
Abstract
Background:
Diagnosis of Attention Deficit Hyperactivity Disorder (ADHD) in preschool children is challenging and complicated owing to the presence of developmentally appropriate overactivity and a dynamic developmental/learning phase shaping their behaviour. We aimed to study the clinical profile and co-morbidity of ADHD in preschool children.
Methods:
Fifty consecutively presenting preschool children with ADHD were enrolled from our child guidance clinic (CGC) between January 2017 and December 2018. The diagnosis and assessment of comorbidities were based on the DSM-5 criteria and Vanderbilt teacher and parent rating scales. Relevant clinical and sociodemographic profiles were assessed and analyzed for association with ADHD subtypes and comorbidity.
Results:
Preschool children with ADHD constituted 8% of all patients visiting the CGC and one-fifth of all children with ADHD. Male:female ratio was 11.5:1. Hyperactive-impulsive was the commonest type, and oppositional defiant disorder (ODD) was the commonest comorbidity. Most children belonged to the lower-middle socioeconomic group. Language delay was observed in 20%. Median social quotient measured using the Vineland Social Maturity Scale was 83.
Conclusions:
Preschool children predominantly have the hyperactive impulsive type of ADHD. Isolated language delay was the predominant comorbid developmental disorder, and ODD was the predominant comorbid behavioural disorder. Addressing these issues would help in the appropriate management of these children.
Keywords
Preschool attention deficit hyperactivity disorder (ADHD) constitutes 22.2% of all childhood ADHD patients seen in the Child Guidance Clinic. Hyperactive-impulsive type is more common than the inattentive or combined types of ADHD. Oppositional defiance disorder is the commonest comorbidity, seen in 60%.Key Messages:
Attention deficit hyperactivity disorder (ADHD) is the most common neurobehavioral disorder of childhood and one of the most prevalent chronic health conditions affecting school-age children. It is a developmental disorder characterized by a pattern of severe inattention and/or hyperactivity-impulsivity beyond that observed in individuals at a comparable level of development. 1 Worldwide, the prevalence of ADHD is estimated at 5% for children. 2 Prevalence of ADHD varies depending on whether the study is population- or hospital-based. The hospital-based prevalence of ADHD in Indian children range from 8–20%.3–5 The problem persists beyond childhood and into adulthood, causing significant limitations in the functioning. Parents of children with ADHD also undergo enormous stress and experience marital disharmony. Preschool children with ADHD later exhibit significant social and chronic educational difficulties during school years.6–8 Preschoolers may have difficulty paying attention, following directions, and awaiting their turn. These symptoms not only affect behaviour, learning, and academic skills development but also impact a child’s emotional, social, and adaptive development and functioning. In preschool children, behavioral difficulties are predictive of academic and social functioning throughout childhood and adulthood and hence need early intervention and treatment. Diagnosis and treatment of ADHD and associated comorbidities in the preschool-age population are more complicated than in older children because of developmental and physiological differences. Hence, identification of comorbidities in preschool children with ADHD and risk factors associated with particular comorbidities can help in effective management, thereby preventing long-term adverse outcomes. There are no Indian studies exclusively done in children with preschool ADHD to look for comorbidities to the best of our knowledge. The objectives of our study were to identify the relative frequency of ADHD in preschool children attending a child guidance clinic (CGC) and to study the relevant clinical and sociodemographic parameters and comorbidities in them.
Materials and Methods
Setting
This cross-sectional study was carried out at the CGC of the paediatric outpatient service of Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry, in collaboration with the Department of Psychiatry, from January 2017 to December 2018, after obtaining approval from the Institute Ethics Committee. Informed consent was obtained from the parents before the inclusion of subjects in the study.
Participants
Preschool children (aged 2–5 years) with clinical features suggestive of ADHD were included in the study. Children with sensory deficits (visual or hearing loss), intellectual disability as defined by a social quotient (SQ) of 70% or less by Vineland Social Maturity Scale (VSMS), thyroid disorders, post-encephalitic sequelae, neurodegenerative disorders (especially leukodystrophies), autism spectrum disorder, or other mental disorders like schizophrenia were excluded.
