
Abstract
Background:
Attention deficit hyperactivity disorder (ADHD) is the most common neurobehavioral disorder among children, with an estimated prevalence of 1.3 per 1000 in India. The nationwide lockdown imposed due to the COVID-19 pandemic has led to the closure of schools for an indefinite period. After the reopening of schools, the lockdown period was feared to have caused a deterioration in symptoms of existing mental health conditions among school-going children. This field study aimed to probe the association of school closures due to lockdown with any change in symptoms of ADHD in aged 6–15 years in the largest tertiary care hospital in Kolkata.
Methods:
A longitudinal observational study was conducted involving 34 prediagnosed ADHD patients attending the Clinical Psychology outpatient department (OPD) of a tertiary hospital for follow-up. Data was collected by face-to-face interviews with the patients’ parents using a predesigned, pretested structured study schedule. Conners’ Parent Rating Scale (CPRS) was used to assess the ADHD symptoms.
Results:
Twenty-three (67.65%) patients were observed to have worsened ADHD symptoms after lockdown. Significant worsening was observed in the ADHD indicator and the mood disorder indicator. Significant contributing factors were rural residence, nuclear family, non-attendance at school, and knowledge inadequacy among parents.
Conclusion:
There was a significant worsening of symptoms of ADHD owing to the school closure due to the lockdown.
Keywords
The school environment is important for the overall nurturance of the mental faculty in childhood. The drastic measure of school closure for a prolonged period, as adopted during the COVID lockdown, may serve some temporary respite in exigencies but is detrimental, especially in children with pre-existing mental health needs like ADHD. Policymakers should consider this aspect seriously while notifying similar decisions about school closures in future emergencies.Key Message:
Attention deficit hyperactivity disorder (ADHD) is the most common neurobehavioral disorder in childhood. In India, its prevalence was estimated at 1.3 per 1000. 1 The COVID-19 pandemic has led to a nationwide lockdown in India. In West Bengal, schools were closed continuously for children up to Class 8 from the first lockdown (April 2020) to the third wave of the COVID-19 pandemic (February 2022). Perhaps the most affected among school-going children were those who have ADHD. First, the lockdown restricted them inside homes with minimal outdoor activity. These conditions may have aggravated their symptoms. 2 Second, children with ADHD have problems sitting in one place and concentrating persistently for long. So, the sudden shifting of the educational platform from “offline” to “online” might have just added to the academic challenges they faced. Third, school closure has led to decreased teacher–student interaction. Many times, symptoms of ADHD are identified by teachers in their schools. 3 Such changes were substantially reduced during the lockdown. Lastly, the lockdown had brought the country’s economy to a standstill, and many people were pushed to extreme poverty, with many suffering significant economic losses. That might have further prevented the parents of such children from seeking medical help. Very little research has been conducted and published focusing on the effect of school closure on ADHD in India. 4 A few online surveys have been conducted to study the association between school closures due to lockdown and the worsening of ADHD symptoms. However, to the best of our knowledge, no field-based study on this topic has been conducted in India till the date of commencement of this study. Recently, an online survey that evaluated the impact of the COVID-19 lockdown on children with ADHD and their families revealed that the COVID-19 lockdown led to worsening symptoms of ADHD in the form of an increase in activity level, irritability, and disturbing and disruptive behaviors among children. 2
This research aimed to study the association of school closures due to lockdown with worsening symptoms of ADHD in children aged 6–15 in the largest tertiary care hospital in Kolkata, West Bengal. Its primary objective was to compare the symptoms of ADHD before lockdown from the data repository in the Department of Clinical Psychology of this hospital with the symptoms of ADHD after lockdown in children who were on regular medication and/or psychological intervention during that period.
The secondary objective of the study was to assess the knowledge and perceptions regarding ADHD among parents of children with ADHD.
Materials and Methods
It is a longitudinal observational study. The data was collected from the Outpatient Department (OPD) of the Department of Psychiatry and the Department of Clinical Psychology in the said tertiary care institute between 25 July 2022 and 25 September 2022, for 2 months. As schools in West Bengal were closed continuously from April 2020 to February 2022, this period was considered the “lockdown period.” The period before April 2020 was considered the “pre-lockdown period” and that after February 2022, the “post-lockdown period.”
