
Abstract
Background:
Dhat syndrome (DS) is considered a culture-bound syndrome of South East Asia. It is often associated with multiple sexual and psychiatric comorbidities. We aimed to assess the quality of life (QoL) and disability in patients of DS with and without comorbidity.
Methods:
This cross-sectional study included 117 patients with DS and 117 matched controls. DS was diagnosed based on the International Classification of Diseases, 10 version, Diagnostic Criteria for Research diagnostic criteria. Comorbidities were assessed on MINI 6.0.0, and the patients were divided into two groups (with and without comorbidity). The QoL and disability were estimated and compared between patients with and without comorbidity and their respective control groups consisting of healthy volunteers, using standardized tools.
Result:
Most of the patients were unmarried males aged 18 to 25 years and from rural backgrounds. Most of the patients (72.64%) had comorbidities (psychiatric/sexual). The QoL of patients with DS was poor compared to healthy individuals. The QoL of patients with comorbidity was worse than that of those without them (P < o.ooo). The disability of patients with DS was more than that of healthy individuals (significant in all domains of the World Health Organization Disability Assessment Schedule [WHODAS]).
Conclusion:
Patients having DS had poor QoL and higher disability than healthy controls. Patients having psychiatric or sexual comorbidities had less QoL and higher disability compared to healthy controls and those without comorbidities.
Patients with DS have a poor QoL and higher disability than healthy controls; The presence of comorbidities with DS is associated with a further decrease in the QoL and disabilityKey Message:
Dhat syndrome (DS) is a culture-bound sexual neurosis prevailing within the Indian landmass. It is characterized by excessive concern about harmful consequences of loss of seminal fluid (International Classification of Diseases, 10 version—ICD-10). 1 In South East Asia, patients with semen loss anxiety often manifest various physical, psychological, and sexual symptoms attributed to loss of semen.2–4 Prakash and Meena (2008) reported that DS patients believed that whatever blood collected during an erection in the cavernous areas probably turns into semen (by ultracondensation, semen is formed from food in multiple steps: 40 drops of food=1 drop of blood; 40 drops of blood= 1 drop of marrow; 40 drops of marrow= 1 drop of semen), and consequently, with any sexual activity, they lose blood. Because blood is their energy source, they lose strength every day and become weaker and more lethargic. 5 Uncertainty over the nosological status of DS continues to persist.6–10 Most studies found depressive neurosis (40%–42%) as the commonest psychiatric comorbidity, whereas anxiety disorder (21%–38%) and somatoform disorder/hypochondriasis (32%–40%) are other psychiatric disorders related to DS. Erectile dysfunction (ED, 22%–62%) and premature ejaculation (22%–44%) are the frequently associated psychosexual comorbidities DS.3, 11
QoL indices have been used in medical practice to estimate the impact of different diseases on functioning and well-being and compare outcomes between different treatment modalities. Patients of DS are preoccupied with semen loss and persistently complain of bodily weakness (attributing these problems to semen loss).3, 12–14 In addition, many studies revealed that DS is associated with common mental disorders (CMDs) such as anxiety disorders and depressive disorders and runs a persistent and long course.2, 3, 12, 14–17 These factors may be associated with impairments in QoL and can cause disability in the patients. However, researchers have not focused on the QoL of the patients with DS and disabilities it caused. Previous studies on DS have shown that up to two-thirds of cases with DS have psychiatric and sexual comorbidities. 15 Hence, it would be worth investigating the impact of the presence of psychiatric and sexual comorbidities on the QoL and disability domain of patients of DS with these comorbidities in reference to DS without these comorbidities. 18 Furthermore, understanding the QoL and disability among patients with DS may guide clinicians in holistically planning their psychosocial management.