Sample Size Estimation
This study did not use a formal sample size calculation. As per the proportion of ADHD in preschool children attending our CGC, based on our previous records, we expected to enroll about 50 children during the study period. Therefore, a convenient sample size of 50 participants was considered for inclusion.
Diagnosis and Tools for Measurement
ADHD was diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria. 9 The Vanderbilt ADHD Diagnostic Rating Scale, including both parent and teacher rating scales (both English and Tamil), was used to assess ADHD as it also has measures for assessing comorbidity. History was obtained regarding the presence/absence of seizures, socioeconomic status, family history, personal history, age of onset of symptoms, their duration and severity, and the settings in which they occur. Parents and teachers were asked to complete the Vanderbilt rating scales to evaluate the child’s behaviour. If the child is not going to school, an assessment of symptoms during the clinic visit was completed by the investigator by observing the behavior of the child and interacting with the parents. Vanderbilt rating scales contain 55 questions in the parent version and 43 in the teacher version. Assessment was done by rating the frequency of the child’s behavior on a 0–3 scale (0—never, 1—occasionally, 2—often, 3—very often). A score of 2 or 3 (“often” to “very often”) is considered a positive response. Children with ≥6 positive responses to the nine core inattentive symptoms on questions 1–9 are considered to have the inattentive type (IA), those with ≥6 positive responses on the nine core hyperactive-impulsive symptoms on questions 10–18 are considered to have the hyperactive-impulsive type (HI), and those with symptoms of both IA and HI are considered to have the combined type (CT).
Assessment of comorbidities was also done using the Vanderbilt rating scales. Assessment of SQ was done using the Indian adaptation of VSMS, which has 89 items under eight domains arranged in the order of increasing ability as per age. Depending on the ability of the child to perform a particular item in each domain, a score is given, and the total score is converted to a social age as per the table provided. A detailed examination, including for dysmorphology and of the central nervous system, was also performed.
Statistical Analysis
Continuous variables like age were expressed as mean with standard deviations or median with interquartile ranges (IQR), as appropriate. The normality of data was checked with the Kolmogorov–Smirnov Z test, and the significance of non-normally distributed data were assessed with the Mann–Whitney U test. Categorical variables like sex, socioeconomic status, type of ADHD, comorbidity, prematurity, low birth weight, and family history are presented as proportions. Chi-square test or Fisher’s exact test were used to test their significance. P value <0.05 was considered significant. Statistical Package for the Social Sciences (SPSS) software version 19.0 (SPSS Inc. Chicago, Illinois) was used for data analysis.
Results
A total of 707 children attended the CGC in the study period. Out of these, 256 were diagnosed to have ADHD with or without intellectual disability. Of these, 57 in the preschool age group satisfied the criteria for diagnosis of ADHD using Vanderbilt rating scales and as per DSM-5. Out of them, seven were excluded (six had intellectual disability with SQ ≤70% and one had post-encephalitic sequelae). Finally, a total of 50 children were included in the study. Of these, 46 (92%) were males and four, females. For most (78%), the parents were not graduates. Ten children (20%) had at least one parent as graduate, and for only one child (2%) both parents were graduates. Most (29, 58%) belonged to the lower middle class, 11 (22%) to the upper lower class, 9 (18%) to the upper middle class, and only 1 (2%) belonged to upper socioeconomic class. The median age with IQR for boys was 54(44–60) months, and for girls, it was 60 (55–60) months.
The sociodemographic profile, perinatal factors, neonatal factors, and comorbidity in different types of ADHD are given in Table 1. The most common type was the HI, seen in 29 (58%) children, followed by IA in 11 (22%) children and CT in 10 (20%) children. A difference in the distribution of different types of ADHD among both sexes was observed with IA being more common in girls 3 (75%) versus 8 (17.4%) in boys, and the HI being more common among boys 29 (63%) versus 0 girls. CT was seen in 9 (19.6%) boys and 1 (20%) girl.
