
Abstract
Background:
Injection drug use remains a significant public health concern globally, with injection drug users (IDUs) facing elevated risks of contracting blood-borne infections such as hepatitis C (HCV), hepatitis B (HBV), and acquired immune deficiency syndrome caused by the human immunodeficiency virus (HIV). This study delves into the seroprevalence of these disorders among IDUs in Kashmir and extends further to explore the relationship between injection drug use and psychiatric co-morbidities.
Methods:
A cross-sectional study was conducted among IDUs recruited from tertiary care drug addiction centers. Those who agreed to participate underwent serological testing for HCV, HBV, and HIV. The presence of psychiatric disorders was assessed using the Mini International Neuropsychiatric Interview, a standardized instrument for diagnosing mental health conditions.
Results:
The results showed that the prevalence rate of HCV, HBV, and HIV was 73%, 12%, and 1%, respectively. Genotype 3a was the predominant genotype in 71 (51.5%) participants with detectable HCV-RNA. A total of 151 (50.3%) participants had a comorbid psychiatric illness with attention-deficit hyperactivity disorder and major depressive disorder in 63 (21%) and 36 (12%), respectively. Sharing of paraphernalia was the most common high-risk behavior in 234 (78%). Early initiation of opioid use, a history of sharing of paraphernalia, and the presence of comorbid psychiatric illness were found to be significantly associated with positive serology results, indicating a higher risk of contracting infection (χ2 = 24.55, p < .01; χ2 = 121.56, p < .01; and χ2 = 4.534, p <.01, respectively).
Conclusion:
IDUs have an elevated prevalence of HCV, substantial rates of infection with HBV and HIV, and a considerable burden of psychiatric morbidities. Considering the high seroprevalence of hepatitis infections and alarming rates of psychiatric morbidity in IDUs, this calls for a comprehensive and integrated approach to address the interconnected challenges faced by IDUs in Kashmir.
The IDUs have a high prevalence of infections such as HCV, HBV, and HIV. The IDUs often experience significant psychiatric issues and are likely to engage in high-risk behaviors.Key Messages:
Injection drug use involves introducing a substance into the bloodstream using a hollow hypodermic needle and syringe, penetrating the skin to reach the body. The drugs can be administered through veins (IV drug use), under the skin (skin popping), or into the muscle (IM injection).1,2 Opioids are the most commonly injected substances; other drugs like barbiturates, benzodiazepines, amphetamines, and cocaine can also be administered by this method. In Asian countries, heroin is the most commonly injected substance, although 70%–80% of individuals engaging in injection drug use utilize multiple drugs.3–6 This practice presents a significant public health challenge that has garnered global attention. Currently, there are approximately 13.48 million IV drug users worldwide facing severe health consequences. 7 It has been estimated that India has 8,50,000 injection drug users (IDUs), and Jammu and Kashmir is home to 25,000 IDUs. 8
Injection drug use is linked to a multitude of complications, including acute, medical, local, social, and psychiatric. Acute complications include fatal respiratory depression due to overdose, posing a significant risk of death.9,10 Medical complications include pneumonia; cardiovascular effects such as Takotsubo cardiomyopathy, arrhythmias, and heart attacks; CNS complications like stroke and GI effects including constipation, stomach ulcers, and perforation; renal complications may manifest as kidney failure due to rhabdomyolysis.11–14 Local complications include abscesses, cellulitis, and arterial damage due to unintended intra-arterial injection leading to pseudo-aneurysms and arteritis causing vasospasm and thrombosis, compartment syndrome, and tissue necrosis, sometimes requiring amputation of fingertips and forearms.15,16
IDUs are at a higher risk of contracting blood-borne infections like those caused by the hepatitis B virus (HBV), the hepatitis C virus (HCV), and the human immunodeficiency virus (HIV). IDUs are the major contributors to the global disease burden due to infection by these viruses. 17 HCV infection is the most prevalent in IDUs because of its high transmissibility, and even a single instance of the sharing of paraphernalia is identified as sufficient for HCV transmission.18,19 Chronic HCV infection leads to the development of chronic liver disease, including cirrhosis and end-stage liver disease. Approximately 80% of individuals exposed to HCV progress to chronic infection, and 3%–11% develop liver cirrhosis within 20 years. 20 Co-infection with HIV and HCV adversely impacts the prognosis of both. 20 Five percent of adults exposed to HBV develop chronic infection, cirrhosis, and death due to hepatocellular carcinoma (HCC), which are significant complications associated with chronic HBV infection. 21 HIV prevalence in India is concentrated among specific populations, particularly sex workers, IDUs, and homosexual men, referred to as “most at-risk populations.” 22 Among these groups, IDUs exhibit the second-highest prevalence in the country, at 7.14%. HIV is associated with depression, anxiety, psychosis, and HIV-associated neurocognitive disorders. 22