Material and Methods
A cross-sectional study was conducted (between October 2016 and September 2017) at a tertiary care center in North India after getting approval from the Institutional Ethics Committee. Patients diagnosed with DS attending the psychiatry outpatients department were initially assessed by a resident doctor according to the ICD-10 Diagnostic Criteria for Research (DCR), and then consultant psychiatrists confirmed the diagnosis. Patients suffering from DS as diagnosed by ICD-10 DCR, with age greater than 18 years and consenting to participate in the study, were included. Patients with any comorbid medical illness, mental retardation, organic brain syndrome, severe mental illnesses, and those who did not cooperate with assessment because of any other psychiatric condition requiring prior management were excluded. A general physical examination of the patient was done, with a focused physical examination evaluating the genitourinary system to rule out other causes of urethral discharge. Patients were screened on mini-international neuropsychiatric interview 6.0.0 (MINI 6.0.0) to rule out other psychiatric disorders and to diagnose comorbidities as per the selection criteria. A semi-structured proforma was used to collect information about the patient’s demographical, clinical, and psychosocial variables. Physical illness was ruled out by history provided by family members, general physical examination, and review of medical records. They were assessed on the World Health Organization Quality of Life (WHO QoL-BREF) 19 for the QoL and the World Health Organization Disability Assessment Schedule (WHODAS 2.0) 20 for disability. The patient group was divided into two based on the presence or absence of comorbidities. As this was a time-bound study, we included all the patients meeting the selection criteria during the study period.