In our study, we could find a difference in the distribution of different types of ADHD among the different socioeconomic classes too, with most children belonging to the lower middle class and all children with CT belonging to the lower middle class (Table 1).
Socioeconomic Status, Perinatal and Neonatal Factors, and Comorbidity in Different Types of ADHD.
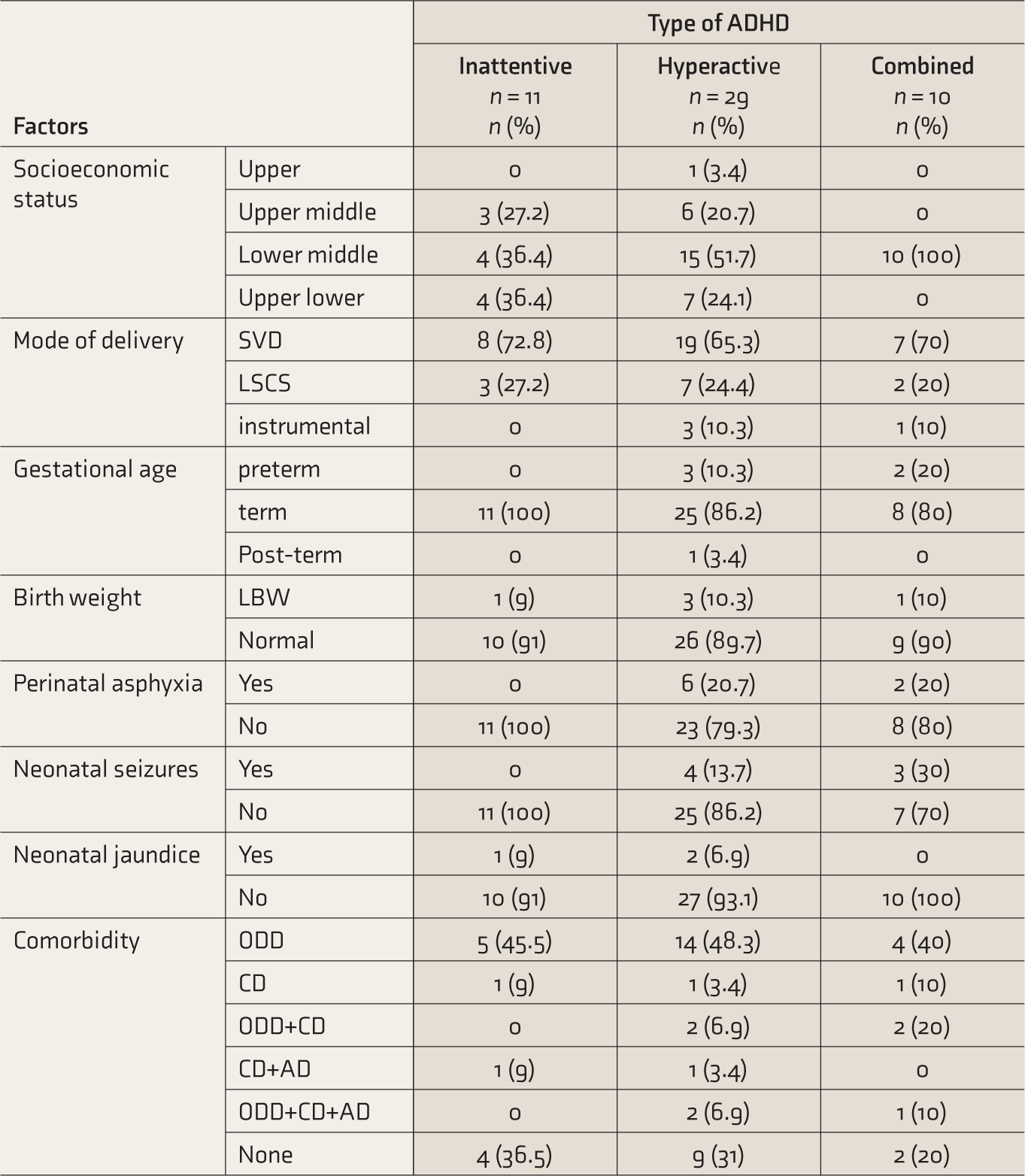
ADHD: Attention deficit hyperactivity disorder, SVD: spontaneous vaginal delivery, LSCS: lower segment caesarean section, LBW: low birth weight, ODD: oppositional defiant disorder, CD: conduct disorder, AD: anxiety disorder.