Psychiatric disorders are among the top 10 leading causes of disease burden worldwide, affecting nearly 1 billion, and substance use disorder (SUD) patients are more susceptible to developing psychiatric and/or medical co-morbidities. 23 Compared to patients with a single psychiatric disorder, those with comorbid drug use face limited treatment access, higher hospitalization rates, poorer treatment outcomes, a greater prevalence of suicide, and increased morbidity and mortality.24–27 Psychiatric illnesses may precede or follow substance use, both driven by common risk factors. The risk of developing substance use increases manifold in the presence of psychiatric conditions, especially when untreated. This may be explained by the “self-medication hypothesis,” suggesting individuals use substances to cope with mental health challenges. 28 Conversely, substance use may lead to mental health issues and/or trigger or worsen underlying mental health conditions. 29 SUDs and psychiatric illnesses can coexist independently due to shared risk factors like trauma, stress, negative temperament, impulsivity, and genetic influences. Family history, conflict, academic failure, economic deprivation, childhood adversity, and social exclusion are also recognized as risk factors for both drug use disorders and mental health problems. 30
Methods
Study Aims
(i) To determine the seroprevalence of HIV, HBV, and HCV infection among IDUs. (ii) To study the associated psychiatric co-morbidities among IDUs.
Study Design
This hospital-based study was conducted at the drug addiction center of a tertiary care hospital, which has an in-patient facility for individuals with SUD. The study, which was cross-sectional in design and conducted over 18 months, represented the population of the entire valley.
Study Sample
The sample size was determined using a formula with a 95% confidence interval, a 5% margin of error, and an anticipated prevalence of opioid use based on previous studies, resulting in a calculated value of 289.
Study Population
Three hundred participants were recruited consecutively from the outpatient and inpatient departments of Institute of Mental Health and Neurosciences, Government Medical College, Srinagar, Jammu and Kashmir, India. All the IDUs who fulfilled the inclusion criteria were recruited for the study. The triple serology test for HIV, HBV, and HCV is done as a baseline in the hospital’s laboratory.
Interview Process
Interviews were conducted in a single setting, with selected patients interviewed at the time of entry into the study. Individuals were interviewed when they were stable and not intoxicated/withdrawn. Written informed consent was obtained in the local, understandable language, and rigorous measures were taken to maintain confidentiality. Participants were briefed about the purpose of the interview, and incomplete interviews were not considered. Individuals who tested positive during triple serology screening via the chemiluminescent immunoassay method underwent additional confirmatory testing using the enzyme-linked immunosorbent assay (ELISA) method. Subsequently, individuals confirmed positive by ELISA were tested further to determine HCV-RNA levels, HCV genotype, and/or HBV DNA levels.
Operational Definitions
The IDU was defined as a patient with opioid use disorder (OUD) having a history of using injection opioids in the last 12 weeks. 31 A history of sharing of paraphernalia was considered positive if the patient reported needles and/or syringe sharing in the last 12 weeks, that is, having injected with the same needles and syringes as any of their injecting partners during the last 12 weeks (both borrowing and lending). 32
The research work was initiated following approval by the institutional Ethical Committee and Board of Research Studies (BORS). Inclusion criteria included: (a) active injection drug user (verified by evidence of fresh injection stigmata and a positive drug screen test for opiates); (b) self-reported injection drug use within the past 12 weeks; those willing to participate in the study by providing written informed consent. The following participants were excluded: (a) those with acute substance intoxication, withdrawal, and/or delirium; (b) those with a history of leprosy, tuberculosis, COPD, bronchial asthma, or severe liver disease.
Measures
The following instruments were utilized in the study.
A semi-structured proforma was prepared that recorded the socio-demographic variables: age, gender, education, occupation, marital status, family type, residence, status of HIV/HBV/HCV, and presence of high-risk behaviors.