Study Sample
Parents of children in the age group 6–15 years, enrolled in school who were clinically diagnosed with ADHD before lockdown school closure as per Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5) 5 and attending OPD of the Department of Psychiatry and Department of Clinical Psychology of the institute were taken up. Parents of children with other etiological factors that may promote symptoms mimicking ADHD and parents of children who had stopped taking medications, leading to the worsening of symptoms, were excluded.
Sample Size and Sampling Technique
This study was conducted as a part of the Short-Term Studentship (STS) program of the Indian Council of Medical Research (ICMR). Before submission of the protocol to the Institutional Ethics Committee, a pilot assessment was conducted for about 1 week to estimate the number of patients fulfiling the inclusion and exclusion criteria and attending the Psychiatry and Clinical Psychology OPD. Initially, a target sample of 40 was kept. However, within the stipulated time duration, a total of 34 samples were collected.
Materials Used
A predesigned, pretested, structured study schedule was prepared with the following subsections: sociodemographic profile, academic profile, knowledge and perception regarding ADHD, and Conners’ Parent Rating Scale (CPRS). A participant information sheet was prepared in English, Bengali, and Hindi to provide information to the participants.
Study Variables
Independent Variables
Sociodemographic and Academic Profile
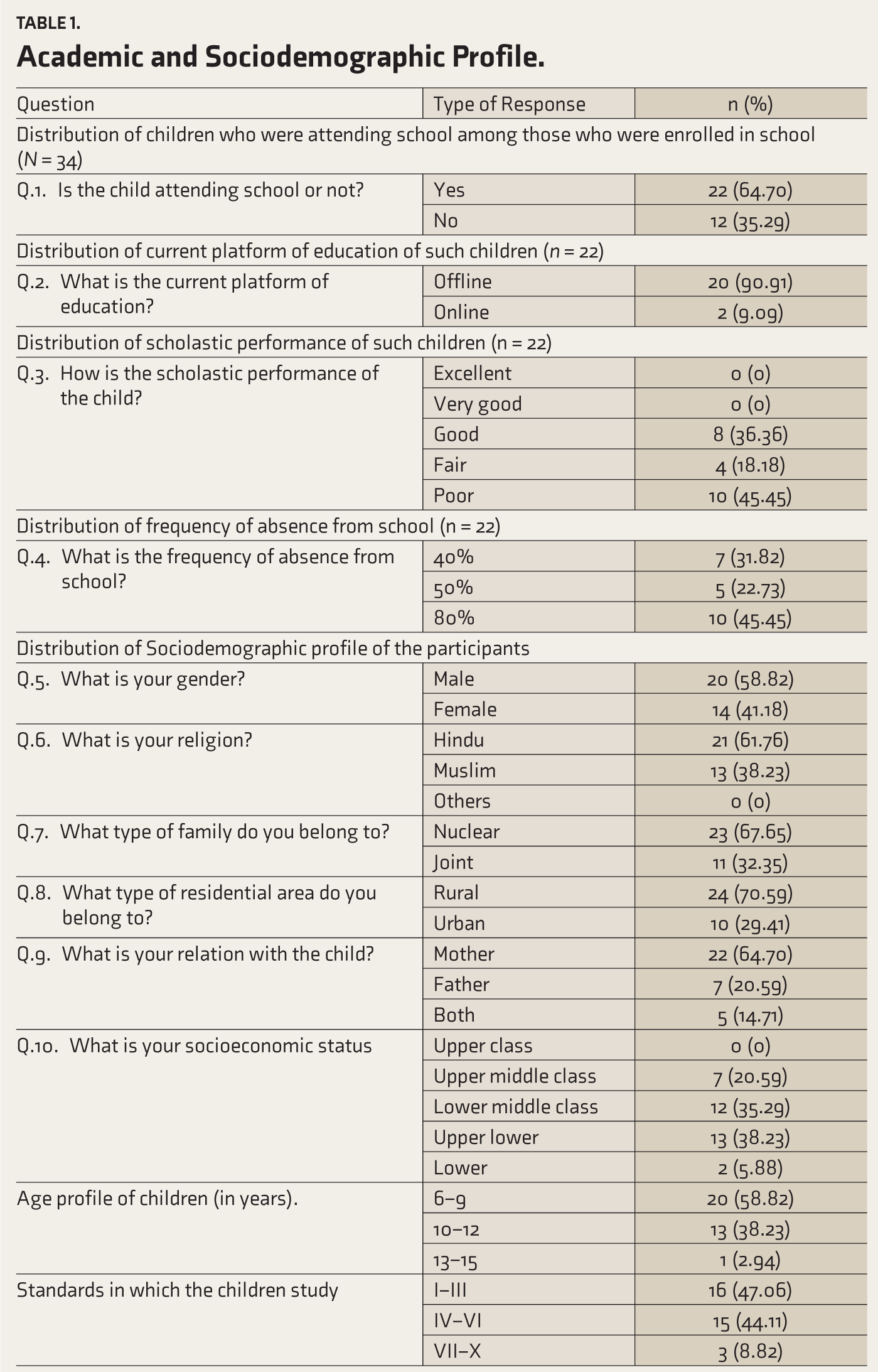
Age of the child (in completed years), sex, residence, type of family and socioeconomic status (modified Kuppuswamy Scale), attending classes or not, current educational platform (offline/online), scholastic performance, frequency of absences from school.
Knowledge and Perceptions Regarding ADHD
Whether have heard about ADHD, the source of information, whether they think that ADHD is a real disease or not, the cause of ADHD, symptoms, treatment, curable or not, some questions were extracted from the Knowledge of ADHD (K-ADHD) scale. 6 .
Dependent Variable
All the children were diagnosed as having ADHD by the consultants in Psychiatry in the treating hospital, and all of them were assessed by the shorter version of Cooners’ Parent Rating Scale before the lockdown school closure. All of them were carrying the assessment report and their other treatment documents.
Part D: CPRS