Four (8%) children were born out of instrumental delivery, 5 (10%) were born preterm, 5 (10%) had low birth weight, 8 (16%) had perinatal asphyxia, 7 (14%) had neonatal seizures, and 3 (6%) had neonatal jaundice. Four (8%) children have been on phenobarbitone during the neonatal period. Six (12%) had family history of other psychiatric illness, including depression (n = 1), obsessive compulsive disorder (n = 2), tic disorder (n = 1), and schizophrenia (n = 1). In 33(66%) children, parental substance use was seen, which were all seen in the father and included smoking and alcohol consumption. History of excessive television viewing (defined as viewing television for more than two hours per day) was seen in 23 (46%) children, and one child (2%) had history of ADHD in a parent. There was no significant differences in the distribution of familial or environmental factors in different types of ADHD.
The commonest developmental delay found was isolated language delay, which was seen in 10 (20%) children, followed by gross motor delay in 1 (2%) child. Out of the 10 children with language delay, five had HI type of ADHD, four had CT, and one had IA. The overall median SQ (IQR) in the children was 83 (82, 84.2). There was no significant difference in median SQ in children with different types of ADHD.
The commonest comorbidity was oppositional defiance disorder (ODD), seen in 30 children (60%), followed by conduct disorder (CD) in 12 (24%) and anxiety disorder (AD) in 5 (10%). In 3 (6%) children, no comorbidity was seen. ODD was more prevalent in HI type but the difference was not statistically significant. More than one comorbidity was seen in nine (18%) children and they more often had the HI type. Out of total comorbidities, a higher proportion of comorbidities (80%) was found in CT (Table 1). No significant difference was found in the distribution of perinatal or neonatal factors (Table 2) as well as familial or environmental factors (Table 3) in different types of comorbidity. Regarding developmental delay and comorbidity, motor delay was seen in a child with ODD. Of the 10 children with language delay, six had ODD and two each had CD and no comorbidity. We did not find a significant difference in the distribution of SQ based on comorbidity. On exploratory analysis none of the perinatal/neonatal factors or familial/environmental factors were significantly associated with the type of comorbidity (Table 4).
Perinatal and Neonatal Factors and Comorbidity.
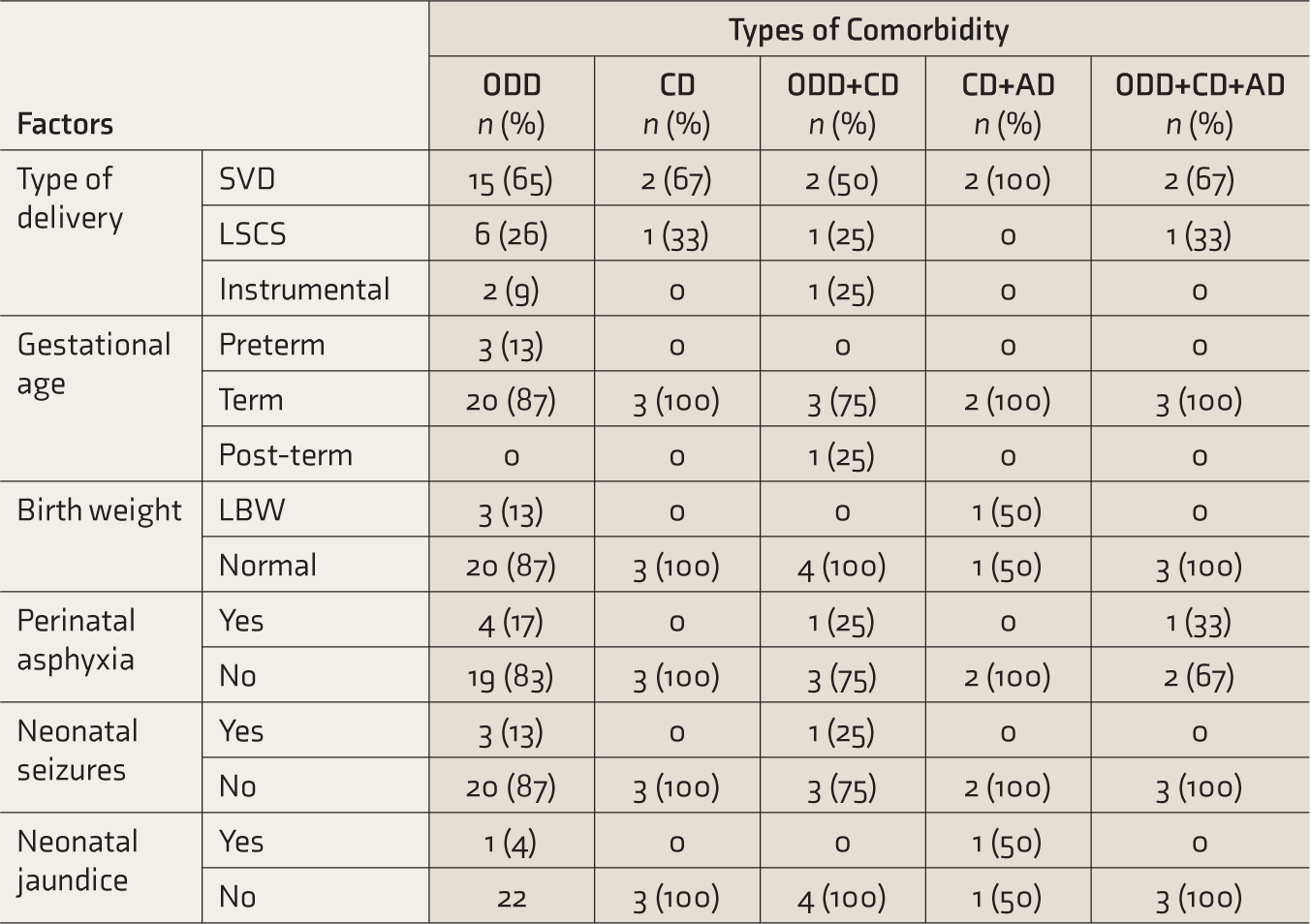
SVD: spontaneous vaginal delivery, LSCS: lower segment caesarean section, LBW: low birth weight, ODD: oppositional defiant disorder, CD: conduct disorder, AD: anxiety disorder.
Familial and Environmental Factors in Different Comorbidities.