Kuppuswamy’s Socio-demographic Scale
It is a measurement tool that calculates a composite score based on the education and occupation of the head of the family, as well as the monthly income of the household. This score ranges from 3 to 29. This scale utilizes the variables of education, occupation, and family wealth to categorize research groups into five distinct social classes: (a) upper, (b) upper middle, (c) lower middle, (d) upper lower, and (e) lower socio-economic status. 33
The Mini-International Neuropsychiatric Interview v.7.0.2 (M.I.N.I.) is a structured diagnostic interview with high reliability and validity for DSM-5 and ICD-10 psychiatric disorders. It is designed to meet the need for a short and accurate structured psychiatric interview for multicenter clinical trials and epidemiological studies. It was used for the assessment of psychiatric co-morbidities, and all the diagnoses were confirmed by a consultant psychiatrist. 34
Statistical Analysis
Data were entered in Statistical Package for Social Sciences (SPSS) V27. 35 Descriptive statistics was used for continuous variables, and the chi-square test was applied for categorical variables. Group scores were compared using the chi-square test and the Student’s t-test. All p values were two-sided, and a p value < .05 was considered statistically significant.
Results
Participants’ Socio-demographic Characteristics
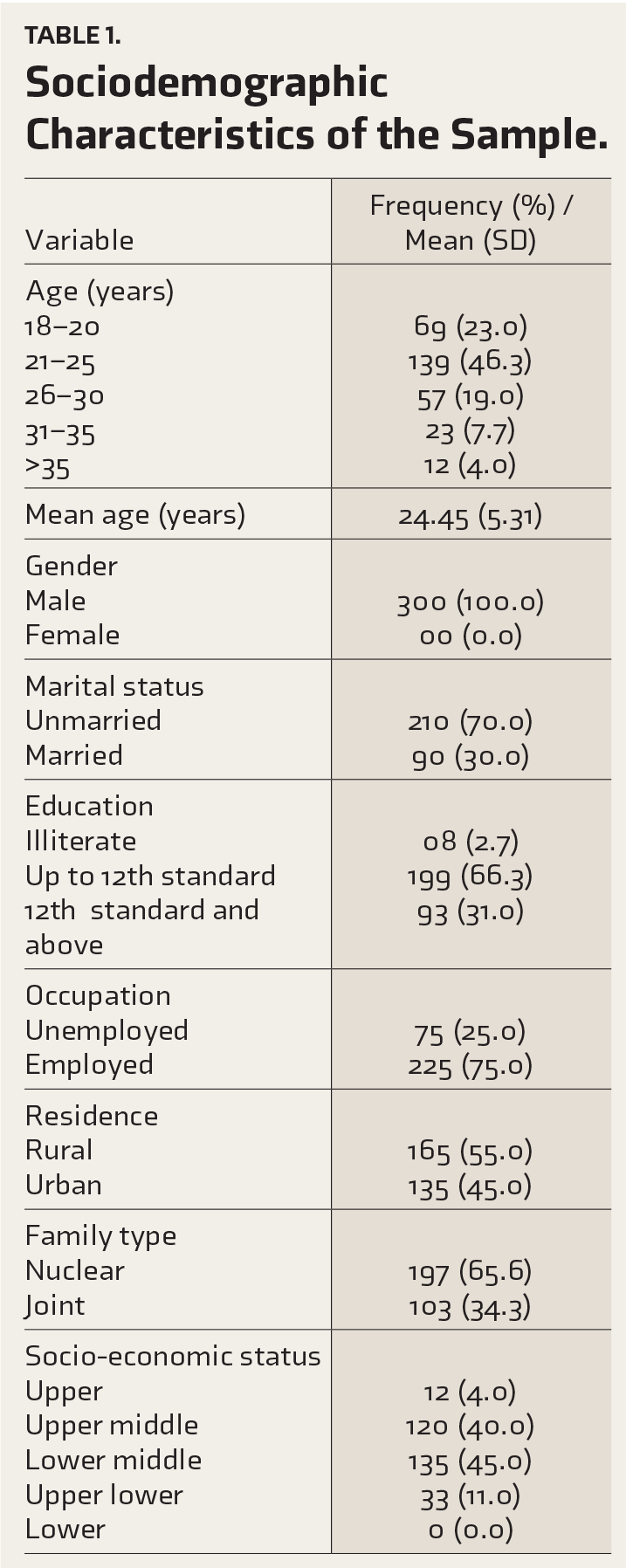
The study sample predominantly consisted of individuals in early adulthood, with a mean age of 24.45±5.31 years, as depicted in Table 1. Among the participants, 210 (70%) were unmarried, 199 (66%) had completed education up to the 12th grade, 165 (55%) resided in rural areas, 197 (65%) belonged to nuclear families, and 255 (85%) were classified within the middle-class socio-economic status.
