
Abstract
Background:
Patients with dementia usually have multiple comorbidities. The presence of comorbidities may exacerbate the progression of dementia and decreases the patient’s ability to participate in health maintenance activities. However, there is hardly any meta-analysis estimating the magnitude of comorbidities among patients with dementia in the Indian context.
Methods:
We searched PubMed, Scopus, and Google Scholar, and relevant studies conducted in India were included. The risk of bias was assessed and a random-effects meta-analysis model was used in which I 2 statistics were calculated to measure heterogeneity among studies.
Results:
Fourteen studies were included in the meta-analysis based on the inclusion and exclusion criteria. Altogether, we found the coexistence of comorbid conditions such as hypertension (51.10%), diabetes (27.58%), stroke (15.99%), and factors like tobacco use (26.81 %) and alcohol use (9.19%) among patients with dementia in this setting. The level of heterogeneity was high due to differences in the methodologies in the included studies
Conclusions:
Our study found hypertension as the most common comorbid condition among patients with dementia in India. The observed lacuna of methodological limitations in the studies included in the current meta-analysis provides the urgent need for good quality research to successfully meet the challenges ahead while devising appropriate strategies to treat the comorbidities among patients with dementia.
Dementia, a neurodegenerative disorder associated with population aging, was estimated to have increased by 117% (95% uncertainty interval [UI] 114–121) between 1990 and 2016 globally. 1 There is emerging evidence of decreasing prevalence of dementia in high-income countries such as North America and Europe, due to the increase in educational attainment and improvements in the management of cardiovascular disease and its risk factors.2–3 On contrary, an increase of 197% change (95% UI: 160–238) and an age-standardized rate of 6.4% (95% UI: –3.6–20.4) for dementia is forecasted in India by 2050. This forecasted transition is attributed to changes in population growth, population aging, changes due to education, and risk factors. 4 Globally, 12 modifiable risk factors such as low education, hypertension, hearing impairment, smoking, midlife obesity, depression, physical inactivity, diabetes, social isolation, excessive alcohol consumption, head injury, and air pollution were associated with dementia.5–7 In India, the risk factors for dementia were observed as vascular and metabolic (diabetes, hypertension, dyslipidemia, obesity, stroke, high BMI), genetic (Apolipoprotein 8 Presenilin-1), 9 and other risk factors (gender differentials, 10 nutritional deficiencies, 11 low literacy, change in social system urban living). 12
Worldwide literature on the comorbidities in dementia suggest prevalence rates of 6%–39% for diabetes, 13 3%–34% for stroke, 13 15.9% for major depressive disorder, 14 20% for depression, 15 14% for anxiety, 15 and 4.4% for post-traumatic stress disorder. 15 The corresponding rates are likely to be different in India due to the differences in socioeconomic status, lifestyle, and literacy, as well as access to health care and the internet. Further, the increasing prevalence of multi-morbidities and the underdiagnosed and undertreated medical illnesses, particularly in rural Indian settings, complicates studying the comorbidities of dementia. 16 Understanding the burden of comorbidities among dementia patients is critical to addressing future changes in modifiable risk factors that might influence the trajectory of trends in age-specific prevalence. The changes in the brain leading to dementia start at least two decades before the presentation of overt clinical symptoms. 17 In this context, it is important to quantify the burden of comorbidities and/ or multi-morbidities among dementia patients in India, to advance the strategies for prevention.
Methods
The meta-analysis was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and was registered in the PROSPERO database (CRD42022321019)
Search Strategy and Selection Criteria
We searched the following electronic bibliographic databases: PubMed, Scopus, and Google Scholar. To prevent omissions, a snowball search was conducted for references to include articles and relevant reviews to supplement the relevant literature. We used the combination of Medical Subject Headings and keywords of the following search concepts: “dementia”; “comorbidity”; “India.” The details of the search strategy in PubMed are given as Supplementary Material 1. The data search was carried out by two investigators (HH and VLN). The archives of relevant Indian journals were reviewed for maximum inclusion of the available studies. The screening of the potentially eligible studies was performed by two investigators (BV and MD) who further appraised the full texts of appropriated records to reach a common consensus regarding the inclusion and exclusion of individual studies.