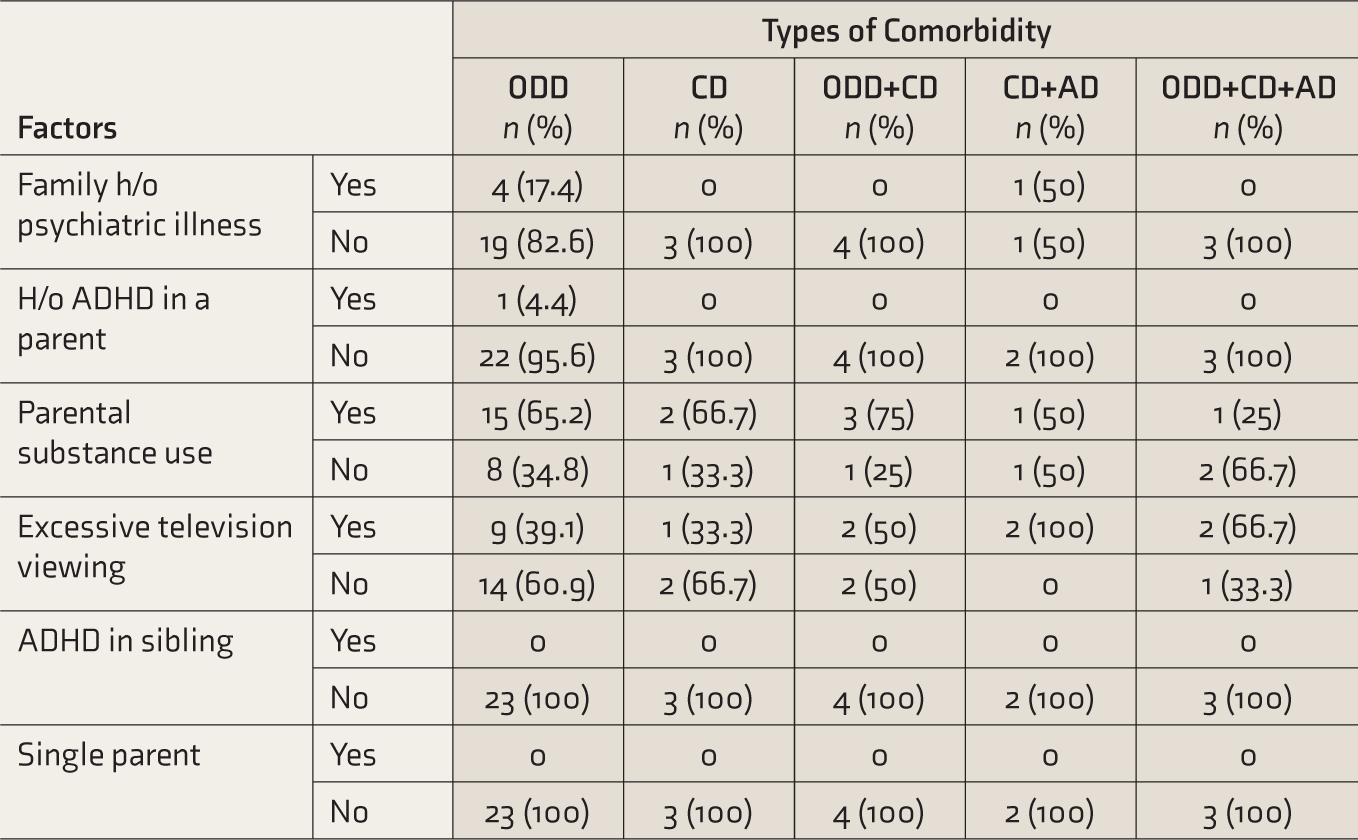
ADHD: attention deficit hyperactivity disorder, ODD: oppositional defiant disorder, CD: conduct disorder, AD: anxiety disorder.
Exploratory Analysis of Factors Associated with Comorbidity.