Sociodemographic Characteristics of the Sample.
Participants’ Clinical Characteristics
The mean age of initiation for opioid use and injection opioid use of the participants was 21.41±5.36 and 22.58±5.41 years, respectively. Seropositivity for HCV was observed in 216 (72%) of participants, and HCV-RNA was detected in 138 (46%), with genotype 3 detected in 91 (65.9%). Within genotype 3, subtype 3a was the most commonly seen in 71 (51.3%), while subtype 3b was identified in 14.4%. Our study’s second most frequent genotype was genotype 1, in 24.5%, with subtype 1a in 14.4% and 1b in 10%, while genotype 4 was identified in 9.4%. A history of sharing paraphernalia was reported by 234 (78%) of the participants, while 20 (6.6%) reported a history of unprotected sexual intercourse. Furthermore, as can be seen in Table 2, 151 (50.3%) of participants had a comorbid psychiatric illness, with ADHD being the most prevalent at 63 (21%), followed by MDD at 36 (12%). Personality disorders were diagnosed in 28 (9.3%), generalized anxiety disorder in 13 (4.3%), and obsessive-compulsive disorder in 06 (2%).
Clinical Characteristics of the Study Sample.
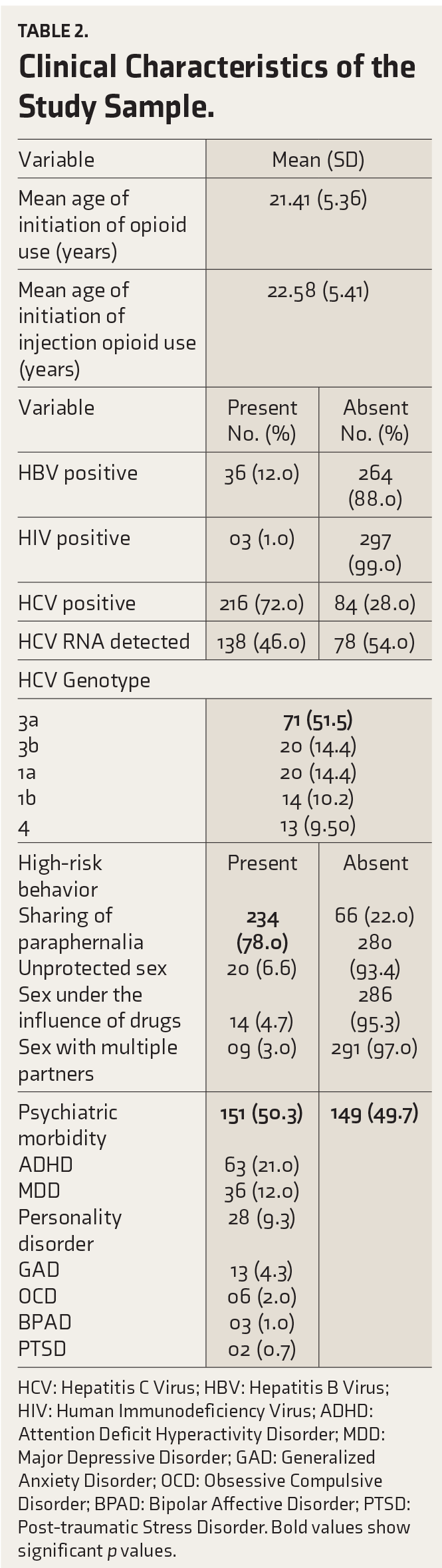
HCV: Hepatitis C Virus; HBV: Hepatitis B Virus; HIV: Human Immunodeficiency Virus; ADHD: Attention Deficit Hyperactivity Disorder; MDD: Major Depressive Disorder; GAD: Generalized Anxiety Disorder; OCD: Obsessive Compulsive Disorder; BPAD: Bipolar Affective Disorder; PTSD: Post-traumatic Stress Disorder. Bold values show significant p values.