CPRS can evaluate a broad range of psychopathology and behavioral symptoms in children apart from ADHD, like disruptive behavior disorders, mood disorders, anxiety disorders, and learning and language disorders. 7 Multiple forms of the Conners’ Rating Scale exist, like the self-report instrument, the parent rating, and the teacher rating. This study used the 24-item shorter version of CPRS as it was the most suitable and comprehensive for the study condition and study sample. This scale has very high internal consistency.
In the tertiary hospital where the study was conducted, which is a regional Centre of Excellence, this scale is most commonly used for routine clinical assessment of ADHD in children. The scale was owned by the Department of Clinical Psychology, and the department has a translated copy of it in the local language, which they developed following appropriate methods of translation and back translation. So, using this scale was considered appropriate for evaluating the worsening of ADHD symptoms. Each item is rated on a four-point scale from “not at all true” (0) to “very much true” (3). All the item scores are then summed up to get the raw scores, which are then converted to standardized scores, known as T-scores.
There are different categories:
A T-score of >70 indicates a very elevated range (many more concerns than are typically reported). A T-score of 65–69 indicates an elevated score (more concerns than are typically reported). A T-score of 60–64 indicates a high average score (slightly more concerns than are typically reported). A T-score of 40–59 indicates an average score (typical level of concern). A T-score <40 indicates a low score (fewer concerns than are typically reported).
8
Data Collection
Approval was obtained from the Institutional Ethical Committee.
The parents were approached and informed written consent was obtained.
A face-to-face interview was conducted with the predesigned, pretested structured study schedule, and the responses were recorded.
The pre-lockdown data was collected from the case files brought by the parents.
Data Analysis
The data was checked for completeness and consistency. All 34 study participants were included in the analysis. Data was entered in Microsoft Office Excel 2010 and SPSS Version 20 and analyzed. Descriptive statistics were used to summarize the findings. A paired t-test was performed to find the association between school closure and the worsening of symptoms. A chi-square test was performed to find the association between the study variables and the worsening of symptoms. The significance level was set at p < .05.
Quality Control
The study schedule used for this research was validated.
A valid and reliable scale was used.
The data collected was kept confidential and anonymous by the source.