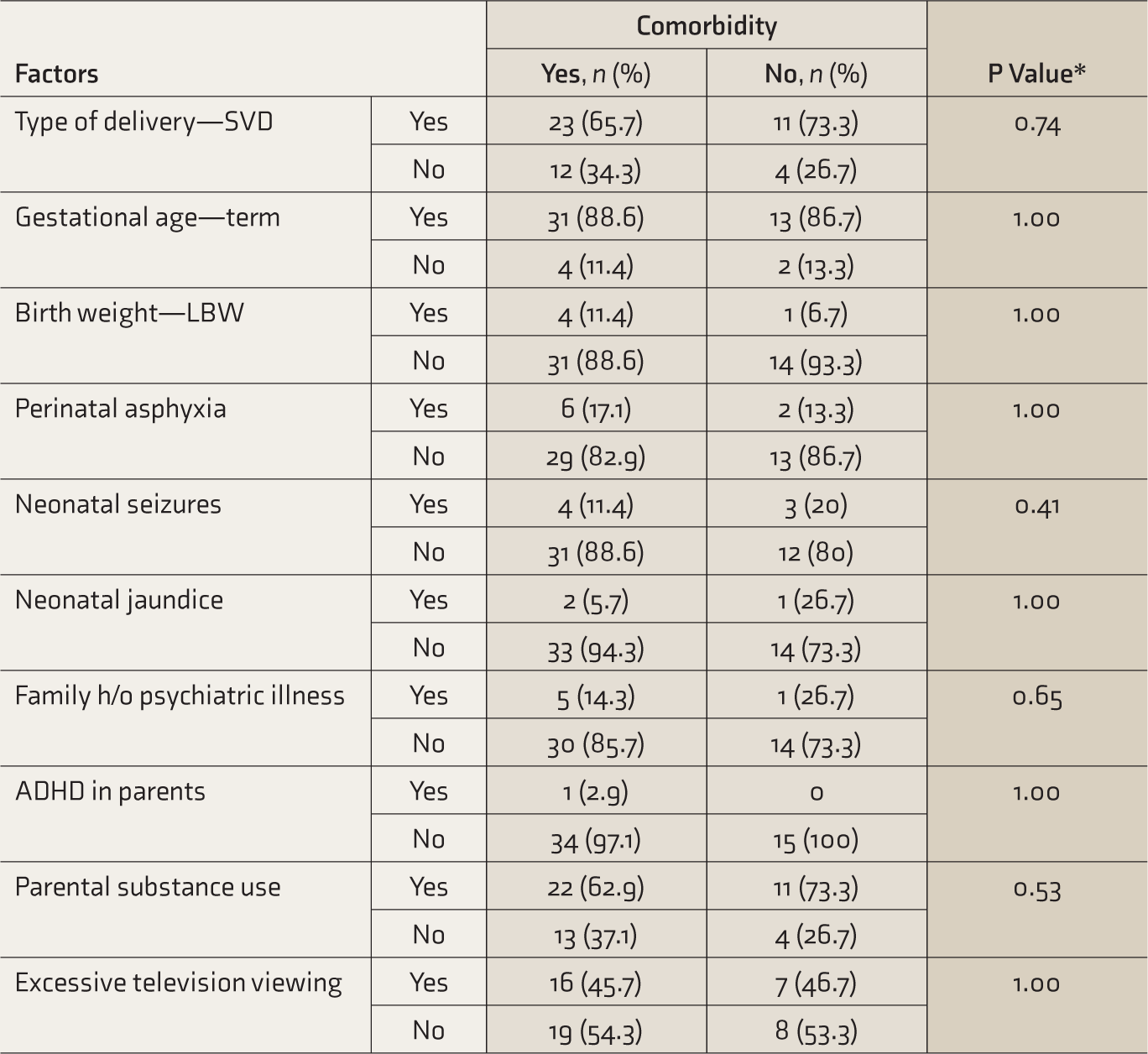
SVD: spontaneous vaginal delivery, LBW: low birth weight, ADHD: attention deficit hyperactivity disorder. Parental Habits include smoking and alcohol consumption. *Fischer’s exact test.