Inclusion and Exclusion Criteria
Observational studies (hospital and community-based studies) conducted in the Indian setting reporting the comorbidities in patients with dementia and published in the English language were included. Studies were included if participants had dementia based on standard diagnostic or screening criteria. Global or Indian prevalence or incidence studies that did not estimate the comorbidity among patients with dementia were excluded. Besides, studies with inadequate data and studies that exclusively evaluated cognitive deficits without diagnosis/screening for dementia were excluded.
Data Extraction
The data extraction was done based on the following study characteristics: namely author (year of publication), period of study, study type, criteria for dementia, sample size, gender, age, education, comorbid conditions such as hypertension, diabetes, dyslipidemia, tobacco use, alcohol use, family history of dementia, history of stroke, etc. Two investigators (BV and SG) were involved in the preparation of the data extraction table based on the eligibility criteria. The extracted data were cross-verified by the author EM. A mutual consensus resolved disagreements between the authors (BV, SG, and EM).
Quality Assessment
The JBI Critical Appraisal Checklist was used for the risk of bias assessment (Available from
Statistical Analysis
The R software was used to perform this meta-analysis, and the pooled estimate of outcome measures was estimated using inverse-variance weighting methods (Available from:
Results
Identification of Studies
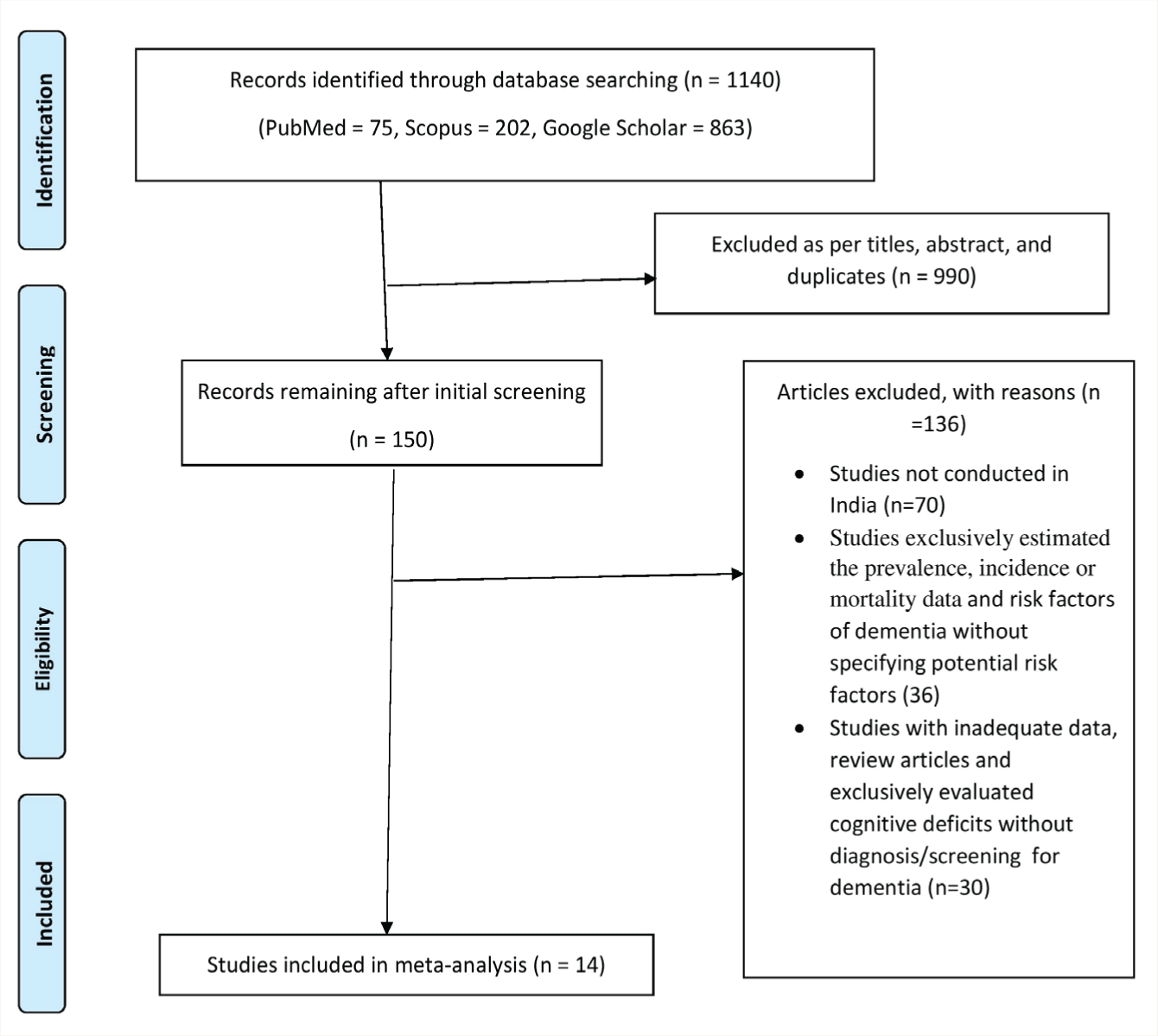
The database search identified 1140 reports: 990 were excluded based on title and abstract screening and after eliminating duplicates, 150 articles were retrieved for detailed evaluation, and 136 of these were excluded for the reasons summarized in Figure 1. Finally, 14 eligible articles were included in the meta-analysis.