Association Between Serological Status and Demographic and Clinical Variables
The association between serological status and various sociodemographic and clinical variables is shown in Table 3. Individuals testing positive on serology exhibited a lower mean age of onset for both opioid and injection opioid use, with a p value < .01 for both. Additionally, positive serology was significantly associated with unemployment (p = .01), a history of psychiatric illness (p = .03), and a history of sharing paraphernalia (p < .001). However, HCV prevalence was similar among urban and rural residents, but co-infection with HBV and HCV was more common in rural areas (p value < .01).
Association of Serology with Demographic and Clinical Variables.
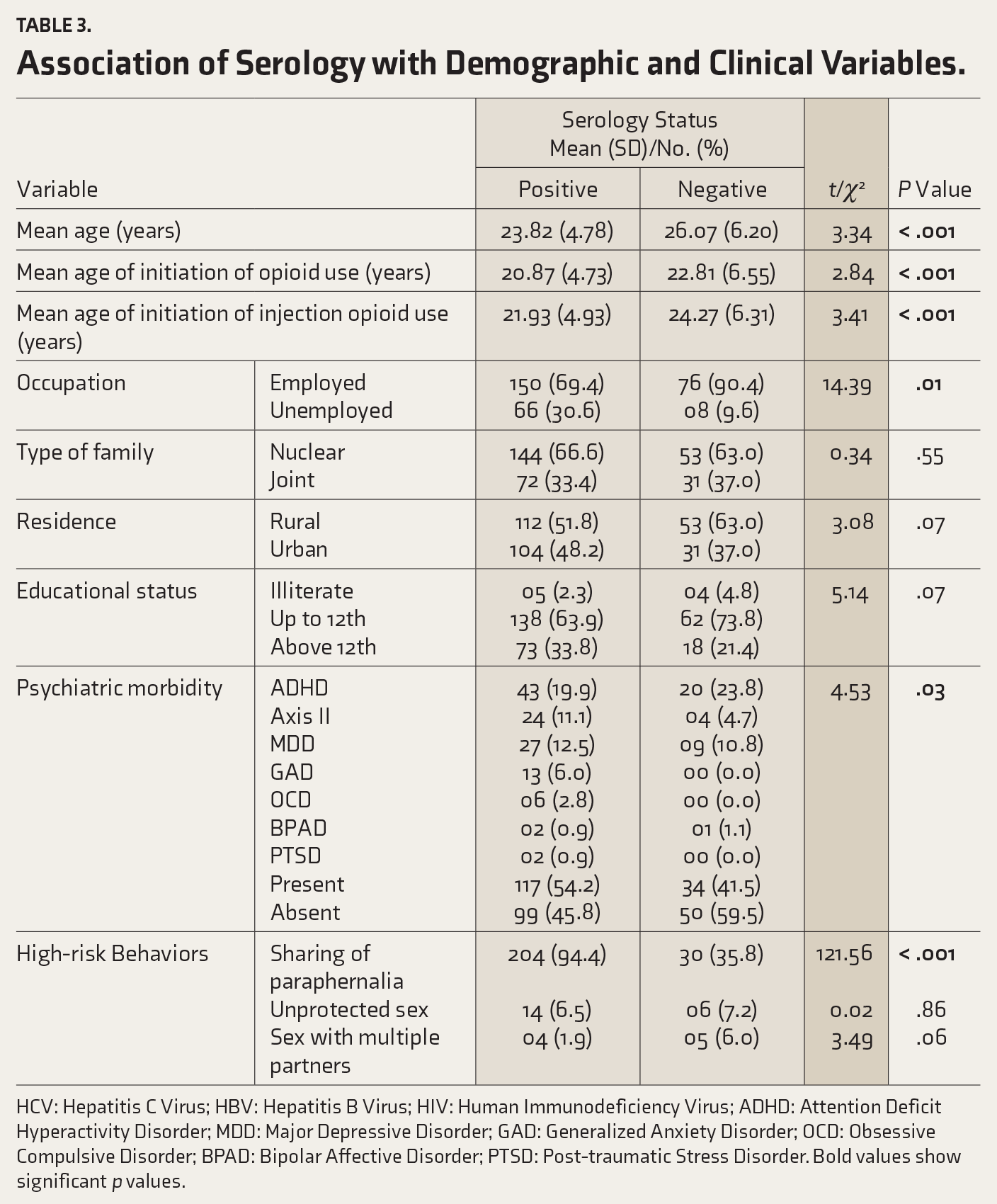
HCV: Hepatitis C Virus; HBV: Hepatitis B Virus; HIV: Human Immunodeficiency Virus; ADHD: Attention Deficit Hyperactivity Disorder; MDD: Major Depressive Disorder; GAD: Generalized Anxiety Disorder; OCD: Obsessive Compulsive Disorder; BPAD: Bipolar Affective Disorder; PTSD: Post-traumatic Stress Disorder. Bold values show significant p values.