Two different control groups were recruited for patients with DS with and without comorbidities. The controls were recruited from the hospital staff and attendants of the patients attending for minor ailments in the medical outpatient departments (OPDs) of the institute. The controls were assessed using 12 items general health questionnaire (GHQ), 21 and subjects with scores <3 were included. They were matched on age, education, and domicile with the corresponding patient subgroups. Different control groups were taken to minimize the sociodemographic confounders by accurate matching. The controls also were assessed on WHO QoL-BREF and WHODAS 2.0. 20
Thus, the sample was divided into four groups (A, B, C, and D). Group A consisted of the patients of DS having sexual and/or psychiatric comorbidity. Group B consisted of the patients with DS without comorbidity. Groups C and D consisted of healthy individuals matched to Groups A and B, respectively. The patient groups and healthy controls were compared for the rest of the sociodemographic characteristics and clinical profile, QoL, and disability.
Before including them in the study, written informed consent was taken from the patients and control group. The data collected were found to be normally distributed. Analysis was done using SPSS 16.0 (SPSS Inc., Chicago, IL, USA). Analyses done were exploratory. Comparison between the groups was done using the Chi-square test and student’s t-test.
Results
A total of 145 patients were screened and 117 were included. The most common causes of exclusion were the presence of medical comorbidities (n = 12) and severe mental illnesses (n = 10). For the control group, 125 subjects were screened to enroll 117 subjects. The most common causes for exclusion from the control group were GHQ > 3 (n = 5) and refusal to give informed consent (n = 3). There were 85 participants in Group A and 32 in Group B. For all the patients, it was their first psychiatric consultation in our center. Before, they had consulted traditional healers, dermatologists, general physicians, and psychiatrists in private clinics. They have been receiving different types of medications (antidepressants, nutraceuticals, and benzodiazepines) for varied periods.
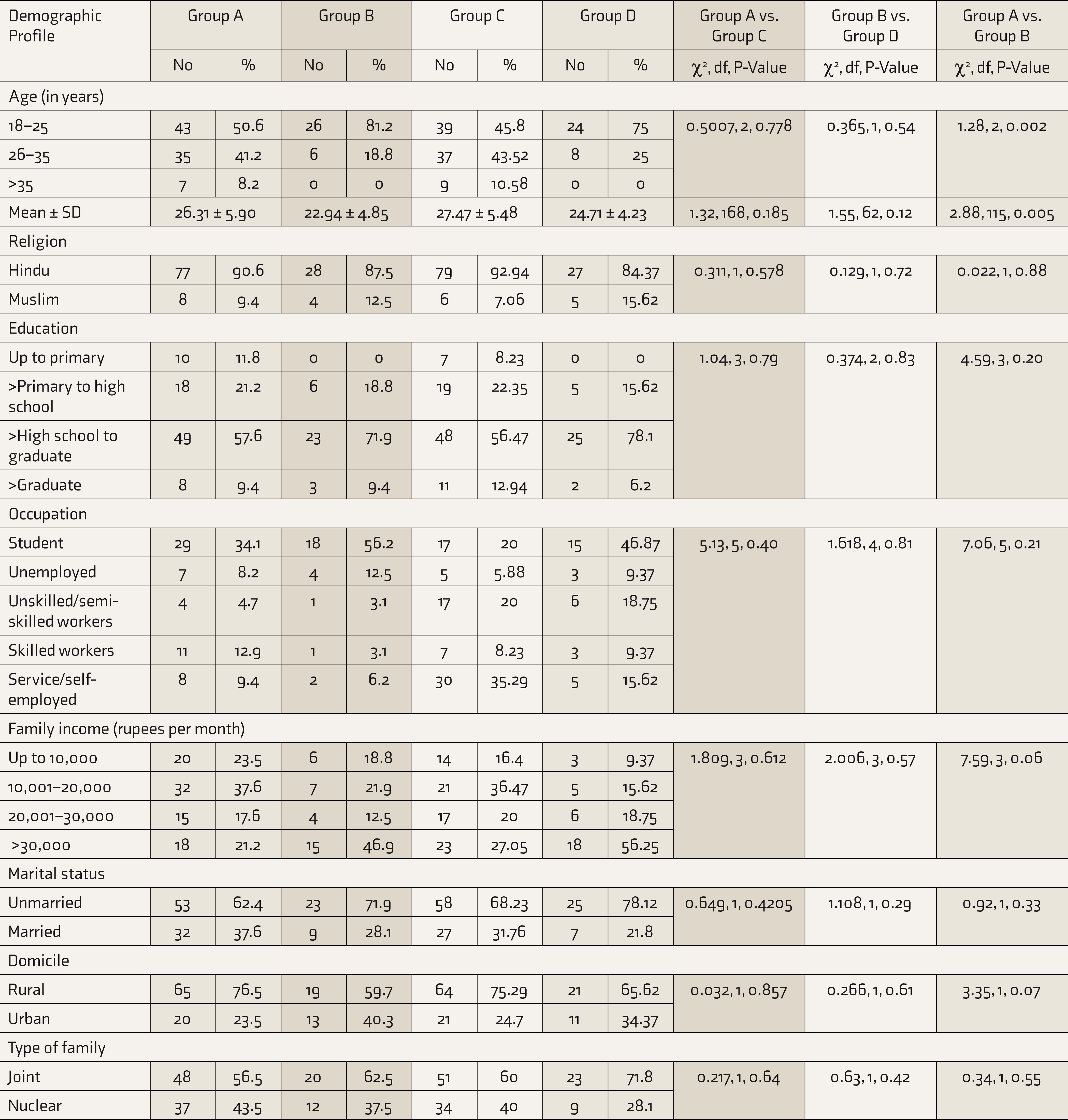
