions produced greater neural activation in remitted BD patients in comparison to HC. The significant differences in this context were seen in the hippocampus, the inferior parietal and superior temporal cortices, and the cerebellum. In BD, the response to fear and disgust is mediated by the amygdala and insula, respectively. Since there was specific difference in the response to fear, the neural substrate for fear could have a specific circuit abnormality, which is different from those involved in other emotions such as disgust. 7 It is possible that there is a specific emotion processing circuit of fear, which needs to be explored in further studies, which has an endophenotype characteristic in BD because it has a differential impairment among the HR subjects.
We used a specific paradigm that allows examination of directive higher cognitive and intuitive lower cognitive subfunctions of emotion processing. Our findings provide important information on the cognitive processes that remitted BD patients and HR subjects of BD engage when identifying facial affect. The strengths of our study are relatively good sample size and the use of structured, standardized scales for subject assessment. The study of FERD across remitted BD subjects and HR establishes its endophenotype characteristic. The use of a culturally validated tool for the assessment of FERD provides evidence for the cross-cultural substantiation of the presence of FERD in BD.
Bilderbeck et al. studied the effects of drugs on the FERD in BD subjects and found that lithium and possibly dopamine antagonists may be associated with reduced processing of anger cues in BD. 37 Our subjects with BD were on various psychotropic medications, including mood stabilizers. This can be considered as a limitation. However, the RTs of BD subjects were not sluggish compared to that of other groups, indicating that generalized mental slowing due to drug side effects like sedation might not be significant. The lack of intelligence quotient assessment could be considered a limitation. However, the groups have been matched based on the years of education, even though this might not actually reflect one’s intelligence. In addition, our study involves both siblings and offsprings of BD probands within the HR group. The heritability of genetic attributes could vary between offsprings and siblings, and hence, a more homogeneous group might have provided a better picture.
In conclusion, this study demonstrates that adult euthymic bipolar patients have significant emotion–cognitive processing deficits across a wide range of emotions. This may have clinical significance with respect to the psychosocial functioning. On the other hand, HR subjects appear to have relatively specific higher order cognitive abnormalities subserving unique emotions, pointing toward a potential endophenotypic nature of these deficits. Further rigorous examination of these specific abnormalities and their imaging-based neural substrates is needed. Such studies can help us enhance the understanding of the neurobiology of BD and its neurocognitive vulnerability attributes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.