Comparison of Psychiatric Morbidity Across Demographic and Clinical Variables
The presence of psychiatric morbidity showed an association with a younger age of onset for both opioid and injection opioid use, with p = .01 and p < .001, respectively, as evident in Table 4. However, no statistically significant differences were observed between the two groups concerning the history of sharing of paraphernalia (p = .61), positive serology for HCV (p = 0.52), and positive serology for HBV (p = .75).
Comparison of Psychiatric Morbidity Across Variables.
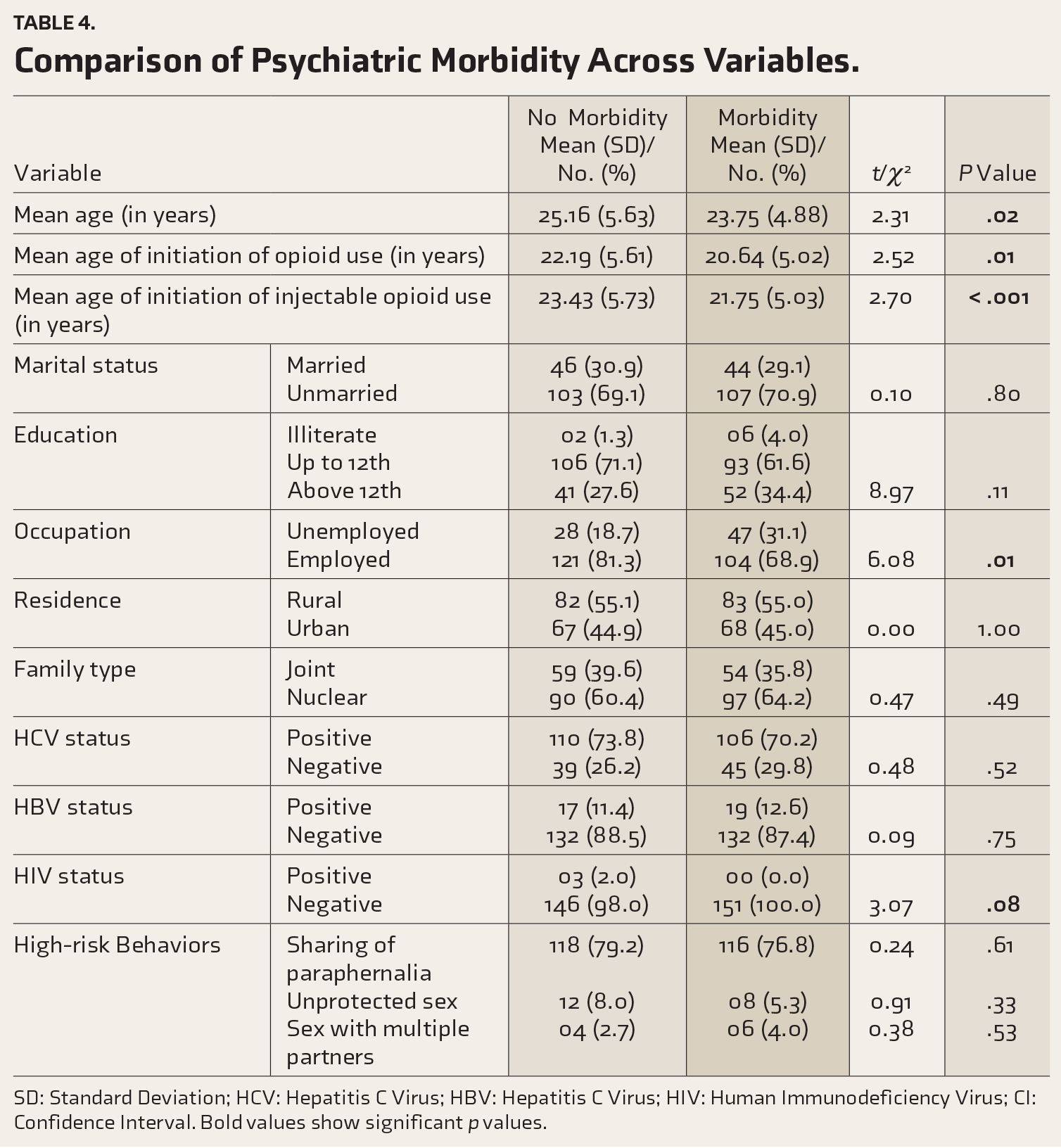
SD: Standard Deviation; HCV: Hepatitis C Virus; HBV: Hepatitis C Virus; HIV: Human Immunodeficiency Virus; CI: Confidence Interval. Bold values show significant p values.