The sociodemographic profile, that is, age, education, family income, religion, occupation, and domicile of Group A and its control group Group C showed no significant differences (Table 1). Likewise, the sociodemographic profiles of Groups B and D too did not show any significant difference. The mean ± SD age of Group A was 26.31 ± 5.90 years and that of Group B was 22.94 ± 4.85 years, with the difference in age being statistically significant (P = 0.005). There were no significant differences between Groups A and B on the rest of the sociodemographic parameters.
Sociodemographic Profiles of Subjects
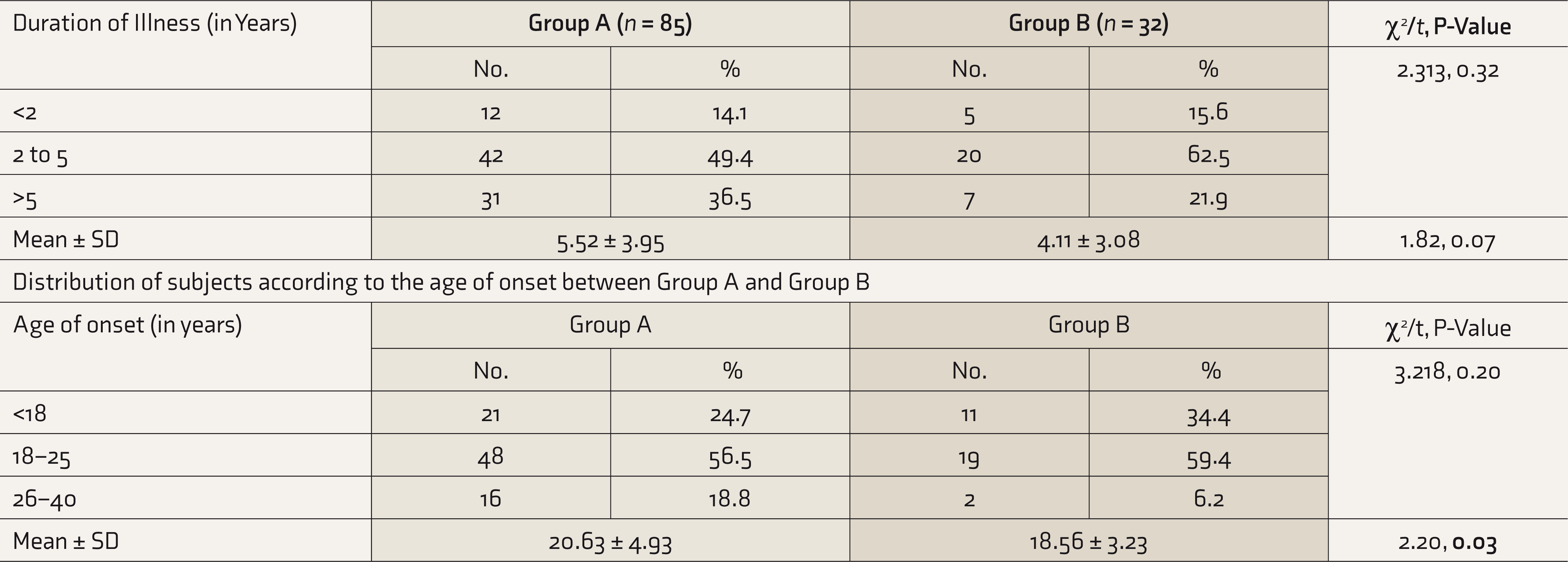
Most of the patients had duration of illness between two and five years in both Groups A and B (Table 2). The mean duration of illness in Groups A (5.52 ± 3.95 years) and B (4.11 ± 3.08 years) had no statistically significant difference. Most DS patients in Groups A and B were in the age group of 18 to 25 years. There was a significant difference (P = 0.03) in the mean age of onset between Group A (20.63 ± 4.93 years) and B (18.56 ± 3.23 years).
Clinical Variables of the Patients with Dhat Syndrome
Most of the DS patients (n = 85, 75.35%) had comorbidities; psychiatric comorbidities (n = 68, 58.11%) were more common than sexual comorbidities. Among the sexual comorbidities, premature ejaculation (n = 59, 50.42%) was more common, followed by ED (n = 54, 46.15%) and lack of sexual desire (n = 43, 36.75%; this data is not mutually exclusive). Among the psychiatric comorbidities, depression (n = 56, 47.86%) was the most common, followed by anxiety disorders (n = 41, 35.04 %), personality disorders (n = 23, 19.65%), and somatoform disorders (n = 13, 11.11%).
The QoL of DS patients with and without comorbidities was poor in all domains of WHO QoL-BREF scores compared to healthy individuals (Table 3). A significant difference was found in all domains of the WHODAS too (Table 4).
Comparison of Quality of Life on the Basis of WHO QoL-BREF Score Among Participants

WHO QoL-BREF, World Health Organization quality of life-BREF version.
Comparison of Disabilities on the Basis of WHODAS Scores
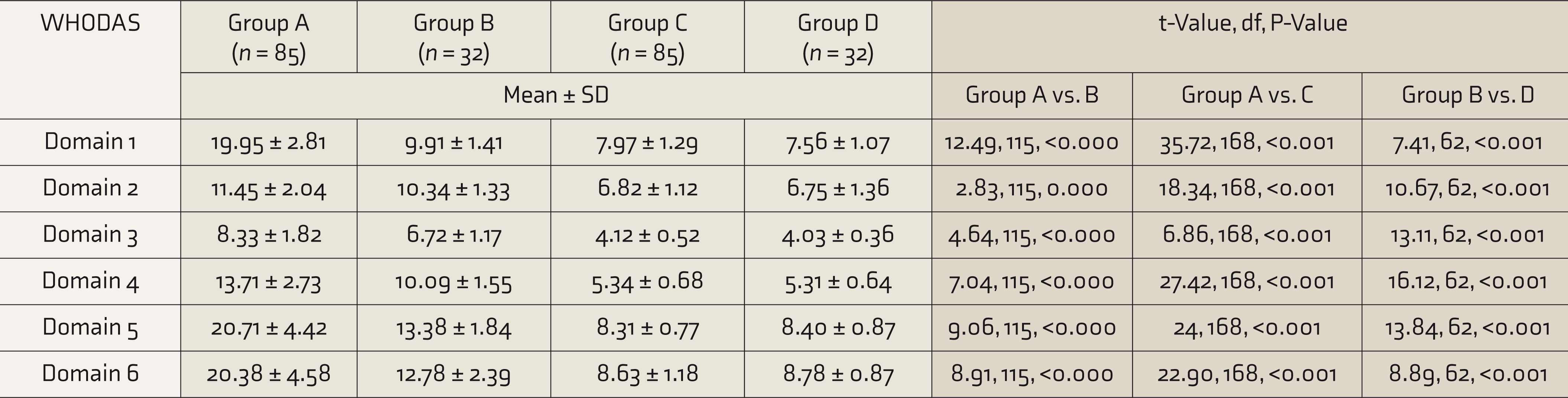
WHODAS, World Health Organization disability assessment schedule.