Results
Sociodemographic and Educational Profile
The sociodemographic and academic profiles of the participants are shown in Table 1.
Academic and Sociodemographic Profile.
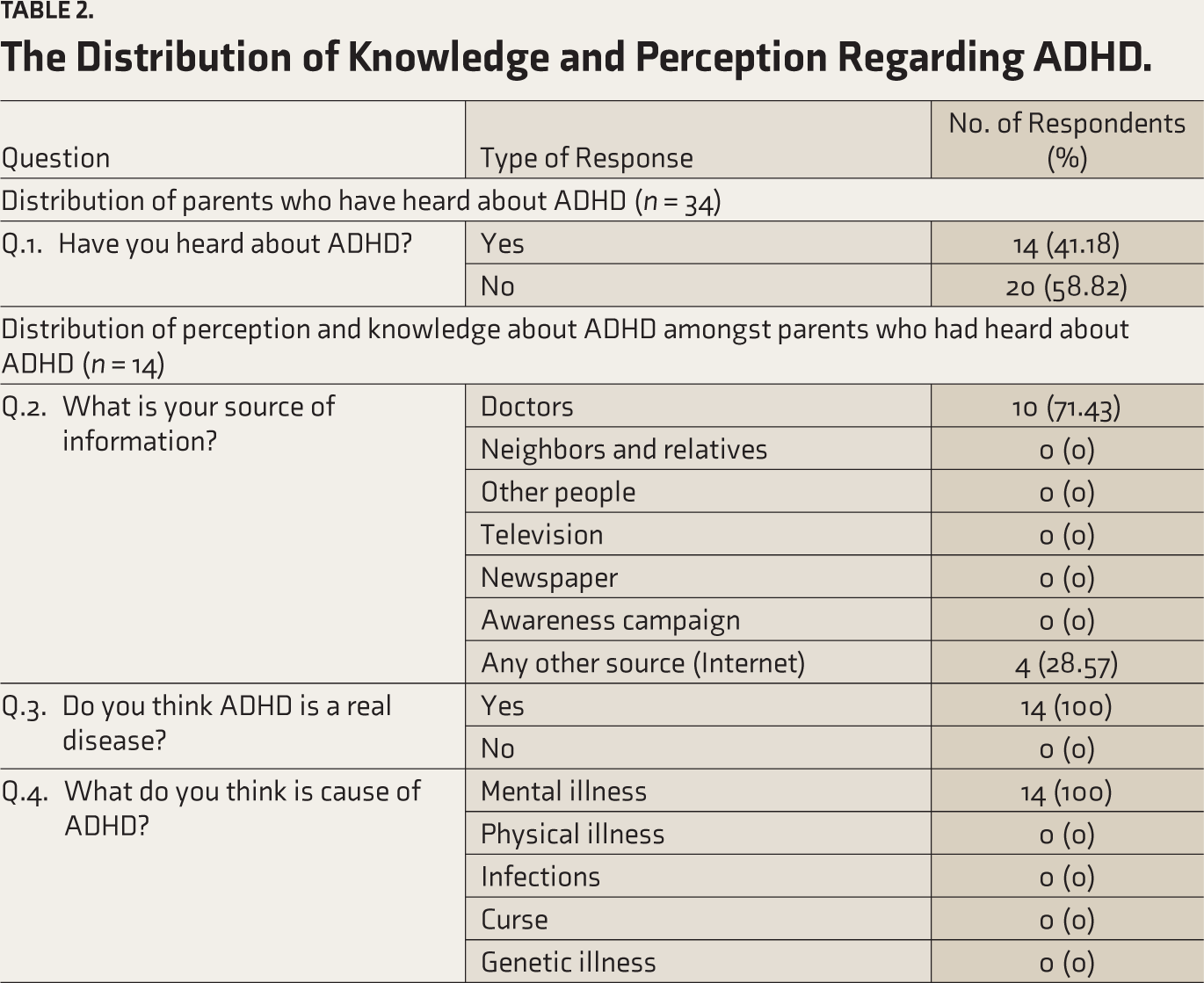
Knowledge and Perceptions Regarding ADHD
A total of 14 questions were asked. Q.3–Q.14 tested the knowledge and perceptions of the parents. Each right answer was awarded 1 point, and each wrong answer was awarded 0 points. Unanswered questions were also awarded 0. A score in the range of 0–12 was possible to be obtained. Parents who said they had not heard about ADHD were directly given 0 points and did not proceed with other questions. A score of >8 (66.67%, i.e., two-third of the total score) was considered “adequate” knowledge. A score of ≤8 was considered “inadequate” knowledge. The individual scores of the participants were calculated. A mean score of 3.85 was obtained, with a standard deviation (SD) of 4.75.