Flow chart of search stretegy and selection process.
Study Characteristics
The sample size ranged from 27 to 1777 in which the age of the study subjects was mainly in the early sixties (Table 1).18–31 The studies recruited study participants from the hospital-based setting19, 21–26, 29 and community-based population.18, 20, 27, 28, 30, 31 Half of the studies were conducted in the southern part of India19, 20, 23, 26, 29–31 and the period of conducting the studies ranged from 2003 to 2017. The assessment of dementia was most commonly done by using a Mini-Mental status examination.19–21, 23–31 Other scales used to measure dementia include the Clinical Dementia Rating Scale, 22 Early Dementia Questionnaire, 18 Community Screening Instrument—Dementia, 29 Geriatric Mental State. 30 Around 55% of the dementia patients with comorbidities were males (55.4%; 95% CI: 46.64–63.84) while the proportion of females was 44.6% (95% CI: 36.16–53.36). The total score of risk of bias assessment according to the JBI Critical Appraisal Checklist for analytical cross-sectional studies was 8 and the score ranged from 1 to 5. The mean risk of bias score was 3 and the median score was 1 indicating a high risk of bias in the included studies. A major proportion of the studies did not provide detailed descriptions of the study settings. Out of the 14 studies, the information on the procedures for the measurement of the various comorbidities of dementia was reported only in six studies. None of the studies listed the possible specific confounding factors and did not state the strategies to deal with the same. Appropriate statistical analyses were not performed in the majority of the studies. The details of the quality assessment of the studies using the JBI checklist are described in Table 2.
Characteristics of the Studies Included in the Meta-analysis (N = 14).