Discussion
Our study showed that the patients with DS experience significant distress, have adversely affected QoL, and have a significant disability. To our best knowledge, no earlier study had assessed the QoL and disability in patients of DS in a systematic manner using standardized tools.
The mean age of our DS patients was 25.39 ± 5.81 years. In earlier studies, adolescence and young adulthood were the most common age groups for the presentation of DS.12, 15, 22–27
The majority of our patients (61.53%) were educated beyond matriculation. In contrast to earlier studies, our patient sample had more numbers of educated people. In recent years, the literacy level of the Indian population has increased 28 ; however, DS continues to exist in our society despite the improvement in education levels. This shows that only academic education may have no role in preventing DS, and specific sex education may be required to target this illness. The usual education does not equip the individual with knowledge and attitudes related to sexual health. The physiological basis of sexual functioning and normal variations in the sexual area is not discussed in the classes. A few other recent studies also found that DS continues to persist despite increasing educational qualification of adolescents and young adults in India.24, 27, 29
The majority (72.65%) of the patients were unmarried. This is consistent with the findings of earlier studies.25, 30, 31 Unmarried people have fewer opportunities to engage in coitus and are more likely to indulge in masturbation, have more frequent nocturnal emissions, etc., resulting in higher chances of developing semen-loss-related anxiety. The majority (72.65%) of the subjects were from rural backgrounds. Available literature suggests that DS is reported more in the people living in rural areas.26, 30, 31
We found young age of onset and a long time to reach for psychiatric consultation in our sample. This is consistent with the findings of Grover et al. 12 This shows that even cases of DS without other comorbidities may have chronic and persistent course.
Comorbidities
Depression has been reported among DS patients by several studies and is by far the most common reported comorbidity, with prevalence ranging from 40% to 66% in various studies.31–34 It is understandable, as the “loss” of semen, like the loss of any other valued possession, produces a sense of grief and may precipitate clinical depression in a patient of DS. Anxiety neurosis (21%–38%) and somatoform and hypochondriacal disorders (40%) too have been reported.30, 35 This is consistent with our findings. Different types of anxiety disorders also were studied in our samples. A nationwide multicentric study to evaluate comorbidity in patients with DS in India by Grover et al. 15 revealed that 67.2% of patients have comorbidities. Among psychiatric comorbidities, depression was the most common and present in 20.5% of DS patients. In the above-mentioned study, 20.5% of patients had comorbid anxiety disorders, and the most common anxiety disorder was other anxiety disorders (9.4%). The variation in finding maybe because of our small sample size and because patients were taken from a tertiary care center’s treatment-seeking population. Most of our patients were referred from various departments, and these patients mostly presented with additional complaints of various sexual and psychiatric comorbidities. An earlier nationwide multicentric study by Grover et al. 12 reported that the most common consequences perceived by the patients because of DS were weakness in sexual ability (75.6%), closely followed by other consequences like early ejaculation (62.2%) and poor erection (62.2%). Those authors argued that the presence of comorbid sexual dysfunction in patients with DS is secondary to their core belief system. Because of myths and misbelief systems, patients become anxious and anticipate difficulty in sexual functioning. This could be the possible cause of high sexual comorbidity in DS. A multicentric study 15 with samples from various centers of India reported 51.3% of patients to have sexual comorbidities. Several recent studies reported premature ejaculation in 22% to 44% and ED in 22% to 62% of the DS patients.15, 24, 25, 36 The above-mentioned multicentric study reported that 32.4% had premature ejaculation, 20.3% had ED, and 6.3% lacked sexual desire. 15 The reasons for the discrepancy may be that our sample was taken from the treatment-seeking population and that most of the patients were referred from various departments.
Quality of life
Patients with DS had a lower score on WHO QoL-BREF and lower QoL. Patients with DS with comorbidity had poorer QoL than healthy individuals (P < 0.001).
Patients with DS without comorbidity also had poorer QoL (in all the domains of QoL) than healthy individuals (P < 0.001). This suggested that DS per se causes impairment in the QoL.