Ten (29.41%) participants were categorized as having “adequate” knowledge.
Impact of the Lockdown on ADHD Symptoms
Twenty-three patients (67.65%) were found to have worsening symptoms. The mean of the calculated T-scores of the CPRS before and after lockdown is shown in Table 3. The paired t-test revealed a significant worsening of the ADHD indicator (p < .001) after the lockdown period. Significant worsening was also observed in the mood disorder indicator (p < .001). No significant changes were observed in other indicators.
The results of the association between sociodemographic characteristics, academic profile, and knowledge adequacy and worsening symptoms are shown in Tables 1–3.
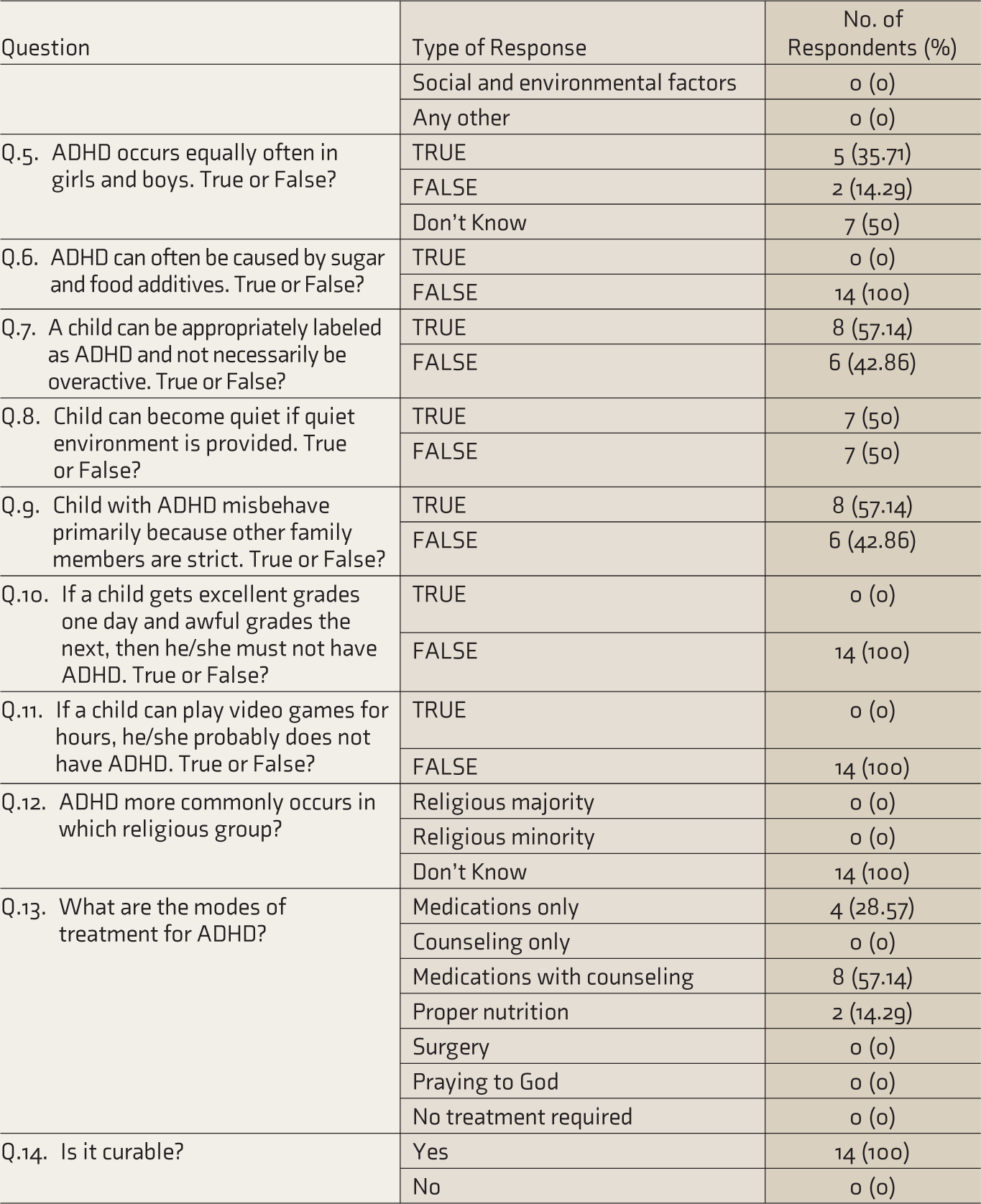
The Distribution of Knowledge and Perception Regarding ADHD.