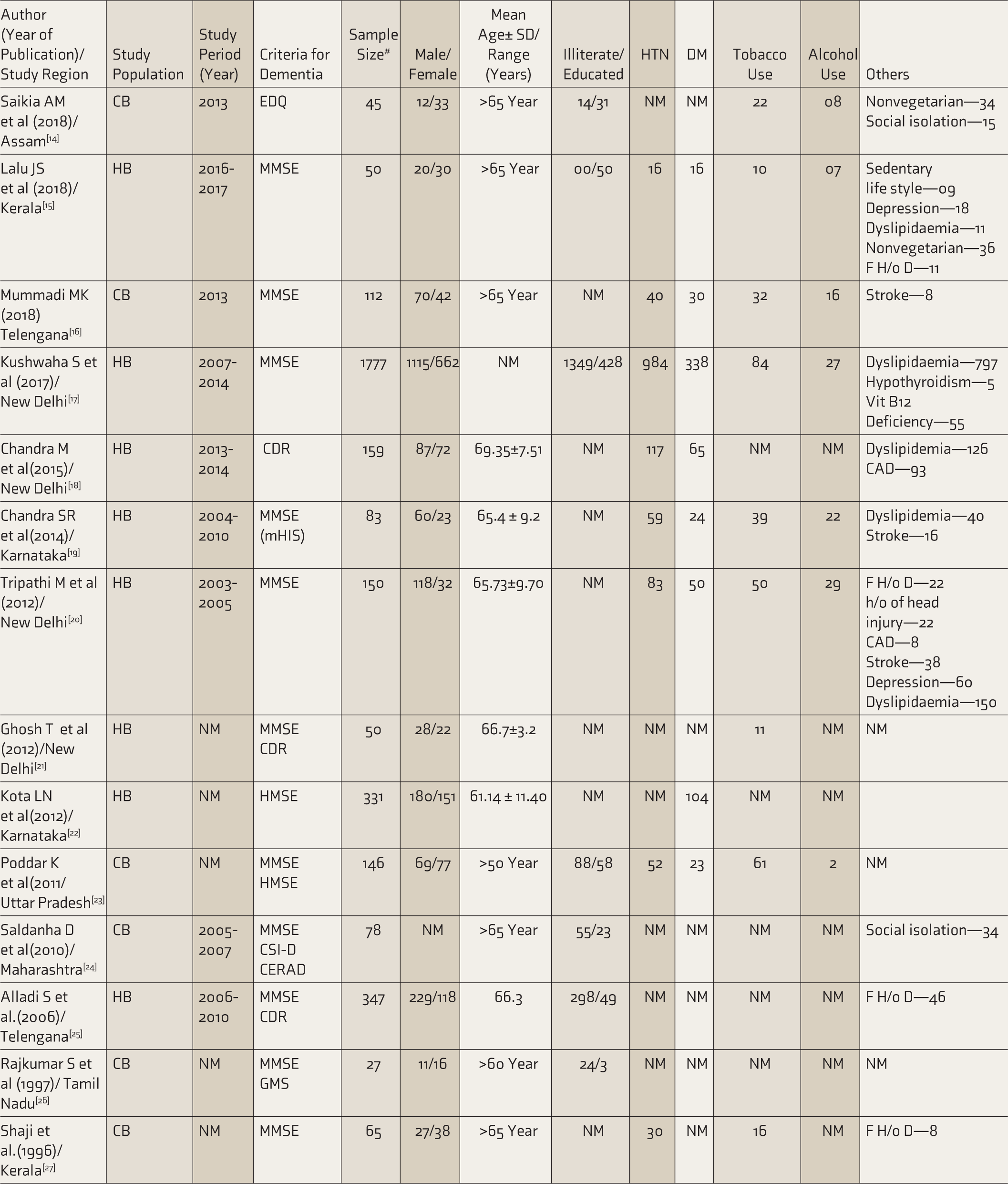
NM: not mentioned, CBS: community based, HBS: hospital based, EDQ: early dementia questionnaire, MMSE: mini-mental status examination, HTN: hypertension, DM: diabetes mellitus, AD: Alzheimer’s dementia, VD: vascular dementia, CDR: clinical dementia rating scale, MINI: mini international neuropsychiatric interview, mHIS: modified Hachinski ischaemic scale, CSI-D: community screening instrument—dementia, GMS: geriatric mental state, F H/o D: family history of dementia. #The subjects with dementia based on a criterion.
Risk of Bias Assessment of Included Studies.