Discussion
Injection drug use represents an extreme form of illicit substance use, persisting as a significant challenge in India, posing a grave risk of blood-borne infections such as HBV, HCV, and HIV, primarily facilitated through needle sharing and related paraphernalia.36,37 These viral infections can manifest in a spectrum of severity, ranging from mild illness to life-threatening conditions like cirrhosis, HCC, and death, highlighting the critical importance of early detection and intervention to mitigate organ damage and enhance prognosis. Recently, data compiled by the UNODC revealed a significant global burden of HCV, HIV, and HBV infection among IDUs, with estimated prevalence rates of 50.6%, 11.9%, and 7.5%, translating to approximately 6.8, 1.6, and 1.1 million individuals, respectively, within this vulnerable population. 38 Notably, 23%–39% of new HCV infections occur among people who inject drugs, and one in three HCV deaths are attributable to injection drug use. 39
Our study revealed several key findings among IDUs: (a) a huge prevalence of HCV infection; (b) early onset of opioid use and injection opioid use; (c) the substantial occurrence of high-risk behaviors, particularly sharing paraphernalia; and (d) a significant burden of psychiatric morbidity within the IDU population.
The mean age of participants was 24.45 + 5.02 years, with the majority between 21 and 25 years and only 4% over 35 years, aligning with findings from other studies emphasizing young adulthood. 40 All participants were males, reflecting barriers faced by females in seeking treatment due to the lack of awareness and associated stigma. 41 Many studies have suggested that women face more obstacles and barriers affecting access and entry to substance use treatment. 42 Most of the study participants were literate, unmarried, from rural areas, and living in nuclear families, which is explained by the fact that most of the sample belonged to early adulthood, a demographic more likely to be educated, and Kashmir being a predominantly rural population. Individuals living in nuclear families may face heightened life stresses without extended family support, potentially increasing vulnerability to substance use.
A notably high prevalence of blood-borne infections was seen, with 73% testing positive for HCV, 12% for HBV, and 1% for HIV. These findings are consistent with previous research indicating a high prevalence of such infections in IDUs. Indian studies demonstrate a wide range of HCV seropositivity among IDUs, varying from 20% to 90%, with a recent study showing a prevalence of 50%. 43 Certain regions, such as Manipur, exhibit particularly high rates (90%–98%).44,45 It is pertinent to mention that studies consistently show higher rates of HCV compared to HBV and HIV. 46 Global studies, such as one conducted by Anderson et al., also emphasize the higher prevalence of HCV among IDUs compared to HIV, with rates of 52.7% and 6.2%, respectively, surpassing general population rates (3.4% for HCV and 1.8% for HIV). 47 This elevated prevalence can be attributed to the presence of high-risk behaviors, notably needle sharing and the sharing of paraphernalia among IDUs. The increased transmissibility of HCV per unit of blood contributes to its higher prevalence compared to HBV and HIV. 19
The HCV-RNA was detected in 46% of HCV-positive participants, consistent with rates reported in other studies ranging from 30% to 38%.48,49 HCV-RNA testing directly detects the genetic material of HCV in the blood, confirming active infection and indicating ongoing viral replication. The most common HCV genotype detected was genotype 3, specifically subtype 3a, followed by 3b. Our study’s second most frequent genotype was genotype 1, followed by genotype 4. These findings are consistent with past studies, which reported genotype 3a as the most common. 50 Understanding the specific genotypes is crucial for predicting therapeutic responses and determining the appropriate duration of treatment. 51 It is essential to assess the risk of transmission and monitor the treatment response. In the Indian context, genotype 3 is predominant, followed by genotype 1. Genotype 3 is more prevalent in the northern, eastern, and western regions of India, while genotype 1 is more commonly found in southern India. 52
The sharing of paraphernalia was present in 78% of the study population. In comparison, sex under the influence of drugs was reported by 4.67% and sex with multiple partners by 3%, indicating that the sharing of paraphernalia is the most common high-risk behavior among IDUs. These findings are consistent with previous research, a study conducted by Karlsson et al. in a Swedish remand prison, where 56% of IDUs admitted to lending out used needles or syringes and 62% admitted to receiving already used injections. 53 The studies have consistently shown a wide prevalence of sharing of paraphernalia, ranging from 55% to 75% among IDUs.54,55 Reasons for sharing paraphernalia may include the unavailability of clean syringes and a lack of awareness regarding the adverse consequences. Our study demonstrated a significant increase in HCV among individuals who engaged in the sharing of paraphernalia compared to those who did not, with 87.17% versus 18.18% testing positive for HCV, respectively (p < .001). This association between the sharing of paraphernalia and HCV infection has been consistently observed in prior studies. 56 However, we did not find a significant association between HCV seroprevalence and the number of sexual partners or unprotected sexual intercourse, consistent with findings from other research studies. 57