Discussion
Children of preschool age accounted for about one-fifth (22.2%) of all children with ADHD. In Venkatesh et al.’s cohort of ADHD, 20% were preschool children. 5 This shows ADHD is quite prevalent among preschool children. Similar observations have been made by Palfrey et al. in their longitudinal study in which 13% of children aged 14–29 months had definite features suggesting the possibility of ADHD. 10 Studies had shown overall prevalence rates of ADHD in school children ranging widely from 1% to 23%, depending upon the definition and tool used to diagnose the disorder and whether the studies are hospital- or community-based. 11
The male-to-female ratio in our sample was 11.5:1. Several studies have documented a greater prevalence of the disorder among boys, both in the western countries 12 and in India.4,5 This may be because externalizing disorders are more common in boys and internalizing behavior, in girls. Though boys and girls with ADHD behave the same symptom-wise, boys are more likely to be diagnosed with IA type of ADHD, more likely to be affected with anxiety and depression as well as poor self-esteem. 13
We found low educational qualification of parents in higher frequencies. In 78% of children, neither parent was a graduate. On the contrary, a recent study from India did not find any relation between parents’ education and the prevalence of ADHD. 5 A similar observation was made by Gross-Tsur et al., according to whom there was no relationship between ADHD and parental age or profession. 14 This needs to be analysed in population-based studies as our study group may not represent the community. We also found that children with ADHD belonged to a lower socioeconomic class. This finding was consistent with other Indian studies.4,10 Compared to community samples from western studies, the number of children with a single parent, parental substance abuse, or psychiatric illness in family was not significantly high in our study. 15 This might be due to wide variation in cultural and demographic characteristics among the communities. Similarly, we did not find any significant association between gestational age, birth weight, perinatal asphyxia, neonatal seizure, or neonatal jaundice and prevalence of ADHD. This may be attributed to our small sample size. According to published literature numerous prenatal risk factors appear to be associated with ADHD, including maternal substance use and stress during pregnancy, prematurity, low birth weight, and several other complications related to childbirth. 16 Previous reviews have concluded that despite the demonstration of association, there is as yet insufficient evidence to support the notion of a truly causal relationship between those prenatal risk factors identified to date and the later outcome of ADHD. 16 Eight percent of children had used phenobarbitone during the neonatal period. Previous studies reported the use of phenobarbitone as a risk factor for ADHD. 17 We found a history of excessive television watching in 46% of the children. This was proposed as a risk factor for ADHD in previous studies.18,19 Further research is needed regarding the same.
Family history of other psychiatric illness was found in 12% of the children. A previous study has reported that parental psychopathology is a strong risk factor for conduct problems among children with ADHD (20); yet, the impact of paternal psychopathology remains relatively understudied. Because ADHD is highly heritable, parental ADHD symptoms have emerged as a focus of intervention and research. 20
The commonest type of ADHD in our study was HI (58%). This is consistent with other Indian studies, where they reported HI to be more prevalent in preschool children.4,5 A possible explanation is that younger children who qualify for HI do not exhibit inattention because they are not required to display a longer attention span in preschool years but might be required to do so in higher classes, and inattention becomes evident at older ages. Therefore, as the children with HI get older, they may also show maladaptive levels of inattention and change their sub-type to CT.
The commonest comorbidity we found was ODD (63.2%), followed by CD (26.5%) and AD (10.2%). This finding is similar to another Indian study, where ODD was the most common comorbidity in preschool children. 5 In our study, 18% of the children had multiple comorbidities. These include ODD+CD (8%), CD+AD (4%), ODD+CD+AD (6%). Similarly, studies had reported the presence of multiple comorbidities in children with ADHD.21,22
Regarding developmental profile, 20% (n = 10) had language delay, which was comparable to a previously reported study from India, though we did not find any significant association between language delay and ADHD. 5 Several studies have reported a significant association between language problems and ADHD.5,23
Limitations
As most preschool children in our study did not go to school, the researcher completed the teacher assessment form based on observation of the child’s behaviour and parental account. The study was conducted at a tertiary referral hospital, and the profile of enrolled subjects may not represent the ADHD profile encountered at the community level. Hence, the proportion of ADHD in preschool children encountered by us may be related to Dr Berkson’s bias. Risk factors like familial, prenatal, and neonatal factors were not significantly associated with ADHD in our study, but this may be due to the inadequate sample size. We did not collect information about the child’s temperament. Similarly, we did not collect information for qualitative analysis. Longitudinal studies are needed to evaluate the risk factors associated with this disorder and to understand the role of comorbidities and their effects on symptom stability and the level of functioning of these children.
Conclusion
Pre-school ADHD constitutes 8% of all patients seen in CGC and about one-fifth of all children with ADHD. The commonest subtype of preschool ADHD seems to be HI. A male preponderance was conspicuous, and most children belonged to the lower socioeconomic class. Isolated language delay seems to be the predominant developmental delay in these children and hence they might need speech/language training. ODD was the commonest comorbidity. CT was associated with more comorbidities and might negatively impact a child’s behaviour and functioning. Further studies with a larger sample size and longitudinal follow-up are needed to ascertain the effect of comorbidities on the outcome of these children.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.