Patients with DS with comorbidities had significantly poorer QoL (P < 0.001) than those without comorbidities. The relationship between QoL and comorbidities is bidirectional. More comorbidities are expected to compromise the QoL, and in turn, poor QoL may increase subjective distress, increasing the development of comorbid mental illness. The worse QoL among patients of DS with comorbidities can be simply because of the comorbidities themselves than because of DS.
Patients with DS often undergo significant psychological distress because of their symptoms. These symptoms cause impairment in their routine activities. This distress and resultant impairments might contribute to the poor QoL in patients with DS.
Because of the predatory advertisement practices promoted by self-proclaimed sexologists and quacks prevalent in India, which wrongly emphasizes ill consequences of semen loss, patients of DS frequently seek help with self- proclaimed sex specialists, Vaids, Hakim, and local quacks and receive further misinformation. This increases their fear, anxiety, and insecurities. They also spent a significant amount of money and time with them. This situation also leads to increased dissatisfaction and may result in impairment in QoL.
In our study, the mean age of onset of DS was around 24 years, and the mean duration of symptoms was around 4.5 years, which shows DS has a chronic and persistent course. Sexual issues are frequently laden with shame and guilt and are often considered taboo subjects. This leads to delayed help-seeking, and patients often continue to suffer in silence. The cultural and social constraints related to a discussion of sexual topics frequently add to the difficulties in help-seeking for DS-related problems. The information available to such patients is often confusing, contradictory, and incomplete, leading to further confusion and insecurity. Such situations lead to the prolongation of misery and contribute to the poorer QoL in such patients. An earlier study done at our center regarding the pathway of care of patients with DS showed that these patients present late to the mental health professions and would take primary consultation from sex specialists, quacks, Hakims, and Vaids. These patients also spend a lot of money on these consultations.32, 37 This may also add to the impairment in QoL.
In this study, 50.42% of the DS patients had premature ejaculation and 46.15% had ED. These findings are similar to the results of Rosen et al., 38 who reported that patients with ED had poorer psychosocial function than healthy populations, and the emotional domain of QoL was more profoundly affected by ED than the physical domain. MacDonachet al. 39 observed that ED greatly decreases patient satisfaction with their sexual life and partners and has a negative impact on their social relationships.
Disability
This study shows that DS without comorbidity per se causes significant disability. Patients with DS with comorbidities had more disabilities than those without any comorbidity. A study done by Grover et al. concluded that the most common consequence perceived by the DS patients was weakness in sexual ability (75.6%). 12 As per existing literature, patients with DS have various psychiatric and sexual comorbidities.26, 33, 40 The commonly reported psychological and somatic complaints are body weakness; feeling tired or low energy level; feeling down, depressed, or hopeless; feeling little pleasure or interest in doing things; mental weakness; anger; irritability; getting annoyed easily; excessive worry; pains in arms and leg or joints; trouble sleeping; and feeling bad about self. The prevalence of these symptoms was also affected by the presence of comorbidities. Out of these symptoms, bodily weakness is more common in DS patients even without any sexual or psychiatric comorbidities. 12 These factors can cause disability. Earlier studies have not assessed disability in patients with DS. Common mental illnesses like depression have been commonly associated with disability and low productivity of the patients. 41 In our study, the mean duration of illness was more than four years in both groups (A and B). This showed that the course of DS could be persistent and chronic. This may also add to the disability DS.
Limitations
Our sample was small and was taken from a treatment-seeking population from a tertiary center. So, the generalizability of our findings is limited. Being a cross- sectional study, the direction of association between DS and comorbidities cannot be established. As patients with DS often seek multiple consultations before reaching a tertiary care center, recruitment of drug-naïve patients was not possible. We had excluded the diagnosed cases of physical illness, which may be another limitation. Our results need to be validated in a prospective study and a large clinical sample.
Conclusion
Despite being a common and disabling disorder, research on DS remains far from being complete. QoL and disability are very clinically relevant and useful domains. This cross-sectional observational study found that DS patients with and without comorbidities have poor QoL and greater disability in comparison to healthy controls. Patients with additional psychiatric and sexual comorbidities have a poorer QoL and greater disability than patients without comorbidities. Evaluation of disability and QoL in individuals with DS will provide a comprehensive clinical picture, leading to adequate planning and implementation of management strategies for the patients.
Footnotes
Declaration of Conflicting Interests
The authors have no potential conflicts of interest to declare with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.