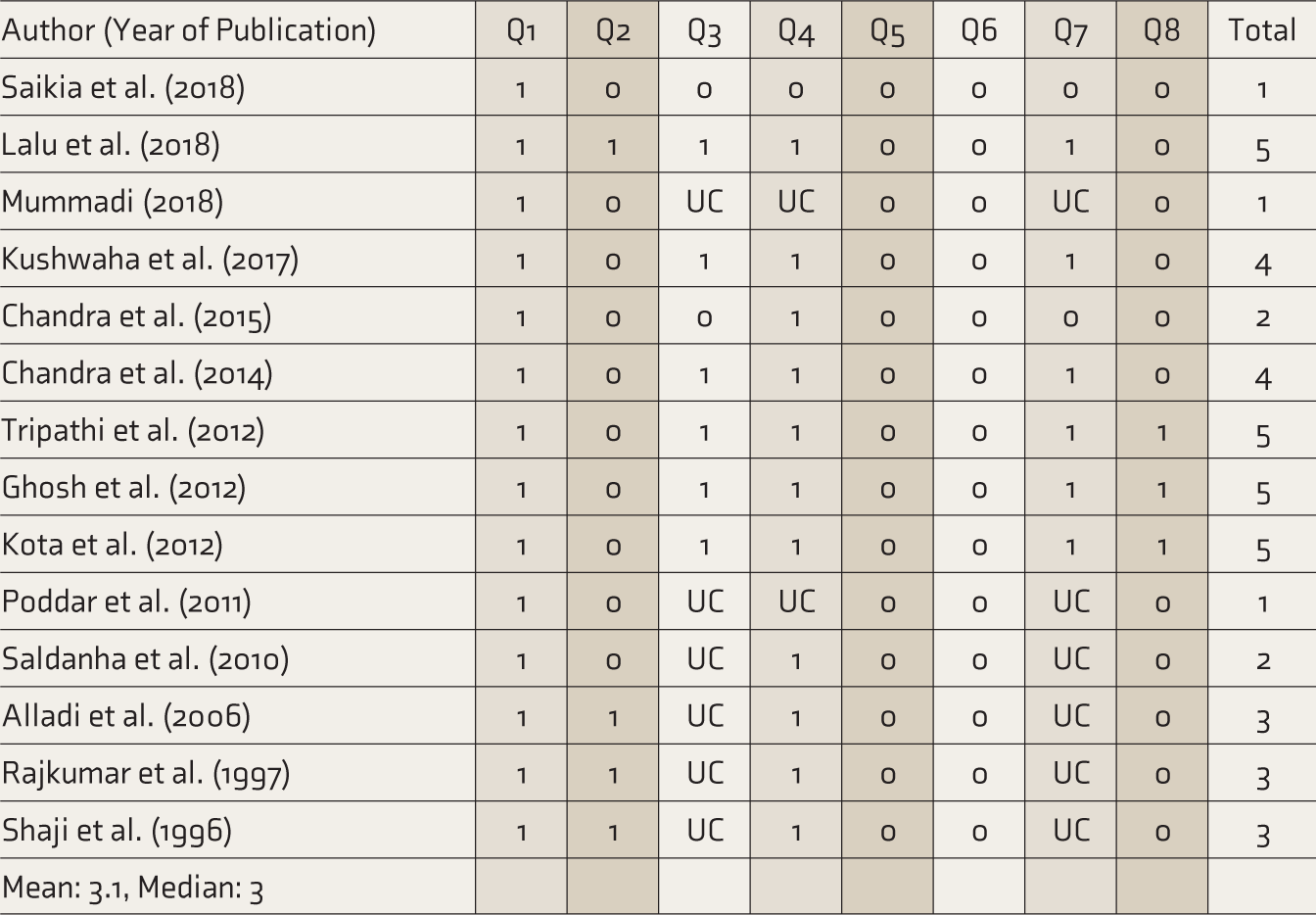
Q1: Were the criteria for inclusion in the sample clearly defined? Q2: Were the study subjects and the setting described in detail? Q3: Was the exposure measured in a valid and reliable way? Q4: Were objective, standard criteria used for measurement of the condition? Q5: Were confounding factors identified? Q6: Were strategies to deal with confounding factors stated? Q7: Were the outcomes measured in a valid and reliable way? Q8: Was appropriate statistical analysis used? (1—Yes, 0—No, NA—Not applicable, UC—Unclear).