Association Between School Closure During Lockdown Period with Worsening of Conners Parent Rating Scale indicators.
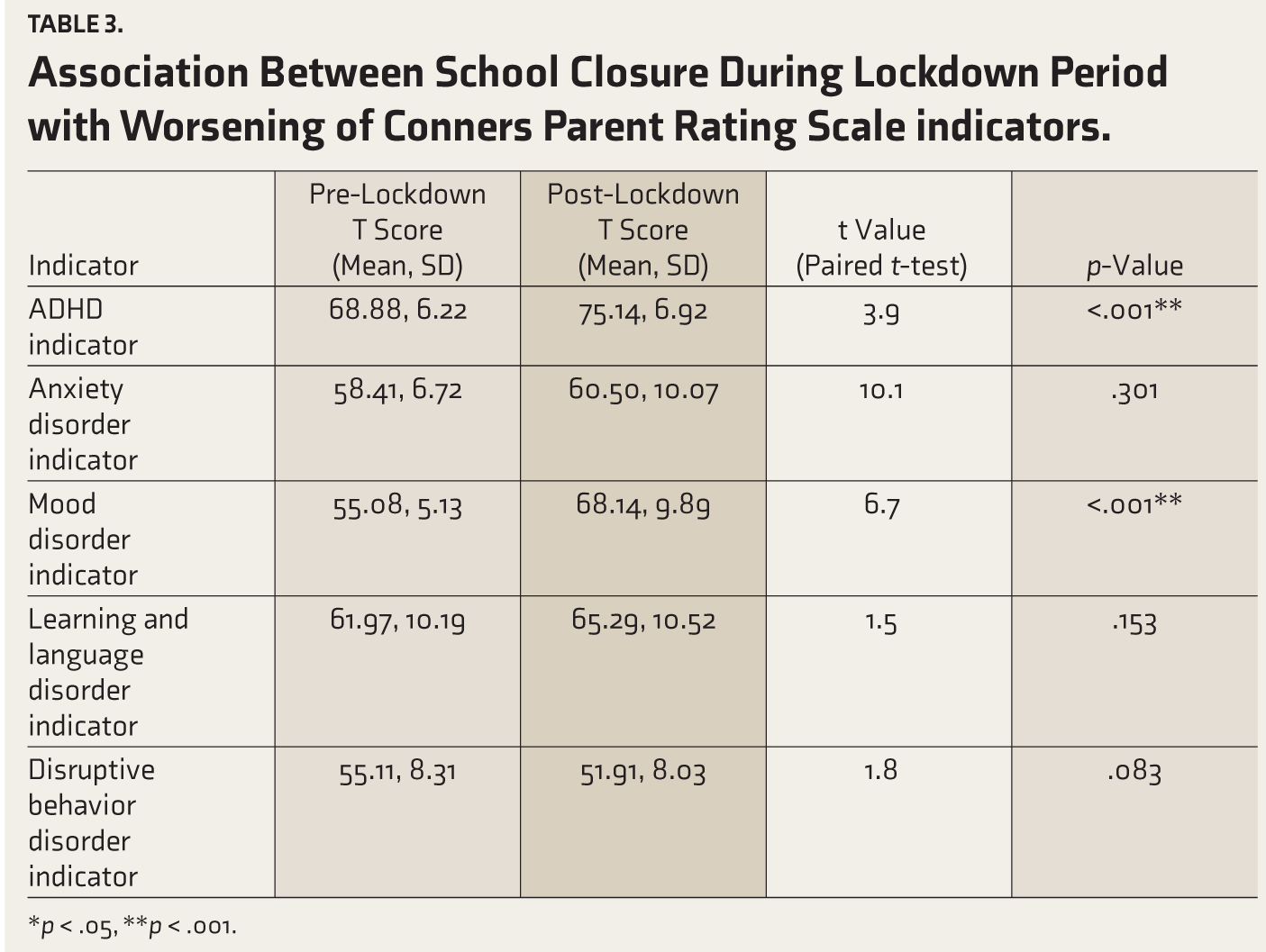
*p < .05, **p < .001.