A total of 50.3% of individuals had a concurrent psychiatric illness, with ADHD being the most prevalent disorder, followed by MDD. Similar studies have shown that over half of substance users have experienced at least one psychiatric illness in their lifetime. 25 A study conducted by Dar et al. identified psychiatric morbidity in 67% of participants, with ADHD as the most common diagnosis. 58 There is a reciprocal relationship between drug use behavior and psychiatric morbidity, wherein each exacerbates the occurrence of the other. Individuals with psychiatric disorders are more susceptible to engaging in substance use, and conversely, substance use increases the likelihood of developing psychiatric illnesses. 59 Individuals with ADHD often have impulsivity and difficulty with self-regulation, which can increase the likelihood of experimenting with substances at an earlier age and engaging in risky behaviors like sharing paraphernalia. 60 The heightened prevalence of psychiatric illnesses can also be attributed to various psychosocial challenges, including insufficient social support, experiences of discrimination, and living arrangements characterized by solitude. Pertinent to mention that one-third of our participants faced challenges related to their primary support groups, such as family disruption through separation/divorce, removal from the home, physical abuse, and inadequate discipline, which further exacerbated their susceptibility to psychiatric illnesses. Financial hardships resulting from the detrimental cycle of continuous drug use and its consequences also contribute to the vulnerable situation of IDUs. The current study showed that, compared to individuals without psychiatric morbidity, those with psychiatric morbidity are more likely to be unemployed and have an early age of initiation of both opioid and injectable opioid use. However, no significant differences between the two groups were seen concerning high-risk behaviors and HCV positivity.
The alarming prevalence of HCV among IDUs represents a significant public health concern, with the convergence of high-risk behaviors like needle-sharing leading to a disproportionate burden of HCV within this population, only to be further complicated by startling rates of comorbid psychiatric illnesses. The findings highlight the critical importance of comprehensive testing and intervention strategies, emphasizing the need for early detection through routine screening programs restricting further transmission. Moreover, targeted interventions, such as needle exchange programs, opioid substitution therapy, and access to evidence-based treatment for substance use disorders, are vital components of harm reduction efforts aimed at curbing HCV transmission rates.
Strengths
While many studies have been conducted among substance users, our study was the first of its kind, focusing on IDUs in Kashmir. Our study is the first one conducted to find the seroprevalence of HCV, HBV, HIV, and psychiatric morbidities in this high-risk population in Kashmir.
Limitations
The assessment was conducted at a single center, so the findings cannot be generalized to the community. The study lacked a control group (non-IDUs) for comparative analysis.
Conclusion
The study reveals a troubling landscape marked by high seroprevalence of HCV, significant rates of HBV and HIV, and a prevalent burden of psychiatric co-morbidities. The findings highlight the urgent need for strengthened screening protocols to identify undetected infections, especially given the often asymptomatic nature of HCV infection. The coexistence of mental health issues, notably ADHD, MDD, and anxiety disorders, emphasizes the complexity of addressing both substance use and psychiatric co-morbidities. It also highlights the role of sharing paraphernalia in spreading infections, particularly HCV, and underscores the necessity for targeted education on safe injection practices within this population. In conclusion, a comprehensive and integrated approach is imperative to address the interconnected challenges faced by IDUs in Kashmir.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
The research work was initiated following approval by the Institutional Ethical Committee, Government Medical College Srinagar, via No: IEC/GMCSGR/2024/PSY/141 and BORS (Board of Research Studies) of Government Medical College Srinagar, Jammu and Kashmir, India.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.