Comorbidities
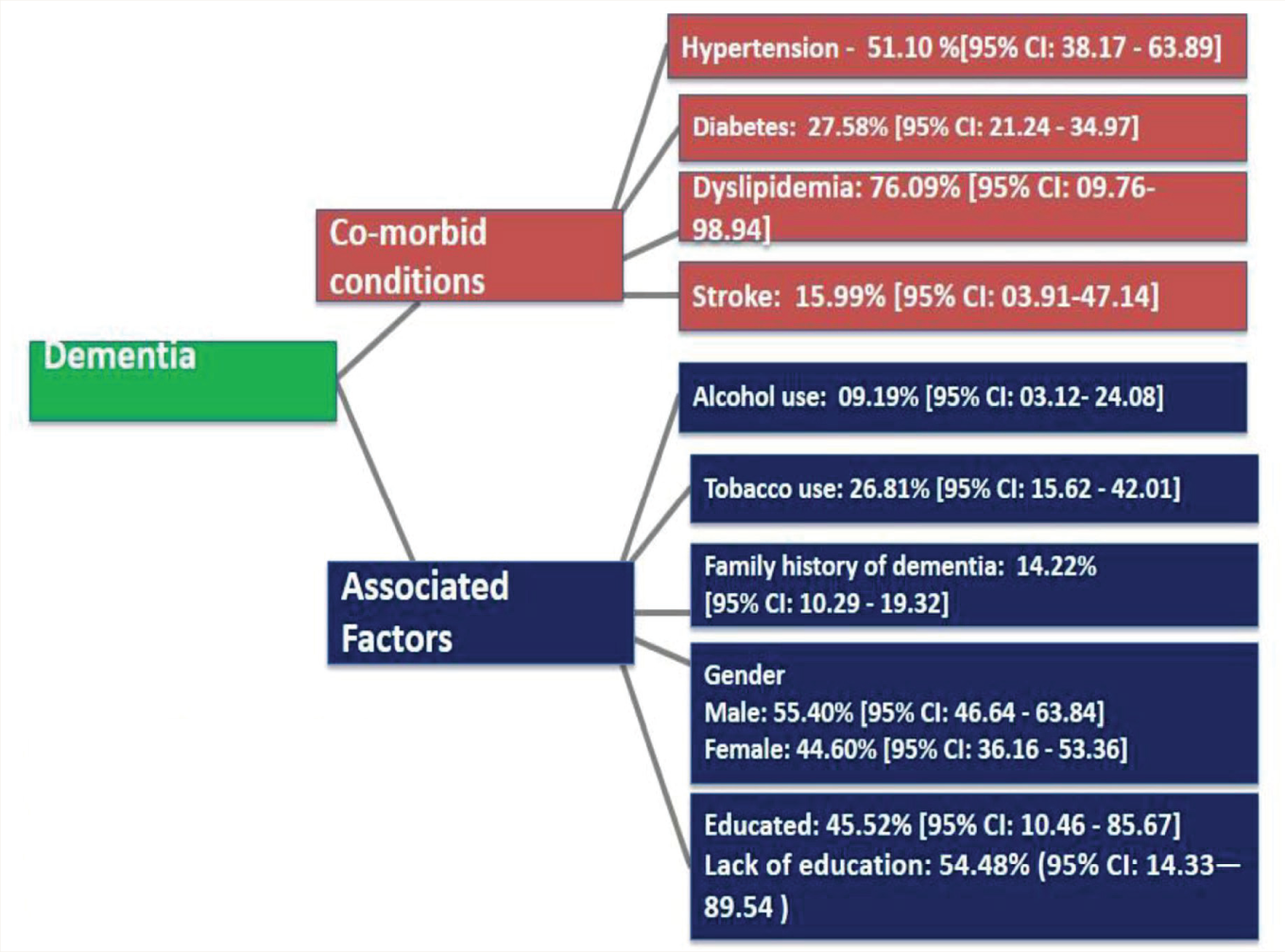
Dementia being a chronic illness, we identified the comorbidities and the associated factors based on the cross-sectional studies conducted in the Indian setting (Figure 2). Of the 2542 patients included in the analysis from 8 studies, the pooled proportion of dementia patients with hypertension as comorbid condition was 51.1% (95% CI: 38.17–63.89).19–24, 27, 31 Overall, 2808 patients were included in the analysis from 8 studies for detecting the pooled proportion of dementia patients with diabetes mellitus which was found to be 27.58% (95% CI: 21.24–34.97).19–24, 26–27 The other comorbidities associated with dementia patients were dyslipidemia (76.09%; 95% CI: 10–99; n = 5 studies)19, 21–24 and stroke (15.99%; 95% CI: 03.91–47.14; n = 3 studies).20, 23–24 Two studies reported depression (36% and 40%)19, 24 and coronary artery disease (5.3% and 58.8%)22, 24 as comorbid conditions associated with dementia in this setting. One study reported the presence of hypothyroidism (0.2%) and vitamin deficiency (3.09%) in treatment-seeking patients with dementia. 21
The distribution co-morbid conditions and associated factors among patients with dementia in India.
Associated Factors
The history of tobacco use, both smoking and smokeless forms was 26.81% (95% CI: –15.62–42.01; n = 9 studies)18–21, 23–25, 27, 31 and alcohol use was 9.19% (95% CI: –03.12–24.08; n = 7 studies).18–21, 23–24, 27 Approximately 