In the chi-square test, a significant association of worsening ADHD symptoms was observed with rural residence (p = .002), nuclear families (p < .001), Hindu religion (p = .035), non-attendance at school (p = .027), and knowledge inadequacy among parents (p < .001).
No significant association was observed with the gender, age, or socioeconomic class of the child.
Discussion
Impact of School Closures on ADHD Symptoms
There was a significant change (6.26 ± 0.7; p-value < .001) in the ADHD indicator post-lockdown period. This finding corroborated previous studies from China, Canada, Japan, and India that found a worsening in symptoms.2,9-11 This result was expected considering the environment to which the children were exposed. There was decreased interaction with classmates and teachers and minimal outdoor activity. The children were bound to their homes, not only because their schools were closed but also due to fear of contracting COVID-19. This led to the children becoming more impulsive, aggressive, and hyperactive. Also, because, during this time, most parents were confined to their homes as well, they could pay better attention to their child’s behavior. Thus, the parents who spent more time at home noticed their child’s symptoms. Also, as researchers in Kolkata, West Bengal, have found an association of ADHD symptoms with increased stress levels among parents of such children, such conditions might have forced the parents to unleash increased amounts of verbal and physical abuse on their children. 12 This, in turn, might have caused a further worsening of symptoms. 12
One online “text message-based” survey that assessed the impact of the COVID-19 lockdown on children with ADHD and their families revealed certain positive findings, like better creativity. 2 We did not find such a positive outcome because of less access to electronic communication devices and rural disadvantages. One of the significant contributing factors is online education. Some of them were unfortunate to have no smartphone and/or internet connection owing to their financial conditions. Researchers in Canada observed that increased digital media usage negatively impacted children with ADHD. 10 This can also be a possible cause behind the worsening of symptoms, as the lack of physical activities during the lockdown period increased the children’s exposure to digital media by multifold.
To the best of our knowledge, no previous study has assessed the association of worsening ADHD symptoms with sociodemographic characteristics, academic profile, or knowledge adequacy. We found a significant association between the deterioration of symptoms and the rural residence of the children. This can majorly be blamed on the decreased availability of health resources in rural areas. As many parents noted, traveling from their villages to the city for treatment purposes was too hectic. Also, during the lockdown, means of transport became very limited and unaffordable. Low socioeconomic class per se was not significantly associated with the deterioration of the condition, as treatment in the study hospital was free of charge.
Another significant association found was with the nuclear family setting. Unlike nuclear families, joint families have more family members to attend to the emotional needs of the children, and thus, very rarely do such children feel lonely. In nuclear families, both parents are often busy in their workspace, and there is no one to pay attention to their child. Moreover, unlike joint families, verbal and physical abuse is increasingly unleashed on children unrestrictedly in nuclear families. 2 Regarding religion, the researchers could not think of any possible explanation for the significant association. More research is needed in this regard.
Children who were not attending school even during the study duration, which was the post-lockdown period, were also found to have significant deterioration of their symptoms. This can be explained by the fact that the post-lockdown period is apparently an extension of the lockdown period for such children. So, the children were continually exposed to the same environment and contributing factors that all the children faced during lockdown. Another possible explanation is that the teachers, often the first to identify children’s behavioral problems, are absent in this scenario.