55% of the patients were illiterate (54.48%; 95% CI: 14.33–89.54) and the remaining subjects had undergone formal education (45.52%; 95% CI: 10.46–85.67).18–19, 21, 27–30 The family history of dementia was reported in 14% of the subjects (14.22%; 95% CI: 10.2–19.32; n = 4 studies).19, 24, 29, 31 The presence of social isolation (33.3% and 43.6%)18, 28 and nonvegetarian diet (75% and 72%) were reported among patients with dementia in two studies.18, 19 One study reported sedentary lifestyle patterns (18%) in treatment-seeking patients with dementia. 19
We used the random-effects models to calculate the pooled estimates as there was a significant heterogeneity on the outcome measures (hypertension—I 2 = 91%, Tau Squared = 0.35, P < 0.01; diabetes mellitus—I 2 = 90%, Tau Squared = 0.13 P < 0.01; dyslipidemia—I 2 = 94%, Tau Squared = 6.81, P < 0.01; tobacco—I 2 = 98%, Tau Squared = 0.72, P < 0.01; alcohol—I 2 = 96%, Tau Squared = 1.39, P < 0.01; stroke—I 2 = 85%, Tau Squared = 0.3, P < 0.01; previous history of stroke—I 2 = 96%, Tau Squared = 0.61, Q = 447.43, P < 0.01; family history of dementia—I 2 = 92.6%, Tau Squared = 0.70, Q = 162.83, P < 0.001). The pooled analysis of the proportion of individual predisposing factors and heterogeneity are depicted in supplementary materials (S2.1–2.7). The funnel plot and Egger’s test regarding the publication bias of individual predisposing factors were not evaluated as the number of studies was less than 10.