Finally, knowledge inadequacy among the parents was significantly associated with worsening symptoms. This was highly expected, as parents with inadequate knowledge about their child’s condition will have less health-seeking behavior. Small changes in their child’s symptoms might have gone unnoticed and little attention was paid to them.
Socioacademic Profile
Only children enrolled in school were included. Those children’s academic performances were compared by interviewing the accompanying parents about their pre-COVID and post-COVID scholastic performance. A worrying fact was that a sizeable number of children were not attending school. These findings corroborated earlier studies on the academic performance of children with ADHD. Inattention and unwillingness to study were blamed as the primary reasons behind their underperformance.13,14 Even among those who were attending school, a majority of them reported a high frequency of absence. As most of the children came from underprivileged rural backgrounds, poor internet and road connectivity, poverty, and loss of income also may have played a role in the academic backwardness.
Knowledge and Perception Regarding ADHD
Most parents had inadequate knowledge regarding ADHD. These findings corroborated an earlier study where parents reported poor knowledge of ADHD. 15 However, they differed from a study conducted in Florida, USA, where 98.2% of parents had heard of ADHD, and 78% considered themselves knowledgeable about it. 16 Since the study was conducted in a government hospital setting, most patients who attended the OPD came from rural areas, from a low socioeconomic class, and with very meager resources. Thus, their source of information was very limited. Their only information source was their doctor, who had explained to them that it is a “mental disorder” and nothing more.
All the parents opined that it is a real disease, which was considerably more than the 78% figure reported by an earlier study. 15 All of them opined that sugar does not cause ADHD, compared to a study where 27% of parents thought that sugar causes ADHD. 16 A small majority answered that a child can be appropriately labeled as having ADHD, if not necessarily overactive. These findings were corroborative with an earlier study. 6
None of the parents commented on which religious group had the highest prevalence. Lack of awareness can be blamed for this. Most parents felt that medications and counseling combined were the mainstay of treatment. This corroborated with another study. 15 Finally, all the parents considered the disease curable, probably due to the confidence provided to them by their doctors and psychologists and that motivated them to continue their child’s treatment despite all the hardships.
Overall, the gap in knowledge calls for more focused government initiatives and health programs to combat this disease. Health education programs need to be more inclusive. Also, more research is needed since the research literature in India regarding ADHD is scanty.
However, the study had certain limitations. The limited availability of time, that is, 2 months, prevented us from interviewing a large number of patients, making the sample size small and increasing the chances of bias were increased. The parental education was not assessed, which may act as a bias in the outcome regarding parental knowledge of the disorder. Most parents had a rural background and belonged to the underprivileged section of society. Because of the limitations of available resources, many have inadequate knowledge about the intricacies of ADHD. This reduces its generalizability. Many had not heard about ADHD and hence we were able to assess further details. The lockdown ended in February 2022, whereas the data was collected from July to September 2022, almost 5–6 months after the lockdown ended. Other factors, such as natural progression, could have affected ADHD symptoms.
Many questions still remain unanswered. The effects of worsening symptoms or the parental stress levels of such children in other parts of the country have also been poorly researched. The knowledge adequacy of the general population, teachers, healthcare workers, and normal school-going children must also be assessed.
Large-scale studies spread across the state and country, involving primary-level and secondary-level healthcare centers, are essential to get a more accurate reflection of the problem. The study emphasizes the need for more intense and elaborate psychoeducation.
Conclusion
School closure for prolonged periods, as adopted during the COVID lockdown, may serve some temporary respite in exigencies but is detrimental, especially in children with pre-existing mental health needs like ADHD. There was a significant association between school closure due to lockdown and the worsening of symptoms of ADHD among school-going children aged 6–15 years. The results indicate that health education and medical support programs must be implemented on a much larger scale. Policymakers should consider this aspect seriously while notifying similar school closure decisions in future emergencies. More Indian research is needed on ADHD to fill the existing gaps in knowledge.
Footnotes
Acknowledgements
The authors are grateful to the institution for their technical assistance. The authors are also grateful to the ICMR STS program for its valuable support and financial assistance.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The project was carried out as a part of the ICMR Short-Term Studentship Program (2022–3072).