Discussion
Early recognition of comorbidities and associated factors of dementia has been identified as a potential strategy for decreasing the severity of the disease process. Patients with dementia usually have multi-morbidities. However, there is hardly any meta-analysis estimating the magnitude of comorbidities and/or multi-morbidity among patients with dementia in the Indian context. Around the world, hypertension is a common comorbidity in adults with major chronic illnesses, with a prevalence rate of more than 50% in the Asian population. 32 Our study found that 51% of patients with dementia had hypertension as a comorbid condition. These findings are in line with a previous study conducted in Europe that identified hypertension as a major comorbid condition among patients with dementia. 33 Diabetes is also considered an established risk factor for dementia, 34 and our analyses suggested that the proportion of diabetes mellitus among patients with dementia is 27.58%. This proportion is, however, considerably lower than the results obtained in a study from Germany. 35
According to the current meta-analysis, the proportion of dyslipidemia in dementia patients was 76% (95% CI: 10%–99%); however, the wide confidence interval of the pooled proportion questions the validity of these findings within this setting. Our aggregates of evidence revealed that the proportion of stroke among patients with dementia was 15%. The evidence across the globe strongly suggests stroke is an independent and potentially modifiable risk factor for dementia. 36 As dementia is a disorder developing slowly over many years, it is often identified in the late course of the disease. Besides, it could be possible that patients with an earlier stroke were not examined for dementia, which might have affected the pooled analysis of the proportion of stroke in patients with dementia in this setting. Our study showed that around 9% and 26% of the patients with dementia reported a history of alcohol use and tobacco use. Similar findings were observed in other studies which identified a significant association between smoking and alcohol use in patients with dementia.37–38 The existing evidence indicates various genetic factors for dementia 39 and the current study identified a family history of dementia in 14% of the subjects. Our study identified that other conditions such as depression, coronary artery diseases, and social isolation were reported in dementia patients but the number of studies was relatively low for estimating a pooled proportion.
It is evident that the comorbid medical conditions may exacerbate the progression of dementia and increases the vulnerability of the patient’s ability to health maintenance activities. 40 Altogether, we found the coexistence of comorbid conditions such as hypertension, diabetes mellitus, dyslipidemia, tobacco use, and alcohol use among patients with dementia in this setting. However, the risk of bias assessment of the included studies has implications for the generalization of our findings. First, there was a high risk of bias in the studies included in the current meta-analysis. Reporting was incomplete in most studies. To cite, the existing evidence suggests that the associated factors for dementia may vary according to different age groups. 41 However, the proportion of comorbidities according to gender and age groups was not reported in the majority of the included studies. Furthermore, with increasing age, the propensity of occurrence of multi-morbidities is higher, which could worsen dementia. We could not estimate the prevalence and pattern of multi-morbidities due to the inherent data limitations. Second, as the case-control studies were very limited we could not substantiate the risk factors with dementia, but the associated factors. Further, overlapping comorbidities were not reported in the majority of the studies. Third, the meta-analysis showed significant heterogeneity which is commonly observed in epidemiological studies and could be attributed to several factors such as differences in defining, measuring, and analyzing outcomes; criteria for patient selection; study objectives; and statistical analysis. Though the studies we analyzed were cross-sectional and do not prove causation, based on evidence from other parts of the world, the factors we identified are known to increase the risk of dementia. Hence, older adults, their family members, clinicians, other health workers, and policymakers should be sensitized about these factors and the importance of their early detection and management to reduce the burden of dementia in a country where the proportion of older adults is gradually increasing.
There are certain limitations to generalizing our findings. The results are purely based on cross-sectional studies with methodological limitations. The level of heterogeneity of the included studies was high due to differences in the study contexts. No attempts were made to acquire grey/unpublished literature considering the inherent conflict of interest which might increase the risk of bias. The age and gender-specific proportion of comorbidities of dementia were not reported in the majority of the included studies. A major strength of this study was that we were able to generate the pooled estimates of the comorbidities and associated factors among patients with dementia based on the epidemiological studies conducted in the Indian setting.
Conclusion
Our study found hypertension to be the most common comorbid condition among patients with dementia in this setting. The observed lacuna of methodological limitations in the included studies in the current meta-analysis suggests that there is an urgent need for good quality research to successfully meet the challenges ahead while devising appropriate strategies to curtail the comorbidities among patients with dementia. Future research exploring the role of multi-morbidity in the onset and progression of dementia is warranted.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Elezebeth Mathews would like to thank DBT, India for the Clinical and Public Health Early Career Fellowship (grant number IA/CPHE/17/1/503345).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.